
Abstract
Study Design:
Retrospective cohort study.
Objective:
To determine whether a low-density (LD) screw construct can achieve curve correction similar to a high-density (HD) construct in adolescent scoliosis.
Methods:
Patients treated operatively for idiopathic scoliosis between 2007 and 2011 were identified through a database review. A consistent LD screw construct was used. Radiographic assessment included percent correction of major and fractional lumbar curves, T5-T12 kyphosis, and angle of lowest instrumented vertebra (LIV). Costs were compared with HD constructs.
Results:
Thirty-five patients were included in the analysis. Ages ranged from 12 to 19 years (mean = 14.9 years). Average screw density was 1.2 screws per level (range = 1.07-1.5 screws). Mean percent curve correction at latest follow-up: major curve, 66.9%; fractional lumbar curve, 63%. Average postoperative thoracic kyphosis: 29.5°. Mean LIV angle: 5.6°. Average construct cost was $14 871 per case compared with $23 840 per case if all levels had been instrumented with 2 screws, amounting to an average savings of $9000.
Conclusions:
Our LD screw construct is among the lowest density constructs reported and achieves curve correction comparable to HD constructs at substantially lower cost.
Introduction
During the past decade, thoracic pedicle screw (TPS) instrumentation for adolescent idiopathic scoliosis (AIS) has gained popularity. 1,2 Many consider TPS constructs the standard of care for deformity correction. 3,4 Several previous studies have demonstrated the advantage of pedicle screws in absolute and percent of curve correction in scoliotic curves compared with hook and wire constructs. 5 –7 Other potential benefits of pedicle screw constructs include higher pullout strength, lower rate of implant failure, less long-term loss of correction, selective fusion, and lower pseudarthrosis rates. 8 –10
Bilateral placement of pedicle screws at every level has commonly been used, and the method provides maximal rigidity to the scoliosis construct; however, it is possible that fewer screws are adequate. Decreasing implant density has the advantage of decreasing operative time, risk of screw malposition, and cost. These advantages need to be weighed in relationship to the ability to obtain and maintain correction. The optimal implant density remains unknown. Previous studies have shown that screw density does not matter regarding curve correction. 11 –15
The present study was designed to evaluate a single surgeon’s experience with low-density (LD) screw constructs using a monaxial side-loading screw technique for scoliosis correction. The primary purpose was to define effectiveness of curve correction using this unique LD construct. Considering the climate of health care and the increased focus on the cost of health care, our secondary purpose was to analyze the cost of an LD construct compared with traditional high-density (HD) screw placement.
Materials and Methods
Patient Identification
After obtaining approval from the institutional review board, the records of consecutive patients from a single surgeon’s practice between 2007 and 2011 were evaluated. Patients were identified by retrospectively reviewing the surgeon’s operative database. Patients between the ages of 10 and 21 years with a diagnosis of AIS, a surgical procedure of posterior spinal fusion with TPS instrumentation, and a minimum of 2 years of follow-up were identified. All AIS patients during this timeframe were treated with an LD screw-rod construct (described below) independent of curve magnitude or flexibility, and no patients were treated with a HD construct.
Surgical Technique
A single surgeon at a single institution performed all surgeries using the surgical technique described as follows. After routine exposure of the levels to be fused out to the tips of the transverse processes, bilateral facetectomies were performed to increase the mobility of the curve. No Ponte or other osteotomies were used. Pedicle screws were placed with a freehand technique (Universal Spinal System [USS]; Depuy-Synthes, Raynham, MA). The USS uses side-opening monaxial screws, which permits direct reduction of each screw to the rod. No rod derotation maneuver is necessary. As determined by preoperative lateral bending films, all structural curves were generally included in the instrumentation construct. The proximal extent of the fusion was Cobb −1, and the distal extent of the instrumentation was either Cobb +1 or the vertebra bisected by the center sacral line on the standing preoperative radiograph, whichever was more proximal. Flexibility films were utilized to determine which curves would be considered structural, but not specifically for the determination of fusion levels. Bilateral pedicle screws were placed in the 2 vertebrae at the most proximal and distal ends of the construct. The transitional vertebra between 2 structural curves was also instrumented bilaterally. To control the apices of the instrumented curves, additional screws were placed at the convex apex of each curve. If the apex was a vertebra, 1 screw was utilized. If the apex was a disk, a screw was placed in the vertebra on either side of the disk. Finally, a screw was placed unilaterally on the concave side of the curve 1 level proximal and 1 level distal to the convex apical screws. Thus, a 3- or 4-screw cluster allowed for reduction of the apices of the instrumented curves in relation to the end vertebrae (Figure 1).
