
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To analyze the impact of performing a formal decompression in patients with adult lumbar scoliosis with symptomatic spinal stenosis on perioperative complications and long-term outcomes.
Methods:
Adult patients undergoing at least 5 levels of fusion to the sacrum with iliac fixation from 2002 to 2008 who had a minimum 5-year follow-up at one institution were studied. Patients who had 3-column osteotomy were excluded from the study. Perioperative complications and clinical outcomes (Scoliosis Research Society [SRS], Oswestry Disability Index [ODI], and Numerical Rating Scale [NRS] back/leg pain) were analyzed. Patients who underwent formal laminectomy/decompressions were compared with those who did not. Differences between the 2 groups were analyzed using Student’s t test.
Results:
A total of 147 patients were included in the study (Decompression: n = 55 [37%], No decompression: n = 92 [63%]). Average fusion levels for the decompression and no decompression groups were 11 and 12 levels, respectively (P = .26). Mean improvements in SRS domains for decompression versus no decompression patients, respectively, were pain (1.1 vs 0.9, P = .3), function (0.7 vs 0.5, P = .09), self-image (1.1 vs 1.1, P = .9), and mental health (0.5 vs 0.4, P = .5). Furthermore, additional mean improvements were ODI (21 vs 21, P = .14), NRS-Back pain (3.0 vs 1.3, P = .16), and NRS-Leg pain (3.9 vs 0.5, P = .002). Complication rates between the decompression group and no decompression group differed in incidental durotomies (18.2% vs 0%) and cardiac-related (9.1% vs 1.1%).
Conclusions:
Performing a formal decompression in adult lumbar scoliosis with symptomatic spinal stenosis is associated with increased perioperative complications but favorable long-term clinical outcomes.
Introduction
Symptomatic spinal stenosis in patients with adult lumbar scoliosis with degenerative changes is not uncommon, especially in the elderly population. 1 -3 In addition to back pain, many patients may present with incapacitating leg pain from spinal stenosis. A substantial number of adult scoliosis patients with concomitant radiographic lumbar stenosis often do not suffer from such debilitating radiculopathy. 2 The subset of patients with scoliosis and mild to moderate but not incapacitating leg pain presents the greatest treatment challenges. In these patients, the treating surgeon must weigh the risks and benefits of doing a decompression. Decompression in this patient population is not trivial, as the pathology typically resides in the concavity of the curve where there may be limited working room, severe compressive pathology, and the presence of a dural deficiency, which may lead to longer surgical times and more blood loss. These factors may lead to higher complication rates.
This study was aimed at determining the impact of performing a formal decompression in patients with adult lumbar scoliosis with degenerative changes with symptomatic lumbar stenosis in comparison with those patients that did not undergo a decompression. We hypothesized that patients undergoing a formal decompression would have increased perioperative complications and will not achieve similar long-term functional outcome improvements to those not having decompression, based on Scoliosis Research Society (SRS), Oswestry Disability Index (ODI), and Numerical Rating Scale (NRS) back/leg pain scores. To our knowledge, this is the first study to address this question in adult scoliosis patients.
Materials and Methods
A retrospective analysis of prospectively collected data of adult patients (age >18 years) undergoing at least 5 levels of fusion to the sacrum with iliac fixation from January 2002 to December 2008 were included. Informed consent was obtained from the institutional research board. A minimum of 5-year follow-up was required to be included in the study. All surgeries were performed by 2 spinal deformity surgeons, at the same institution, who had 50 years combined surgical experience. Patients who underwent a decompression as part of a Ponte or Smith-Petersen osteotomy, pedicle subtraction osteotomy, or vertebral column resection were excluded from the study. Thus, this study only included those patients undergoing formal decompressions (without osteotomy) and those that did not. The indications for decompression was moderate to severe spinal stenosis associated with neurogenic claudication and unilateral or bilateral motor or sensory radiculopathy unresponsive to prior conservative management. A chart review was performed to obtain demographic data, operative data, and hospital course. Preoperative sagittal T5-T12 and T12-sacrum angle, TL coronal Cobb angle, and sagittal vertical axis were also collected on each patient. Preoperative and postoperative clinical outcome measures included SRS (1-5), ODI (0-100), and NRS back and leg pain (0-10) scores. Differences between the 2 patient groups were analyzed using Student’s t test. Correlations between preoperative sagittal and Cobb angles were determined by pairwise method. A P value of <.05 was considered statistically significant.
