
Abstract
Study Design:
Retrospective database study.
Objectives:
Analysis of economic and demographic data concerning interspinous device (ID) placement throughout the United States to improve value-based care and health care utilization.
Methods:
The National Inpatient Sample (NIS) database was queried for patients who underwent insertion of an interspinous process spinal stabilization device (ICD-9-CM 84.80) between 2008 and 2014 across 44 states. Demographic and economic data were obtained which included the annual number of surgeries, age, sex, insurance type, location, and frequency of routine discharge. The NIS database represents a 20% sample of discharges from US hospitals, which is weighted to provide national estimates.
Results:
There was a 73% decrease in ID implanted from 2008 to 2014. The mean cost associated with insertion of the device increased 28% from $13 653 in 2008 to $17 515 in 2014. The mean length of stay (LOS) increased from 1.8 to 2.4 days. Patients aged 45 to 64 years increased from 14.1% to 34.3% while patients aged 65 to 84 years decreased from 74.4% to 60.6%. By region, 34% of ID placement occurred in the South followed by 19.7% that occured in the Northeast. When stratifying by median income for patient zip code, the procedure was performed more in cities designated as higher rather than lower income areas (74.2% and 19.5%, respectively).
Conclusions:
Throughout the United States, there was a progressive decline in the insertion of interspinous spacers by 73% over the study period. The total costs for the procedure increased by 28% while the aggregate national charges decreased by 55.6% between 2008 and 2014.
Introduction
Traditional decompressive surgery is the surgical standard of care for symptomatic lumbar spinal stenosis. However, implantation of standalone interspinous spacers is a minimally invasive alternative surgical option for lumbar spinal stenosis and degenerative disc disease. This modality allows for the use of local anesthesia, preserves bone and soft tissue, and results in shorter hospital stays versus traditional open decompression. 1 Neurogenic claudication is a common presentation of lumbar spinal stenosis with patients relieving their symptoms by assuming a flexed posture after sustained ambulation. Interspinous devices (IDs) utilize this concept of flexion to decrease symptoms of spinal stenosis by increasing canal volume, restoring foramina height and unloading the facet joint. 2,3 IDs are indicated for patients with lumbar spinal stenosis who have failed at least 6 months of nonoperative treatment. 2,4 Despite the minimally invasive approach and comparable outcomes with traditional decompressive surgery, the procedure has failed to gain popularity in the United States.
Despite the relative recent introduction of IDs to the market, the concept of IDs is not novel. The first ID prototype was designed in the 1950s and meant to provide symptomatic relief for patients who experienced an acute herniated disc. Referred to as the Knowles device, this implant was designed to be placed between adjacent spinous processes to provide indirect decompression. 5 However, due to high failure rates, the device never garnered wide acceptance. In contrast, modern IDs have been designed for permanent implantation and can be utilized for the treatment of multiple pathologies including stenosis, herniated nucleus pulposus and degenerative disc disease. 6 –9 The spacer is fixed anteriorly in the interspinous space to achieve maximal flexion as well as to avoid loss of fixation and spinous process deformation. Device migration is prevented by the supraspinous ligament posteriorly and lamina anteriorly. The most commonly implanted ID includes X-STOP, Coflex, Wallis, and DIAM, with most literature surrounding the X-STOP device. 4,10 –16
The purpose of this study was to determine the trend in ID placement procedures over the recent decade, and to evaluate the decline in procedure utilization. By performing a longitudinal analysis of an administrative inpatient database, we may understand the annual trends and economic data surrounding percutaneous vertebral augmentation procedures. An appreciation for the yearly national aggregate cost of these procedures is of significant importance to surgeons, policy makers and hospital administrators. In this study, we utilized data from the National Inpatient Sample (NIS) database to compare a large, national cohort of patients who underwent ID placement from 2008 to 2014.
Methods
Data Source
Data was collected from 44 states between 2008 and 2014 in the NIS database. The NIS database was developed for the Healthcare Cost and Utilization Project (HCUP) and constitutes the largest all-payer inpatient database in the United States. The database represents a 20% sample of discharges from US hospitals (excluding rehabilitation and long-term acute care hospitals), which is weighted to provide national estimates.
