
Abstract
Study Design
Case report.
Objective
Incidental durotomy (IDT) is a common complication of spinal surgery. The use of collagen matrix graft along with hydrogel dural sealant is a common method of IDT repair. With this method, there have been several reported cases of detrimental dural sealant expansion in the literature. One case study reported an expansion rate greater than 300%; many report neurologic damage. This article reports the clinical course of two patients who developed postoperative transcutaneous drainage of a gel-like substance after the use of a dural sealant, which is a previously unreported complication.
Methods
The clinical course and treatment outcome of two patients is presented.
Results
Both patients experienced postoperative transcutaneous drainage of a gel-like substance at the surgical site. Case one began draining this substance on postoperative day 14. This patient required no further intervention, and the drainage ended after 3 mL of a gel-like substance was expressed from his incision while in the clinic. Case two began draining the gel on postoperative day 16. This patient underwent two washout procedures and resolution of the drainage. No infection was ever detected.
Conclusions
To our knowledge, our patients are the first reported cases of transcutaneous drainage of expanded dural sealant. It is important to take into consideration the unexpected expansion of a dural sealant when using it for the repair of IDT.
Introduction
Despite meticulous attention to surgical technique, an incidental durotomy (IDT) is one of the most common complications of spinal surgery. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 This complication has led to innovative developments in materials and methods to assist surgeons in repairing these complications to avoid cerebrospinal fluid (CSF) leaks. Primary closure with polytetrafluoroethylene (PTFE) such as 7.0 GORE-TEX (L. Gore & Associates, Newark, Delaware, United States) has historically been the method of choice. 9 Other primary methods used to repair these defects are microdural staples, muscle and fat grafts, xenograft dural patches (e.g., bovine pericardium), and collagen matrix grafts. 9 To improve the repair, secondary augmentations are often utilized. 9 Two main categories are dural sealants and fibrin glues. 9 Numerous comparisons demonstrate that PTFE sutures along with secondary fibrin glue is significantly more effective than just sutures at reducing CSF leaks. 10 , 11 Success rates as high as 97.7% have been reported for preventing CSF leak using these methods. 8 Similarly, success rates of 93 to 95% have been reported with tight dural suture and fibrin glue. 12 , 13 A recent study looking at IDT repair, without the use of sutures, using DuraGen (Integra, Plainsboro, New Jersey, United States), a collagen matrix graft, combined with DuraSeal (Covidien, Mansfield, Massachusetts, United States), a dural sealant, reported a success rate of 95.7%. 14 Although this figure falls within the same range, this method is much more efficient than suturing. 14 Moreover, during dural suturing, pinholes are made, which may cause persistent CSF leakage. Suturing the dura whenever possible, with or without augmentation, remains the gold standard for IDT repairs.
There are concerns about the swelling properties of DuraSeal. DuraSeal's product insert is required by the U.S. Food and Drug Administration (FDA) to include the following statement: “DuraSeal can swell after application, it should not be used in areas where neural structures could be compressed, and no difference in the prevention of long-term CSF leakage has been demonstrated and standard diligence in wound closure should be performed when using this device.” 15 Based on FDA approval documents, when tested in phosphate-buffered solution, DuraSeal swells no more than 200%. 16 Based on instructions provided by the FDA, in vivo, “hydrogel may swell up to 50% of its size in any dimension.” 15 Through a search of the literature, we have found that the expansion properties of DuraSeal are not always predictable. 17 , 18 , 19 , 20 , 21 , 22 One study reports a 333% expansion after the use of a dural sealant. 21
The aim of this case series is to report a rare complication (hydrogel cutaneous fistula) of the use of a dural sealant.
Materials and Methods
This is a case series report (n = 2) of a previously unreported complication of the use of a dural sealant. In both cases, DuraSeal was used for the correction of IDT and led to transcutaneous drainage of clear gel-like substance. DuraSeal is FDA-approved for its use as an adjunct to sutured dural repair. 15 It is a resorbable synthetic hydrogel sealant that is composed of two solutions: a polyethylene glycol ester solution and a trilysine amine solution. 15 DuraSeal is provided in a syringe applicator that mixes both solutions as pressure is applied. 15 This application causes a crosslink between the two compounds forming the hydrogel sealant. 15
Both patients were born in Mexico and were of Spanish descent. These cases were performed by one surgeon (F.T.) in a single institution. Institutional Review Board approval was granted for this study.
