
Abstract
Study Design
Retrospective cohort study.
Objectives
To identify whether thresholds exist beyond which operative duration or age increases risks for complications among patients ≥65 years undergoing elective spine surgery.
Methods
Elective inpatient spine procedures unrelated to infection/trauma/tumor diagnoses in patients <65 years recorded in the 2006-2019 American College of Surgeons National Surgical Quality Improvement database were identified. Univariate analyses was used to compare 30 day complication rates among 5 operative duration and age-stratified groups. To quantify the risk of prolonged operative duration on complications, multivariate analyses were performed controlling for confounders. A generalized linear model was used to assess the individual and combined effect strength of age and operative duration on complication rates.
Results
Among 87,705 patients stratified by operative duration, 30 day complication rates rose nonlinearly as operative duration increased, with a sharp rise after 4.0-4.9 hours (28.3% at 4.0-4.9 hours, 51.7% at ≥5 hours, P < .001). Multivariate analysis found operative duration was independently associated with increased risk of overall complications (odds ratio 1.10→1.69, P < .001) and medical complications (odds ratio 1.19→1.98, P < .001). Although complication rates rose by age (all P < .001), age was not independently predictive of overall complications within any operative duration group on multivariate analysis. Operative duration had a greater effect (η2P = .067) than age (η2P = .003) on overall complication rates.
Conclusions
Increased operative duration was strongly associated with 30 day complication rates, particularly beyond a threshold of 5 hours. Furthermore, operative duration had a notably larger effect on overall complication rates than age.
Keywords
Introduction
The 2020 U.S. Census reported that 54.1 million Americans are now aged ≥65 years, 1 and this demographic is projected to be ∼ 84 million people by 2050.2,3 Older individuals are especially susceptible to degenerative spine disease, and virtually all individuals ≥60 years exhibit degenerative changes on magnetic resonance imaging. 4 When indicated, spine surgery in elderly patients is effective at improving quality of life;5,6 however, older patients harbor more comorbidities and are at greater risk of complications after spine surgery than nonelderly patients.7-9
It is well established that prolonged operative and anesthesia duration are associated with increased postoperative complications.10-15 Within the field of spine surgery, Hersey et al 16 identified that longer operative duration was associated with more complications among patients ≥65 years undergoing posterior lumbar fusion procedures. However, a large-scale, multi-institutional analysis characterizing an operative duration threshold that portends significantly increased postoperative complications has yet to be identified. Likewise, it is unknown whether a similar threshold exists for age, whereby excess complications arise as a consequence of advanced age at surgery. Additionally, a direct analysis evaluating whether age or operative duration is the more influential risk factor among elderly spine surgery patients also remains unexplored.
As the population ages, it is imperative to identify criteria rendering higher rates of postoperative complications to help guide clinical decision making for elderly patients undergoing elective spinal surgeries. In this study, we expanded the current knowledge by (1) employing the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP), a large multi-institutional database, to increase the rigor of analysis, and (2) expanding the demographic to incorporate all elective spinal procedures. Because age and operation duration demonstrate known impacts on complication rates, we examined whether operative duration had a threshold after which complication rates significantly increase and whether this inflection was consistently reflected across age groupings. As a tertiary objective, we sought to characterize the effect sizes of operative duration and age on complication rates when factored both independently and concurrently.
Materials and Methods
Data Source
The ACS-NSQIP database is a prospectively maintained, risk-adjusted surgical outcomes registry of data from >700 member hospitals with >8.7 million cases recorded to date. 17 Participating data abstracters are trained, and audits have reported an inter-reviewer disagreement rate of 1.56%. 18 The ACS-NSQIP database is entirely deidentified, thus no institutional review board approval was required.
Population Selection
Demographics and Comorbidities of Patients Classified by the Length of Operation and by Age Grouping.