Patient Selection and Characteristics
The NIS database was queried for patients who underwent insertion of an interspinous process spinal stabilization device between 2008 and 2014 using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM) 84.80.
Demographic and economic data were obtained for ID procedures. Insurance types included Medicare, Medicaid, private, uninsured, and other. The “other” category included workman’s compensation, TRICARE/CHAMPUS, CHAMPVA, Title V, and a number of other government insurance programs. The annual number of surgeries, patient age, sex, total charges, total costs (in then-year dollars), insurance type, length of stay (LOS), location, and frequency of routine discharge were recorded. Aggregate charges or the “national bill” was defined as the sum of all charges for all hospital stays in the United States. Total charges were converted to costs using cost-to-charge ratios based on hospital accounting reports from the Centers for Medicare and Medicaid Services (CMS). Costs reflect the actual costs of production, while charges represent what the hospital billed for the case. Relative standard error (SE [standard error/weighted estimate]) was reported where applicable.
Descriptive statistics were performed to compare variables. Two-sample Student t test was employed to analyze the difference in continuous variables and chi-square or Fisher’s exact employed for categorical variables. Findings were considered statistically significant when P < .05. Analysis was conducted using IBM SPSS Statistics version 24. The NIS database is deidentified and was therefore deemed exempt by our institutional review board.
Results
An estimated 14 225 patients underwent ID placement in the United States from 2008 to 2014. In 2008, 4012 IDs were implanted followed by a peak in ID placement in 2009 at 4251 procedures. However, there was a subsequent sharp decline in the number of procedures by 86% from 2009 to 2012. In 2014, the number of procedures increased to 1080, marking a net 73% decline in procedures from 2008 to 2014 (Figure 1).
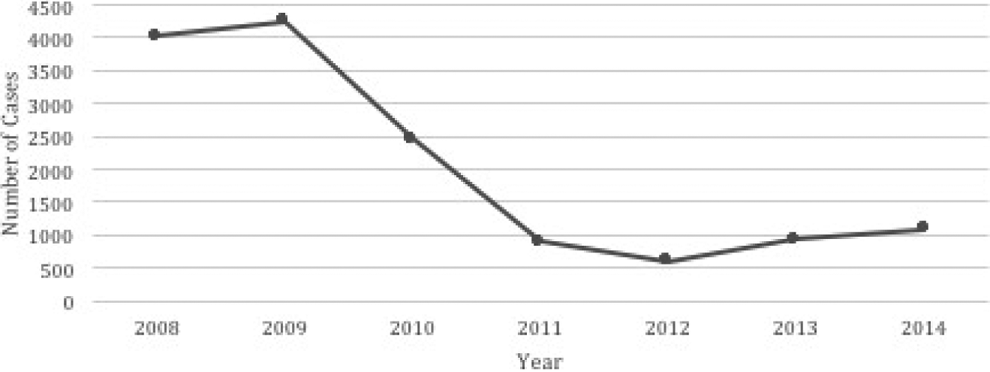
Total number of discharges per year was plotted for Interspinous device placement from 2008 to 2014. Interspinous process spinal stabilization device ICD-9-CM: 84.80. Interspinous device placement procedures sharply decreased from 2009 to 2012.
The mean LOS for ID placement increased from 1.8 days in 2008 to 2.4 days in 2014. The mean LOS from 2008 to 2014 was 2.03 days (SE = 0.143; range = 1.8-2.4). On average, 75% of patients underwent routine discharge. In all, 13.5% of patients were discharged with home health care, and 10.5% of patients were discharged to another institution, defined as a nursing home or a rehabilitation center. The percentage of patients discharged with home health care rose from 5.8% in 2008 to 15.8% in 2012, and then subsequently declined to 11.1% in 2014. The number of patients discharged to another institution remained relatively stable around 15.5% from 2008 to 2014, except for in 2013 where there was a sharp decline to 8% (Figure 2).
