
Abstract
Study Design:
Narrative literature review and expert recommendation.
Objective:
To establish treatment recommendations for axis ring fractures based on the knowledge of the experts of the Spine Section of the German Society for Orthopaedics and Trauma.
Methods:
This recommendation summarizes the knowledge of the experts of the Spine Section of the German Society for Orthopaedics and Trauma with regard to the treatment of axis ring fractures based on a narrative literature review.
Results:
Typical “hangman’s fractures” with bilateral separation of the neural arch from C2 and atypical “hangman’s fractures” with irregular fracture morphology are described. Computed tomography is the “gold” standard used to detect and analyse these fractures adequately. Furthermore, the detection of vertebral artery integrity is necessary. To classify axis ring fractures, the Levine-Edwards or Josten classification is recommended. In particular, the integrity of the C2/3 disc and the integrity of the anterior longitudinal ligament are used to determine the treatment strategy. While Levine-Edwards type I and type IIA (Josten type 1 and 2) fractures should be treated conservatively, Levine type II and type III (Josten type 3 and 4) fractures should be treated operatively. Levine-Edwards type II fractures will be predominately treated by anterior C2/3 fusion. Levine-Edwards type III fractures have to be primary reduced, if an anterior fusion is planned (anterior cervical discectomy and fusion [ACDF] C2/3). If a closed reduction of a type III fracture is impossible, an open reduction and posterior fixation/fusion is the treatment of choice.
Conclusion:
Conservative treatment is predominantly reserved for Levine-Edwards I and IIA fractures. Operative treatment should be performed in case of Levine-Edwards II and III fractures.
Keywords
Introduction
The upper cervical spine displays a unique anatomy and biomechanical properties, which, in case of trauma, can result in specific injury patterns. One particular type of injury is an axis ring fracture, also referred to as a “hangman’s fracture” or traumatic spondylolisthesis of the axis. These fractures can be subdivided into 2 fracture subcategories. The first is the common form of a “hangman’s fracture” with bilateral fracture of the pars interarticularis. The second, is an atypical/asymmetrical “hangman’s fracture” involving the vertebral body at C2 bilaterally or the pars interarticularis and the posterior cortex of C2 unilaterally at the contralateral side.
The following recommendations for the treatment of “axis ring fractures” rely on the experiences of the participating spinal surgeons of the Spine Section of the German Society for Orthopaedics and Trauma Society (DGOU) under consideration of the current literature. These recommendations refer to the diagnostics and treatment of acute traumatic axis ring injuries of otherwise healthy, skeletally mature patients with normal bone quality.
Pathobiomechanics
The term traumatic spondylolisthesis of the axis refers to the common location of failure in the pars interarticularis of the neural arch, the separation from the C2 vertebral body and the subsequent slippage of the C2 over the C3 vertebral body. The main cause of such an injury is a hyperextension or hyperflexion force 1 on the head with backward or forward tilt of the upper cervical spine. Such a force causes failure in the interarticular portion of the neural arch. Depending on the additional force vector along the longitudinal axis the injury mechanism can be a hyperextension-distraction injury (similar to “judicial hanging”) or a hyperextension-compression injury, which can be observed in injured vehicle occupants.
The distraction type injury may cause a complete disruption of all ligamentous structures thereby generating severe instability and sometimes fatal neurological damage to the spinal cord at the C2 level. The compression type injury might be associated with multiple fractures of the adjacent spinous processes or vertebral body fractures in the lower cervical spine. The exact location of the fracture line shows a high degree of variability, with fracture lines running through the isthmus itself, the facet joint surface and through the vertebral body.
