
Abstract
Study Design:
Retrospective review.
Objectives:
This study investigates the prevalence of adverse postsurgical events, or osteoporosis-related complications (ORCs), following spinal fusion.
Methods:
Patients undergoing primary posterior thoracolumbar or lumbar fusion by 1 of 2 surgeons practicing at a single institution were analyzed from 2007 to 2014. ORCs were defined in one of the following categories: revision surgery, compression fracture, proximal junctional kyphosis, pseudarthrosis, or failure of instrumentation. Patients with a bone mineral density of the hips and/or spine performed within 1 year of the index procedure were included. Patients were stratified into normal bone density, osteopenia, and osteoporosis using WHO guidelines. Patients were excluded if they were younger than 18 years at the time of surgery, with infection, malignancy, skeletal dysplasia, neuromuscular disorders, concomitant or staged anterior-posterior procedure, or fusion performed because of trauma.
Results:
Out of 140 patients included, the prevalence of normal bone density was 31.4% (44/140), osteopenia 58.6% (82/140), and osteoporosis 10.0% (14/140). There were no differences between groups for gender, age, body mass index, and interbody device rate. The overall prevalence of ORCs was 32.1% (45/140). By group, there was a prevalence of 22.7% (10/44), 32.9% (27/82), and 50.0% (7/14) for normal bone density, osteopenia, and osteoporosis, respectively. These differences were significantly higher for both the osteopenia and osteoporosis groups.
Conclusions:
Patients with T scores below −1.0 undergoing posterior lumbar fusion have an increased prevalence of ORCs. Consideration of bone density plays a crucial role in patient selection, medical management, and counseling patient expectations.
Keywords
Introduction
In an aging population, osteopenia and osteoporosis have become an increasingly common condition and so too has the concern from spinal surgeons. 1 The concern for achieving adequate fixation and fusion is often part of the treating physician’s treatment algorithm. Many adverse outcomes have previously been associated with osteopenia, even catastrophic failure. 2
Advances in medical management of osteopenia have allowed for several changes in surgical and nonsurgical treatment algorithms of spinal pathologies. The development of bisphosphonates, 3 anabolic agents for bone synthesis, 4 biologics and bone substitutes, 5,6 and the widespread recognition and treatment of vitamin D deficiency 7 have made spinal fusion an option where previously it may have been inadvisable.
The purpose of this study was to analyze adverse outcomes with regard to bone density. Although the challenges are not unique to spinal surgery, there are often unique risks associated with poor bone density. The selection criteria for ORCs was based on several variables that have been shown to have an association with osteopenia, including compression fractures, 8,9 proximal junctional kyphosis (PJK), 8,10 instrumentation failure, 2,8 and pseudarthrosis. 11
Methods
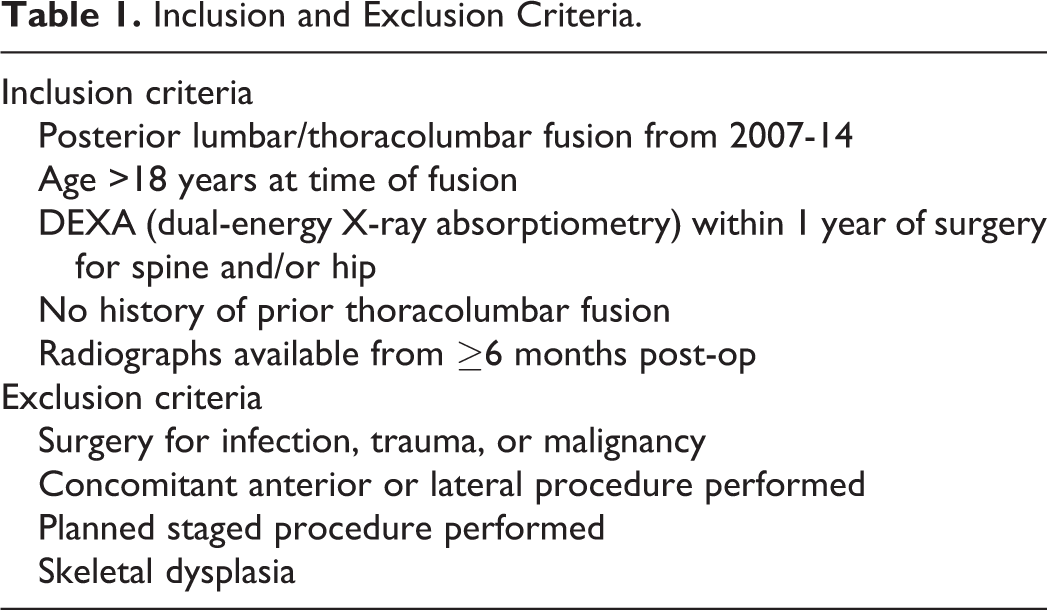
Consecutive patients who underwent posterior thoracolumbar or lumbar spinal fusion from 2 surgeons practicing at a single institution were analyzed from 2007 to 2014. Inclusion criteria were as follows: isolated posterior thoracolumbar fusion without planned staged operation, older than 18 years at the time of surgery, dual-energy X-ray absorptiometry (DEXA) of the spine and/or hip performed within 1 year of the index operation, no prior history of thoracolumbar fusion, and availability of follow-up digital radiographs at least 6 months following surgery. Patients were excluded as follows: surgery performed for or as a sequela of infection, trauma, or malignancy, concomitant or staged anterior or lateral procedure, or for a diagnosis of skeletal dysplasia. All study criteria are summarized in Table 1.
