
Abstract
Design:
Systematic review.
Objective:
To conduct a systematic review to (1) summarize various classification systems used to describe cervical ossification of the posterior longitudinal ligament (OPLL) and (2) evaluate the diagnostic accuracy of various imaging modalities and the reliability of these classification systems.
Methods:
A search was performed to identify studies that used a classification system to categorize patients with OPLL. Furthermore, studies were included if they reported the diagnostic accuracy of various imaging modalities or the reliability of a classification system.
Results:
A total of 167 studies were deemed relevant. Five classification systems were developed based on X-ray: the 9-classification system (0.60%); continuous, segmental, mixed, localized or focal, circumscribed and others (92.81%); hook, staple, bridge, and total types (2.40%); distribution of OPLL (2.40%); and K-line classification (4.19%). Six methods were based on computed tomography scans: free-type, contiguous-type, and broken sign (0.60%); hill-, plateau-, square-, mushroom-, irregular-, or round-shaped (5.99%); rectangular, oval, triangular, or pedunculate (1.20%); centralized or laterally deviated (1.80%); plank-, spindle-, or rod-shaped (0.60%); and rule of nine (0.60%). Classification systems based on 3-dimensional computed tomography were bridging and nonbridging (1.20%) and flat, irregular, and localized (0.60%). A single classification system was based on magnetic resonance imaging: triangular, teardrop, or boomerang. Finally, a variation of methods was used to classify OPLL associated with the dura mater (4.19%).
Conclusions:
The most common method of classification was that proposed by the Japanese Ministry of Health, Labour and Welfare. Other important methods include K-line (+/−), signs of dural ossification, and patterns of distribution.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is defined as ectopic bone formation within the posterior longitudinal ligament. 1 OPLL can result in spinal canal or foraminal narrowing, cause myelopathy or radiculopathy, and increase the risk of spinal cord injury following a traumatic event. It is a multifactorial, degenerative disease in which both environmental and genetic factors contribute to its development, type, and severity. 2,3
Various imaging modalities can be used to assess the extent, shape, thickness, and location of OPLL, including plain radiographs, magnetic resonance imaging (MRI), and computed tomography (CT) scans. The ossification is often classified based on its morphology, distribution, or configuration of the compressed spinal cord. Furthermore, OPLL can be categorized according to its association with the vertebral bodies, intervertebral discs, or the dura mater. The type of OPLL may influence neurological symptoms, other imaging characteristics, treatment strategies, outcomes, disease progression, and risk of surgical complications.
While there are numerous classification systems in the literature, it is unclear how to best categorize various types of OPLL. In addition, there is uncertainty as to what imaging modality is the most reliable for diagnosing and classifying OPLL. It is therefore the objective of this study to conduct a literature review to Summarize various classification systems used to describe cervical OPLL Evaluate the diagnostic accuracy of various imaging modalities and the inter- and intrarater reliability of classification systems.
Methods
Eligibility Criteria
Our review targeted studies on patients with cervical OPLL with or without neurological signs and symptoms of myelopathy. We sought studies that used a classification system to categorize patients based on type of OPLL. Studies were excluded if they stratified patients based on severity of stenosis or occupying ratio (the thickest part of OPLL divided by the anteroposterior diameter of the spinal canal).
Information Sources
Studies were identified using 4 electronic databases: MEDLINE, MEDLINE in Process, EMBASE, and Cochrane Central of Controlled Trials. The last search was run October 5, 2015.
Search
We used the following search terms to search all databases: OPLL AND Cervical. Only studies on humans and written in English or Japanese were considered for inclusion, with no other limits applied.
Study Selection
All abstracts and titles were reviewed independently in an unblinded, standardized manner by 2 of the authors (LT, MK). The abstracts were sorted using predefined inclusion criteria and classified as relevant, possibly relevant, or irrelevant. Any study that included patients with OPLL was further investigated (LT, HN). Full text review of these articles was done to determine whether a classification system was used to define type of OPLL (all authors). Case reports were excluded as well as case series that did not indicate or reference an OPLL classification system. Systematic reviews, opinions, editorials, and commentaries were also excluded.
Data Extraction and Synthesis
The following data was extracted from each included article: patient sample and characteristics, the classification system used to categorize OPLL, the image modality used to diagnose OPLL, and any data on inter- and intrarater reliability.
Reporting
This systematic literature review was formatted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Results
Study Selection
The search yielded a total of 1616 unique citations from Medline, Medline In-Process, EMBASE, and Cochrane Central Register of Controlled Trials. After initial review of abstracts and titles, 845 studies did not meet our inclusion criteria. Following full text investigation, an additional 405 studies were excluded because (1) patients did not have OPLL, (2) a classification system was not used to categorize the type of OPLL, and/or (3) they were systematic reviews or case reports. Furthermore, 199 studies could not be located through the libraries at the University Health Network, University of Toronto, or University of Western Ontario mostly because they were not in English. Seventy-five studies in Japanese were obtained from the library at Nagoya University Graduate School of Medicine; of these, 12 met our inclusion criteria. In total, 167 studies were deemed relevant following this rigorous review process. Figure 1 provides an overview of our search strategy.
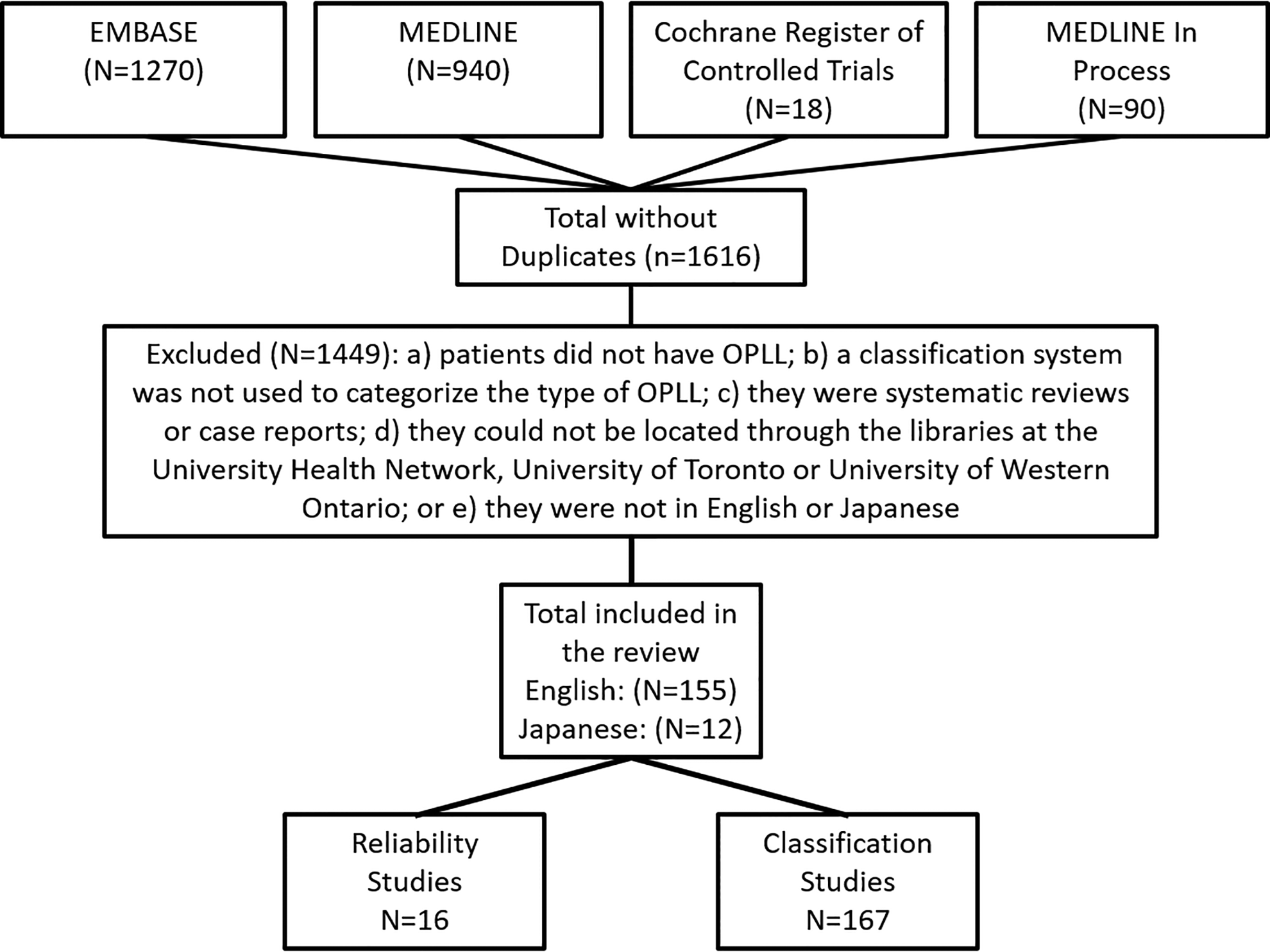
Overview of search strategy.