An important criterion for stability of traumatic spondylolisthesis is the ligamentous integrity of the C2/3 motion segment. The 2 most significant features are firstly the integrity of the anterior longitudinal ligament (ALL) and secondly the integrity of the disc at C2/3 level. Especially in a hyperextension injury, with a 60° upward directed translational component, a rupture of the ALL might occur. 2
A neurological damage is rarely documented in survivors with an isolated traumatic spondylolisthesis. However, in case of “atypical/asymmetrical” traumatic spondylolisthesis C2, the posterior wall of the C2 vertebral body might stay partially connected to the neural arch. If the upper cervical spine is moving forward due to C2/3 instability, the myelon can be compromised and neurological damage (eg, Brown-Sequard syndrome 3 ) might be observed. 4
Clinical Symptoms
Patients complain mostly about neck pain, located in the upper cervical spine, rotational pain, and muscle tenderness. If additionally, a bruise on the head (frontal or parieto-occipital) is detectable, a spinal lesion should be carefully ruled out.
Frequency of neurological impairment, regardless whether temporary or permanent, varies among reported case series from 6.5% to 25%. 1,5,6
Basic Principles
The diagnostic algorithm applied should include precise morphological detection, classification and quantification of instability. In case of C2 ring fractures, a stable upper cervical spine with adequate restoration of cervical alignment and fracture gap closing are the most important treatment goals. If these fractures are treated surgically, then clinicians should aim to preserve the mobility of the upper cervical spine as much as possible.
Diagnosis
According to Schleicher et al,
7
there are 3 main goals of the diagnostic process: An awareness that patients with a suspicious trauma mechanism and/or complaints may suffer from this type of fracture. To determine whether the lesion is unstable or not. In case of an unstable lesion (which indicates the need for surgery) to decide on the surgical strategy; in particular whether to choose an anterior or posterior approach.
ImagingPlain X-rays have a low sensitivity for detection of a fracture of the cervical spine, with a false negative rate of up to 40%. 8 This is why computed tomography (CT) with axial cuts, including 2-dimensional (2D) reconstructions in the frontal and sagittal plane is the “gold standard” in detection of upper cervical spine fractures. Furthermore, CT allows for adequate fracture classification while also analyzing the fracture morphology and the extent of fracture dislocation.
Ding et al 9 detected a vertebral artery injury in 17.8% out of 101 patients with isolated C2 fractures more often in correlation with C2 traumatic spondylolisthesis. Therefore, in all cases with C2 traumatic spondylolisthesis, the detection of a concomitant vertebral artery injury is necessary. A conventional angiography, a CT angiography (CTA), or magnetic resonance imaging (MRI) angiography are potential tools used to detect a vascular lesion or an anatomical anomaly (eg, high riding artery). 10 -12
Assessment of Stability
Following identification of a fracture, the most critical step is to determine whether the present fracture is stable or unstable. Stability is mainly determined by the degree of discoligamentous injury at the C2/3 level, especially considering the integrity of the anterior longitudinal ligament (ALL).
If instability of the C2/3 complex is suspected, an additional MRI and/or fluoroscopic controlled functional imaging might be helpful to rule out unstable lesions of the ALL/PLL and/or the soft disc. 13
Figure 1 depicts a differentiated diagnostic algorithm, including CT, MRI, and functional imaging used in the analysis of fracture morphology and to determine fracture classification and stability/instability.