Inclusion and Exclusion Criteria.
Using World Health Organization (WHO) guidelines, 12 the lowest T score was analyzed; patients with a lowest T score less than −2.5 were designated to have osteoporosis, those with a lowest T-score greater than −1.0 were designated as having normal bone density. All remaining patients were designated as having osteopenia.
Determination of Osteoporosis-Related Complications
The latest postoperative radiographs and cans were used in comparison to preoperative radiographs. New compression fractures within 2 levels of the existing fusion mass were documented by a decrease in anterior column height.
PJK was defined as a proximal junctional angle (PJA) more than 10° and a change in PJA of more than 10°. PJA is defined as the sagittal Cobb angle between the inferior endplate of the upper instrumented vertebra and the superior endplate of the vertebra 2 levels above.
Instrumentation failure was defined for this study as broken or dissociated arthrodesis components, or pullout of greater than 5 mm. Screw loosening was evaluated, but not included in the final analysis.
Pseudarthrosis as determined by the latest dynamic radiographs and computed tomography (CT) scan. 13 Since static radiographs have proven to have low sensitivity, 14 we did not include suspected pseudarthroses as measured by static radiographs alone. The lack of bridging bone on fine cut CT scan 15,16 was used as the gold standard. When CT was unavailable, the difference on flexion-extension radiographs of more than 5° for each fused level was used to define a pseudarthrosis. 17 When disagreement existed between the radiograph and CT measurement, we deferred to the CT scan, which has proven to be more reliable. 18
Only one ORC was documented per patient; if greater than one ORC was listed per patient, the most detrimental event was listed at the authors’ discretion.
Statistical Methods
All statistical analysis was performed by a biostatistician using JMP (SAS, Cary, NC). For categorical variables, a Pearson’s chi-square test was performed; for continuous variables, we used the nonparametric Kruskal-Wallis test. For all tests, we used α = 0.05 and β = 0.20 to represent statistical significance.
Results
After application of all inclusion and exclusion criteria, 140 patients were included for final analysis. Patients were grouped into normal bone density (NBD), osteopenia (OPe), and osteoporosis (OP). Further analysis was performed comparing groups OP and OPe to NBD. The prevalence of NBD, OPe, and OP were 31.4%, 58.6%, and 10.0%, respectively as seen in Figure 1.