Study Characteristics
For Objective 1, we identified 167 studies that used a classification system to categorize patients with OPLL. Sample sizes ranged from 5 to 581 patients. Diagnosis and classification of OPLL were based on findings from radiographs, CT scans, MRI, or a combination of modalities. Table 1 summarizes existing classification systems used for OPLL.
A Summary of Studies That Classified Type of OPLL.
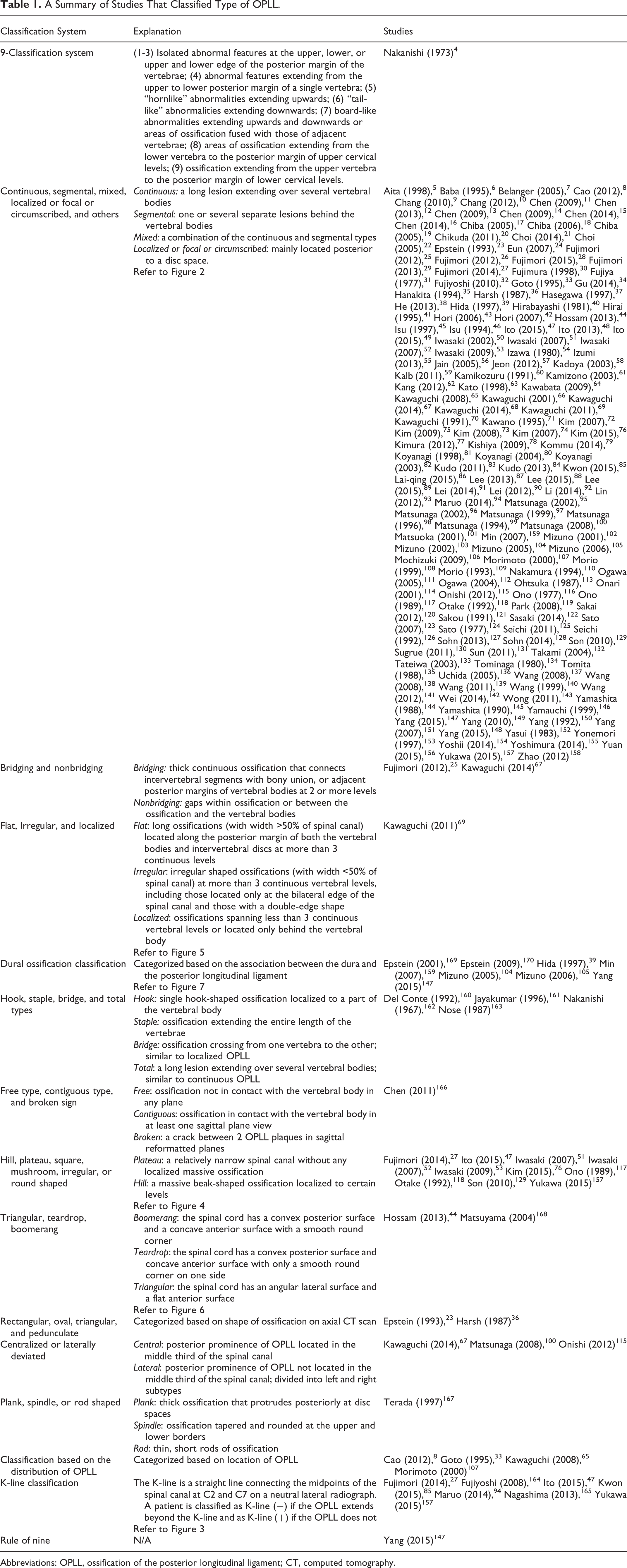
Abbreviations: OPLL, ossification of the posterior longitudinal ligament; CT, computed tomography.
For Objective 2, we retrieved 9 studies that evaluated the inter- or intrarater reliability of classification systems and 7 that discussed correlations between and diagnostic accuracy of various imaging techniques. Table 2 reports the diagnostic accuracy of various imaging modalities and the reliability of several classification systems.
Reliability of Imaging Modalities for Diagnosis and Classification of OPLL.