Surgical Technique for Decompression
All patients who underwent a decompression were positioned prone on an operating table. Decompression was typically performed following placement of pedicle screw instrumentation. In cases where pedicle anatomy was difficult, decompression was performed first to also allow palpation of pedicle prior to placement of screws. Care was taken to preserve some facet joint surface to allow for a surface area for fusion. In cases where an incidental durotomy was encountered, a primary suture repair was always attempted. If the dura was completely absent, the defect was covered with collagen matrix and fibrin glue of the surgeon’s choice and frequently a porcine pericardium xenograft was also sutured in place over the defect.
Results
A total of 147 patients were included in the study. Fifty-five (37%) patients underwent a decompression and 92 (63%) patients did not. Mean age and follow-up were 60 years and 74 months, respectively, for the decompression group and 55 years and 76 months for the group that did not undergo a decompression, respectively (P = .007 and P = .7). Average fusion levels for the decompression and no decompression groups were 11 and 12 levels, respectively (P = .26). The Charlson Comorbidity Index for the decompression and no decompression groups were 3.3 and 2.6, respectively (P = .006). Mean estimated blood loss (EBL), length of surgery, and length of hospital stay for the decompression group were 1408 mL, 7.7 hours, 9.6 days, respectively, compared with 1050 mL, 7.0 hours, 10 days, respectively, for the group that did not undergo decompression (P = .01, .03, and .4 for EBL, length of surgery and hospital stay, respectively; Table 1). There were no significant differences in preoperative sagittal T5-T12 angle (P = .017), TL coronal Cobb angle (P = .46), and sagittal vertical axis (P = .81) between both cohorts. However, there was significant difference in sagittal T12-sacrum angle (°), with the decompression cohort being lower than the no-compression cohort (Decompression: 36.04 ± 16.60 vs No Decompression: 42.46 ± 20.57, P = .04; Table 1). Mean improvement in SRS domains of pain, function, self-image, and mental health were 1.1, 0.7, 1.1, and 0.5 for the decompression group, respectively, compared with 0.9, 0.5, 1.1, and 0.4, respectively, for the group without a decompression (P = .3, .09, .9, and .5 for pain, function, self-image, and mental health, respectively). Mean improvement in ODI and NRS back and leg pain scores were 21, 3.0, and 3.9 for the decompression group, respectively, versus 16, 1.3, and 0.5, respectively, for the group without a decompression (P = .14, .16, .002 for ODI, NRS back, and NRS leg pain, respectively; Table 2). Within the decompression group, there were a total of 10 incidental durotomies, 5 cardiac complications, 1 deep vein thrombosis, 1 deep wound infection, and 3 systemic infections. There were no neurological deficits or deaths. In the group without a decompression, there were no incidental durotomies, 2 motor neurological deficits, 1 cardiac complication, 1 deep vein thrombosis, 2 wound infections, 1 respiratory failure, and 3 systemic infections. There were no deaths (Table 3). There was no significant correlation between EBL and sagittal T5-T12 angle (P = .90), sagittal T12-sacrum angle (P = .76), and preoperative sagittal vertical axis (P = .86; Table 4). However, there was a significant positive correlation between TL coronal Cobb angle and intraoperative EBL (coefficient = .2391, P = .0054; Table 4). There were no significant correlations between the angles and complication rate (Table 4).