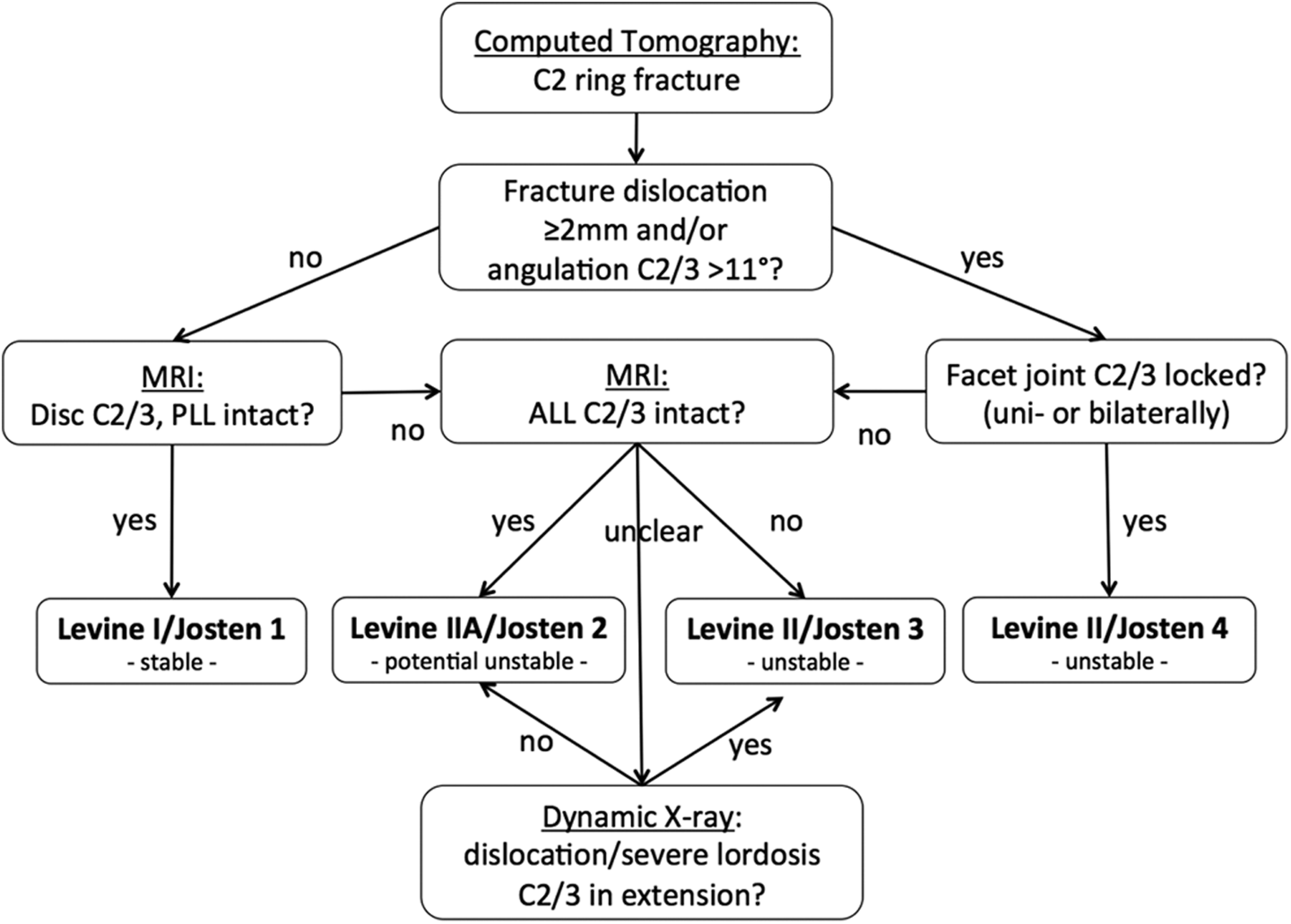
Flowchart for classification of axis ring fractures.
Radiographic Evidence for Segmental Instability
The following are radiographic evidence for segmental instability 7,14 -16 :
Significant angulation C2/3 ≥11°. Significant translation C2/3 ≥3.5 mm. Tear drop fragment endplate C2 or C3 (bony avulsion of ALL). Disc rupture/edema (MRI). Progredient hyperlordotic angulation C2/3 (Dynamic x-ray in extension).
Classification
Typical “Hangman’s Fractures”Typical hangman’s fractures should be classified using the modified Effendi 5 classification, described by Levine and Edwards 1 in 1985. Alternatively, the Josten 17 classification can be applied.
Levine-Edwards type I/Josten type 1 (Figure 2a) describes a nondisplaced “hairline” fracture of the neural arch. Fracture dislocation has to be less than 3 mm without angulation in the C2/3 disc, ALL, and soft disc remaining intact.