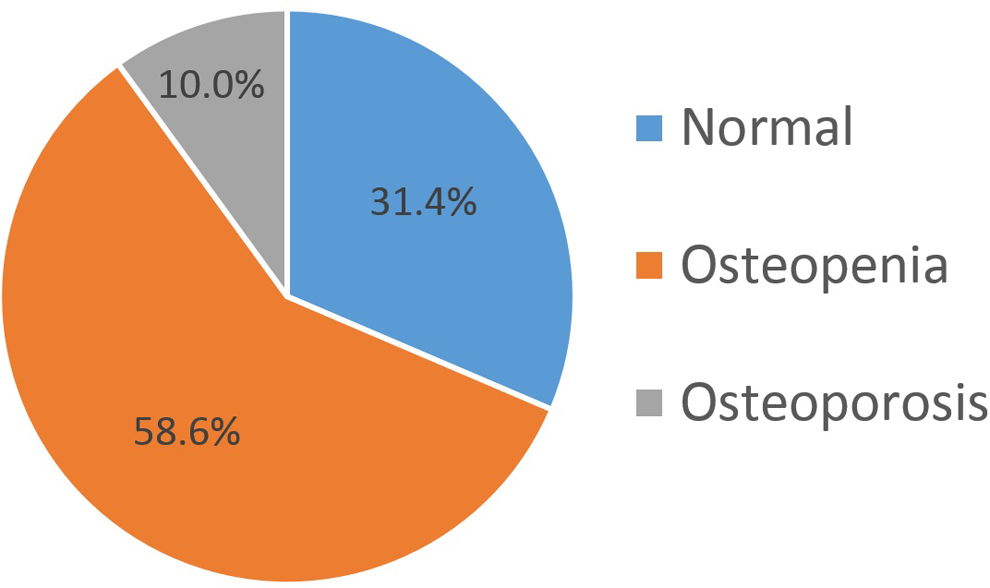
Patients by bone density prevalence.
Demographics are listed in Table 2. There were differences among groups for gender, age, body mass index, instrumented fusion rate, and interbody device rate. There were no differences among groups for number of levels fused, surgeon, or time to follow-up.
Patient Demographics by Bone Density.
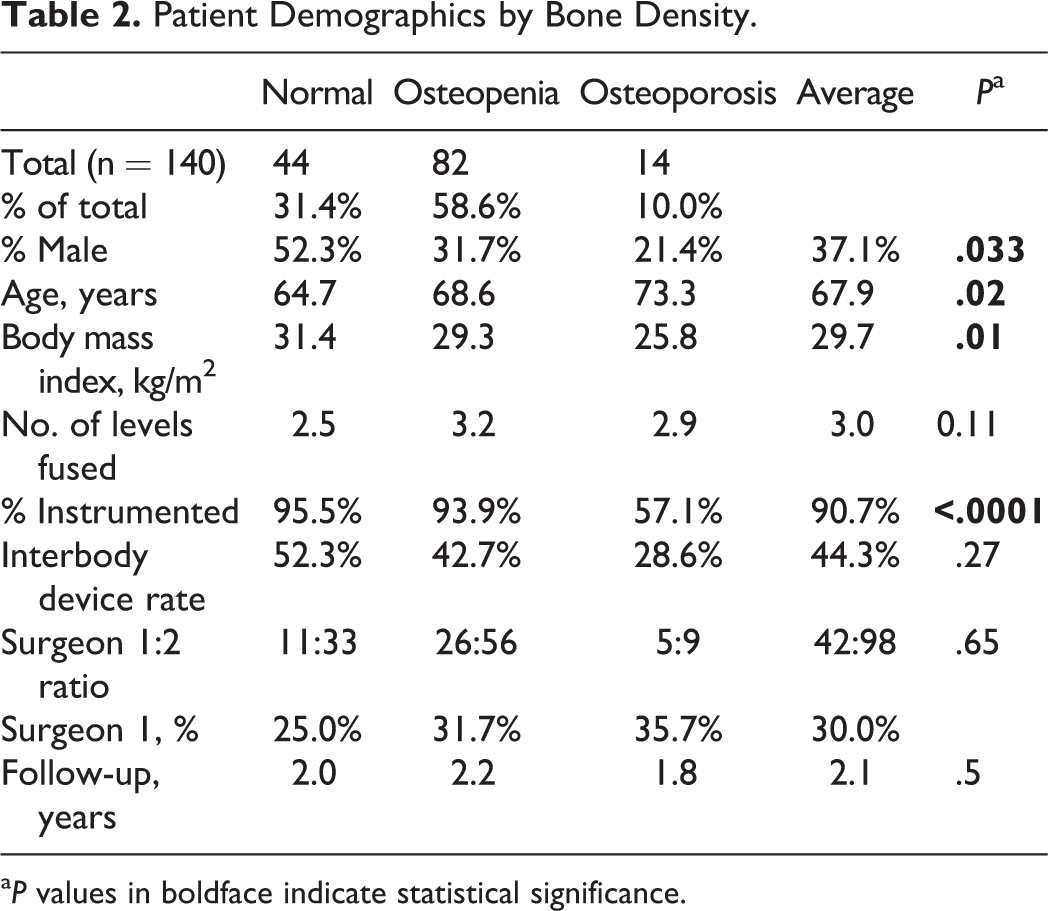
a P values in boldface indicate statistical significance.
