
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The objective of the present study was to compare the effectiveness of 2 different pharmacological formulae in selective nerve root injections.
Methods:
We studied a series of 298 patients who received a selective nerve root injection and made a comparative study dividing them into 2 groups according to the drugs used. In group A, we used betamethasone 6 mg and lidocaine, while in group B, triamcinolone 60 mg and bupivacaine were used for the procedure. We evaluated the patients for a period of at least 8 months, assuming the need for surgical therapy as the failure of the procedure.
Results:
Both groups had 149 patients with similar etiological characteristics. Forty-seven patients (16%) required surgery to relieve pain with a similar distribution between groups (24 from group A and 23 from group B). Time between nerve root injection and surgery was 86.79 (14-360) days on average in group A and 75.76 (2-180) days in group B with no statistical difference (P = .67). Only one complication was documented, an anaphylactic shock in a patient in group B.
Conclusions:
Based on these results, we found no difference in the type of steroid or local anesthetic used for selective nerve root injections.
Keywords
Irritation signs of lumbar nerve roots are habitual patients’ complaints in daily practice, usually caused by mechanical compression and/or secondary to a cascade of inflammatory biochemical interactions. 1 The treatment options for these radiculopathies in the early stages include administration of periradicular steroid injections and local anesthetics. This option has proven to improve pain and reduce the need for a surgical intervention. 2
Ever since this treatment option was described, several variables to improve effectiveness have been studied: X-ray or computed tomography (CT) scan guidance, procedure made in the acute or chronic phase, and/or accurate needle tip placement. However, few studies assess the differences comparing 2 pharmacological formulae.
In our search in the literature, we found an article by El-Yahchouchi et al about comparing particulate and nonparticulate steroids using subjective questionnaires and with a maximum 2-month follow-up. 3 The aim of this study was to compare the results obtained in a series of patients with lumbar nerve root symptoms treated with selective nerve root block injection using 2 different pharmacological formulae, with a longer follow-up and in a large case series.
Material and Methods
A comparative retrospective study was performed including a series of patients treated with selective nerve root injection with CT scan guidance. The procedures were conducted by the same operator in 2 different health care centers.
Patients were divided into 2 groups depending on the pharmacological formula used for the intervention. Group A included patients receiving 3 mL of betamethasone 6 mg + 5 mL of 5% lidocaine; group B included patients receiving 1 mL of triamcinolone 60 mg + 5 mL of bupivacaine. Randomization was performed according to the center where nerve root injection was conducted.
The inclusion criteria were the following: (1) selective nerve root injection of the lumbar spine, (2) CT scan guidance, and (3) intervention conducted by the same operator in 2 different health care centers. The exclusion criteria were the following: (1) patients referred from a different center for the procedure and (2) lack of follow-up after the procedure.
A comparative assessment was performed between the 2 groups; the success rate was defined as patients who did not require surgery; injection failure was defined as the need for surgical intervention at some point in the follow-up period.
Institutional review board approval was not necessary because data was anonymized for the present work. It was presented and considered of no risk since the procedure is a validated treatment according to the present evidence.
Statistical Analysis
Student’s t test and χ 2 test were used to compare the differences between the mean values of the 2 groups. Microsoft Excel 2011 version 14.5.4 was used.
Results
A cohort study was performed from January 2011 to December 2014 in the 2 centers; 298 patients met the inclusion criteria. All the patients received conventional treatment including painkillers and rest and physiotherapy.
The patients were then divided into 2 groups according to the pharmacological formula used. Each group included 149 individuals with similar and matched etiological characteristics.
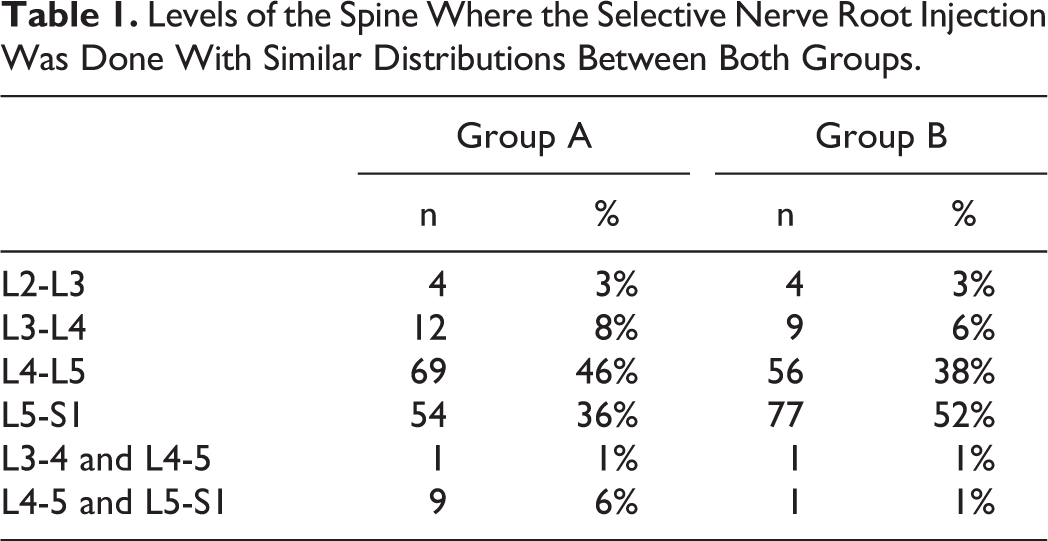
The mean age in group A was 49.60 years (20-81), and 93 (62%) were males; the mean age in group B as 51.76 years (15-90), and 81 (54%) were males. Minimum follow-up was 8 months. In group A, 77 nerve root injections were performed at the level of L5-S1 (52%), 56 at the level of L4-5 (38%), 9 in L3-4 (6%), 4 in L2-3 (3%), and 2 (2%) were multilevel procedures (Table 1). At the same time, 62 (42%) procedures were conducted on the right side, 79 (53%) on the left side, and 6 (4%) were bilateral. In group B, 54 nerve root injection were conducted at the level of L5-S1 (36%), 69 at the level of L4-5 (46%), 12 in L3-4 (8%), 4 in L2-3 (3%), and 10 (7%) were multilevel procedures (Table 1). At the same time, 62 (42%) procedures were conducted on the right side, 66 (44%) on the left side, and 21 (14%) were bilateral procedures.