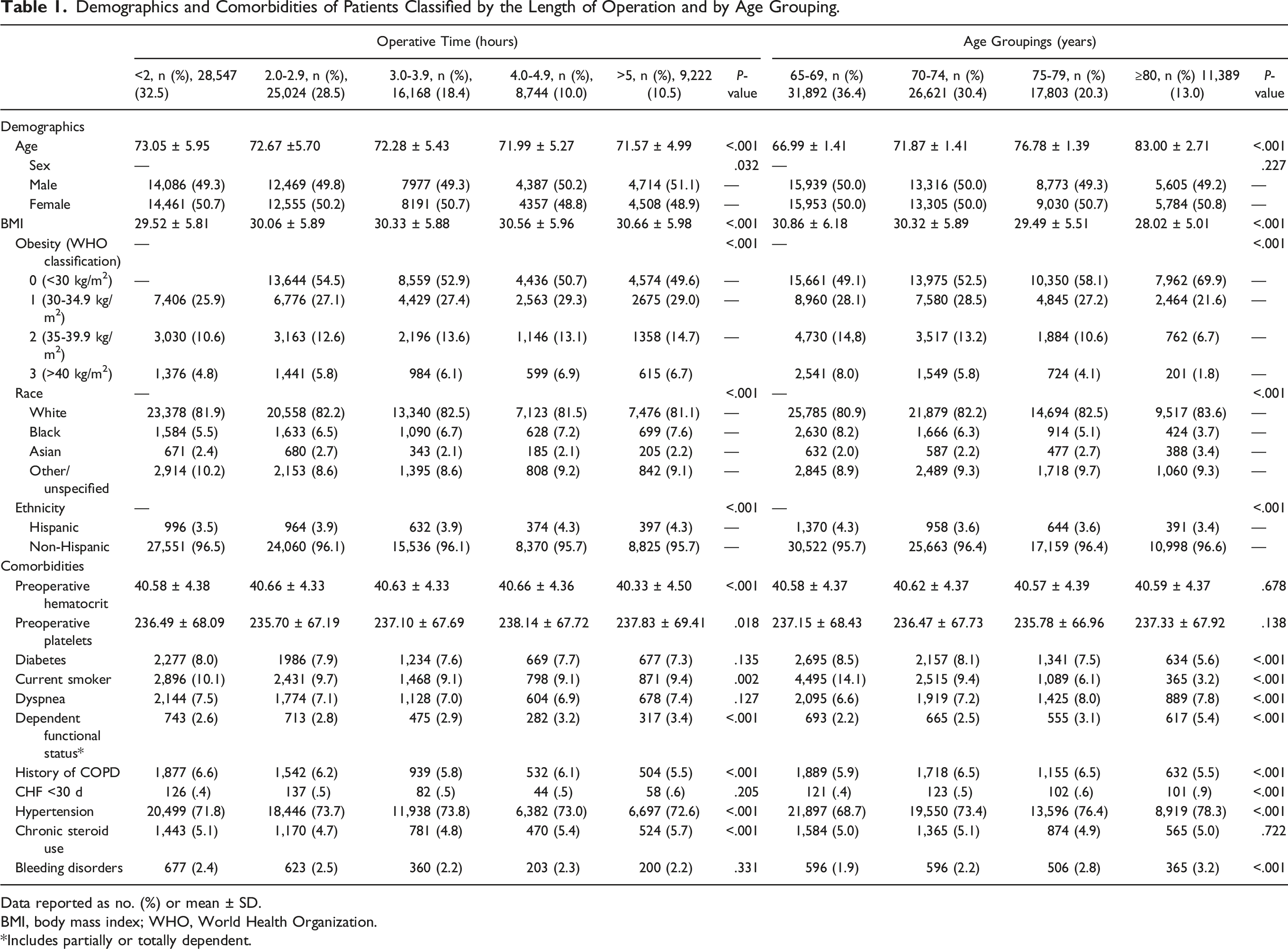
Data reported as no. (%) or mean ± SD.
BMI, body mass index; WHO, World Health Organization.
*Includes partially or totally dependent.
Data Collection
The patient demographics, preoperative characteristics, comorbidities, and operative characteristics collected are shown in Table 1. The primary outcome was complications—overall, surgical, and medical—occurring up to 30 days postoperatively. Surgical complications included superficial surgical site infection (SSI), deep incisional SSI, and wound dehiscence. Medical complications included pneumonia, unplanned reintubation, pulmonary embolism, mechanical ventilation >48 hours, renal insufficiency, acute renal failure, urinary tract infection, stroke, myocardial infarction, postoperative transfusion, deep venous thrombosis, septic shock, and sepsis. Reoperation within 30 days of the index procedure, death within 30 days, and length of hospital stay were also recorded.