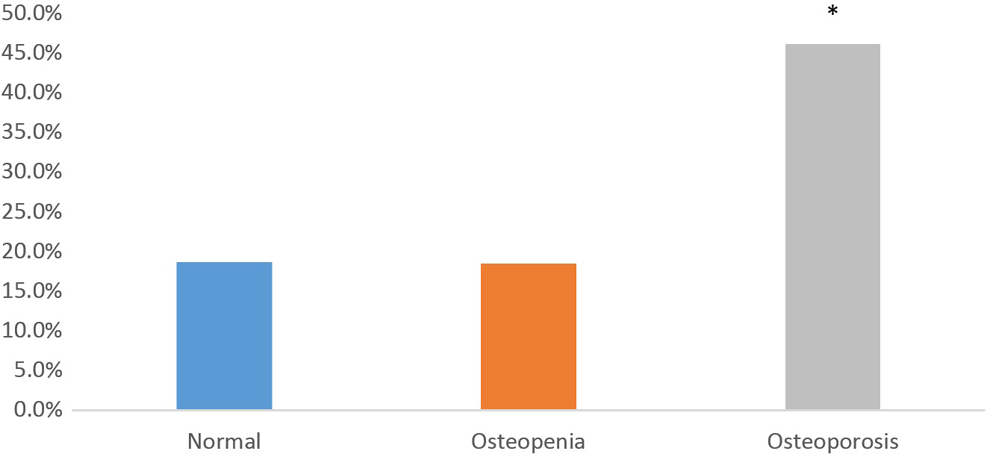
The overall prevalence of ORCs was 32.1% (45/140). By group, there was a prevalence of 22.7% (10/44), 32.9% (27/82), and 50.0% (7/14) for NBD, OPe, and OP, respectively, as seen in Figure 2. There was a significantly greater prevalence in the OP and OPe groups (P = .009).
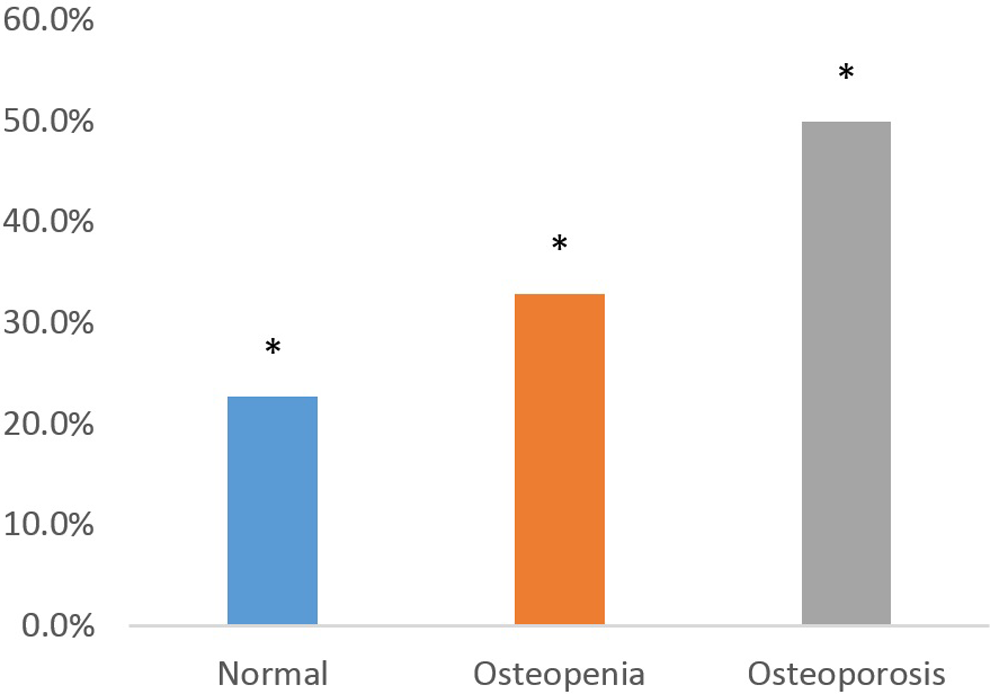
Osteoporosis-related complication (ORC) prevalence for all bone density groups.
