
Abstract
Study Design
Retrospective comparative clinical case series.
Objective
Burst C2 fractures are very rare. Treatment options include conservative treatment or fusion (anterior, posterior, or anterior and posterior). Anterior fusion addresses mainly hangman component. The bursting body usually needs posterior or combined anterior-posterior fusion, but both permanently sacrifice atlantoaxial motion. Can anterior-“first” approach preserve C1–C2 motion and restore function?
Methods
We report nine cases of burst C2 combined with C2–C3 spondylolisthesis and an odontoid fracture. The surgical group included six patients treated initially with an anterior approach, moving to a posterior one when necessary. All were treated with anterior diskectomy fusion using one session and one incision. The halo group included three patients treated conservatively using halo traction followed by rigid collar. Assessments included self-reported, physiologic, and functional measures. Reduction was assessed using Roy-Camille's criteria and improvement of canal compression ratio. Clinical outcome was graded excellent, very good, good, or poor according to pain, range of motion, and work status.
Results
Mean follow-up was 44.5 ± 8.3 (range 36.0 to 62.0) weeks. Results in the surgical group were judged to be excellent in four and good in two. One patient developed atlantoaxial osteoarthritis. Results were good in one patient and poor in two patients in the halo group. Two patients developed atlantoaxial osteoarthritis. All three cases had work limitations.
Conclusion
A single anterior approach achieved union and preserved C1–C2 motion and function in some cases. Conservative treatment achieved union but failed to achieve good reduction or good clinical outcome in grossly instable fractures. However, we believe that the ideal management is yet to evolve.
Keywords
Introduction
Axis fractures account for almost 20% of acute cervical spine fractures. 1 They include three types: odontoid fractures, traumatic spondylolisthesis of the axis, and body fractures. The axis body is the region between the odontoid base and the pars interarticularis. Benzel et al reported 3 sagittally oriented burst fractures among 15 body fractures. 2 Fujimura et al reported 3 burst fractures among 31 axis body fractures. 3 Hironobu et al reported a case of burst axis fracture. 4 Nonburst fractures are best treated nonsurgically because most of these fractures are more or less stable by nature. Burst fractures can be treated conservatively, but surgery is indicated in the presence of marked C2–C3 dislocation, associated unstable hangman fracture, or neurologic compromise. 3 , 5 , 6 , 7 Surgery could be anterior C2–C3 fusion, 5 posterior fusion, 6 or combined anterior then posterior fusion. 8
We present six cases of combined burst axis fractures and traumatic spondylolisthesis with one odontoid fracture that were managed with single-stage anterior fixation fusion and three treated conservatively. This study is a retrospective analysis of burst C2 cases to answer the following questions: Could anterior surgery first preserve C1–C2 motion? Can it be enough for these complex fractures? Does conservative treatment have a role in the management?
Materials and Methods
After obtaining Institutional Review Board approval, this retrospective comparative study was performed. Among 452 cases with upper cervical spine injuries, only 9 patients with burst C2 fractures between 1996 and 2012 were identified. They all had associated atypical traumatic spondylolisthesis of the axis (caused by bilateral articular facets fracture), 9 with one case having an additional Anderson and D'Alonzo type III odontoid fracture. The patient demographics and fracture information are shown in Table 1.