Statistical Analysis
SPSS Statistics v.20 (IBM, Armonk, NY) was used for the statistical analyses. Pearson χ2 test was used to analyze categorical variables and one-way ANOVA to assess continuous variables. Univariate analyses were performed to identify potential confounders, namely preoperative and intraoperative categorical variables with P < .2 and ≥10 occurrences and continuous variables with P < .2 (Supplemental Table 2). To evaluate the impact of increasing operative duration on each outcome of interest, we constructed multivariate logistic regression models that controlled for identified confounders. Model adequacy and discrimination were assessed using the Hosmer and Lemeshow statistics and C-index, respectively. Pearson χ2 test and multivariate analyses were performed to assess the impact of age on overall complication rates. A generalized linear model (GLM) was used to estimate partial eta-squared (η2) values and provide estimates of whether the effects of age and operation duration on overall complication rates were small (.001), medium (.059), or large (.138) as defined by Cohen. 19 No assumptions were made in conducting the statistical analysis. Statistical significance was defined at P < .05 for all tests.
Results
Patient Population Stratified by Operative Duration
After the exclusions shown in Supplemental Figure 1, 87,705 patients remained for analysis. Patients were stratified according to operative duration: 32.5% of cases lasted <2 hours, 28.5% lasted 2.0-2.9 hours, 18.4% were 3.0-3.9 hours, 10.0% were 4.0-4.9 hours, and 10.5% lasted ≥5 hours (Table 1). The overall median operative duration was 154 (IQR 106-221) minutes.
There were statistically significant demographic and comorbidity differences among the operative duration cohorts (Table 1), yet altogether the differences among the groups were of negligible clinical value. Shorter surgeries (<2 hours) involved slightly older patients compared with longer operations (≥5 hours) (mean age 73.05 years vs 71.57 years, P < .001). Body mass index values were statistically different across the groups; however, the numerical differences were marginal (29.52 vs 30.66, P < .001). Female patients predominated slightly in shorter surgeries, whereas male patients were a slight majority in surgeries lasting ≥4 hours. Black and Hispanic patients were minimally more prevalent in the longer operation groups, but no other patterns were observed for race and ethnicity.
Similarly, while many comorbidities were significantly different among cohorts, because of the large populations, the differences between groups were minimal and demonstrated no consistent pattern of having less healthy patients in the longer duration groups. The rates of diabetes, dyspnea, and congestive heart failure and prevalence of bleeding disorders among the operative duration groups were not significantly different. Smokers tended to have shorter surgeries, although the lowest smoking rates (9.1%) were seen in surgeries lasting 3.0-3.9 and 4.0-4.9 hours (P = .002). Likewise, fewer patients with a history of chronic obstructive pulmonary disease had long surgeries (P < .001). Proportions of patients classified as being partially or totally dependent on others for their daily care consistently rose as operative duration increased (P < .001). Additionally, every operative duration group had hypertension rates >70%, as might be expected in elderly populations, and rates were higher in the 4 groups having longer surgeries (P < .001). The rates of chronic steroid use were also significantly different among groups (P < .001) but did not steadily increase or decrease as observed in the other comorbidities.
The average relative value unit increased across operative duration increments (P < .001), supporting that more complicated surgeries required additional time (Supplemental Table 3). Additionally, the proportion of cervical spine surgeries decreased (27.9 vs 12.7%, P < .001) and those of thoracic (1.0 vs 4.5%, P < .001) and lumbar (71.1 vs 83.9%, P < .001) surgeries steadily increased for longer surgeries.
Patient Population Stratified by Age Grouping
The overall cohort was restratified according to age group (Table 1): 36.4% of cases were 65-69, 30.4% were 70-74, 20.3% were 75-79, and 13.0% were ≥80 years. As in the duration-based analysis, no notable differences were observed regarding sex; however, stratifying by age group demonstrated a decreasing body mass index with increasing age (30.86 vs 28.02, P < .001). Black patients saw decreased representation from youngest to oldest age groups (8.2 vs 3.7%, P < .001) as did Hispanic patients (4.3 vs 3.4%, P < .001).