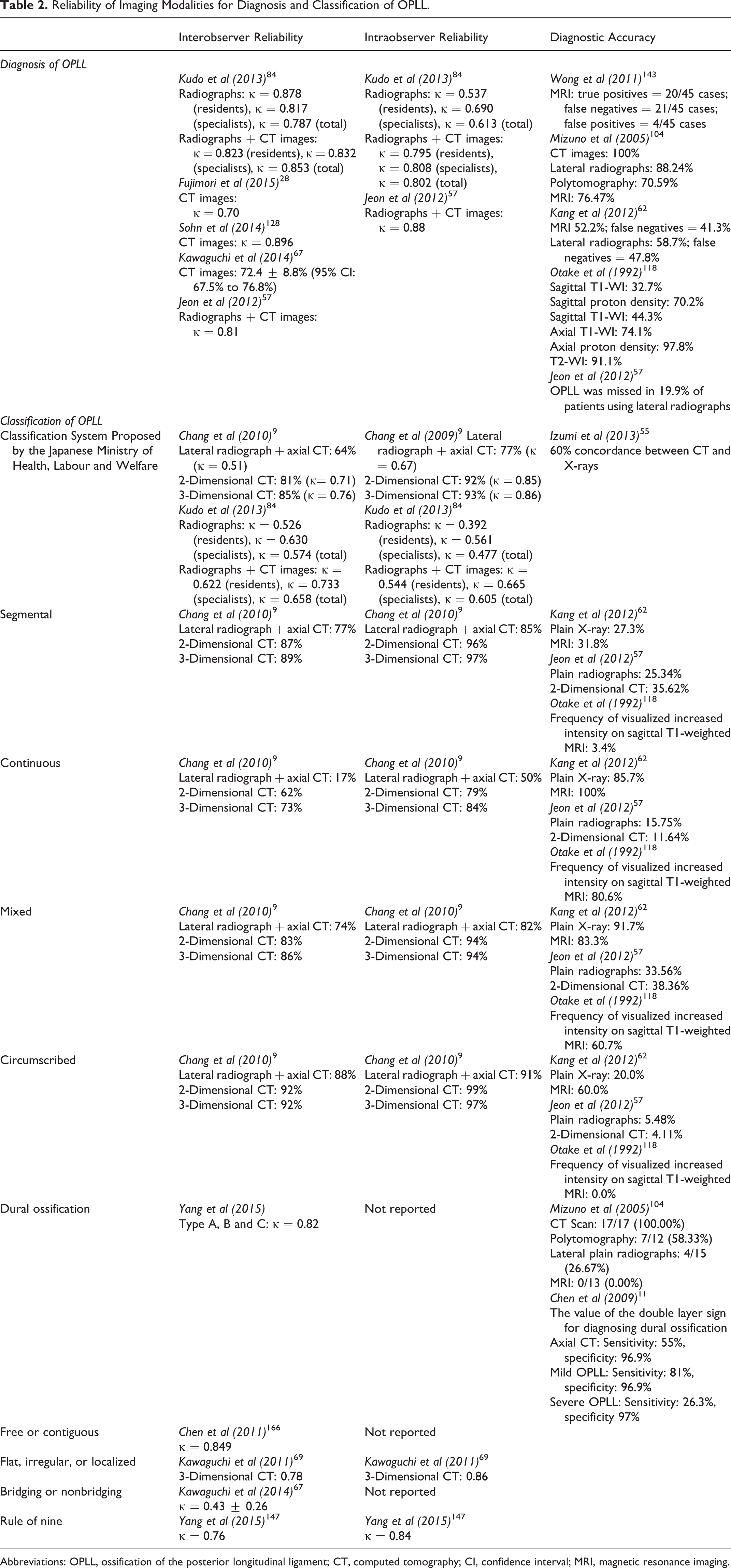
Abbreviations: OPLL, ossification of the posterior longitudinal ligament; CT, computed tomography; CI, confidence interval; MRI, magnetic resonance imaging.
Part A: Classification Systems
Classifications Based on X-Ray
Nine-classification system (0.60% of articles)
Nakanishi et al quantified the incidence of cervical OPLL in 698 asymptomatic subjects. 4 This study classified the type of OPLL into 9 groups based on roentgenographic features: (1-3) isolated abnormal features at the upper, lower, or upper and lower edge of the posterior margin of the vertebrae; (4) abnormal features extending from the upper to lower posterior margin of a single vertebra; (5) “hornlike” abnormalities extending upwards; (6) “tail-like” abnormalities extending downwards; (7) board-like abnormalities extending upwards and downwards or areas of ossification fused with those of adjacent vertebrae; (8) areas of ossification extending from the lower vertebra to the posterior margin of upper cervical levels; and (9) ossification extending from the upper vertebra to the posterior margin of lower cervical levels.
Continuous, segmental, mixed, localized or focal, circumscribed, or other (92.81% of articles)
The Investigation Committee for Ossification of the Spinal Ligaments (part of the Japanese Ministry of Health, Labour and Welfare) established a commonly used classification system for OPLL. 5 -159 This system categorizes OPLL into 4 types: (1) continuous, a long lesion extending over several vertebral bodies; (2) segmental, one or several separate lesions behind the vertebral bodies; (3) mixed, a combination of the continuous and segmental types; and (4) circumscribed, mainly located posterior to a disc space (Figure 2). In some studies, the term circumscribed was replaced by localized, solitary, or herniated/discal type (ie, ossification surrounding intervertebral disc herniation) and the term segmental by fragmented. In addition, a study by Sohn et al categorized segmental OPLL into single or multilevel. 128 Across 135 studies (n = 9150), 2376 (25.97%) patients were diagnosed with continuous, 3135 (34.26%) with segmental, 2971 (32.47%) with mixed, and 668 (7.30%) with either localized or circumscribed OPLL.

Classification system proposed by the Japanese Ministry of Health, Labour and Welfare: continuous, segmental, mixed, and localized.
A study by Ito et al divided OPLL type into 6 groups: covered disc, covered vertebra, unconnected vertebra, connected vertebra (continuous), connected vertebra (localized), and other. 49 The covered disc and covered vertebra groups were defined as ossification of the cranial or caudal vertebra with incomplete or complete coverage of the adjoining intervertebral disc, respectively. The unconnected vertebra group consisted of complete ossification of 2 adjacent vertebral bodies and the connecting intervertebral disc, with potential ossification of other cranial or caudal vertebrae or discs. The definitions for connected vertebra, either continuous or localized, were similar to those defined above. The other group had vertebrae with osteophytes, disc ossification, or no problematic features. In another study by Ito et al, OPLL morphology was classified as “connection department,” “coating part,” and “nonconnection department.” 48 The “connection department” included both continuous and localized OPLL, whereas the “coating part” included either the tip of continuous or segmental OPLL.
Hook, staple, bridge, or total type (2.40% of articles)
Three studies used a classification system proposed by Nakanishi et al: type I or hook, type II or staple, type III or bridge, and type IV or total/continuous. 160 -163 Hook-type OPLL appears as a single hook-shaped ossification localized to a part of the vertebral body, whereas staple type develops as a lesion extending the entire length of the vertebrae. 161,163 Bridge type is similar to localized OPLL, with the ossification crossing from one vertebra to the other, whereas total type is analogous to continuous OPLL.
Classification based on the distribution and extent of OPLL (2.40% of articles)
Two studies categorized patients with OPLL based on the distribution of OPLL. 33,65 A study by Goto et al classified the type of OPLL as upper, lower, or wide. 33 Upper type was defined as ossification involving the upper half of the cervical spine (C1-C3), lower type as ossification involving the lower half of the cervical spine (C4-C7), and wide type as ossification involving upper and lower levels of the cervical spine (C1-C7). In a study by Kawaguchi et al, patients were categorized into a C1(+) and C1(−) group; the C1(+) group had ossified lesions behind the dens at the level of the C1 lateral mass. 65
Two other studies classified OPLL based on its extent. 8,107 Morimoto et al divided their patients with OPLL into 2 groups: multilevel ossification that spanned more than 3 vertebral body lengths and localized OPLL. 107 Another study classified local OPLL as less than or equal to 2 levels, and continuous as greater than 2 levels. 8
K-line classification (4.19% of articles)
Seven studies categorized patients into a (+) or (−) K-line group. 27,47,85,94,157,164,165 The K-line was originally described by Fujiyoshi et al as a straight line connecting the midpoints of the spinal canal at C2 and C7 on a neutral lateral radiograph. 164 A patient is classified as K-line (−) if the OPLL extends beyond the K-line and as K-line (+) if the OPLL does not (Figure 3).