Patient demographics and fractures
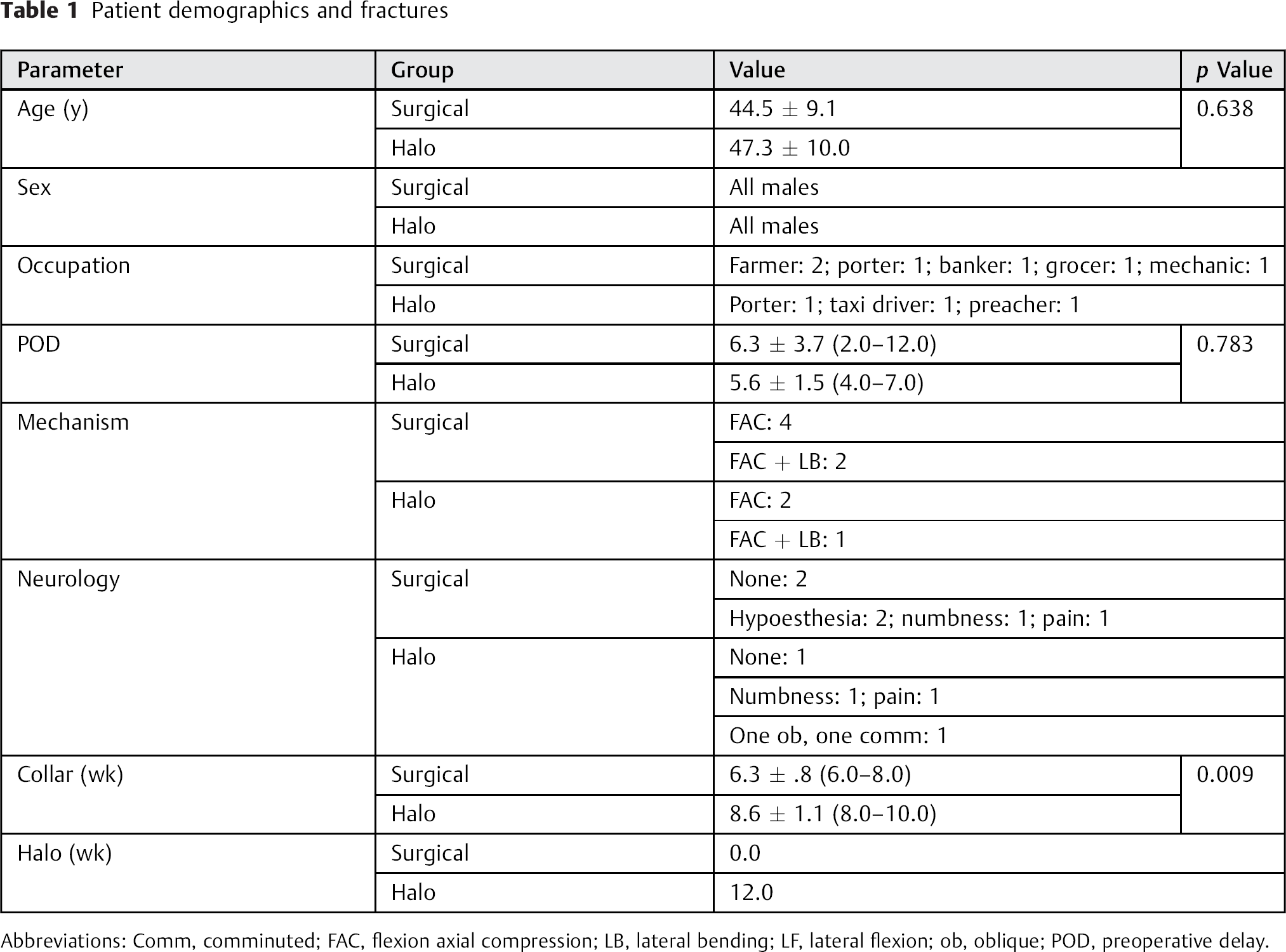
Abbreviations: Comm, comminuted; FAC, flexion axial compression; LB, lateral bending; LF, lateral flexion; ob, oblique; POD, preoperative delay.
The indications for surgery included: (1) neurologic deficit, (2) failure to achieve or maintain reduction nonoperatively, and (3) patients refusing halo traction or halo vest. Contraindications to surgery included complete cord transection, known allergy to metals, severe osteoporosis, and concomitant spinal infection. The algorithm of decision making is shown in Fig. 1.