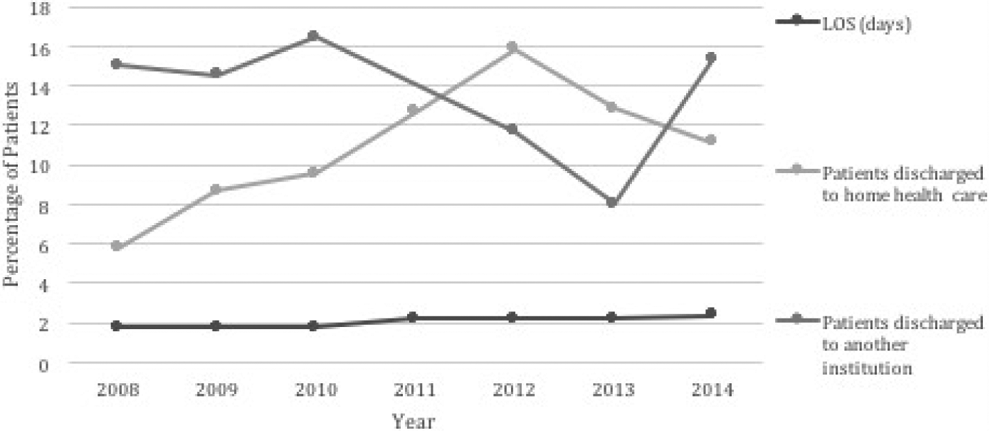
Length of stay and type of discharge were plotted for interspinous device placement from 2008 to 2014. Length of stay remained stable at 2.03 days.
The mean total hospital cost for ID placement increased over the 6-year period from 2008 to 2014 (Figure 3). The mean cost associated with insertion of the device increased 28% from $13 653 in 2008 to $17 515 in 2014 (mean = $15 774; SE = $1040, range = $13 561-$18 846). The aggregate national charges (“The National Bill”) for ID placement decreased by 55.6% from $189 940 130 in 2008 to $84 304 255 in 2014 (Figure 4). The total aggregate national costs for ID placement from 2008 to 2014 totaled $741 611 718 (mean = $105 944 531; SE = $34 607 249; range = $40 856 278-$190 567 601).
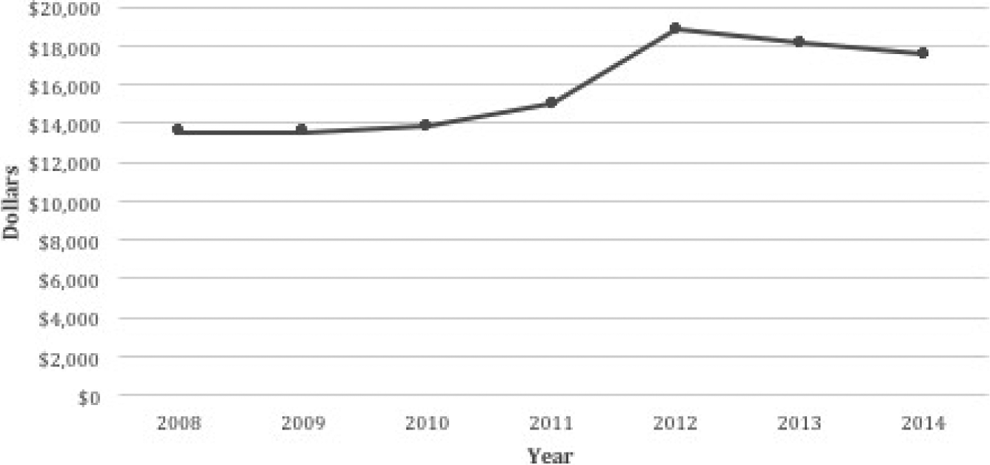
Mean total cost per year was plotted for interspinous device placement from 2008 to 2014. Mean total cost increased from $13, 563 in 2008 to $17 515 in 2014, marking a 28.3% increase.