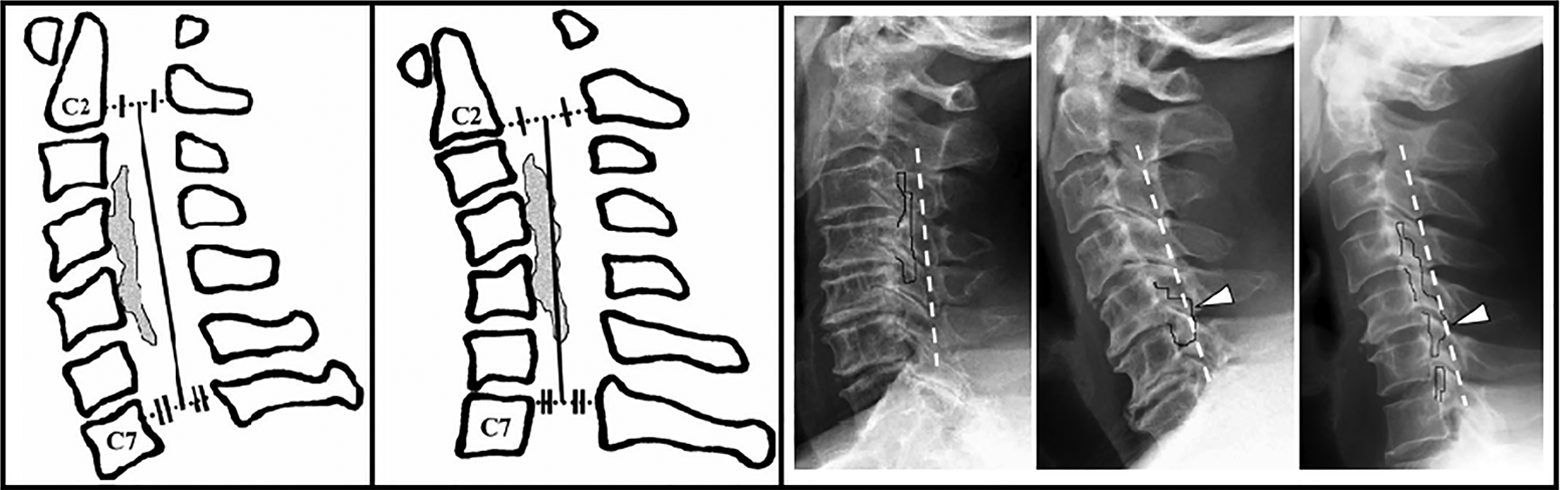
The K-line.
Classifications Based on Computed Tomography
Free type, contiguous type, or broken sign (0.60% of articles)
A single study classified OPLL plaques into 3 categories according to multiplanar reformats of CT sagittal images: free type, contiguous type, and broken sign. 166 A free-type plaque was defined as ossification not in contact with the vertebral body in any plane. On the other hand, a contiguous plaque is in contact with the vertebral body in at least one sagittal plane view. A broken sign was defined as a crack between 2 OPLL plaques in the sagittal reformatted planes.
Hill, plateau, square, mushroom, irregular, or round shaped (5.99% of articles)
Ten studies used hill, plateau, mushroom, irregular, or round shaped to classify the type of OPLL (Figure 4). 27,47,51 -53,76,117,118,129,157 Plateau-shaped ossification is characterized by a relatively narrow spinal canal without any localized massive ossification. 52 In contrast, hill-shaped OPLL appears as a massive beak-shaped ossification localized to certain levels. Plateau-shaped ossification is often found in segmental- and in most cases of continuous- and mixed-type OPLL, whereas hill-shaped OPLL is typically associated with circumscribed ossification. In a study by Otake et al, OPLL was classified into 3 types based on its shape on axial MR images: (1) square with parallel lines tangential to the bilateral margins of the ossified lesion, (2) mushroom with ventrally crossing lines, and (3) hill with dorsally crossing lines. 118 Mushroom shaped was also used to define the type of OPLL in a study by Son et al. 129 Finally, Ono et al used mushroom, irregular, and round to categorize the shape of ossification. 117
Classification of ossification morphology: hill, plateau, and mushroom shaped.
Rectangular, oval, triangular, or pedunculate (1.20% of articles)
Two studies classified OPLL based on the shape of the mass on an axial CT scan: rectangular, oval, triangular, or pedunculated. 23,36 No further explanation was provided of these categories.
Centralized or laterally deviated (1.80% of articles)
Three studies classified the type of OPLL as central or laterally deviated based on its position on an axial CT scan. 67,100,115 OPLL was categorized as central if the posterior prominence of the OPLL was located in the middle third of the spinal canal. The lateral-type OPLL was further divided into left and right subtypes.
Plank, spindle, or rod shaped (0.60% of articles)
A single study used 3-dimensional CT image reconstruction to visualize the configurations of OPLL in the cervical spine. 167 The OPLL was classified as plank, spindle, or rod shaped. In plank-shaped OPLL, the region of ossification is thick and protrudes posteriorly at disc spaces. Furthermore, the ossified ligament typically abuts the vertebral bodies; however, in some cases, there may be a gap between the OPLL and the posterior margins of the vertebral bodies. Spindle-shaped OPLL is tapered and rounded at the upper and lower borders. Finally, patients with rod-shaped OPLL have relatively thin, short rods of ossification typically confined to the center of the posterior margin of the vertebral body and discontinued at the intervertebral discs.
Rule of nine (0.60% of articles)
A new method of classifying OPLL was developed to determine whether the ligament can be surgically resected completely and safely. 147 On axial CT scans, 2 points were marked at the junction of the vertebral body and pedicle and a straight “baseline” was drawn between the points. The space between the posterior margin of the vertebral body and the root of the spinous process was divided into 3 equal parts by 2 lines, the safety and danger lines. The space (1) between the baseline and safety lines was the safety zone, (2) between the safety and danger lines was the intermediate zone, and (3) below the danger line was the danger zone. The baseline was also divided into 3 equal parts by 2 perpendicular lines, creating a 9-square grid.
Classifications Based on 3-Dimensional Computed Tomography
Bridging or nonbridging (1.20% of articles)
In 2 studies, OPLL was classified as bridging or nonbridging using 3-dimensional CT scans. 26,67 Bridging OPLL was defined as a thick continuous ossification that connected (1) intervertebral segments with bony union or (2) adjacent posterior margins of vertebral bodies at 2 or more levels. In contrast, patients with nonbridging OPLL had gaps within the ossification or between the ossification and vertebral bodies. A third type of OPLL, stalagmite type, was identified in patients with nonbridging OPLL due to differences in range of motion. 26 In this type of OPLL, the ossification originates from the lower vertebra and progresses continuously through and behind the upper vertebral body without contact, imitating stalagmite geological formations.