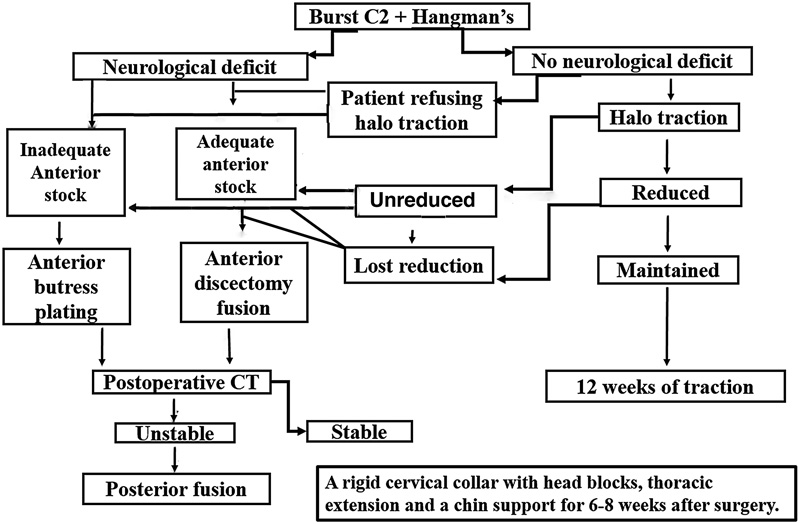
The decision-making algorithm used in our cases. Abbreviation: CT, computed tomography.
Proper reduction criteria were: Roy-Camille's four criteria (anterior translation ≤2 mm; local angulation ≤5 degrees 10 ; obliteration of the fracture site of the facets on computed tomography [CT] scans; restoration of the normal height of C2–C3 disk), and anteroposterior compression ratio < 0.6 on CT scans.
Surgical Group
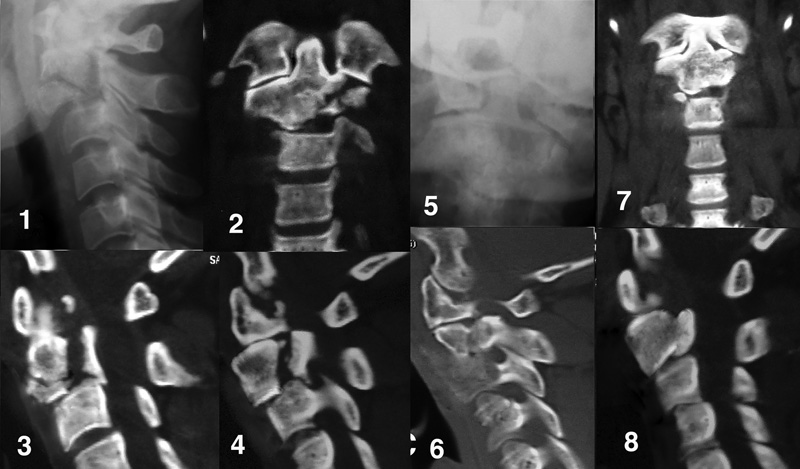
Four cases were managed by anterior diskectomy fusion with iliac autograft and anterior C2–C3 plating under fluoroscopic control on a radiolucent orthopedic table (Fig. 2).
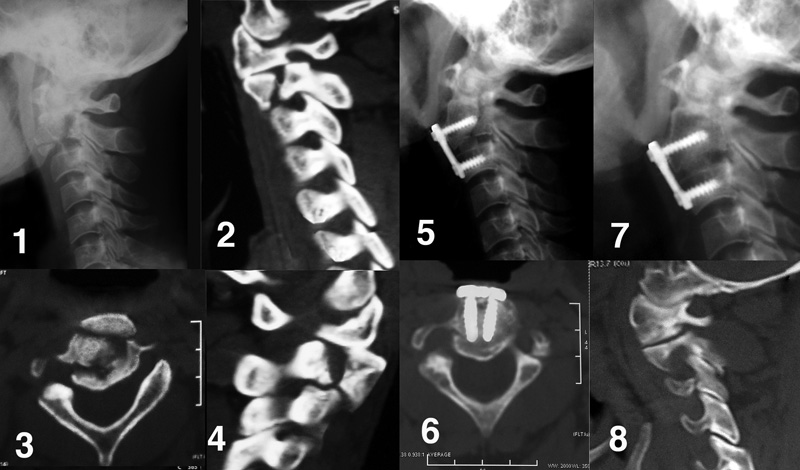
Preoperative radiology: (1) Lateral X-ray showing a three-part fracture. (2 and 4) Sagittal computed tomography (CT) showing fracture of both C1–C2 facet joints. (3) Axial CT showing the comminuted nature of the fracture. Postoperative radiology: (5) Lateral X-ray 3 days after surgery showing reduction, iliac bone graft in place, and fixation with four-screw anterior diskectomy fusion. (7) Lateral X-ray at 6 months showing union and solid C2–C3 fusion. (6) Axial CT showing union and correction of anteroposterior compression ratio. (8) Sagittal CT showing union of articular fracture.