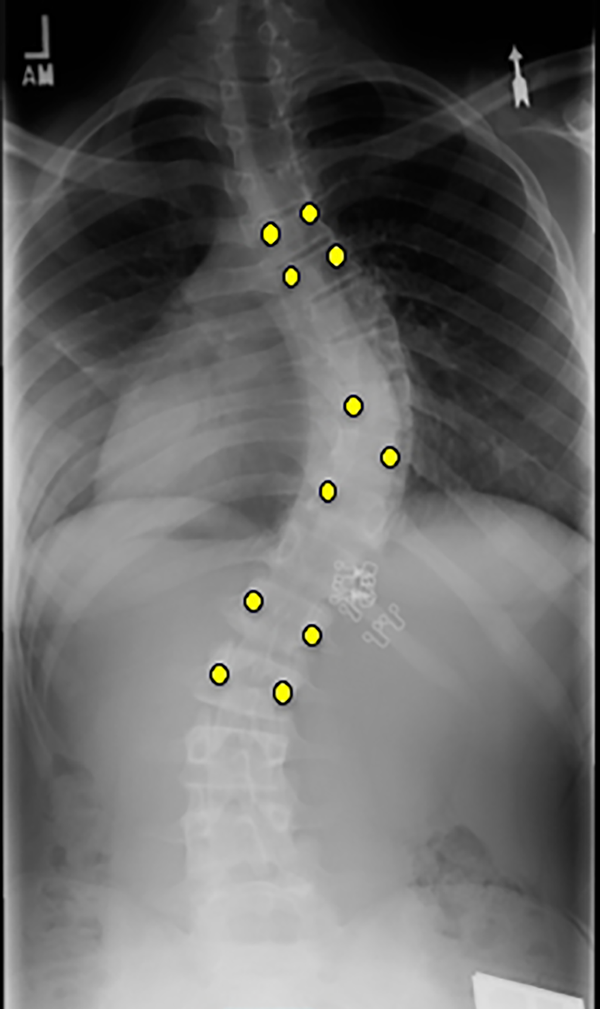
Radiographic representation of a typical instrumentation pattern for a single right thoracic curve.
The reduction sequence was as follows. After screw placement, 2 rods were contoured to physiological sagittal contour. The left rod was introduced into the distal 2 anchors and fixed in the correct sagittal orientation. Each of the left-sided screws was then reduced to the rod, working distal to proximal. The right-sided rod was inserted, beginning proximally and working distally, in similar fashion. Additional compression, distraction, and derotation of individual vertebrae were applied to enhance correction, but no rod derotation or in situ contouring was used.
After final tightening of the rod-screw connections, 2 cross-links were applied. The posterior elements were decorticated and bone graft inserted. Bone graft consisted of local bone harvested during the course of the procedure and crushed cancellous allograft. Patients were allowed to ambulate within 1 or 2 days after surgery. No brace was applied. Activity progressed as tolerated, but sports participation was restricted for 3 months postoperatively.
Radiographic Measurements
All radiographs were evaluated independently by 3 observers who were not involved in the patients’ care. Measurements were performed using Osirix software (Pixmeo, Geneva, Switzerland). Radiographic analyses were performed on 36-inch spine images (Figures 2 and 3). Screw density was calculated as the total number of screws used in the construct divided by the total number of levels fused. Coronal Cobb angles of the major and fractional lumbar curves were measured preoperatively and postoperatively. For patients with Lenke 5 and 6 curves, the thoracolumbar/lumbar curve was measured as the major curve and these patients were excluded from the fractional lumbar curve measurements. Sagittal alignment was assessed using standing lateral preoperative and postoperative radiographs and measuring the angle from the superior endplate of T5 to the inferior endplate of T12. Percent correction was determined by comparing preoperative and postoperative major Cobb angles. The postoperative angle of the lowest instrumented vertebra (LIV) was evaluated by measuring the angle of the inferior endplate of the LIV with the horizontal line.