Kawaguchi et al used another classification system to describe all vertebral and intervertebral levels where OPLL was greater than 2 mm in width: (1) a dot (“.”) is placed when the OPLL is disconnected, (2) a slash (“/”) is used when the OPLL lesion is beyond the intervertebral level without any bridge formation to the adjacent vertebral body, (3) a bar (“-”) is drawn when the ossification is beyond the intervertebral level with bridge formation to the adjacent vertebral body, and (4) the vertebral body is circled when the OPLL lesion is not attached to it. 67
Flat, irregular, or localized (0.60% of articles)
Using 3-dimensional CT, OPLL can be classified into 3 types: flat, irregular, and localized (Figure 5). 69 In flat OPLL, long ossifications are located along the posterior margin of both the vertebral bodies and intervertebral discs at more than 3 continuous levels. The width of ossification is more than 50% of the spinal canal. The irregular type of OPLL consists of irregular-shaped ossifications at more than 3 continuous vertebral levels, including those located only at the bilateral edge of the spinal canal and those with a double-edge shape. The width of the ossification is less than 50% of the spinal canal. Finally, in the localized type, ossifications span less than 3 continuous vertebral levels or are located only behind the vertebral body.

Novel classification system proposed by Kawaguchi et al (2011) using 3-dimensional computed tomography.
Classification Based on Magnetic Resonance Imaging
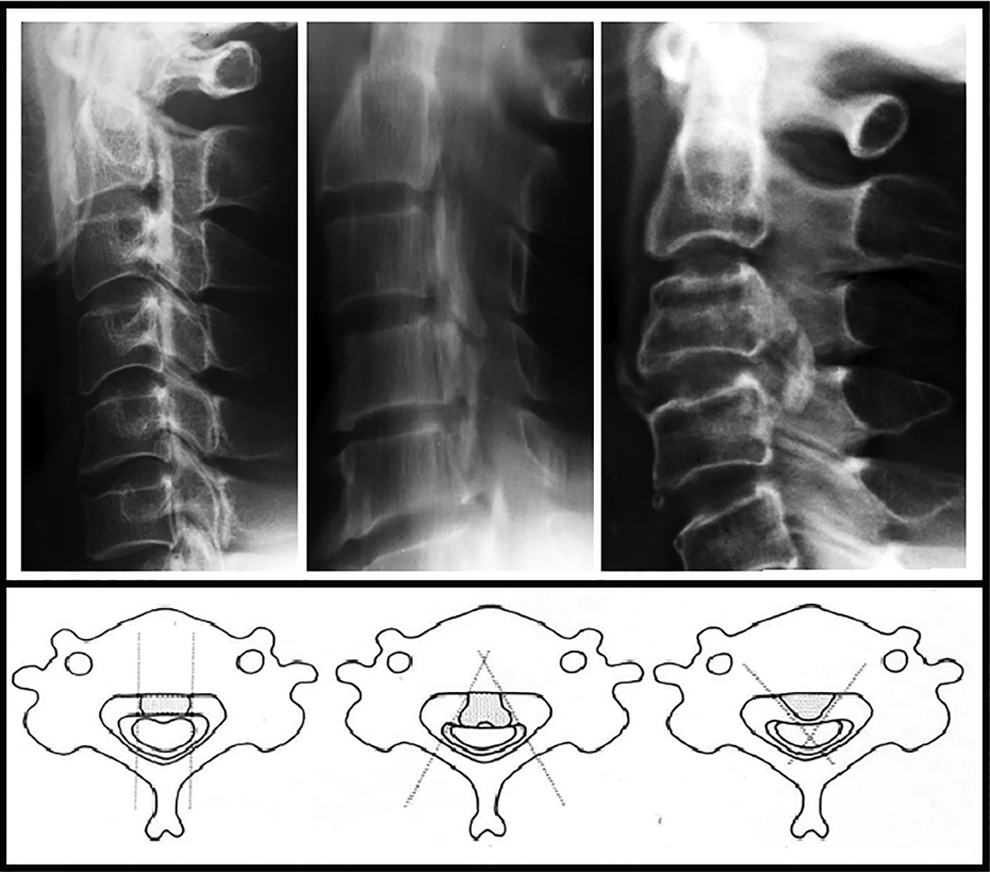
Triangular, teardrop, or boomerang (1.20% of articles)
Two studies classified OPLL into 3 types based on the configuration of the compressed spinal cord on T2-weighted axial images: boomerang, teardrop, and triangular (Figure 6). 44,168 In the boomerang type, the spinal cord has a convex posterior surface and a concave anterior surface with a smooth round corner. The teardrop type has a convex posterior surface and concave anterior surface with only a smooth round corner on one side, and the triangular type has an angular lateral surface and a flat anterior surface.
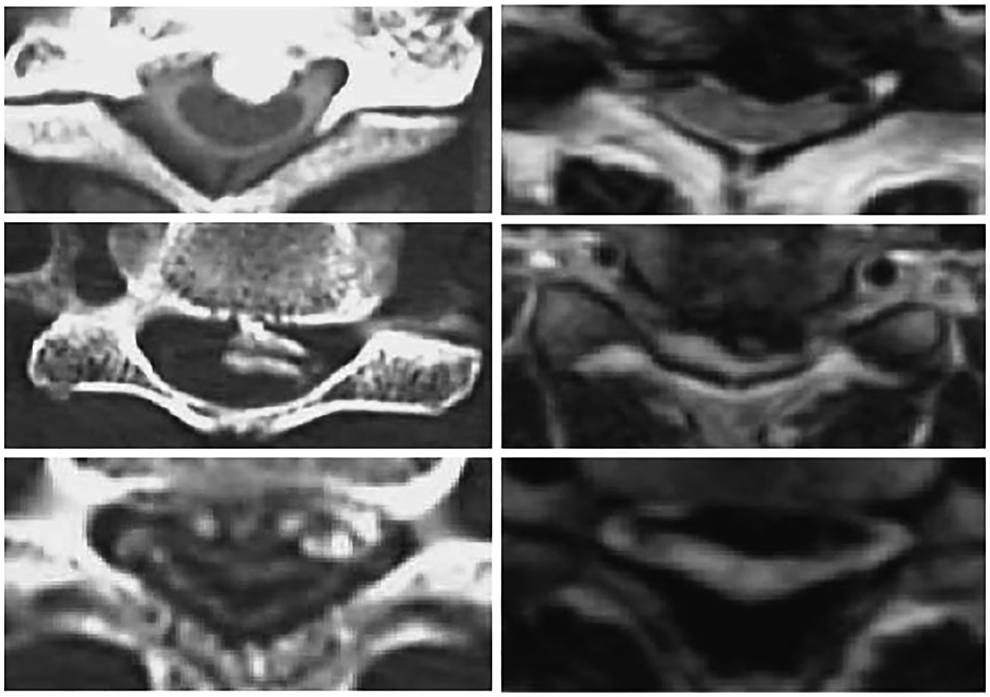
Classification of OPLL based on the configuration of the compressed spinal cord: triangular, teardrop, and boomerang.