Case Reports
Case One
A 19-year-old man presented to our clinic with intractable back and leg pain that failed to improve with standard conservative treatment. Imaging showed severe disk herniation at the L3–L4, L4–L5, and L5–S1 levels. A three-level microdiskectomy was conducted. Three weeks postoperatively, a transcutaneous CSF fistula was diagnosed due to an IDT not recognized intraoperatively. The draining fluid was positive for β2-transferrin. The patient was taken back to the operating room and the durotomy was closed with dural suturing (7.0 GORE-TEX), followed by a collagen matrix graft (1 cm by 1 cm) and dural sealant (5 mL). A four-layer closure was done to repair the incision (interrupted 0 Vicryl [Ethicon, Somerville, New Jersey, United States]; running 0 Vicryl, running 2.0 Vicryl, and running 3.0 nylon). A drain was placed and removed on postoperative day 3. The patient presented to the clinic on postoperative day 14 with mild wound dehiscence and transcutaneous drainage of a clear, gel-like material. The patient did not demonstrate any neurologic findings or signs of CSF leakage. Fig. 1 is an image obtained at time of presentation. Approximately 3 mL of a clear gel-like substance was expressed from a 3-mm fistula on the superior aspect of the incision. Samples of the expelled drainage were taken and sent for testing. The sample was negative for β2-transferrin, bacterial culture growth, Gram staining, and it demonstrated a low white blood count. No further intervention was necessary. By his next visit a week later, the drainage had stopped and the wound had healed. At 18 months’ postoperative follow-up, the patient was free of any symptoms and the incisions were well healed.

Cutaneous fistula with gel-like drainage.
Case Two
A 42-year-old man presented to our clinic with intractable low back and leg pain that failed to improve with standard conservative treatment. Imaging showed a left-sided disk herniation at the L5–S1 level. A single-level microdiskectomy was conducted. The operation was complicated by an IDT, which was repaired by dural suturing (7.0 GORE-TEX), followed by a collagen matrix graft (1 cm by 1 cm) and dural sealant (5 mL). A four-layer closure was done to repair the incision (interrupted 0 Vicryl; running 0 Vicryl, running 2.0 Vicryl, and running 3.0 nylon). A drain was placed and removed on postoperative day 3. The patient presented to the clinic on postoperative day 16 with mild wound dehiscence and transcutaneous drainage of a clear gel-like material. The patient did not demonstrate any neurologic abnormalities or signs of CSF leakage. Samples of the discharge were taken and sent for testing. The sample was negative for β2-transferrin, bacterial culture growth, Gram staining, and it demonstrated a low white blood count. The patient was taken back to the operating room for a washout. During the operation, no dural tear was found using Valsalva maneuver. Two weeks after the washout operation, the patient presented with recurrence of a similar clear gel-like drainage and small wound dehiscence. At this point, the patient consulted another spinal surgeon at a different institution. This surgeon conducted a second washout operation. The drainage stopped after this operation. At 18 months’ postoperative follow-up, the patient was free of any symptoms and the incisions were well healed. Because the second irrigation and debridement surgery was done in Mexico, there is no information on any analysis of surgical tissue or fluids that may have been performed. The patient did not need antibiotic treatment.
Discussion
The case reports we have presented are unique due to the transcutaneous discharge after the use of a dural sealant. There have been no previous reports of such complications. There were no neurologic symptoms or signs of CSF leakage associated with the drainage. Although the amount of gel expelled from the wound site was not measured, we estimate it to be ∼3 mL in both cases.