Levels of the Spine Where the Selective Nerve Root Injection Was Done With Similar Distributions Between Both Groups.
All the procedures were made in patients with radicular pain as the main symptom. Both groups were equivalent as to the origin of the discomfort. In group A, 107 (72%) patients had an herniated disc, 17 (11%) lumbar stenosis, 4 (3%) spondylolisthesis, 15 (10%) facet hypertrophy, 2 (1%) synovial cyst, 2 (1%) disc reextrusion, and 2 (1%) cases complained of postoperative radiculopathy without an active root compression. In group B, herniated disc was the cause in 108 (72%) patients, lumbar stenosis in 18 (12%), facet hypertrophy in 9 (6%), spondylolisthesis in 6 (4%), synovial cyst in 5 (3%), disc reextrusion in 2 (1%), and postoperative radiculopathy in 1 (1%) case.
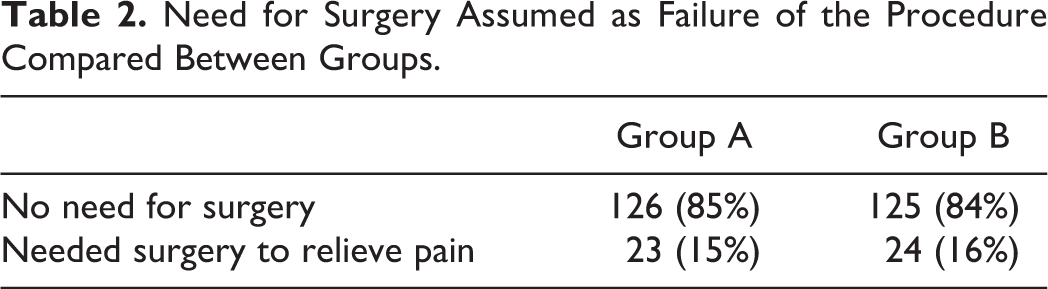
The treatment was considered to have failed if the patient proceeded to have surgery to ameliorate pain. A total of 251 (85%) patients did not require an operation, whereas 47 (16%) required root decompression to improve pain.
Twenty-four (16%) patients in group A and 23 (15%) patients in group B needed surgery; no statistically significant differences were observed (P = .87; Table 2).
Need for Surgery Assumed as Failure of the Procedure Compared Between Groups.
As for the patients in group A requiring surgery, 11 (46%) underwent a simple decompression and 13 (54%) also required instrumented fusion. Fifteen (65%) patients in group B underwent decompression alone, and 8 (35%) also required arthrodesis. After 2-year follow-up we did not have any patient with persistent pain.
Time between nerve root injection and surgery was 86.79 (14-360) days on average in group A and 75.76 (2-180) in group B; although the time was shorter in group A, the comparative difference was not statistically significant (P = .67; Figure 1).