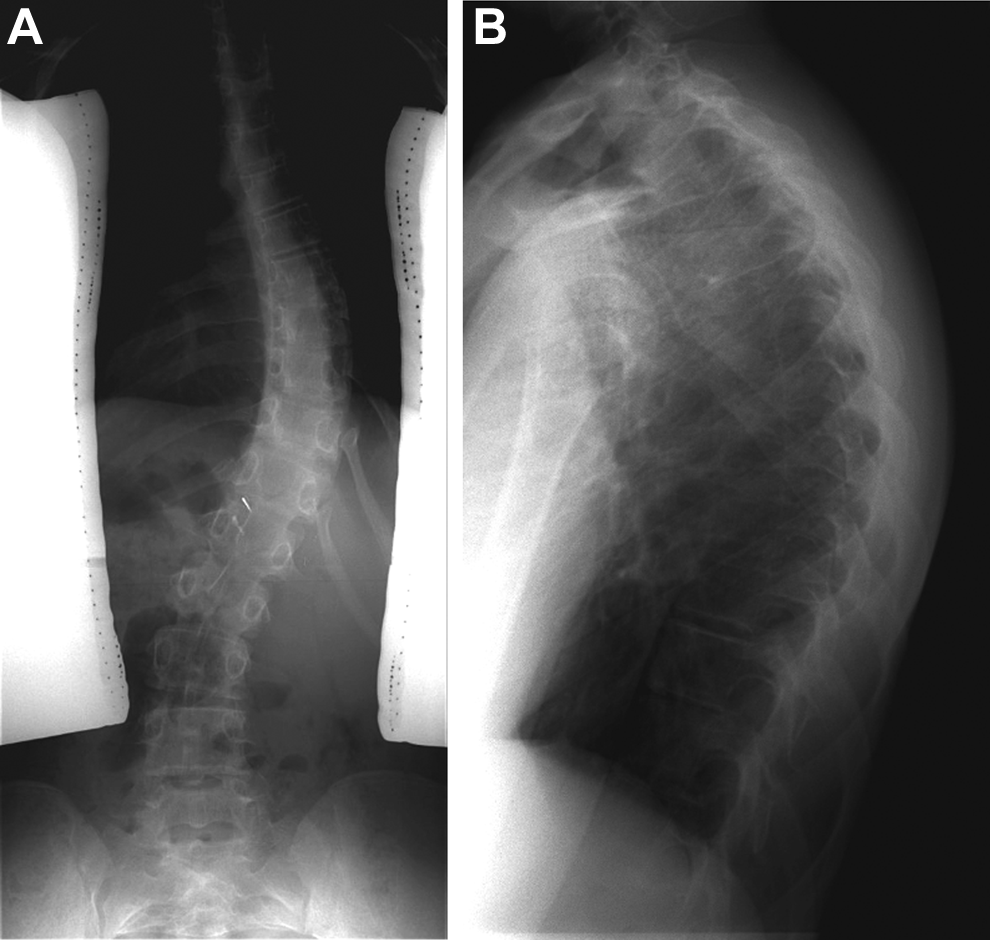
Preoperative posteroanterior (A) and lateral (B) view radiographs of a 14-year-old female patient with a Lenke type 1 idiopathic curve.
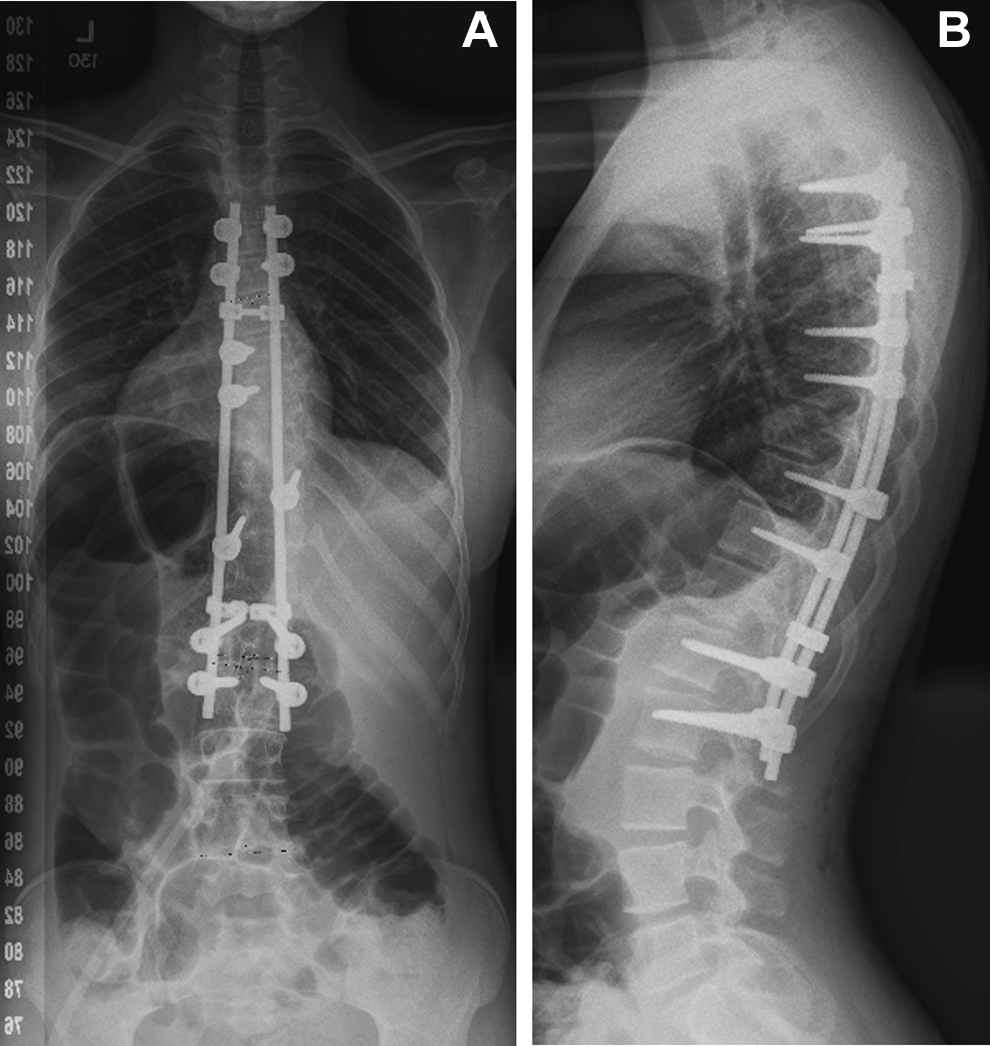
Images of the same patient shown in Figure 2. Postoperative posteroanterior (A) and lateral (B) view radiographs obtained at 2-year follow-up. The screw density in this construct is 1.09 per level.
Determination of Cost
The total cost of instrumentation for each case was estimated based on the 2014 list pricing for our institution. The senior author used USS screws for all cases. Cost per fusion level was determined for LD screw constructs based on the number of screws used in each construct. This was compared with the theoretical cost of a construct with 2 screws used at every level. The cost of rods was not evaluated, because all constructs use 2 rods for which there would be minimal cost difference. Two cross-links were routinely used in LD constructs, and this added cost was evaluated.
Statistical Analysis
Each of the 3 observers calculated the aforementioned measurements independently. For each patient, the mean of each angle measured by the 3 observers was calculated and included in the final analysis. When disagreement occurred among observers regarding curve classification, the curve type was determined by the majority designation.
Results
Forty-five patients were identified after operative database query. Ten patients had incomplete radiographic history and were excluded, leaving 35 cases for analysis. The mean patient age at the time of surgery was 14.9 years (range = 12-19 years), with 28 female and 7 male patients. Of the 35 cases, 23 had Lenke type 1 curves, 6 had type 3, 2 had type 2, 2 had type 4, and 2 had type 5. The average length of follow-up was 2.3 years (range = 2-4.4 years). The mean construct density was 1.2 screws per level fused, with a range of 1.1 to 1.5 screws (Table 1).
Patient, Surgical, and Radiographic Characteristics.