In both patients, a β2-transferrin electrophoresis test was done on the gel-like secretion, and the results were negative, concluding that the fluid was not CSF. Due to the similarity of this gel to the dural sealant used and the negative results for CSF, immune response, and infection, it is our impression that the discharge was due to the cutaneous fistula formation and drainage of the in vivo expansion of a dural sealant. Because the drainage in both cases was through the operative incision and not through the drain orifice, we also believe that using a drain did not contribute to this complication. Although the FDA-approved product information for DuraSeal reports an expansion up to 50%, 15 there have been multiple reports of inappropriate expansion of this hydrogel sealant. Through our search of the literature, we discovered six similar reported cases of DuraSeal expansion. The results of these reports are summarized in Table 1. Our study is the first one reporting a cutaneous fistula complication after the use of a collagen matrix graft along with dural sealant. Unlike other reported cases, the patients in this report did not present with neurologic symptoms. Kacher et al used computed tomography and magnetic resonance imaging to investigate the expansion properties of DuraSeal in two canines. They found that the hydrogel sealant had its maximal expansion between 3 days and 2 weeks. 23 They also report a complete absorption of the hydrogel and closure of the remaining void by ∼8 weeks after implantation. 23 The expansion properties of DuraSeal have also been reported to have protective effects when recombinant human bone morphogenetic protein type 2 is used in transforaminal lumbar interbody fusion (TLIF) surgeries. 24 Its use to seal off the annulotomy site and as a protective covering to the nerve root reduces the incidence of postoperative radiculitis from 20.4 to 5.4% (p = 0.047). 24
Reported cases of DuraSeal expansion
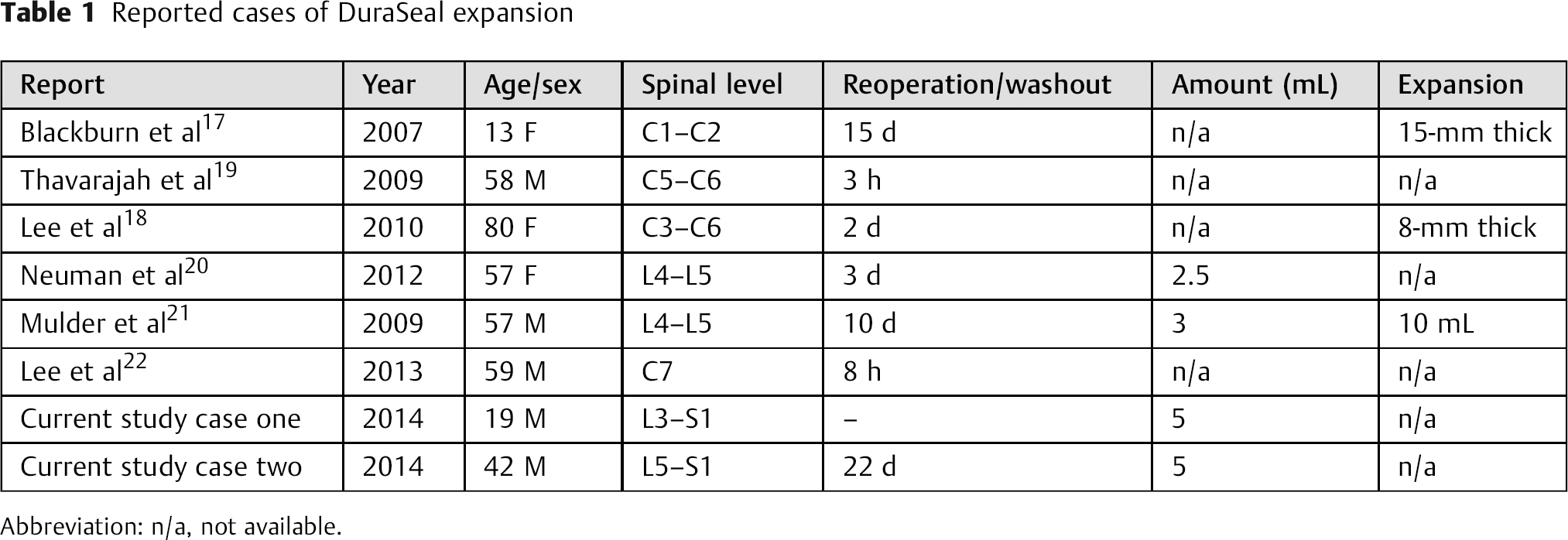
Abbreviation: n/a, not available.
We used 5 mL of a dural sealant for each spinal level, which seems to be higher than the other cases that we have cited in this report. Neuman et al use a maximum of 2 mL for each spinal level in their case of cauda equina after TLIF. 20 DuraSeal's FDA-approved instructions do not suggest an amount; instead, it recommends making a 1- to 2-mm coat and it permits immediate irrigation after application. 15
Conclusion
DuraSeal's expansion is properties are noted in its manufacturer's documentation, numerous case reports, and in vivo and in vitro studies. The amount of expansion, however, is not uniform among these sources. Complications such as neurologic compression and the now reported cutaneous fistula may arise from the material expansion. DuraSeal is effective in reducing postoperative CSF leakage and in most cases reduces surgical complications and operative time. We suggest applying DuraSeal conservatively and using caution with respect to volume and location to reduce possibility of symptomatic expansion. The hydrogel fistula was easily controlled in the two cases. Simple expression of the gel from the wound in the clinic resolved the first case, and a small irrigation and debridement, removing the hydrogel, concluded the second one.
Disclosures
Homayoun Siman, none
Fernando Techy, Consultancy: Amedica, Depuy-Synthes, Grafton; Royalties: Amedica; Educational presentations: Depuy-Synthes