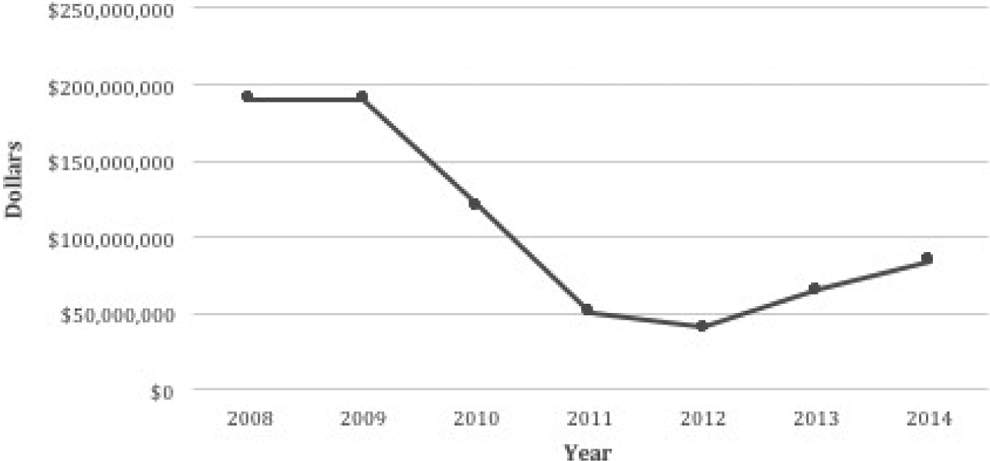
Aggregate national charges (“The National Bill”) was plotted for interspinous device placement from 2008 to 2014. The aggregate national charges decreased by 55.6% from 2008 to 2014.
The majority of patients undergoing ID placement were between the ages of 65 and 84 years, accounting for 72% of patients. This was followed by 16.5% of patients between 45 and 64 years and 7.8% of patients 85+ years. From 2008 to 2014, the percentage of patients undergoing ID placement aged 45 to 64 years increased from 14.1% to 34.3% while the percentage of patients aged 65 to 84 years decreased from 74.4% to 60.6% (Figure 5). Females accounted for 52% of patients, while males accounted for 46% of patients. From 2008 to 2014, the percentage of females decreased from 55.1% to 44% while the percentage of males increased from 43.1% to 56% (Figure 6). Medicare accounted for 79.5% of payer types, and 74.2% of procedures were performed in areas designated as not low income when stratified by median income for patient zip code. From 2008 to 2014, the percentage of patients undergoing ID placement with Medicare decreased from 79.7% to 66.7% while private insurance coverage for ID placement increased from 13.5% to 23.1% (Figure 7). IDs demonstrated a geographic predilection with the South accounting for 34% of procedures followed by the Northeast at 19.7% of procedures. Procedures performed in Metropolitan areas accounted for 91.4% of cases and nonteaching hospitals accounted for 50.5% of cases.
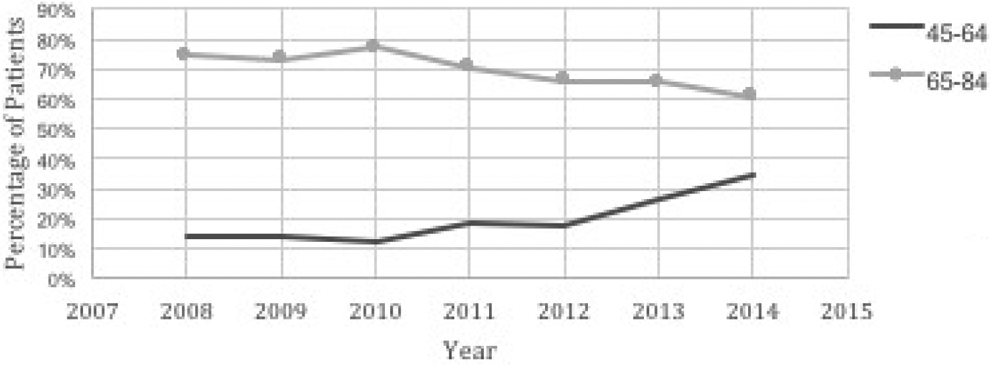
The proportion of patients aged 45 to 64 and 65 to 84 years was plotted from 2008 to 2014. Patients aged 45 to 64 years increased from 14.1% to 34.3% while patients aged 65 to 84 years decreased from 74.4% to 60.6%.