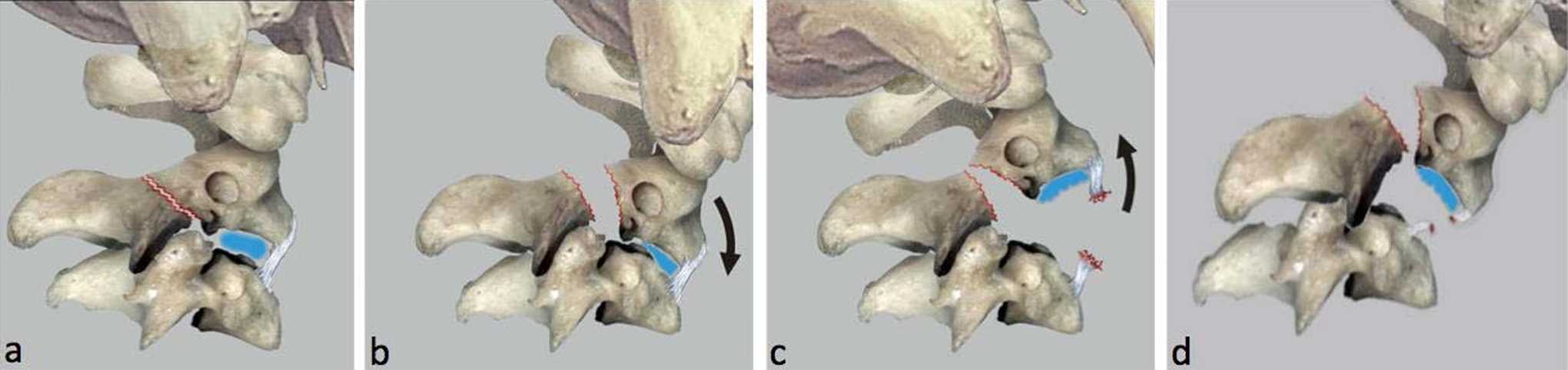
(a) Nondisplaced fracture “Levine-Edwards I/Josten 1”. (b) Significantly displaced fracture with intact anterior longitudinal ligament (ALL) and significant kyphotic angulation of C2/3 “Levine-Edwards IIa/Josten 2”. (c) Displaced fracture with significant lordotic angulation of C2/3 caused by ALL rupture “Levine-Edwards II/Josten 3”. (d) Displaced neural arch fracture with uni- or bilaterally locked facet joint C2/3 “Levine-Edwards III/Josten 4”. Image reprinted from Kandziora et al 42 with permission from Springer Images.
Levine-Edwards type IIA/Josten type 2 (Figure 2b) describes a moderate displaced fracture of the neural arch combined with a significant (≥11°) kyphotic angulation of C2/3 caused by PLL and disc rupture/disruption but intact “hinging” ALL (hyperflexion injury).
Levine-Edwards type II/Josten type 3 (Figure 2c) describes a significant displaced fracture of the neural arch with significant (>11°) lordotic angulation of C2/3. In contrast to Levine and Edwards who did not recognize a specific pathology at the ALL, Josten 17 described an ALL and disc rupture as cause for the severe instability of Josten type 3 injuries (hyperextension injury).
Levine-Edwards type III/Josten type 4 (Figure 2d) describes a neural arch fracture with moderate to significant dislocation in combination with a uni- or bilateral locked facet dislocation of C2/3 (hyperflexion/distraction injury).
Atypical “Hangman’s Fractures”
All nonsymmetrical fractures of the axis ring or fractures affecting the C2 body horizontally may be referred to as atypical “hangman’s fractures.” 4,18,19 A generally accepted classification for these fractures is currently not available. However, a recently published proposal of Al-Mahfoudh et al 18 unveils an optional classification system of the different morphological features of atypical “hangman’s fractures”:
Type 1 (horizontal fracture) describes a potentially displaced horizontally orientated fracture line through the body of C2 with an intact axis ring comparable to a Benzel 20 type I fracture.
Type 2a (oblique fracture) describes a unilateral oblique C2 body fracture with contralateral pars interarticularis fracture.
Type 2b (oblique fracture) describes a unilateral oblique C2 body fracture with contralateral fracture of the lamina.
Treatment
The indication for surgery usually depends on the estimated extent of instability. 7,13,14,16,21 -24 The flowchart for treatment of axis ring fractures in given in figure 3. Estimating the grade of instability and defining the appropriate classification according to the Levine-Edwards 1 or Josten 17 classification system is the most important step in decision making (Figure 1).