The two cases with severe comminution of the body and articular facets were managed by anterior buttress plating. A 2-mm K-wire was inserted into the odontoid (verified under image intensifier) and the plate was then applied with the K-wire passing through its middle slot. The plate position was then adjusted, and the plate was fixed to C3 with two drill bits inserted to a depth of 10 mm through the screw holes. The C3 drill-bit placement was checked with image intensification with coronal alignment additionally checked with a portable X-ray if the fluoroscopy image was not clear enough to interpret. The K-wire helped to manipulate the odontoid-bearing fragment so that the wire passed through the center of the slot. The C3 screws were then fully inserted followed by the middle screw, which was an oblique cancellous screw directed from anteroinferior to posterosuperior. In one of these cases, the plate was precut to remove the upper screw holes and keep the middle slot (Fig. 3).
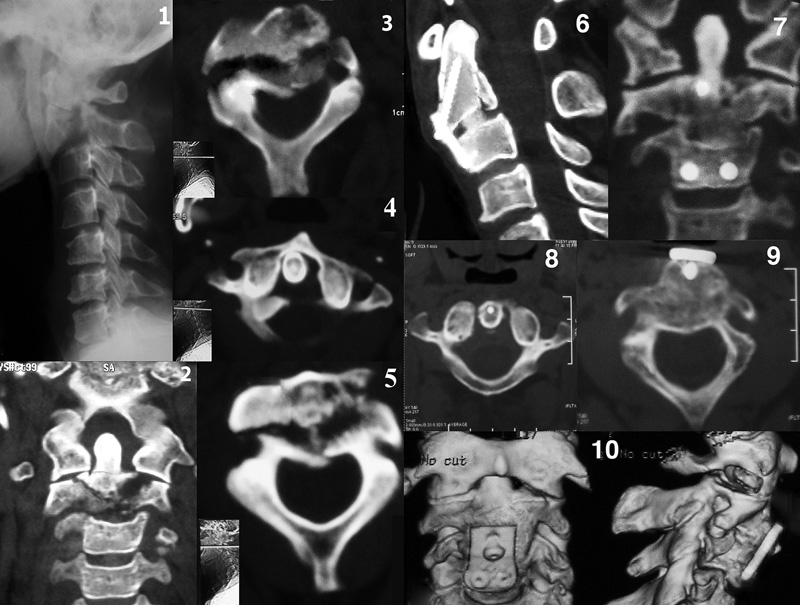
Preoperative radiology: (1) Lateral X-rays showing axis and base of odontoid fractures. (2) Coronal computed tomography (CT) showing comminuted left facet and oblique right facet fractures. (3 and 5) Axial CT showing fracture through articular facets and axis body. (4) Axial cut showing evidence of C1–C2 rotatory subluxation. Postoperative radiology: (6) Sagittal CT after 4 months showing union of axis and odontoid. (7) Coronal cut showing incongruity of left facet joint and progressing fusion of C2–C3. Axial cut showing (8) correction of rotatory subluxation and (9) healing of body fragments. (10) Multislice CT cuts 1 year postoperatively showing solid union and split incongruity of left facet joint.
We used a short screw in the case without an associated odontoid fracture and a long screw in the case with odontoid fracture to purchase the base of odontoid above the fracture line.
The surgery was done in all cases under halo traction. The anterior longitudinal ligament was torn in two cases and was intact in four. Manipulation of the neck was done to reduce the fracture before surgery while the patient was awake. No neuromonitoring was used during surgery.
Halo Group
Three patients were put on halo traction or halo vest for 12 weeks and reduction was judged with CT scans. A rigid cervical collar was then applied until union was achieved.