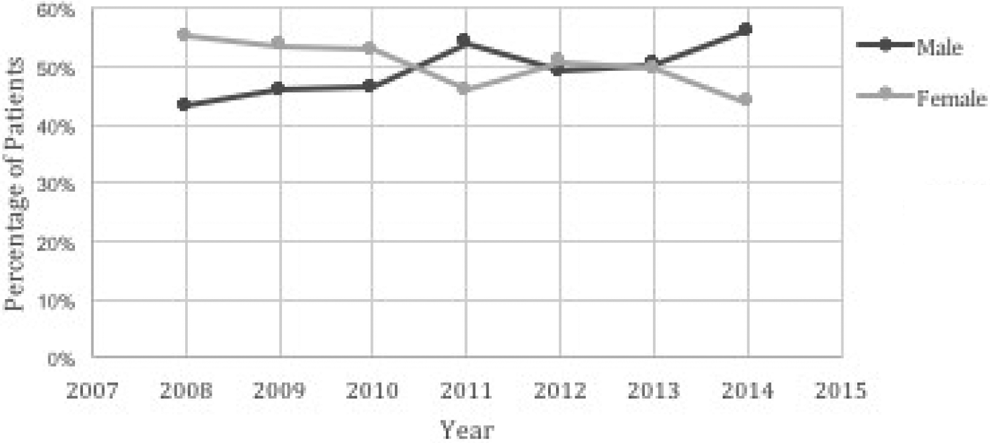
The proportion of males and females undergoing interspinous device was plotted from 2008 to 2014. The percentage of females decreased from 55.1% to 44% while the percentage of males increased from 43.1% to 56%.
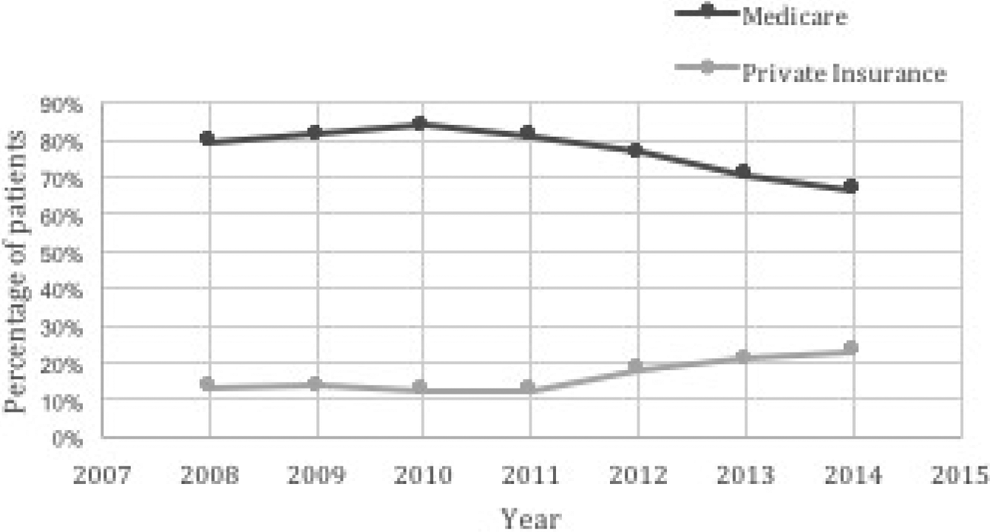
The proportion of Medicare and private insurance patients undergoing interspinous device (ID) was plotted from 2008 to 2014. The percentage of patients undergoing ID placement with Medicare decreased from 79.7% to 66.7% while private insurance coverage for ID placement increased from 13.5% to 23.1%.