Patient Demographics, Hospitalization Characterization, and Preoperative Sagittal and Cobb Angles.a
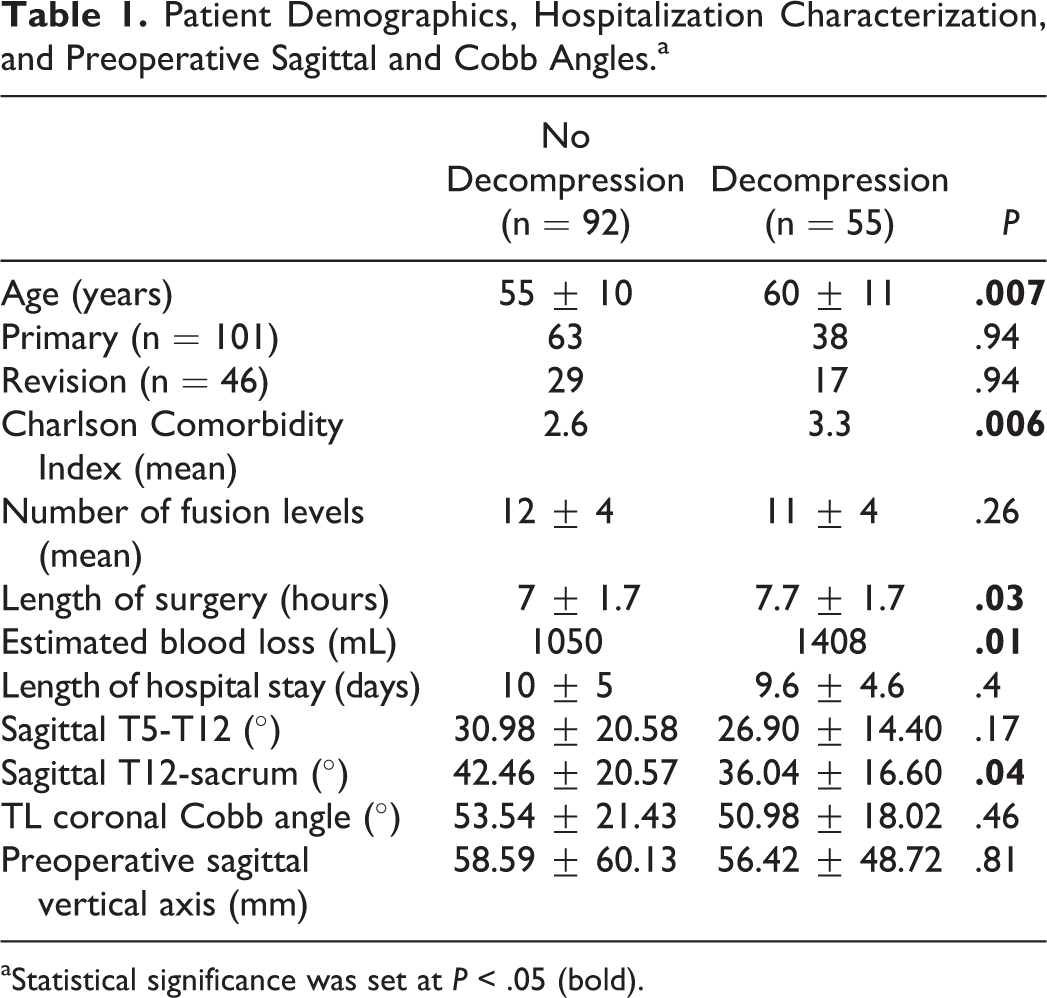
aStatistical significance was set at P < .05 (bold).
Patient-Reported Outcomes.a
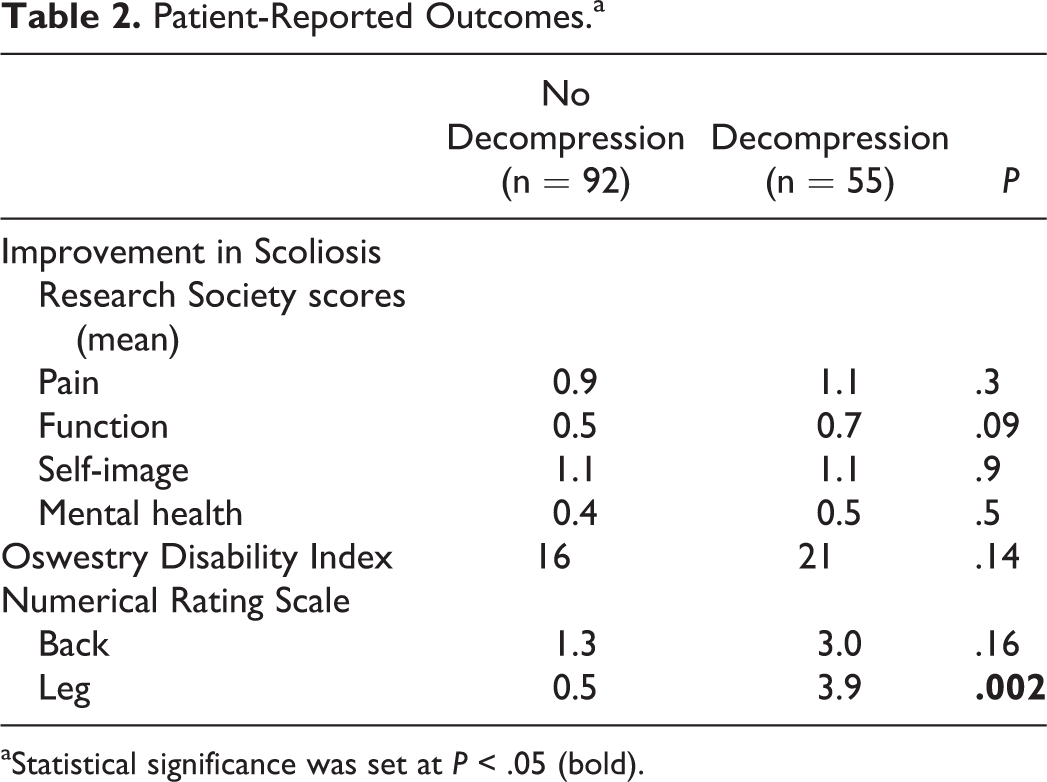
aStatistical significance was set at P < .05 (bold).