Postoperative Care and Follow-Up
Patients in the surgery group were admitted for 2 to 5 days, and the stitches were removed on the day 10. Patients in the halo group were hospitalized for 12 weeks on halo traction. Before discharge, all patients were instructed to wear a rigid cervical collar with head blocks, a thoracic extension, and a chin support till radiologic union.
The postoperative radiologic workup included plain X-rays (anteroposterior, lateral, open-mouth views) and CT scans (coronal, axial, sagittal, and three-dimensional) after surgery or traction as well as after 6 weeks to check for union, maintenance of reduction, and any evidence of hardware failure and to measure canal compression ratio. Reduction was judged by Roy-Camille's four criteria and improvement of canal compression ratio. 10 When these five criteria were met, the reduction was graded excellent; when four were met, it was graded very good; when three criteria were met, it was graded good; when only two criteria was met, it was graded fair; and when one criterion only was met, it was graded poor. The clinical results were graded according to pain, limitation of motion, and ability to return to previous work without restrictions. Results were ranked as excellent when the patient had no pain or limitation of motion and the patient was able return to previous work without limitation; very good when one of these three criteria was absent; good when two were absent; and poor when all three were absent. Pain was scaled according to visual analog scale (VAS) from 1 to 10. Range of motion was measured clinically using a geniometer. Work quality was graded into three grades: 0, normal unlimited; I, unlimited but with painkillers; II, reduced working hours. All patients were followed clinically and radiologically for a minimum of 48 months.
Results
Surgery Group
In the surgery group, reduction was difficult in one case with a short neck. Reduction was judged to be excellent in all but two case where incongruency of one articular facet fracture was present; the result was graded good in one and very good in one. One had comminution of right C1–C2 facet joint with resulting incongruency of the articular facet without osteoarthritic changes, which was manifested by 10-degree painful loss of rotation to the right side and by 10-degree loss of lateral flexion. The patient graded pain as 3 of 10 on the VAS, and his pain was evident with prolonged stationary position