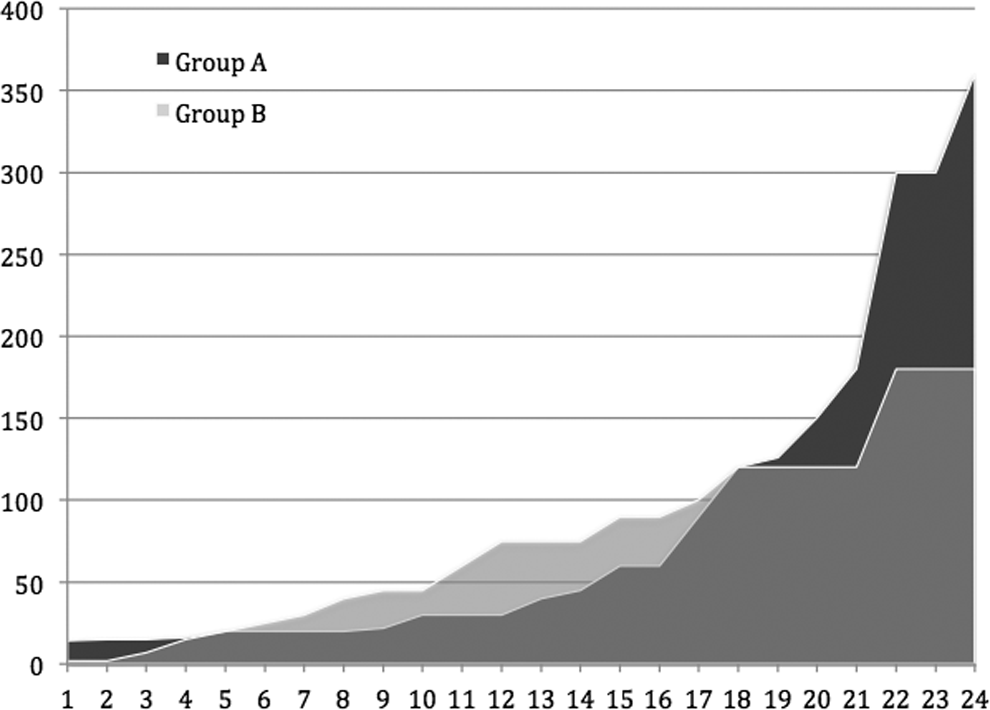
Time between selective nerve root injection and surgery measured in days comparing both groups.
Only one complication was recorded; one patient in group B developed anaphylactic shock 15 minutes after the procedure. The patient required intubation and was hospitalized at the intensive care unit for 48 hours.
Discussion
Selective nerve root injection is a common practice today for patients with nerve root irritation symptoms. It is mainly indicated for the management of intractable nerve root pain in order to ameliorate pain using a less aggressive option than surgery. 4
Considering the main aim of the procedure, surgical decompression of the nerve root was conducted if nerve root injection failed in order to assess the efficacy of each of the pharmacological formulae. The global failure rate was 16%, similar to the results described in the literature. 4,5
Choosing the type of medication for selective nerve root block is controversial, and several alternatives are available. The use of local anesthetic and depot steroids has been suggested in the literature. 6 As for the mechanism of action, the local anesthetic blocks the nociceptive stimulus on afferent fibers, and the addition of a steroid enhances the anti-inflammatory effect by inhibiting the inflammation mediator pathway. 7
We have not found publications comparing the use of different local anesthetics in this type of procedure. In our case series, we used lidocaine in group A and bupivacaine in group B. Supposing that bupivacaine is more powerful and has a longer lasting effect we might conclude that it somehow affects patient outcome, either by enhancing the effect of steroids or promoting a longer action of the steroid. 8 In spite of this observation, no differences were observed between the 2 groups.
Reports have been published describing the efficacy of different types of steroids used for nerve root blocks, comparing drugs from different classes. 3 However, we have not found any report comparing different steroids with a different therapeutic effect time. It should be underlined that the drugs compared in this investigation belong to a class generating an intermediate therapeutic effect (triamcinolone) and a prolonged therapeutic effect (betamethasone). We have not found differences favoring one or the other in relation to patients who might avoid undergoing a surgical procedure (P = .87).
Another aim of our study was to assess the time between the nerve root injection and an eventual decompressive surgery. We hypothesized that a long-acting steroid might generate a longer time to surgery as compared to an intermediate-action steroids. 9 Moreover, betamethasone has a more powerful anti-inflammatory effect. 10 However, although we observed that nerve root decompression took longer to occur (86.79 vs 75.76 days) in patients receiving betamethasone injections, this difference is not statistically significant (P = .67).
Complications reported in this type of procedure are limited. They usually involve inappropriate puncture sites leading to peridural hematomas, cerebrospinal fluid fistulas, or even neurological lesions. 11,12 We observed only one complication throughout the series under study, and it involved the group of patients receiving bupivacaine and triamcinolone. The patient presented signs of progressive hypoxia within 15 minutes of the procedure. Routine evaluations were performed, and she was diagnosed with anaphylactic shock. The patient was intubated in the intensive care unit and discharged within 48 hours without any major sequelae.
We found 2 limitations in this study; one of them involves not studying patient outcome in the initial stage. Most of the studies deal with pain during the first days in questionnaires like Visual Analog Scale, Oswestry, or Roland-Morris 13 ; the objective of our research was to study nerve root injection failure and the eventual need to add a surgical procedure. Another weakness of this study is that patients were not grouped according to the condition generating the nerve root symptoms. However, we do not think this might modify the results of our initial hypothesis.
Conclusion
We have not found any differences as to the drug used to perform the nerve root block. Based on the literature we consider that the use of a local anesthetic and a steroid is the first choice regardless of the origin or the drug class.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.