All ORCs are listed by type and bone density group in Table 3.
Osteoporosis-Related Complications (ORCs) by Type and Bone Density.
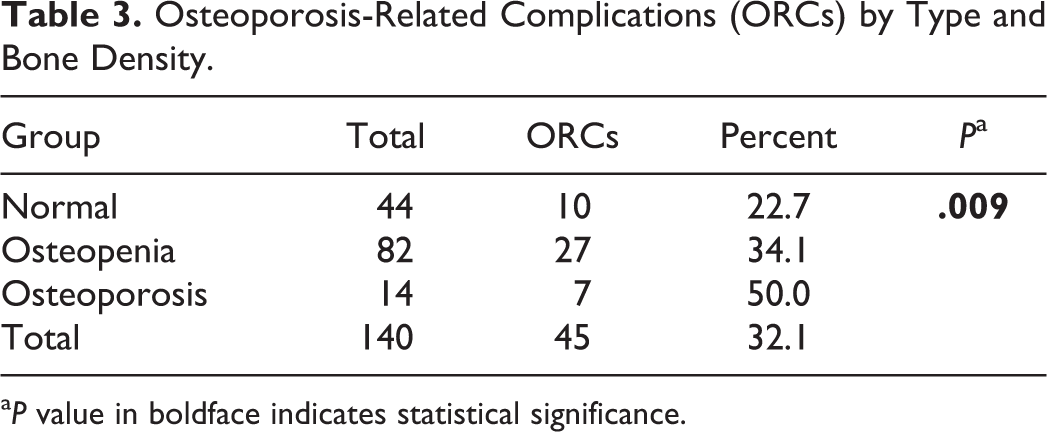
a P value in boldface indicates statistical significance.
All static radiographs were reviewed, but not for spinal fusion assessment (radiographic assessment of fusion with static radiographs has been historically difficult to quantify, and this is discussed later). Postsurgical CT scans were available for 57.1% (80/140) of patients for assessment of fusion, 37.1% (52/140) patients were analyzed by flexion/extension radiographs alone, and 5.7% (8/140) patients did not have dynamic radiographs or a CT scan by which union could be determined. Of the remaining patients, the overall prevalence of pseudarthrosis was 21.2% (28/132). By group, there was a prevalence of 18.6% (8/43), 18.4% (14/38), and 46.2% (6/13) for NBD, OPe, and OP, respectively as seen in Figure 3 and Table 4. There was a significant difference for nonunion in the OP group when compared with the other 2 groups (P = .016).
Nonunion rate by bone density group at latest follow-up.
Nonunion Rate as Determined by Computed Tomography (CT) or Dynamic Radiographs.
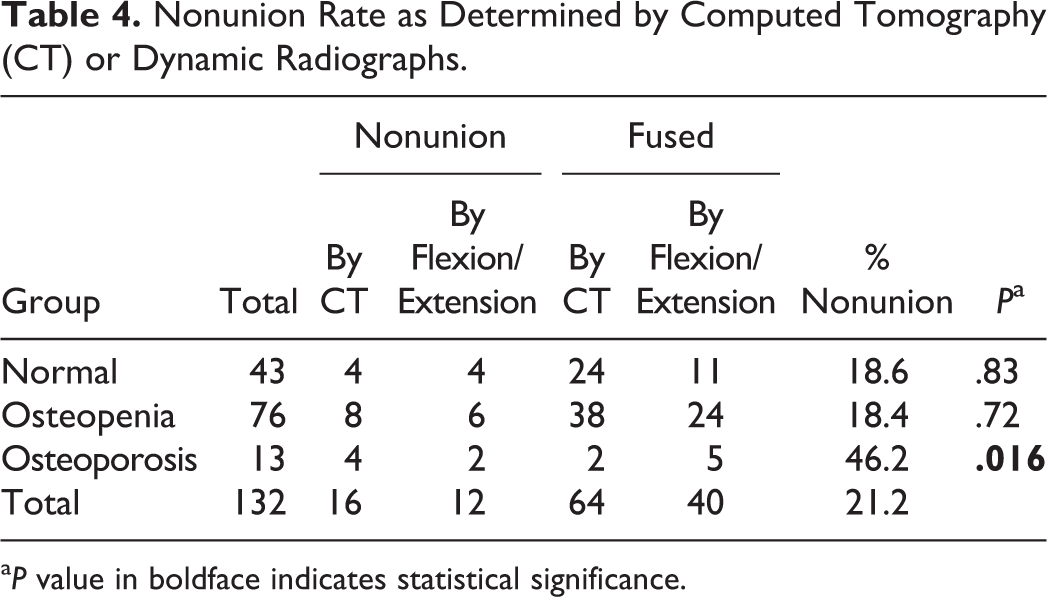
a P value in boldface indicates statistical significance.