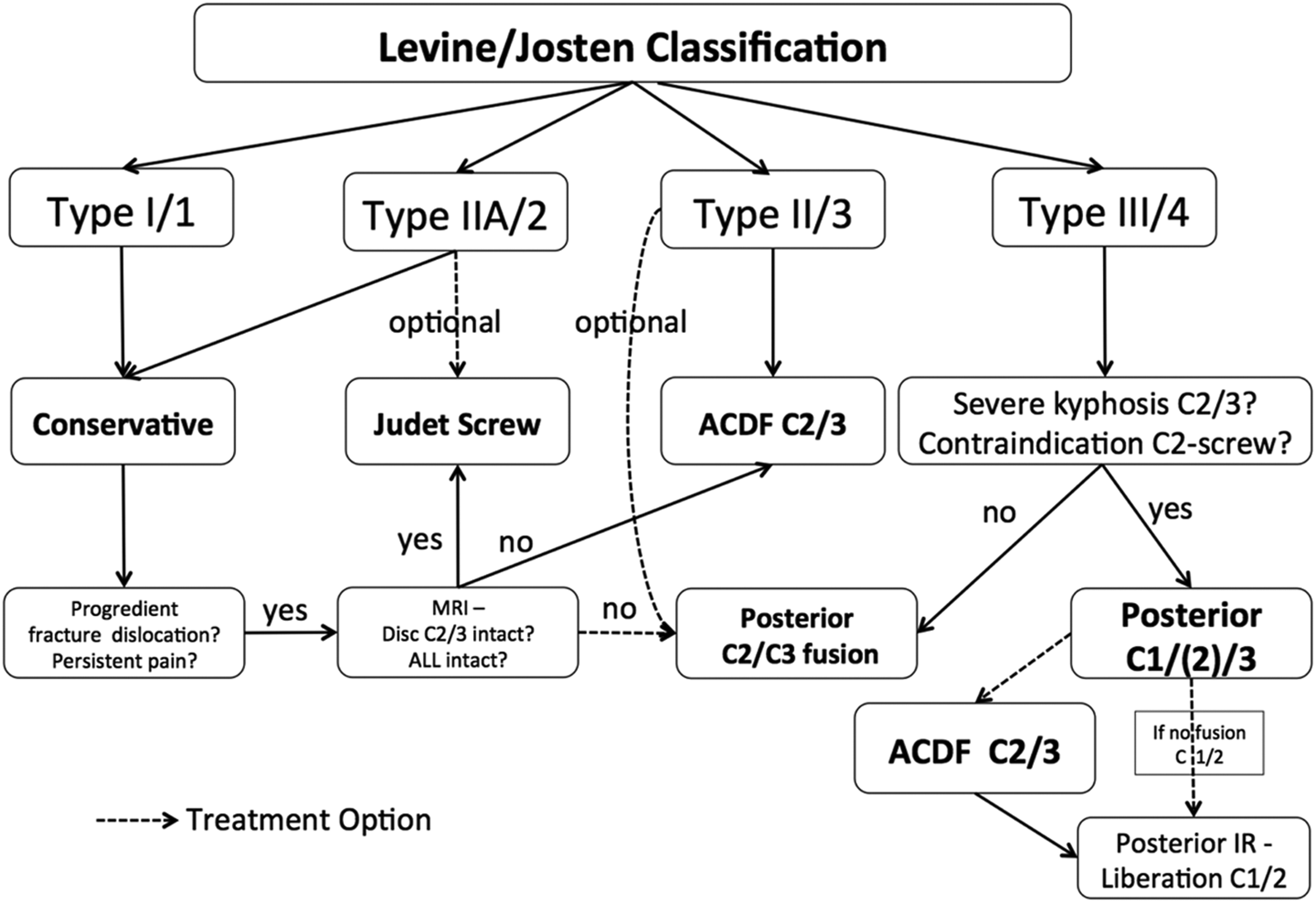
Flowchart for treatment of axis ring fractures.