Discussion
The theoretical advantage of an ID lies in the fact that it is a motion-preserving implant allowing relief from claudication while obviating the need for traditional decompression and segmental fusion. This is accomplished by taking advantage of the postural dependency of neurogenic claudication as it relates to the anatomic effects of flexion and extension on the spinal canal. As the lumbar spine undergoes extension, there is an anterior displacement of the facet capsule by the caudal superior articular facet resulting in neuroforaminal stenosis. Likewise, there is a compensatory buckling of the ligamentum flavum posteriorly and anterior bulge of the disc resulting in a decreased cross sectional canal diameter. 17 By interposing the device between adjacent spinous processes, the spinal segment is held in slight flexion without limitations on lateral bending or rotation. Computed tomography and magnetic resonance imaging studies have demonstrated an increase in cross-sectional spinal cord area by 11% to 22% with segmental flexion provided by an ID. 11,18
Despite numerous advantages, including a minimally invasive approach and motion preserving fixation, there is concern regarding the effect of flexion on overall sagittal alignment. Although flexion permits increased cross-sectional area of the canal, the phenomenon of ID placement predisposing to positive sagittal imbalance has not been reliably reported in the literature. In a prospective longitudinal study of 40 patients receiving ID placement for symptomatic lumbar stenosis, Crawford and colleagues 19 found unchanged sagittal alignment and improvements in back pain and function at final follow-up. Furthermore, the authors reported that back pain and function were not correlated with changes in sagittal alignment or posterior disc angle. 19 Similarly in a study of 60 patients who underwent Coflex ID placement, there were no significant differences between preoperative and postoperative lumbar lordosis, and all patients showed statistically significant improvement in lower back pain and function as measured by visual analogue scale and Oswestry Disability Index scores at the time of final follow-up. 20
Still, there remains a paucity of literature on long-term outcomes for IDs. In the largest multicenter, prospective randomized study to date, Zucherman et al 4 found a significant improvement of 45.4% in Zurich Claudication Questionnaire scores versus a 7.4% improvement in the nonoperative control group. Furthermore, they found that there was a 44.3% mean physical functioning improvement compared with the −0.4% improvement in the nonoperative control with no major complications associated with X-STOP placement. The overall open laminectomy revision rate was 6% for the ID cohort versus 31% for the nonoperative arm. Gazzeri et al 21 performed a large multicenter retrospective study of 1108 patients who underwent placement of an ID device. Seventy-six percent of patients were reported to be “very satisfied” with their outcomes and 12.5% reported “satisfied” at a minimum 2-year follow-up. Overall reoperation rate was 9.6% with mean follow up 44.8 months and minimum follow up of 3 years.
However, when comparing ID implantation to traditional decompression, Moojen et al 22 demonstrated no difference in short-term (8 weeks) outcomes using the Zurich Claudication Questionnaire. They additionally found that the ID group had a higher revision rate (29%) than traditional decompression (8%). Similarly, Patil et al 23 performed a comparative effectiveness study and found higher reoperation rates for IDs (12.6%) versus open laminectomy (5.6%) at 12 months. Furthermore, a meta-analysis by Phan et al 24 showed a higher reoperation rate for ID versus bony decompression at 23.7% and 8.5%, respectively. However, their data did demonstrate statistically lower complication rates (4% vs 8.7%) for the IDs. 24 Other studies have reported revision rates ranging from 13.35% to 33%. 14,24 –28 Gazzeri et al 1 cite the main reasons for ID failure as indication errors, technical errors, and implant failure.
In the current study, the mean total hospital cost of ID placement was $15 774 with a mean LOS of 2.03 days from 2008 to 2014. The aggregate national charges (“The National Bill”) for ID placement decreased by 55.6%, even though the cost of ID placement increased from 2008 to 2014, which can be explained by the overwhelming decrease in ID utilization. A retrospective study by Patil et al 23 reported an ID placement cost of $17 432 and LOS of 1.6 days. At 12 months, there was a higher cumulative cost with IDs ($39 173) versus laminectomy ($34 324). Likewise, Epstein 16 found single level X-STOP placement costs $7900 and double level costing $13 429. This is in comparison with single level laminectomy at $9291 and double level laminectomy at $9329. Epstein 16 concluded that, with double level procedures, laminectomy was more cost effective than X-Stop. Burnett et al 29 studied the cost-effectiveness of ID versus laminectomy and found that stand-alone laminectomy was more effective and less costly than X-STOP ID placement using a cost effect model. They went on to conclude that lumbar laminectomy was the most cost-effective method of treating symptomatic lumbar spinal stenosis.
The driver for the increased cost for ID placement reported in the current study is likely multifactorial; however, prior studies have implicated the increasing cost of the subsequent generations of IDs.