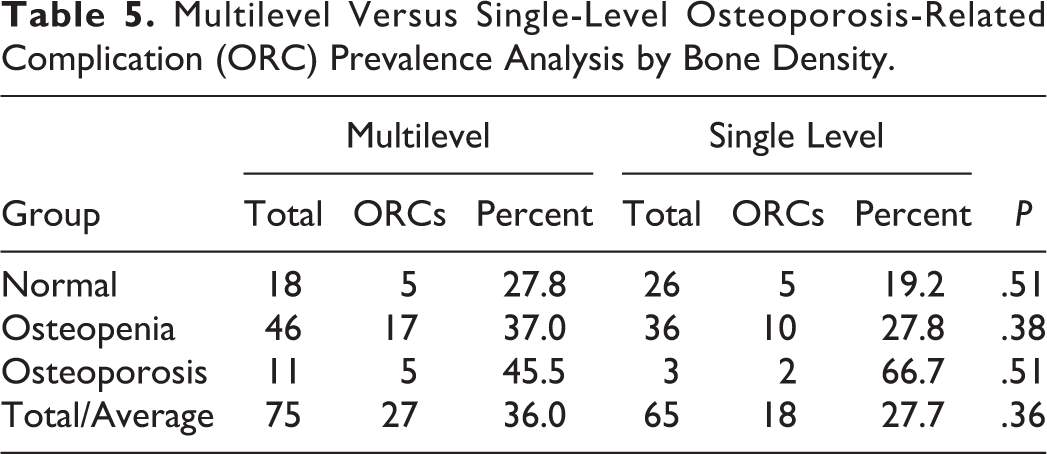
A “multilevel fusion” was defined as more than one level of the spine being fused (eg, L2 to L4). Multilevel fusions were analyzed separately in Figure 4 and Table 5. We found neither a significant difference in the prevalence of ORCs for any group nor an overall difference in single level versus multilevel fusions for all patients.
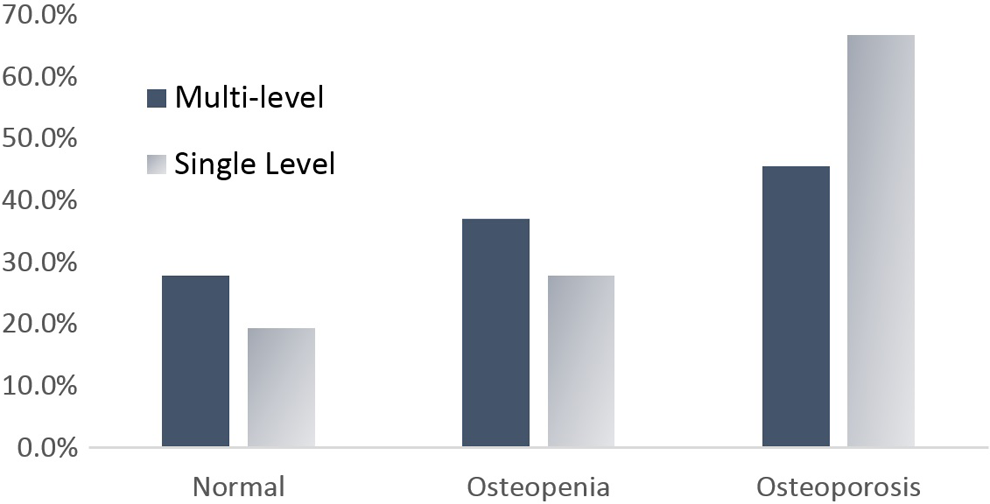
Osteoporosis-related complication (ORC) prevalence by bone density for single-level and multilevel operations.
Multilevel Versus Single-Level Osteoporosis-Related Complication (ORC) Prevalence Analysis by Bone Density.