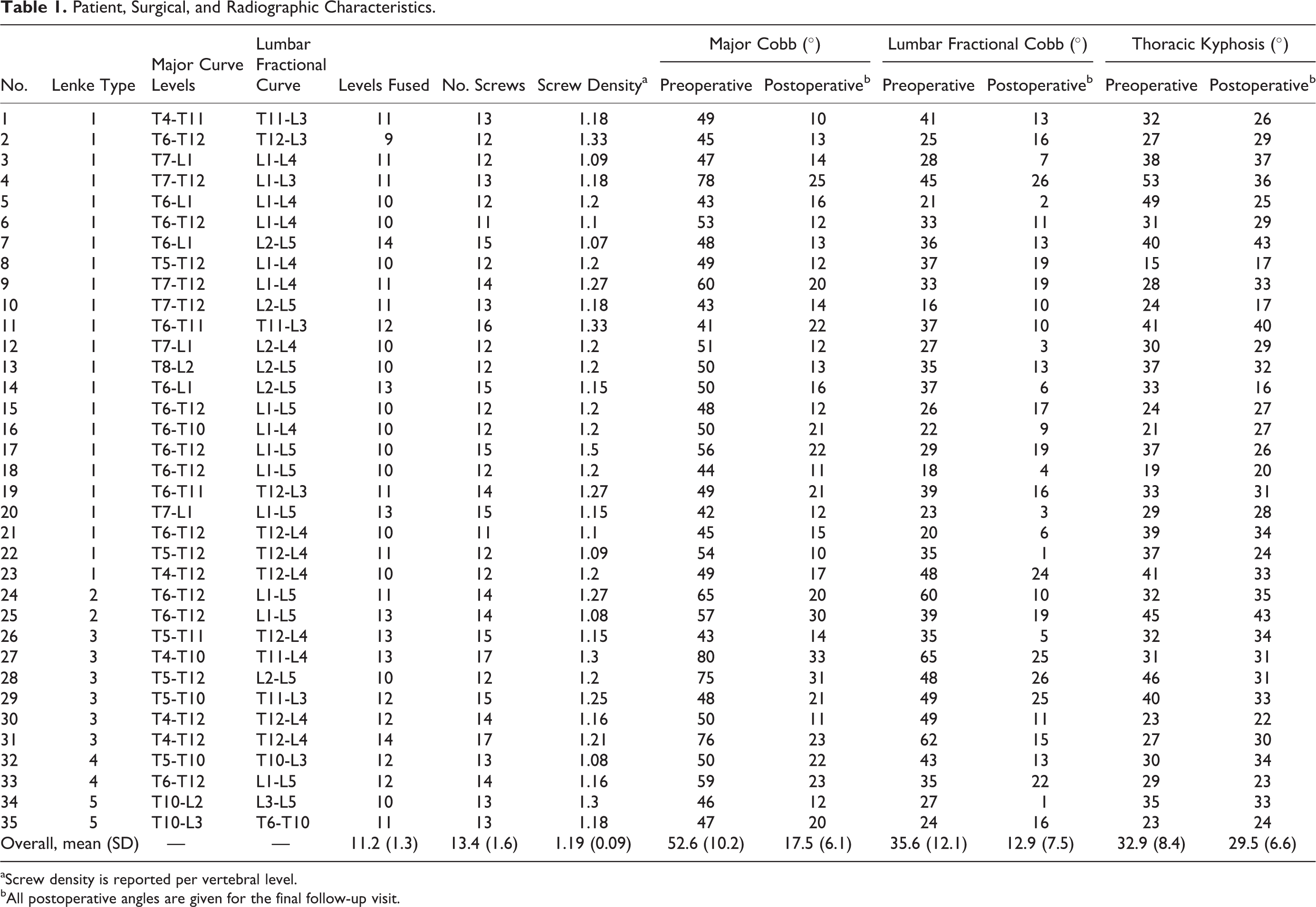
aScrew density is reported per vertebral level.
bAll postoperative angles are given for the final follow-up visit.
Curve Correction
The mean preoperative major Cobb angle measurement among the 3 observers was 52.6° (curve range = 41° to 80°). The mean percent major curve correction was 71.2% at initial postoperative follow-up and 66.9% at latest follow-up. Lumbar fractional curves improved from a mean of 35.6° preoperatively to a mean of 10.6° (70% correction) at initial follow-up and 12.9° (63% correction) at final follow-up. Thoracic kyphosis decreased from a mean of 32.9° preoperatively to a mean of 29.5° postoperatively. The mean postoperative LIV angle measured 5.6° at latest follow-up. Table 1 shows the preoperative and postoperative radiographic results for each patient, and Table 2 summarizes radiographic results.
Radiographic Outcomesa.