Conservative Management
Possible therapeutic options include conservative management with external immobilization (eg, hyperextension cervical collar or halo vest immobilization). According to a systematic review by Murphy et al 23 comparing conservative management by halo vest immobilization versus rigid orthosis, no significant differences for union rate, mortality rate, treatment failure, or complications were detectable.
Taking potential complications of halo vest immobilization into account and acknowledging data from Murphy et al, 23 conservative treatment of axis ring fractures should be performed with a rigid cervical collar. Halo vest treatment should be reserved for gross unstable fractures with contraindication for surgical management.
Operative Treatment
Different operative strategies are described in the pertinent literature. According to Schleicher et al, 7 a C2 pars repair (Judet screw), a posterior monosegmental fusion (C2/3), a posterior bisegmental fusion/fixation (C1-C3), an anterior fusion of C2/3, and combined anterior-posterior/posterior anterior procedures are all potential treatment options.
From a biomechanical point of view, Arand et al 25 and Chittiboinna et al 26 indicated an increase of stiffness in flexion/extension after anterior cervical discectomy and fusion (ACDF) of C2/3 in comparison with that of an intact motion segment. However, a higher stiffness especially for bending and rotation was detectable for a posterior fixation in comparison with ACDF of C2/3. Dugal et al 27 compared the direct pars fixation with a posterior C2-pars/C3 fixation and were able to detect a persistent instability in flexion-extension for direct pars-repair favouring posterior C2/3 fixation.
Several authors published good clinical and radiological results either with an isolated anterior approach (ACDF of C2/3), 20,28,29 with a posterior-only approach, 30,31 as well as with a combined posterior-anterior approach. 32 In a recent review, Murphy et al 23 analyzed up-to-date evidence for the best possible approach (ACDF vs posterior fusion vs anterior-posterior fusion) but they did not find any difference in terms of union, mortality, and complications.
Treatment Suggestions
Levine-Edwards Type I/Josten Type 1 (Figure 2a)
Levine-Edwards type I/Josten type 1 fractures are stable injuries with intact ALL, PLL, and soft disc. These injuries are treated predominantly conservatively 33 with a rigid cervical collar (maximum 6 weeks). While treating patients conservatively, a short-term follow-up with lateral upper cervical spine x-rays should be performed to exclude progressive dislocation. Bony healing should be reassessed after 6 weeks by CT. In young patients with no complaints, normal x-ray follow-up should be sufficient to avoid further radiation.
In case of progressive dislocation or nonhealing with persistent pain, injury mechanism and classification should be reassessed (Figure 3).
Levine-Edwards Type IIA/Josten Type 2 (Figure 2b)
Levine-Edwards type IIA/Josten type 2 fractures are potentially unstable injuries with potentially soft disc rupture. These fractures should be treated conservatively if a closed reduction in a hyperextended head position is possible. This hyperextended head position should be maintained by using a modified (hyperextension) cervical collar or, in rare cases, alternatively by halo-traction/halo-vest immobilization for a period of 6 to 12 weeks.
If reduction cannot be maintained while treating conservatively and C2/3 disc disruption (MRI) is minor, isthmus reconstruction according to the Judet technique 34 is an option. 35,36 The C2-pars reconstruction may be performed with open surgery or with percutaneous procedure. 37,38 In case of severe C2/3 disc disruption (MRI) and/or contraindications for a C2-pedicle screw, an anterior C2/3 fusion with a cage and anterior plate is recommended. 39 Alternatively, a posterior C2/3 fusion can be performed. However, an adequate reduction and the possibility to perform C2-pedicle screws are mandatory if a short segment posterior fixation is planned.
Bony healing should be reassessed after 6 to 12 weeks by CT prior to completing patient treatment. In some instances, the fracture may heal well, but the soft disc may undergo progressive degeneration followed by instability and micro movements. This may require a secondary ACDF procedure.