12,14,30
In a European randomized controlled trial of 160 patients receiving ID placement or bony decompression, the cost of ID placement was significantly higher than bony decompression, with a mean difference of difference
From the 4012 IDs placed in 2008 to the 1080 placed in 2014, there has been a 73% decline in interspinous process utilization. To date, this is the only epidemiological study examining utilization of IDs found in the literature. This article serves to highlight the declining rates of ID utilization and further examine causal factors resulting in such a decline.
As mentioned previously, there is a paucity of data to support the mid to long-term outcomes of interspinous fixation. The literature demonstrates favorable outcomes for ID fixation when compared to nonoperative modalities. However, multiples studies have shown equivocal functional outcomes between ID fixation when compared with traditional decompression. Additionally, IDs have higher rates of reoperation and are less cost-effective than bony decompression alone. 22,23 These factors have likely influenced the decline in ID placement since 2008 as there continues to be insufficient evidence to conclude IDs are superior to traditional decompression. This was further supported by a modified network analysis systematic review of IDs by Chou et al 31 who reported low evidence supporting greater treatment effects for ID placement compared with decompression for disability and pain outcomes at 12 months. Furthermore, the North American Spine Society 2011 clinical guidelines indicate there is insufficient evidence to warrant approving or disapproving ID placement. Given the increasing focus on health care utilization and value-based care, there has likely been pressure on surgeons to pursue more cost-effective modalities such as bony decompression. However, the current study can only speculate on, but not justify, the causal factors mentioned based on the literature. It is the senior author’s opinion that the decrease in ID utilization is more presumably due to a lack of established improvement in clinical outcomes compared with traditional bony decompression rather than financial factors. Interestingly, as the rate of ID placement has declined, the rate of other elective spine procedures to treat degenerative lumbar conditions, including spinal fusion and laminectomy, have correspondingly increased. 32,33
Many of the limitations of this study are due to the intrinsic limitations of large patient databases. The NIS database does not include physician-based fees and costs are calculated from hospital specific cost-to-charge ratios, which may exaggerate surgical cases. Still, these hospital specific cost-to-charge ratios have been internally validated by Agency for Healthcare Research and Quality. Inherent to a large study, the surgeries were performed by a large variety of surgeons, allowing for differences in surgical technique and potential indication bias. Furthermore, there can be potential inaccuracies of ICD-9 CM billing records, errors transferring data from hospital records to administrative records, underreporting of procedures, or exclusion of missing cases in the NIS database.
Conclusion
From the 4012 ID procedures in 2008 to the 1080 in 2014, there has been a 73% decline in ID utilization in the United States. Additionally, the total costs for the procedure increased by 28% while the aggregate national charges decreased by 55.6% between 2008 and 2014. The theoretical advantages of ID aim to increase neuroforaminal and central canal cross-sectional area by holding the vertebral segment in slight flexion while allowing for lateral bending and axial rotation. While this fixation method has shown improved efficacy versus nonoperative modalities, recent literature demonstrates increased cost-effectiveness and decreased reoperation rates with traditional bony decompression. Perhaps these factors have contributed to the decreased utilization of IDs from 2008 to 2014 throughout the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Ronald A. Lehman Jr reports grants from PRORP (Department of Defense Peer Reviewed Orthopaedic Research Program), personal fees and nonfinancial support from DePuy Synthes Spine, personal fees and nonfinancial support from Stryker, personal fees and nonfinancial support from Medtronics outside the submitted work. Dr Lawrence Lenke reports unpaid positions from Board Membership OREF and GSO, personal fees from Consultancy–DePuy Synthes Spine, K2M, Medtronic, personal fees from Expert Testimony–Fox Rothschild, LLP, grants from AO Spine; Scoliosis Research Society; DePuy Synthes Spine; Setting Scoliosis Straight Foundation; EOS, Royalties from Patents–Medtronic, personal fees from Travel accommodations/meeting expenses–AOSpine, Broadwater, Seattle Science Foundation, Scoliosis Research Society, The Spinal Research Foundation, grants from Fellowship Grant–AOSpine, North America, grants from Philanthropic research funding outside the submitted work. No other authors report potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.