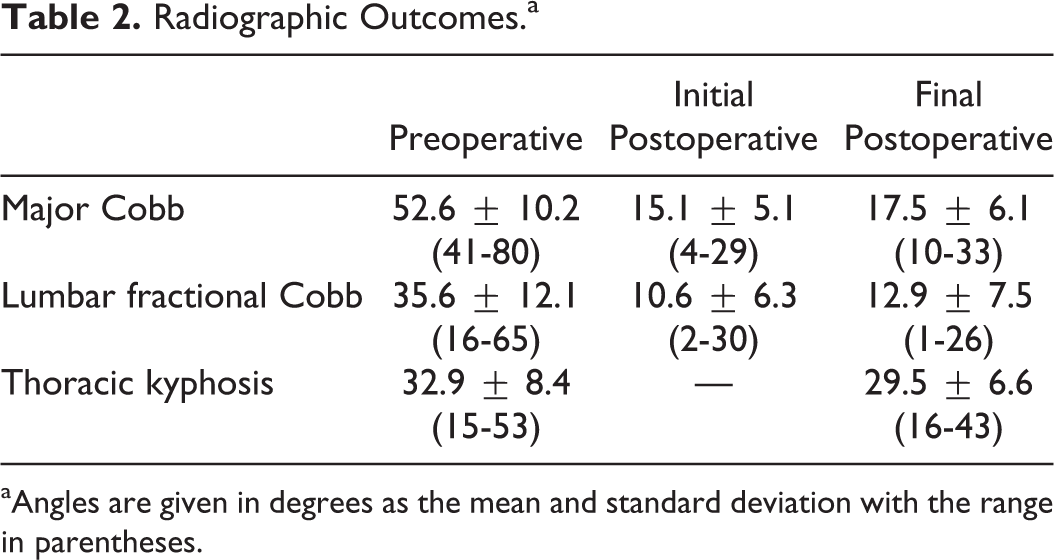
aAngles are given in degrees as the mean and standard deviation with the range in parentheses.
Complications
No intraoperative or postoperative neurological complications occurred. At latest follow-up, no instrumentation failure, pseudarthrosis, “add-on” of other vertebrae, or decompensations had occurred. No patient required revision surgery.
Cost Analysis
At our institution, the cost of all pedicle screws is $1000 per screw, and the cost of a crosslink is $750. In our cohort of 35 patients, we placed a total of 468 screws and 70 crosslinks (2 crosslinks per construct). The total implant cost was $520 500, or an average of $14 871 per patient, excluding the cost of the rods. Assuming an HD construct with 2 screws per level, the cost of our cohort with an HD model would amount to $834 500 ($782 000 for the screws and $52 500 for the crosslinks), or an average of $23 840 per case. In this cohort of 35 patients, we obtained a savings of $314 000 in implant costs, almost $9000 per patient.
Discussion
The purposes of this study were to present a single surgeon’s experience with a unique LD screw-rod construct for scoliosis correction, to determine whether an LD screw construct can achieve curve correction similar to that achieved with HD constructs in AIS, and to assess the cost savings associated with use of an LD screw construct. Several studies to date have reported on the correlation between construct screw density and curve correction. 11 –15 Substantial variability exists among the studies regarding type of screw (monaxial vs polyaxial), stiffness of rods, type of construct (screws, hooks, wires), and density of construct. Nevertheless, several authors have shown that screw density has little effect on curve correction. 11 –15 Our findings corroborate the existing body of evidence. The density of our unique LD construct is among the lowest reported in the literature (mean of 1.2 screws per level fused), and yielded curve corrections (mean 67% correction at latest follow-up) are similar to those described by other authors. 11 –15
In a retrospective review of patients with Lenke 1 AIS, Bharucha et al 12 compared LD versus HD implants. The authors reported a mean LD implant density of 1.1 in curves with a mean of 48°, which resulted in an average of 66% correction; they found no difference in curve correction between the 2 groups. Although our cohort has a slightly greater mean screw density (mean = 1.2 screws per fused level), it differs substantially with a wider range of curve types and greater preoperative curve measurements. Furthermore, the results reported by Bharucha et al exhibit a marked selection bias in that the operative technique changed throughout their study period and no standardization was implemented within their study group. This is in contrast to our cohort, which was treated with a standardized technique regardless of preoperative curve type or measurements.
Li et al 15 obtained an average of 74% correction with a mean preoperative Cobb angle of 61.87° in Lenke 1 curves. Although the authors did not report the screw density, the corrections were obtained using constructs with screws placed at every 1 to 3 levels on the convex side and at every level (consecutive screw group) or every other level (interval screw group) on the concave side. The interval screw group had similar radiographic outcomes compared with the consecutive screw group. The present study provides more detail to select pedicle screw placement for LD constructs (Figure 1). Additionally, our technique involves reducing each screw to the precontoured rod and does not require the rod derotation described by Li et al.