of the head, such as when watching TV for long periods; the pain was relieved with simple analgesics or the application of hot packs to the side of his neck. The other case had comminution of left C1–C2 facet joint with osteoarthritic changes and had 10-degree painless loss of rotation to the left side (VAS score of 2). One patient (with too-prominent plate) had occasional mild dysphagia that did not warrant plate removal.
We had no infection, metal failure, or loss of reduction. Four patients had excellent clinical results and the two with painful limitation had good result. All six patients returned to their previous work (grade 0) except one who used occasional pain killers (grade 1). The anteroposterior compression ratio, anterior translation, and local angulation were all improved after surgery, and the neurologic status returned back to normal in the affected patients (Table 2).
Comparative results
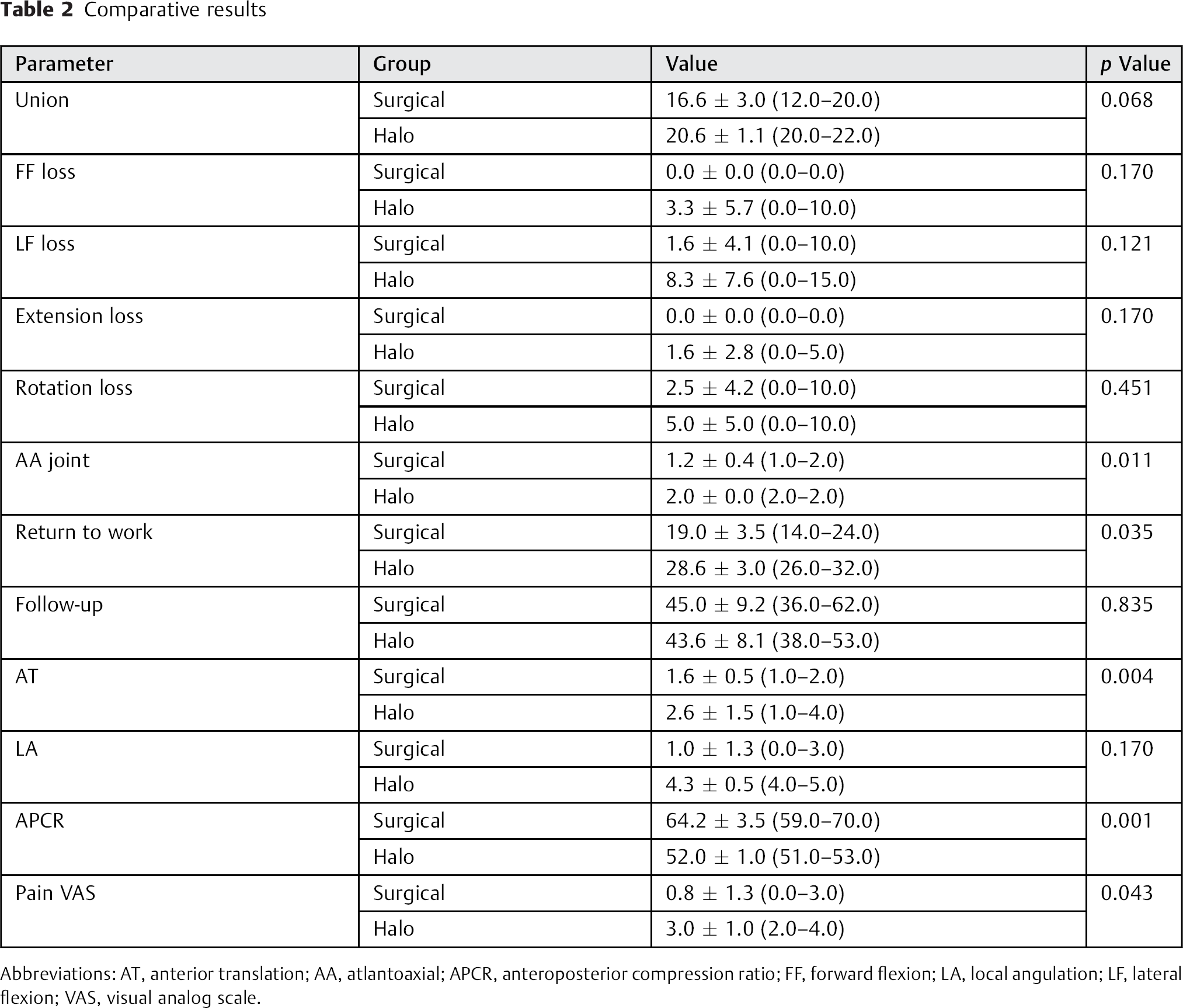
Abbreviations: AT, anterior translation; AA, atlantoaxial; APCR, anteroposterior compression ratio; FF, forward flexion; LA, local angulation; LF, lateral flexion; VAS, visual analog scale.
Halo Group
In the halo group, reduction was judged to be good in one case with uncomminuted articular facet fragments. The other two cases had both poor reduction and clinical outcome. The two cases had painful limitation of motion that affected their jobs (one grade I, and one grade II). All three patients returned to their jobs later than subjects in the surgery group. The two who had articular facets incongruency with pain developed osteoarthritis at 2 to 3 years.
The final clinical and radiologic results are shown in Table 2. The radiologic summaries of two surgical cases and one conservative case are shown in Figs. 2, 3, and 4.
Before conservative treatment: (1) Lateral X-ray showing a three-part fracture. (2) Coronal computed tomography (CT) showing comminuted left facet. (3 and 4) Sagittal CT showing fracture through articular facets and axis body. After conservative treatment: (5) Open-mouth view showing incongruent depressed left facet fragments with uncorrected rotary subluxation. (6) Coronal CT showing same picture with nonfused C2–C3 disk and persistent rotary subluxation. (7) Axial cut showing fused but incongruent articular facet fracture. (8) Sagittal cut showing healing of body fragments but with persistent anterior translation of C2 over C3, nonfused C2–C3 disk and reduced disk height.