Classifications Based on Association With the Dura Mater
Dural ossification (4.19% of articles)
Seven studies classified OPLL based on its association with the dura mater (Figure 7). 39,104,105,148,159,169,170 There are several implications to correctly identifying patterns of dural ossification, including reducing the risk of cerebrospinal fluid leakage after anterior decompression. In the original study, Hida et al defined a single-layer sign as a large focal mass of uniformly hyperdense OPLL and a double-layer sign as a central hypodense line of hypertrophied ligament between an anterior rim and a posterior rim of hyperdense ossification (ie, OPLL involving the posterior aspect of the vertebral body and intradural ossification). 39
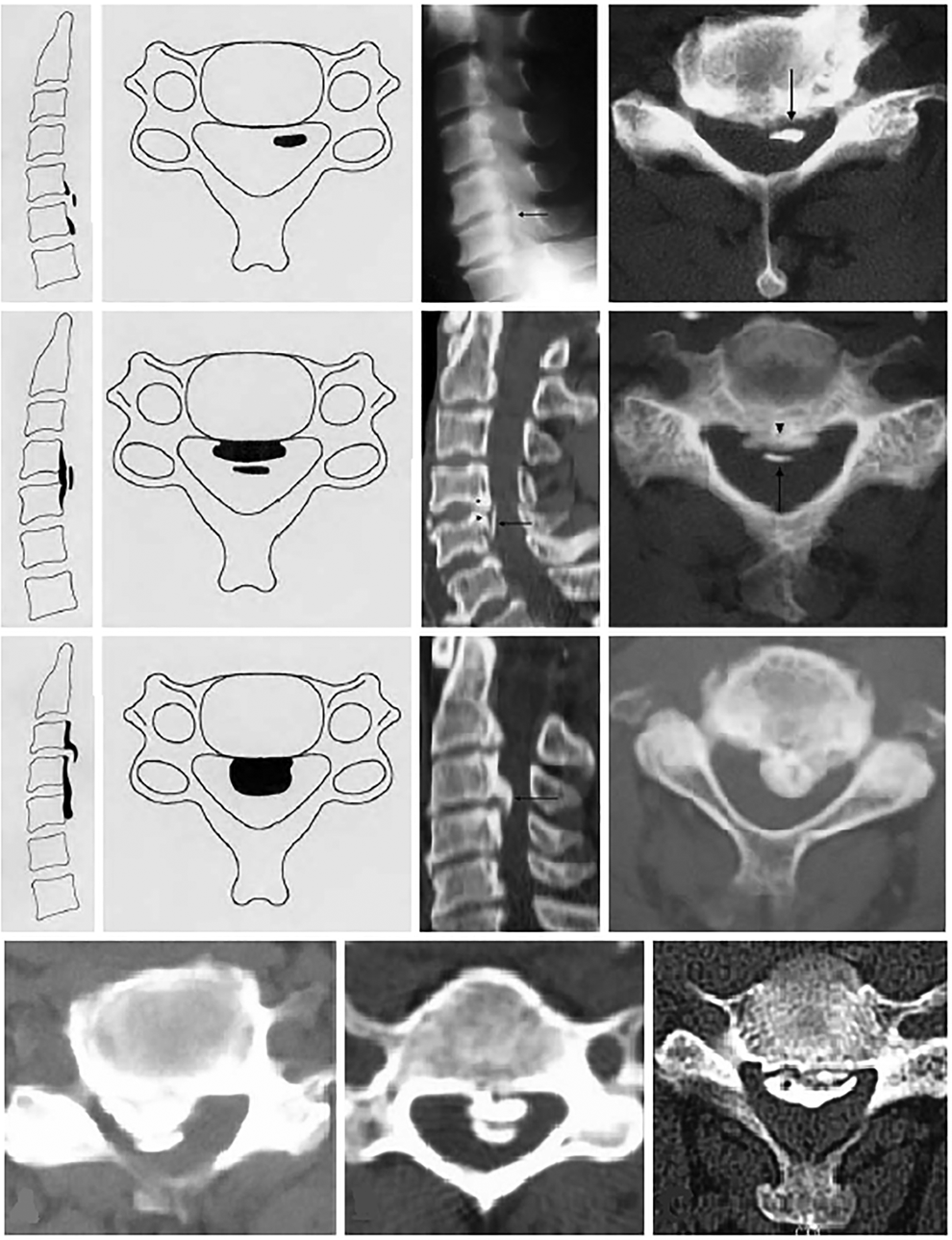
Types of dural ossification.
In 2 studies by Mizuno et al, dural ossification was further classified into 3 types based on its shape and association with the OPLL: (1) an isolated type where the dural ossification is not related to the OPLL, (2) a double-layer type where the dural ossification and OPLL are separated by an epidural space, and (3) an en bloc type where there is en bloc ossification of the dura mater and OPLL, with a meningeal tail sign on a sagittal slice. 104,105
The double-layer sign was further characterized into types A, B, and C based on morphological features of the ossified and central hypodense mass. 148 In type A, the hypodense mass is crescent shaped and the OPLL is much more extensive than the dural ossification. Type B is a short straight hypodense line less than or equal to half of the base width of the vertebrae. Finally, in type C, the dural ossification is much more extensive than the OPLL, and the central hypodense mass is a long straight line that extends more than half of the base width of the vertebrae.
Finally, Epstein et al characterized 2 signs of dural penetration: the modified single-layer sign and the double-layer sign. 169 The modified single-layer sign was characterized by a laterally curved and irregular mass of OPLL with a unique hook-like configuration. A third sign, the smooth-layer sign, indicated an intact dura and was defined as a more classic OPLL without a hook-like C sign.
Part B: Inter- and Intrarater Reliability
Reliability is generally assessed by computing either correlations between continuous variables or κ values for categorical variables. Criteria for strength of agreement are as follows: a κ of 0.81 to 1.00 as almost perfect, 0.61 to 0.80 as substantial, 0.41 to 0.60 as moderate, 0.21 to 0.40 as fair, and 0.00 to 0.20 as slight agreement. 171
Reliability of OPLL Diagnosis Using Various Imaging Modalities
The reliability of OPLL diagnosis was reported by 5 studies. 28,57,67,84,128 In a study by Kudo et al, 8 spine surgery specialists and 8 orthopedic residents were instructed to diagnose either OPLL or cervical spondylotic myelopathy using radiographs only and then both radiographs and CT images. 84 To test intraobserver reliability, the same individuals were asked to reanalyze the images at least 24 hours after the first evaluation. In the second round, the interobserver reliability was κ = 0.787 with radiographs only (κ = 0.817 among specialists, κ = 0.878 among residents) and κ = 0.853 using both radiographs and CT images (κ = 0.832 among specialists and κ = 0.823 among residents). These values were higher than interobserver reliabilities after first round of analysis. Intraobserver reliability of diagnosis was κ = 0.613 (κ = 0.690 among specialists, κ = 0.537 among residents) using only radiographs and was κ = 0.802 (κ = 0.795 among specialists, κ = 0.808 among residents) using both radiographs and CT images. In 3 other studies, diagnosis agreement using CT scans was κ = 0.70 to 0.896 between a radiologist(s) and an experienced orthopedic spine surgeon. 28,67,128
Wong et al analyzed the agreement between MRI and CT scans for OPLL diagnosis. 143 Forty-five patients were first evaluated by MRI and then assessed by follow-up CT scans to confirm the presence or absence of OPLL. Of the 45 cases, 20 were correctly diagnosed using MRI (true positive), whereas in 21 cases, OPLL was not identified (false negative; sensitivity of 49%). Furthermore, 4 patients were diagnosed as having OPLL on MRI when it was not detected on CT imaging (false positive; positive predictive value of 83%). Mizuno et al compared the ability of various neuroimaging modalities to diagnose OPLL in 17 patients, including lateral plain radiography, thin slice sagittal polytomography, CT scans, and T2-weighted MRI. 104 The best modalities were bone window CT scanning and lateral plain radiography, which correctly identified 100.00% and 88.24% OPLL cases, respectively. Polytomography detected OPLL in 12 of 17 patients (70.59%) and MRI in 13 of 17 cases (76.47%). Interestingly, the 4 cases that were incorrectly diagnosed by MRI were segmental OPLL as the ossification could not be differentiated from the posterior spur or the degenerated hypertrophied posterior longitudinal ligament.