No significant differences were recorded across age groups when comparing preoperative hematocrit, preoperative platelet values, or rates of chronic steroid use. Comorbidities that increased across the age groups included dyspnea (6.6 vs 7.8%, P < .001), dependent functional status (2.2 vs 5.4%, P < .001), congestive heart failure (.4 vs .9, P < .001), hypertension (68.7 vs 78.3%, P < .001), and bleeding disorders (1.9 vs 3.2%, P < .001). Conversely, multiple comorbidities diminished across the age groups, including diabetes (8.5 vs 5.6%, P < .001), smoking rates (14.1 vs 3.2%, P < .001), and chronic obstructive pulmondary disease (5.9 vs 5.5%, P < .001). As in the analysis of operative duration groups, the clinical significance of these age-grouped results may be overemphasized because of the large sample sizes. However, the spread of comorbidity rates was generally more pronounced among the age groupings than when stratifying cases by operative duration. Overall, there was no consistent reduction in comorbidities with advancing age to suggest that surgeons selected healthier older patients.
Primary Objective: Operation Duration and Complication Rates
30-day Postoperative Outcomes of Patients Classified by the Length of Operation.
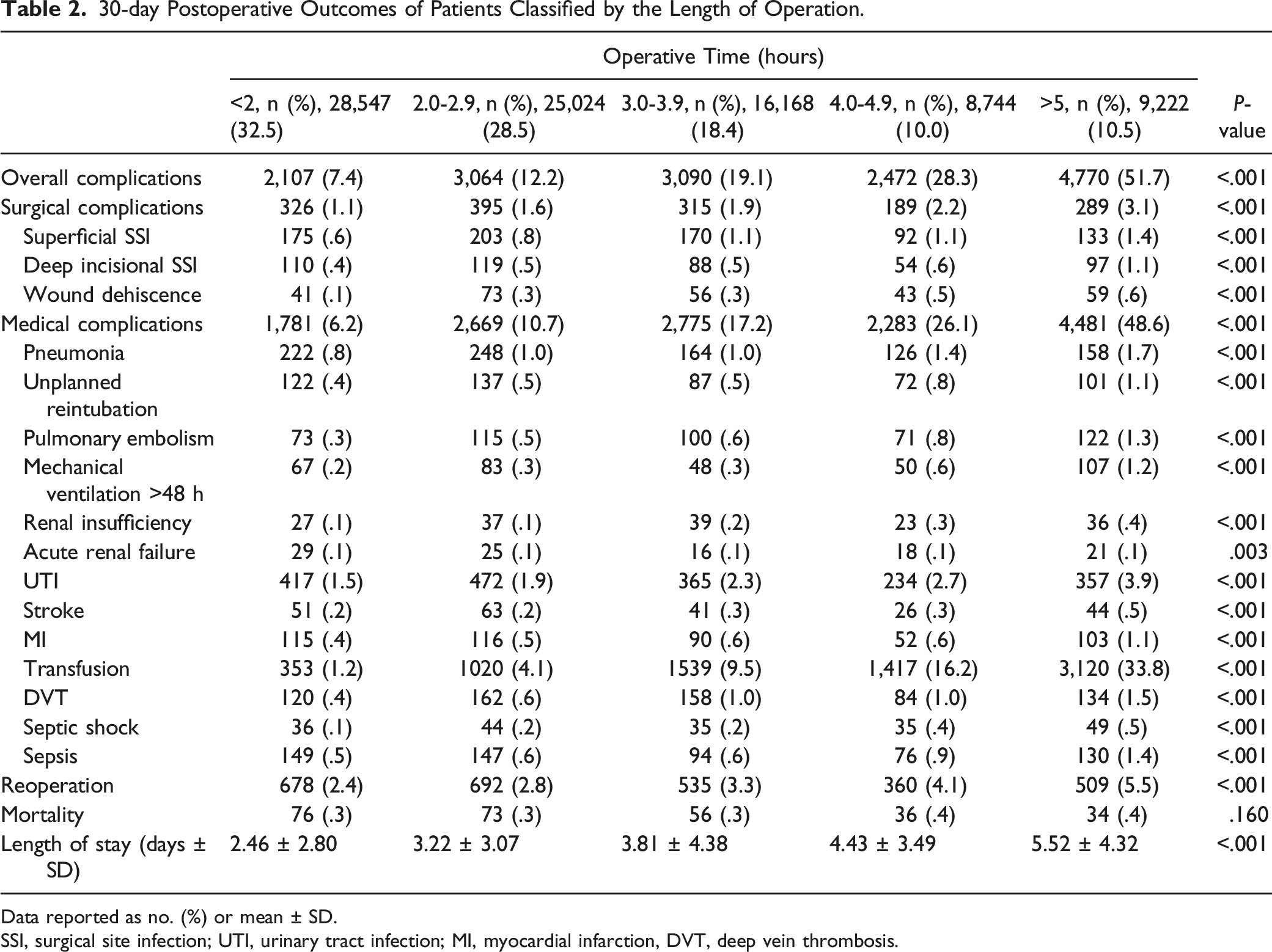
Data reported as no. (%) or mean ± SD.