Levine-Edwards Type II/Josten Type 3 (Figure 2c)
Levine-Edwards type II/Josten type 3 fractures are unstable fractures due to the discoligamentous instability with rupture of disc C2/3 and ALL. These fractures should be stabilized surgically. Alternatively, halo-traction is possible in case of operative contraindications.
While pathology and gross instability is mainly located in the C2/3 disc level, an anterior fusion C2/3 with adequate (indirect) reduction of the isthmic fracture should be performed.
Reassessment following anterior fusion is mandatory. In case of nonsufficient reduction of the isthmic fracture, an additional posterior lag screw fixation according to the “Judet” technique or posterior C2/3 fusion may be an option to avoid painful nonunion. 32
Levine-Edwards Type III/Josten Type 4 (Figure 2d)
Levine-Edwards type II/Josten type 4 fractures are unstable fractures due to disruption of the C2/3 disc, ALL rupture and facet joint luxation. These fractures should be stabilized surgically. Alternatively, halo-traction is possible in case of operative contraindications, if a closed reduction of facet joint luxation is possible.
An operative approach will be determined by the success of closed facet joint reduction. If closed reduction is possible, patients can be treated according to the guidelines for Levine-Edwards II/Josten 3 fractures with an ACDF of C2/3. If closed reduction fails, patients must be treated primarily with open posterior reduction and fixation. If adequate reduction of the isthmic fracture is possible, posterior fusion should be limited to the C2/3 segment. If C2/3 kyphosis is severe or an aberration of the vertebra artery prevents a correct screw placement, then the (temporary) inclusion of C1 in the fixation construct will allow optimal reduction and realignment. 26 In case of ALL rupture and disc disruption at the C2/3 level, an additional anterior fusion of C2/3 is recommended. This will allow for early posterior segment liberation of the temporarily fixed C1/2 level.
A potential alternative in case of ALL rupture and disc disruption at the C2/3 level is the combination of a C2-”Judet screw” and a lateral mass screw of C3 to avoid temporary C1 fixation. 30,36 However, to perform this strategy, adequate reduction of isthmic fracture is mandatory. A secondary anterior fusion of C2/3 is also recommended in order to create adequate stability.
Atypical “Hangman’s Fractures”
The treatment of atypical “hangman’s fractures” are determined by the extent of fracture dislocation and integrity of the C2/3 disc and the ALL with respect to the typical “hangman’s fractures.”
While oblique fractures and horizontal C2 fractures often involve the C1/2 joint, care has to be taken to achieve an adequate fracture reduction. This might prevent the patient from progressive C1/2 arthrosis with potentially persistent rotational neck pain.
If adequate reduction is possible and a C2-pedicle screw is possible, posterior fusion using a C2 lag screw-C3 fixation might be appropriate, if an atypical “hangman’s fracture” may not be managed conservatively. 4 Additional options are a posterior C1-3 fixation or an ACDF of C2/3 in case of contraindications to perform a C2-pedicle screw fixation.
Outcome
If stable axis ring fractures are managed conservatively, a high union rate of up to 93% might be achieved. 18,23 In contrast a failure rate of up to 50% has been described for conservative management of unstable axis ring fractures. 6,18,33 Analysing surgical treatment for unstable axis ring fractures, none of the aforementioned surgical techniques has proven superiority in terms of fusion rates, mortality and complications. 23 Hence, treatment selection should be based on fracture classification, experience of the surgeon and potential patient comorbidities.
Regardless of which treatment strategy will be selected, patient’s inability to work varies between 9 to 16 weeks. Return to full activity can be expected in about 40% of patients, with another 40% being restricted only in high-impact activity such as contact sports. 40,41 A fracture line through the inferior facet of C2 has been described as the major determinant of residual neck pain, which supports the algorithm with surgical treatment of displaced injuries. 40
Conclusion
This article describes current concepts; treatment options and the recommendations of the experts of the Spine Section of the German Society for Orthopaedics and Trauma regarding the treatment of axis ring fractures. Conservative treatment is predominantly reserved for Levine-Edwards type I and IIA/Josten type 1 and 2 fractures. Operative treatment should be performed in case of Levine-Edwards II and III/ Josten type 3 and 4 fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.