Discussion
The role of bone density has become increasingly recognized as an important aspect of spinal fusion. Although prior studies have demonstrated several adverse outcomes associated with low bone density in isolation, 1,2,8,19,20 this study represents a different approach in studying a number of ORCs in aggregate. We believe that this approach allows the treating spine surgeon to have a better appreciation for the impact of poor bone density. The design of this study also included subtle postsurgical changes, which may otherwise be overlooked in a larger series.
This study is not without limitations. The retrospective nature may inherently limit the conclusions that can be drawn from the results. Although several of the patients included in this study were treated with medical therapy for low bone density, those variables were not accounted for in the final analysis. The type, duration, compliance, and documented improvements from medical therapy present far too many variables to control for this study. Furthermore, the accuracy of documentation in a retrospective study adds additional complexity to the study. During initial data collection this information was collected, but was eventually deemed too complex and variable to be meaningful for the study. Other studies have documented the effects of medical therapy on bone density and spine surgery, and we did not focus on that. For this reason, we used DEXA within a year to be a proxy for all variables (including any medical therapies) that contributed to bone density. All DEXA scans were performed within 1 year of the index procedure; however, interim pharmaceutical therapy may have affected bone density at the time of surgery.
There may be some inherent limitations in using DEXA as a measurement of bone density, especially in patients with preexisting degenerative disease of the spine. Subchondral sclerosis, bone spurring, and effects from arthrosis may lead to a falsely elevated DEXA value. There has been evidence that there are many limitations to bone densitometry, and there may be a discrepancy between T scores and actual bone density. 21 –23 Alternative methods of bone density are available and may be more accurate. 24 –26 For the purpose of this study, DEXA is readily available and is a more widely recognized standard of measurement.
PJK has become a well-recognized entity following longer fusions, particularly into the thoracic spine. The most commonly applied measurement for PJA is sagittal Cobb angle between the inferior endplate of the upper instrumented vertebra and the superior endplate of the vertebra 2 levels above. 27 –33 PJK is most commonly defined as a change in PJA of greater than 10° compared with preoperative measurement, although some suggest that a value of 15° 34 or 20° 35 may be more clinically meaningful. The presence of PJK was assessed for all patients using change in PJA greater than 10° compared with preoperative measurement, the most commonly cited value. Kyphosis in the lumbar spine would be far more problematic than a similar measurement in the thoracic spine. Of the 10 patients included in this analysis determined to have PJK, the lowest upper instrumented vertebra was T11. The inclusion of PJK as an ORC may be inherently limiting in scope, as it more commonly applies to fusions that extend to the thoracic spine (ie, long multilevel fusions) and a confounder in the final analysis. Nonetheless, since it is becoming an increasingly recognized complication, we felt that it was important to apply to all fusions, regardless of fusion location.
The assessment of pseudarthrosis always presents a challenge for any study evaluating the outcome of spinal fusion. While spinal arthrodesis has been shown to be an effective treatment for degenerative spondylolisthesis, 36,37 successful outcomes have not been shown to correlate with radiographic evidence of fusion. 38,39
To complicate matters further, radiographic assessment of fusion has been historically difficult to quantify. CT is seen as the modern gold standard for radiographic evaluation of fusion, 16,40 with modern fine-cut imaging, multiplanar reconstruction, and metal artifact reconstruction. 13 Previous classifications that rely on static 39,41 radiographs alone have been shown to be unreliable when compared to open pseudarthrosis inspection, 42 whereas CT scans have been shown to have a positive predictive value of 96% following open pseudarthrosis inspection. 42 The inherent confounding effect of this measurement is that a CT scan is not a standard part of postsurgical imaging. Because a CT scan is costly and comes with a substantial amount of radiation, it is likely more often ordered only for persistent problems or when a pseudarthrosis is suspected. Therefore, relying on CT scans on this subset of patients may overestimate the prevalence of pseudarthrosis for the entire cohort.
Dynamic radiographs have been shown to have better predictive value for arthrodesis than static radiographs 43 ; however, there is some disagreement on the amount of motion between flexion/extension radiographs that indicates a nonunion, from 1° to 5°. 15,17,44,45 We found that most studies use a difference of flexion-extension radiographs of 5° or more to be diagnostic of a pseudarthrosis, including the Food and Drug Administration in a successful premarket approval application for an interbody fusion device. 46 Therefore, in cases where CT scan was unavailable or equivocal, we used a threshold of 5° of motion for each level between flexion and extension radiographs. Because flexion-extension radiographs are a more standard postsurgical imaging modality, it is less likely that patients without this imaging modality represent a different cohort, unlike CT scans as discussed above.