SSI, surgical site infection; UTI, urinary tract infection; MI, myocardial infarction, DVT, deep vein thrombosis.
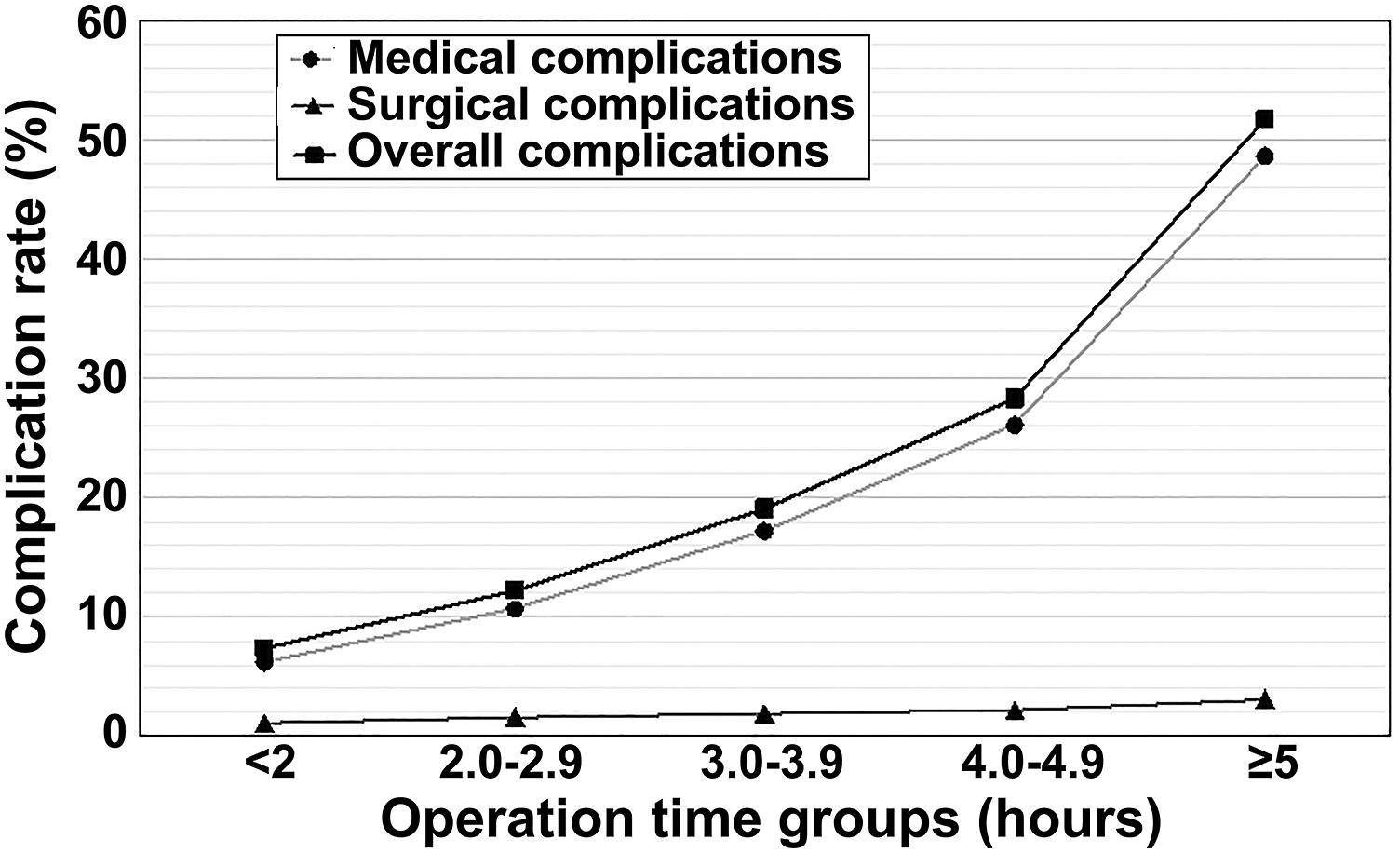
Overall complication rate (%) across operation duration groups. Notably, a ≥5 hours inflection point presents, after which operative duration is associated with dramatic rise in complications. The bulk of overall complications consisted of medical complications, with surgical complications contributing little to the overall complication burden.