A single study compared the diagnostic accuracy of CT scans versus MRI and plain lateral radiographs. 62 MRI and plain lateral radiographs were only able to detect OPLL in 52.2% and 58.7% of cases, respectively. The false negative rate on MRI was 41.3% and on plain lateral radiographs was 47.8%. On MRI, the main misdiagnosis was hypertrophied posterior longitudinal ligament, whereas on plain lateral radiographs, any OPLL less than 2.99 mm thickness was not detected.
Finally, a study by Otake et al reported the likelihood of detecting ossified lesions of variable thickness on T1-weighted, proton density, and T2-weighted MRI. 118 In the sagittal plane, OPLL was more frequently identified on proton density imaging (70.2%) than on T1- (32.7%) and T2-weighted (44.3%) images. On T1- and T2-weighted images, ossification may be mistaken for cerebrospinal fluid or vertebral bodies, respectively. The chance of detecting ossification increased with the thickness of the lesion. OPLL was better detected on axial imaging: (1) 74.1% on T1-weighted MRI, (2) 97.8% on proton density imaging, and (3) 91.1% on T2-weighted imaging. Increased intensity within the ossified lesion was visualized in 61 of 147 patients on T1-weighted imaging and more commonly seen in patients with thick ossification.
The Reliability of the Classification System Proposed by the Japanese Ministry of Health, Labour and Welfare
Two studies evaluated the reliability of the classification system proposed by the Japanese Ministry of Health, Labor and Welfare 9,84 and 4 compared the diagnostic accuracy of various imaging modalities. 55
In a study by Chang et al, 5 spine surgeons were required to classify the type of OPLL in 108 patients using lateral radiographs, axial CT scans, and 2- and 3-dimensional reconstructed CT images. 9 The interobserver reliability of the classification system ranged from κ = 0.51 on lateral radiographs and axial CT scans to κ = 0.76 on 3-dimensional CT. As reported by Kudo et al, the interobserver reliability was κ = 0.574 using just radiographs and κ = 0.658 using both radiographs and CT images. 84 Finally, in a study by Izumi et al, the classification using X-rays corresponded with that of CT images in 9 out of 15 cases (60.0%). 55
All types of OPLL were better classified using only 2-dimensional (continuous: 62%, segmental: 87%, mixed: 83%, circumscribed: 92%) and 3-dimensional reconstructed CT images (continuous: 73%, segmental: 89%, mixed: 86%, circumscribed: 92%) than using lateral radiographs in combination with axial CT images (continuous: 17%, segmental 77%, mixed: 74%, circumscribed: 88%). 9 The diagnostic accuracy of lateral radiographs and MRI was further explored by Kang et al. 62 Plain X-rays were able to better classify continuous (85.7%) and mixed (91.7%) OPLL compared to segmental (27.3%) and localized (20.0%) types. Diagnostic accuracy on MRI was slightly different: 100% in continuous, 31.8% in segmental, 83.3% in mixed, and 60.0% in localized OPLL. The percentage of false negatives was higher in segmental (68.2% on MRI and 72.7% on lateral radiographs) and localized (40.0% on MRI and 80.0% on lateral radiographs) OPLL than in the continuous (0.0% on MRI and 14.3% on lateral radiographs) and mixed (16.7% on MRI and 8.3 on lateral radiographs) types. Increased signal intensity on T1-weighted images within the ossified ligament was more frequently seen in patients with continuous (80.6%) and mixed (60.7%) lesions than in those with segmental (3.4%) and circumscribed (0.0%) OPLL. 118
Intraobserver reliability of the classification system was κ = 0.477 using radiographs, κ = 0.605 to 0.67 using a combination of radiographs and CT scans, κ = 0.85 using 2-dimensional CT, and κ = 0.86 using 3-dimensional CT scans. 84 The intraobserver reliability was high for segmental, mixed, and circumscribed OPLL using lateral radiographs and axial CT (85%, 82%, and 91%, respectively), 2-dimensional CT (96%, 94%, and 99%), and 3-dimensional (97%, 94%, and 97%) CT. 84 Detection of continuous OPLL, however, had low intraobserver reliability using lateral radiographs and axial CT (50%), but good reliability using 2- (79%) and 3-dimensional (84%) CT.
Reliability of Identifying Dural Ossification
A single study calculated the reliability of correctly identifying dural ossification, 148 whereas 2 studies reported the diagnostic accuracy of various imaging modalities. 13,104 Yang et al reported a kappa value of κ = 0.82 for classifying the 3 types of dural ossification. 148 A second study explored the ability of various neuroimaging modalities to detect OPLL and dural ossification in 17 patients, including lateral plain radiography, thin slice sagittal polytomography, CT scans, and T2-weighted MRI. 104 The results were (1) bone-window CT scanning was able to detect dural ossification in all 17 cases of OPLL, (2) polytomography could only identify dural ossification in 7 out of 12 cases (58.3%), (3) only 4 of 15 cases of dural ossification were detected on lateral plain radiographs, and (4) MRI could not distinguish dural ossification in any of the 13 OPLL patients. A third study evaluated the value of the double-layer sign for the diagnosis of dural ossification. 13 On axial CT images, the sensitivity of this method was 55% and the specificity was 96.9%. The sensitivity was much higher in patients with mild OPLL (occupying ratio <60%, sensitivity = 81%) and lower in patients with severe OPLL (occupying ratio ≥60%, sensitivity = 26.3%).