Complications.a
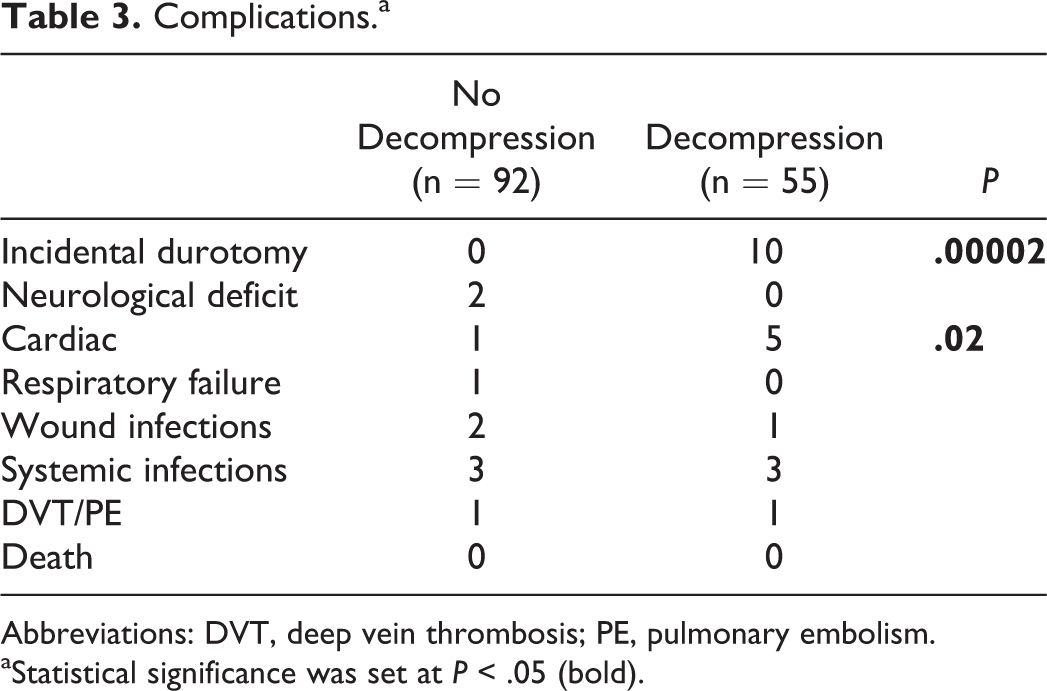
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
aStatistical significance was set at P < .05 (bold).
Correlation of Preoperative Sagittal and Cobb Angles With EBL and Rate of Complications.