Discussion
Fractures of the axis fall into three types: odontoid fractures, traumatic spondylolisthesis, and body fractures. The reports of axis body fractures are sparse. Hadley et al described 47 cases but did not describe their morphology. 11 Three of the patients died, 43 were managed in halo vest or collar, and 1 had early surgery due to marked C2–C3 subluxation. Greene et al reported 67 fractures involving the body or lateral mass with no mention of their morphology. 1 One patient died and another one was managed with early surgical fusion for a lateral mass fracture associated with 5-mm subluxation of C2–C3. The remaining 61 patients were nonoperatively managed with external immobilization for 7 to 17 weeks. Craig and Hodgson reported nine fractures involving the superior articular facet with seven associated odontoid fractures; the authors advised posterior atlantoaxial fusion for displaced fractures to prevent malunion, nonunion, and late arthritis. 12 Bohay et al reported three cases as a variant of spondylolisthesis treated conservatively. 13 Jakim and Sweet reported one case of transverse fracture of the body treated conservatively. 14 Korres et al described 14 avulsion fractures of the axis, one chance fracture, and nine cases of spondylolisthesis combined with odontoid fractures. 15 , 16 , 17 All the patients were treated conservatively with satisfactory results. Burke reported 31 cases of C2 body fractures. 18
Fujimura et al classified axis body fractures into four types: avulsion, transverse, burst, and sagittal fractures. This classification was determined using the anteroposterior and lateral views of the upper cervical spine, tomograms, or CT. 3 Fujimura et al defined burst fracture as a comminuted fracture of the axis body with multiple fragments dislocated anteroposteriorly. The authors identified three cases of this type, and all were associated with a hangman fracture. 3 Fujimura et al treated two of them with C2–C3 anterior decompression and fusion and one conservatively. Benzel et al classified C2 body fractures according to fracture line orientation on CT into coronal, sagittal, and horizontal rostral and defined burst fracture as a sagittally oriented fracture. 2
We found the Benzel et al classification rather confusing as all three types can be multifragmentary (morphologically burst) and because fractures can be a combination of any the three types in one patient. 19 We adopted the classification and definition of Fujimura et al, as it is the best description of the word burst.
There is no consensus about the definition of hangman fractures. Some define it as bilateral pars-interarticularis fracture, 18 with or without C2–C3 displacement. 6 , 18 Most authors adopt the definition of Schneider et al 20 (fracture of lamina, articular facets, pedicles, or pars). 9 , 21 , 22 According to the definition given by Schneider et al and the Effendi classification, our cases were all type II or III atypical hangman fracture. The odontoid fracture in one of our cases was Anderson and D'Alonzo type III odontoid fracture.
Benzel et al reported that despite different mechanisms of injury, the imaging findings are surprisingly similar. 2 We found that the reported mechanism in our patients conforms to fracture morphology, especially with bursting of one facet where the mechanism included lateral and forward flexion and axial compression.
It seems there is a general consensus that isolated nonburst fractures of the body of axis are best treated nonsurgically because of the absence of neural canal compromise in most of reported cases and because most of these fractures are more or less stable by nature. However, surgery is appropriate for marked C2–C3 dislocation and the presence of neurologic compromise. 3
Burst fractures associated with spondylolisthesis or odontoid fractures are difficult to reduce or keep reduced with traction, and therefore surgery seems to be the most appropriate choice. 3 Gleizes et al studied combined cervical spine injuries including 31 upper cervical injuries that came in combination and reported that both fractures can be treated separately but in some cases, the ideal treatment is made difficult or impossible, and the combination has to be treated as a whole. 23 Injuries that require surgery are Anderson-D'Alonzo type II and some type III dens fractures, type II and III traumatic spondylolisthesis of the axis according to Levine and Edwards, bilateral or unilateral facet dislocation and fracture-dislocation, lateral mass separation fracture, and comminuted burst fracture of the vertebral body.