In a study that compared monaxial with polyaxial screws, Lonner et al 16 evaluated 100 consecutive patients who underwent scoliosis correction. Although the study was designed to compare monaxial, polyaxial, and hybrid constructs, the patients within the polyaxial group (n = 33) had a mean implant density of 1.06 with an average of 68% curve correction, whereas the patients in the monaxial group (n = 34) had a mean implant density of 1.69 and an average of 69% curve correction. Our results, although similar overall, differ notably in our larger preoperative curve measurements and our standardized technique. Furthermore, our patients obtained the same correction with a lower density of monaxial screws.
Hwang et al 13 used a unique LD pedicle screw construct, inserting screws into every other segment on the corrective side and 2 to 4 screws on the supportive side. They achieved a mean curve correction of 67%. Although they did not directly report the mean screw density in their article, it is estimated to be 1.04. 11 The series presented by Hwang et al serves as another example of how LD constructs can be used to achieve curve correction similar to that achieved with HD constructs.
Samartzis et al 17 demonstrated the utility of fulcrum bending radiographs to determine fusion levels using an alternate level screw strategy in patients with AIS. While flexibility films helped the authors determine the fusion levels, spine flexibility did not alter the screw density of their constructs. These authors instrumented every other vertebral level bilaterally, including each end of the construct. For even numbered fusion levels, the authors placed screws bilaterally in the vertebra adjacent to the LIV. The constructs used by the authors was very different from the present study, but yielded similar screw density results. If this method of instrumentation were utilized for our study, we would have found a screw density of 1.14 screws per level (vs 1.19 screws per level with our construct). The authors found an immediate postoperative curve correction of 71.3% and final curve correction of 66.6%, which is nearly identical to the present study (71.2% and 66.9%, respectively). The preoperative and final follow-up sagittal alignment Cobb angles were 18.1° and 17.2°, respectively, compared to 32.9° and 29.5° in the present study.
Considering that our operative technique and construct differ from those previously reported (ie, derotation method and screw pattern), the results of our study reinforce the existing body of evidence that LD constructs are similar to HD constructs in ability to correct scoliosis. This is highlighted by the larger preoperative curve measurements and wider range of curve types in our cohort. We demonstrate an average $9000 cost savings per patient. This number is an average for the contract price at our institution, but it emphasizes the substantial difference in costs between HD and LD constructs.
Study Limitations
The present study had limitations. It was a retrospective review of the radiographic findings associated with our patient cohort. As such, we did not have patient-reported outcome measures, which is an important factor to consider while trying to optimize the screw density needed for maximal patient outcomes. Our sample accounts for all AIS patients treated by a single surgeon over a 5-year period, and the consistent use of an LD screw-rod construct makes it impossible to compare our results to a control group over the same timeframe. Finally, the retrospective nature of the study limits our ability to recover enough lateral bending films to report a meaningful measurement of the average curve flexibility. Curve flexibility was not used, however, to determine fusion levels or when to use an LD construct so the absence of lateral bending films does not substantially affect the results of the study. Even curves up to 80° were effectively treated with this technique.
Conclusions
Our LD screw construct is among the lowest density constructs reported in the literature and achieves curve correction comparable to that achieved with HD constructs. In today’s rapidly changing health care environment, emphasis is on cost savings. This study adds to the body of evidence that LD constructs can be used effectively to achieve the goal of an acceptable deformity correction with a low complication rate while achieving substantial cost savings.
Footnotes
Acknowledgment
The authors thank Dori Kelly, MA, senior editor and writer at the University of Maryland School of Medicine, for invaluable assistance with the manuscript and figures.
Declaration of Conflicting Interests
DG received a consulting fee from DePuy Synthes Spine. On an ongoing basis, DG receives payment from AOSpine North America for lectures when serving as faculty at courses. In the past, DG has received payment from DePuy Synthes Spine for lectures presented at a resident leaders’ course. DG currently receives royalties from DePuy Synthes Spine for oracle instrumentation and from Globus Medical for the gateway plate. Dr Ludwig reports grants from AO Spine North America for Spine Fellowship support, Globus Medical, K2M Pacira Pharmaceuticals, and OMeGA. SL receives personal fees and royalties from DePuy Synthes. No other relationships, conditions, or circumstances exist that present a potential conflict of interest. The remaining authors declare no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.