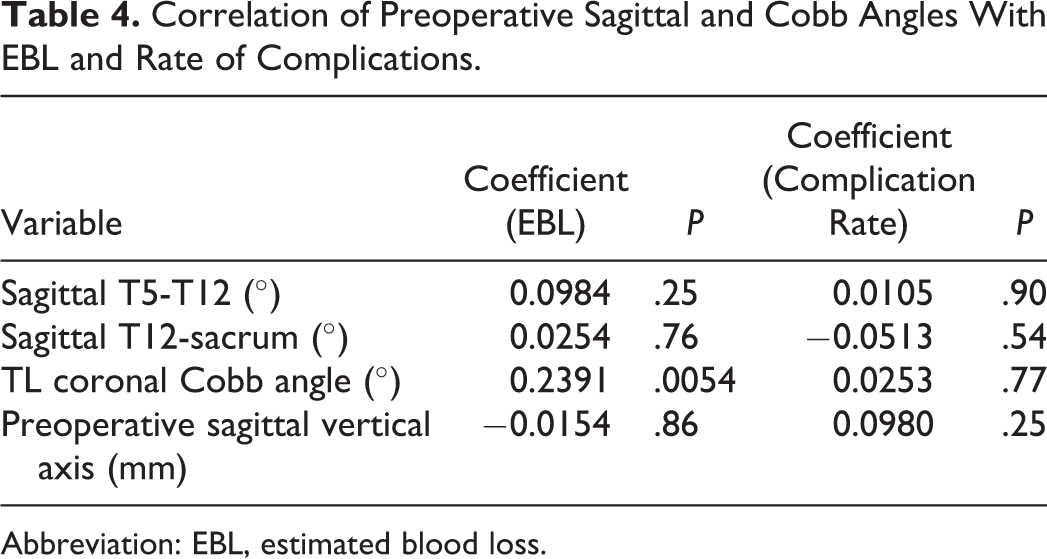
Abbreviation: EBL, estimated blood loss.
Discussion
The decision to perform a formal decompression in patients with adult lumbar scoliosis with degenerative changes undergoing complex multilevel fusions is a common dilemma in an adult deformity practice. Whereas lumbar decompression is not a technically demanding procedure in nondeformity cases, in patients with scoliosis it can be very challenging. In this subset of patients, the most stenotic and symptomatic areas often reside in the concavity of the curve, which inherently creates a difficult working corridor. A dural deficiency is a common finding in this region, resulting from chronic severe compression and osteophytic erosion into the apposed dural layer. 4 Thus, the occurrence of incidental durotomy is common and can pose difficult postoperative issues. 4,5 In patients with incapacitating pain attributed to lumbar stenosis, performing a thorough decompression is warranted, despite the aforementioned challenges that one may encounter. The patient should be counseled about the risks associated with decompression surgery prior to the operation. It is those patients with mild to moderate but tolerable leg pain who pose the significant treatment question. The treating surgeon must weigh the risks and benefits of performing a decompression in this patient subset.
The impact of incidental durotomies on patient-reported outcome (PROs) measures has been previously studied. 1,2,4 -7 In a prospective, multi-institutional propensity-matched analysis of 1741 patients undergoing lumbar spine fusion, Adogwa et al 8 reported no difference in postoperative complications and functional outcomes (ODI and NRS) up to 2 years after incidental durotomies in patients (n = 70) who sustained an incidental durotomy. Moreover, Lan et al 6 performed a retrospective analysis of 46 adult patients with lumbar degenerative scoliosis with stenosis who were treated with decompression and fusion. In their study, 13 patients (28%) had a cerebrospinal fluid leak and at a mean follow-up of 36.2 months reported significant improvement in ODI, NRS, and Japanese Orthopaedic Association scores. Our study similarly found an 18% prevalence of incidental durotomies and an overall improvement in SRS, ODI, and NRS scores. Our follow-up is substantially longer (5 years) than these other studies (2 years). Therefore, our findings and the aforementioned studies suggest that the occurrence of incidental durotomies do not negatively affect PROs.
Although this is the first study to specifically address the perioperative complications and long-term outcomes in patients undergoing complex reconstructions with decompressions, there are some limitations that are worth mentioning. First, this study was not a randomized controlled study and thus cannot accurately answer whether or not a decompression is always warranted in patients with symptomatic lumbar stenosis with spinal deformity. Second, other than incidental durotomies, it is difficult to attribute the occurrence of any complication to performing a decompression. Despite these limitations, our findings that the long-term outcomes (mean 75.0 months) in patients who underwent decompressions, despite having higher complication rates, longer operative times, and more EBL, is informative and can be used to counsel patients preoperatively. Surgeons who are faced with such patients should be prepared for increased operating times, higher EBL, and a higher prevalence of incidental durotomies.
Conclusion
Performing a decompression in adult deformity surgery is associated with increased EBL, increased operative time, and higher incidence of cerebrospinal fluid leaks. However, despite this there is a significant improvement in NRS leg pain scores. The long-term PROs appear to be similar in both groups, namely, the group that had decompression and the group that did not.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.