We assessed screw loosening for this study, including pedicle screw back-out 47 and halo phenomenon. 48 There is considerable heterogeneity in this area of research, and definition of loosening depends largely on the classification utilized. 49 However, screw halo phenomenon has been shown in one study 48 to not have a correlation with bone mineral density, and in isolation may have little clinical significance. Furthermore, any gross loosening and pull-out of screws with loss of fixation was included in patients with true instrumentation failure. For this reason, screw loosening alone was not included in the final analysis of ORCs.
We performed a separate analysis of single level versus multilevel procedures. Neither did we note a greater prevalence of ORCs for any group nor did we note a difference in all single level versus multilevel procedures. There was a trend (36.0% vs 27.7%) for more ORCs in the multilevel group; however, this was not statistically significant (P = .36). While more extensive fusion operations may have a significantly higher complication rate (with the variables studied here), those complications seem not to be compounded by a low bone density.
This study design was intended to isolate complications related only to bone density. However, because low bone density may be a harbinger for advanced age or poor health, there is an inherent confounding effect of the independent variable for this study. Of the variables we included in the study, all except one were purely radiographic: reoperation. Reoperation for ORC is multifactorial, and involves decision making from both the surgeon and patient, both of which are related to age and health status. However, these cases and medical records were all investigated and evaluated separately in an effort to isolate the impetus for re-operation as related to an ORC.
This study does not include patient outcomes. Patient-reported outcomes were available for some, but not all patients included in this study. This is an admitted weakness in this study, and should be included in any future or prospective study on this subject.
One possible confounder in this study is that a significantly greater proportion of patients with osteoporosis had uninstrumented fusions (42.9% of OP patients vs 5.6% of Normal and OPe groups, P < .0001). It is possible that this led to a greater prevalence of pseudarthrosis, as noninstrumented fusions have been demonstrated to lead to a lower fusion rate, 38 or 45% versus 82%. The OP group had roughly 5 more noninstrumented fusions than would be expected when compared with the normal and OPe groups (8/14 noninstrumented fusions, 13.2/14 expected noninstrumented fusions). This likely led to an additional 2 or 3 additional pseudarthroses in the OP group. To test whether this effect is responsible for the significance of the study, we performed 2 additional statistical challenges: removing 3 pseudarthroses from the OP group, and removing all pseudarthroses from the final analysis. In both cases, the significance relationship of ORCs and low bone density remained (P = .05 and .03, respectively).
As previously mentioned, there have been many advances in medical management, 3,4 biologics and bone substitutes, 5,6 and recognition and treatment of vitamin D deficiency. 7 Although medical records were reviewed to exclude some diagnoses, we did not include an analysis of medical therapies or other treatments aimed at low bone density. Investigating the effects of these treatments may be useful for future study in this area.
For the spinal surgeon, fusion is part of a treatment algorithm for degenerative scoliosis. In a study from Transfeldt et al, 50 short- or long-segment fusion for the treatment of degenerative scoliosis did not improve overall satisfaction, while resulting in a 4- to 5-fold increase in complications when compared with decompression alone. For patients in this cohort with low bone density, the effects may be compounded. Therefore, it may be prudent to consider bone density for any treatment algorithm that includes both fusion and nonfusion procedures. Based on the results from our experience, a fusion procedure may be less predictable in patients with a lowest T score less than −1.0.
Bone density has become more widely recognized as a concern in spinal surgery. 1 For these patients, it is important for the treating surgeon to understand nonsurgical treatment and education, consistent with “Own the Bone” initiative from the American Orthopaedic Association. 51
Conclusion
Although the overall prevalence of osteoporosis with this series was low (10%), there were few differences between the groups with osteopenia and those with osteoporosis. These results may suggest that a more conservative treatment algorithm where bone T-score is less than −1.0 warrant consideration for medical therapy or alternatives to spinal fusion.
For the spinal surgeons, referral and coordination with primary care providers or endocrinologists has become an important part of caring for patients with and at risk for low bone density. Based on our experience, we would urge surgeons to recognize that there is in increased prevalence of complications in patients with low bone density and treat accordingly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study received full Institutional Review Board approval from Mayo Clinic prior to initiation.