The available options for type III hangman fractures are either posterior (transpedicular screws, 7 C2–C3 fusion, or even C1–C3 fusion 5 , 6 ) or anterior diskectomy fusion or combined anterior-posterior fusion. 8 Pedicle screw fixation is not on the table as an option simply because the bone stock anterior to the pedicles is not good enough to hold the screws and because biomechanical studies proved that pedicle screws are inferior in flexion and extension to both posterior and anterior fusion. 24 Posterior fusion, on the other hand, obviously cannot correct the burst C2 component or anterior instability. Additionally, biomechanical tests proved that posterior fusion is better than anterior fusion in lateral bending and axial rotation only, but both are equal in flexion–extension (which is the major destabilizing factor). 24 C1–C3 fusion is better than all other fixation methods but at the price of permanently sacrificing C1–C3 motion. 25 These biomechanical studies were performed only on type I and II hangman fractures. No biomechanical data on type III or burst C2 is available in the literature, maybe because of the rarity of these injuries.
Our cases were neither isolated burst fractures (except one) nor isolated hangman fractures. If they were isolated burst fractures, they would have been treated conservatively with success as happened in one case in the conservative group that had a good clinical outcome. The burst fractures were combined with atypical hangman fractures occurring through the articular facets, unlike the typical ones occurring through the pedicles. The combination is essentially two components of the same injury. We decided to treat them surgically to address the dangerous unstable hangman component.
Conservative treatment can achieve union, which happened in our three cases, and even can achieve good reduction, which occurred in one case. The problem with conservative treatment is malunion with marked incongruence of articular facets resulting in pain and osteoarthritis leading to work limitation in mildly as well as severely comminuted fractures involving the pars. We believe that poor reduction in two cases contributed to poor outcome, but the patients refused surgery to achieve or maintain good reduction and accepted the risk of osteoarthritis. Conservative treatment took longer to heal, required longer hospitalization, and allowed return to work later than the surgery group.
Our main concern was to preserve C1–C2 motion even with some limitation, so we approached the cases with a policy to “go anterior first, you may not need to go posterior later.” We decided to perform anterior diskectomy fusion, which proved successful in managing unstable traumatic spondylolisthesis (as reported by Ying et al 26 and Hadley et al 11 ), check for postoperative stability according to Roy-Camille criteria, and perform second-stage posterior C2–C3 fusion if necessary. Fortunately, postoperative reduction was good enough to negate the second procedure. Xie et al used a similar approach for unstable hangman fractures by starting with anterior fusion then performing posterior pedicle screws in the same session for cases with residual displacement. 8 However, posterior screws were needed in only 16 of 45 cases.
When we found a C2 inferior and anterior body fragment big enough to hold two screws, we performed a formal anterior diskectomy fusion. In severely comminuted cases, the bone in the inferior C2 body was not adequate enough to hold two screws, so we used buttress plating with three-screw configuration.
In the case with the fracture extending into the odontoid base, if we had used a partially threaded screw, it would have collapsed the comminuted segment between the odontoid and body, and so we used a fully threaded screw.
There is only one biomechanical study on single-screw fixation comparing single- and bilevel fusion in flexion–extension, lateral bending, and axial rotation in five situations: (1) intact cervical spine; (2) injury (diskectomy); (3) with interbody spacer; (4) in-line one-screw plate + spacer; and (5) two-screw plate + spacer, using four plate brands. 27 The study concluded that a two-screw plate does not appear to provide a biomechanical benefit over a one-screw plate.
This study has several limitations: the small number of cases makes it difficult to draw solid conclusions; patients were young with big bone fragments and good bone quality suitable for screw purchase, which might not be the case in elderly patients; it is not a prospective randomized study; and except for VAS, clinical outcome measures were not validated.
Plate prominence at this level might cause dysphagia, which can be avoided by using precut plates, as we did in one case, or by the use of precontoured plates.
We contribute the incongruence and limitation of motion to the nature of the trauma, with severe comminution of the pertinent facet.
Starting with posterior fusion, another anterior session might be needed to deal with anterior instability. Starting with anterior fusion will correct the anterior instability, which may prove enough to abandon posterior fusion and preserve the C1–C2 motion. Conservative treatment can be utilized in osteoporotic C2 with gross comminution and in isolated burst fractures. However, the ideal management is yet to evolve. Further research and better fixation techniques are needed to obtain better results with these difficult fractures.
Disclosures
Yasser Assaghir: none