Reliability of Other Classification Systems
The reliability of 4 other classification systems was evaluated. The interobserver reliability of classifying the type of attachment as free or contiguous was κ = 0.849 between a radiologist and experienced spine surgeon, indicating high reliability of this method. 166
The interobserver reliability among 7 senior spine surgeons was κ = 0.43 ± 0.26 for the bridging and nonbridging types of OPLL proposed by Kawaguchi et al. 67
The mean inter- and intraobserver reliabilities of the “rule of nine” classification system were κ = 0.76 and κ = 0.84, respectively. 147
Using 3-dimensional CT images, the inter- and intraobserver reliabilities were κ = 0.78 and κ = 0.86, respectively, for classifying patients with flat, irregular, or localized OPLL. 69
Discussion
This study summarizes various classification systems used to categorize patterns of cervical OPLL. Our results indicate that OPLL can differ substantially with respect to its shape, extent, and distribution and the configuration of the compressed spinal cord. Furthermore, the ossification can be associated with the dura mater and different components of the spinal column. Appropriate classification of OPLL is critical as there may be significant variations in neurological presentation, surgical outcomes, disease progression, and risk of complications across subtypes of OPLL. Based on our review, the most common method of classification was that proposed by the Japanese Ministry of Health, Labor and Welfare (continuous, segmental, mixed, localized, or circumscribed). Other important means of categorizing OPLL include using the K-line (+/−), identifying signs of dural ossification, and by distribution. In terms of reliability and accuracy, our results indicate that OPLL is best diagnosed and classified using 2- or 3-dimensional CT images. 9 In addition, the reliability is high for Yang’s classification of dural ossification and Chen’s free or contiguous method. 148,166
Patients with different types of OPLL may have different risks of developing myelopathy or of experiencing a traumatic spinal cord injury. In a study by Matsunaga et al, laterally deviated OPLL on an axial MRI or CT scan was an important predictor of myelopathy development (P = .021). 100 Chang et al evaluated differences in type of OPLL (continuous, mixed, segmental, or localized) between patients with no symptoms, neck pain, or radiculopathy and those with myelopathy. 10 In the myelopathy group, 15% of subjects had localized ossification, 35% segmental, 24% continuous, and 26% mixed OPLL. This is in contrast to the asymptomatic, neck pain, or radiculopathy group: 8% localized type, 60% segmental, 8% continuous, and 24% mixed. In a third study, however, the type of OPLL (segmental, continuous, or mixed) was not predictive of progressive myelopathy. The risk of trauma-induced myelopathy was significantly higher in patients with mixed-type OPLL than in those with segmental or continuous type. 96 However, this finding could not be replicated in a study by Onishi et al, which reported no risk difference among patients with segmental, continuous, mixed, or localized OPLL. 115 The ratio of central to laterally deviated ossification was also similar between a spinal cord injury group and a cervical myelopathy (control) group. 115
Different subtypes of OPLL may also vary in terms of neurological symptoms, preoperative myelopathy severity, occupying ratio, space available for the spinal cord, range of motion, and segmental stability. A single study compared symptoms among OPLL subtypes (continuous, segmental, or mixed) using the visual analog scale (VAS) and Japanese Orthopedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ). 122 Based on their results, neck function on the JOACMEQ in patients with continuous OPLL was significantly lower than those with mixed-type ossification. However, there were no significant differences in upper and lower extremity function, urinary function, quality of life, shoulder stiffness, and neck/arm pain among subtypes. Furthermore, preoperative JOA was similar between patients with mixed, segmental, continuous, and localized OPLL. 44,154 Interestingly, patients with bridging OPLL were more stable over a 2 year monitoring period than those with nonbridging ossification. 26
Mixed and continuous types of OPLL are associated with a greater percentage of spinal canal stenosis, a smaller space available for the spinal cord, an increased compression ratio, and a higher occupying ratio compared to patients with segmental or localized ossification. 30,59,115,139 Furthermore, patients with mixed or continuous OPLL have a greater dynamic OPLL distance than those with segmental ossification. In contrast, a single study reported no difference in the space available for the spinal cord or occupying ratio in patients with mixed, segmental, or continuous OPLL. 32 In addition, Koyanagi et al concluded that patients with segmental OPLL have significantly narrower diameters at C3-C7 than patients with continuous or mixed ossification. 82 K-line (−) OPLL is associated with decreased C2-C7 range of motion and increased occupying ratio, extension/flexion ratio, and thickness. 47,164,165 Moreover, a greater percentage of patients with K-line (−) OPLL are compressed at flexion, whereas those with K-line (+) are more likely to be compressed at extension. 47
Range of motion also varies across subtypes of OPLL. In a study by Fujimura et al, patients with continuous ossification had reduced range of motion as compared to those with mixed, segmental, or localized OPLL. 30 Bridging OPLL is also associated with smaller intervertebral range of motion in both anteroposterior flexion and axial rotation compared to nonbridging OPLL. 26 Furthermore, those with stalagmite nonbridging ossification had significant smaller anteroposterior flexion than other nonbridging types. Yoshii et al concluded that these mobile segments without complete bridging were the areas of greatest spinal cord compression. 154
Patients with different types of OPLL may also vary with respect to surgical outcomes, progression rates, and risk of complications. Several studies have evaluated surgical outcomes in patients with different types of OPLL. For example, patients with K-line (+) OPLL may have significantly higher recovery rates and postoperative JOA scores than patients with K-line (−) OPLL. 164 Hill-shaped OPLL (vs plateau-shaped) was also predictive of worse recovery rates following surgery in a single study. 51 Finally, according to Matsuyama et al, patients with triangle-shaped cord compression have significantly lower postoperative JOA scores and reduced recovery than those with boomerang- or tear-shaped compression. 168 In contrast, type of OPLL (continuous, mixed, segmental, or localized) and presence of dural ossification were not associated with surgical outcomes. 13,21,101,112 Further investigation is required to determine important OPLL predictors of outcome in patients undergoing surgery for OPLL-related myelopathy.
Progression of OPLL was defined as (1) an increase in the longitudinal extent of the ossification by 2 mm or more, (2) an increase in the thickness or sagittal extent of the ossification by 2 mm or more, (3) appearance of a new lesion, and/or (4) the bridging of 2 or more existing lesions to form a continuous segment. This progression can significantly reduce the space available for the spinal cord, cause neurological deterioration, and result in new debilitating signs and symptoms. It is therefore essential to identify patients at high risk of progression, implement appropriate preventative surgical strategies, and regularly monitor these patients following surgery. Five studies evaluated important predictors of OPLL progression and reported that patients with mixed or continuous OPLL were at a higher risk of progression than those with segmental ossification. 19,40,43,50,66
Finally, certain types of OPLL may be predictive of surgical complications. In particular, patients with dural ossification are at a higher risk of cerebrospinal fluid leakage following anterior cervical surgery as it is technically difficult to separate the posterior longitudinal ligament from an ossified dura. 13 Clinicians must identify these high-risk patients and implement rigorous preventative strategies to avoid cerebrospinal fluid leakage and damage to the spinal cord and nerve roots (ie, anterior floating method or separation of ligament from dural ossification through a thin layer of nonossified ligament). Furthermore, surgeons must appropriately educate their patients and be prepared to manage leaks either through direct dural repair, lumbar drains, or chemical seals. Based on 3 studies, patients with a double-layer sign are more likely to have a dural defect than patients with a single-layer sign. 39,159,169 In contrast, there is no difference in the rate of dural penetration between patients with a single-layer sign versus those with no sign. 159 Using the classification system developed by Yang et al, patients with type C dural ossification are at a much higher risk of cerebrospinal fluid leakage than patients with type A or B, and those with type B are at a higher risk than patients with type A. 148 Finally, Epstein et al demonstrated a moderate correlation between her modified single-layer with C sign and dural penetration. 169
While these categorizations are important to distinguish between potential pathological differences, they are based on conceptual and theoretical factors. In practice, it is not always a simple endeavor to categorize OPLL into a specific group. These classifications would be much more useful if they were further supported by other imaging factors, clinical findings, and neurological features.
Conclusions and Knowledge Gaps
This study has identified substantial heterogeneity in the methodology used to diagnose and classify OPLL. Based on this review, OPLL is best diagnosed using 2- or 3-dimensional CT imaging. Several published studies, however, have not used these modalities to identify ossification; as a result, OPLL may be either underdiagnosed or mistaken for milder forms of degenerative calcification. The lack of a standardized and reliable classification system prevents clinicians and researchers from addressing key questions surrounding the natural history, evaluation, and management of OPLL and outcomes related to various interventions. Future studies should use this review as a basis for developing a more reliable classification system for OPLL; given the heterogeneity in presentation, the term “OPLL-spectrum disorder” may be valuable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.