All of the complications demonstrated significant statistical differences and higher incidence rates as operative durations increased (Table 2). Most of the reported complications were medical in nature and mirrored the increases and inflection point found in overall complications. The most notable trend among the medical complications was in blood transfusions, which demonstrated a nonlinear rise from 1.2% in surgeries <2 hours to 16.2% in surgeries 4.0-4.9 hours and 33.8% in surgeries >5 hours. Other striking changes in complication rates between surgeries <2 hours and those ≥5 hours were seen for myocardial infarction (.4 vs 1.1%, P < .001), deep venous thrombosis (.4 vs 1.5%, P < .001), pulmonary embolism (.3 vs 1.3%, P < .001), pneumonia (.8 vs 1.7%, P < .001), mechanical ventilation >48 hours (.2 vs 1.2%, P < .001), and urinary tract infection (1.5 vs 3.9%, P < .001).
Surgical complications also demonstrated positive and significant increases across duration groups, again with the greatest difference between <2 hours and ≥5 hours (1.2 vs 3.5%, P < .001). The most common surgical complication was superficial SSI (1.1 vs 3.1%, P < .001), followed by deep incisional SSI (.4 vs 1.1%, P < .001) and wound dehiscence (.1 vs .6%, P < .001).
Reoperation rates increased consistently from 2.4% in surgeries <2 hours to 5.5% in those ≥5 hours. Length of hospital stay also consistently rose in conjunction with longer surgeries, nearly doubling from 2.5 to 5.5 days as surgeries lasted longer (P < .001). Interestingly, mortality was the single 30 day postoperative outcome that did not display a meaningfully increased prevalence even as surgical durations increased (.3 vs .4%, P < .160).
Adjusted Odds Ratios as Functions of Operative Duration Groups.
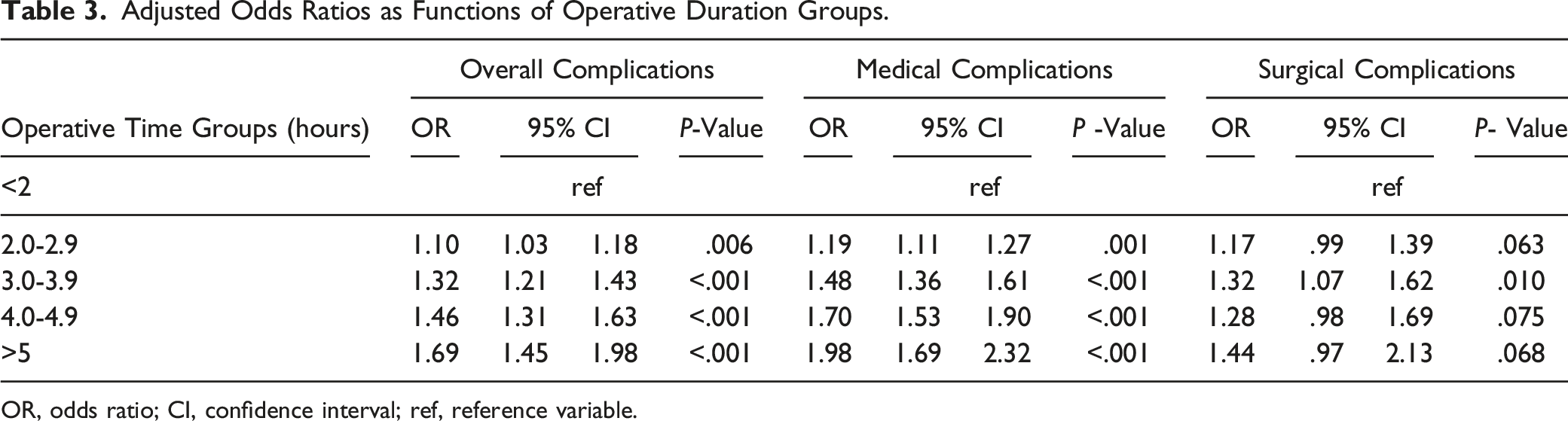
OR, odds ratio; CI, confidence interval; ref, reference variable.
Secondary Objective: Age and Complication Rates
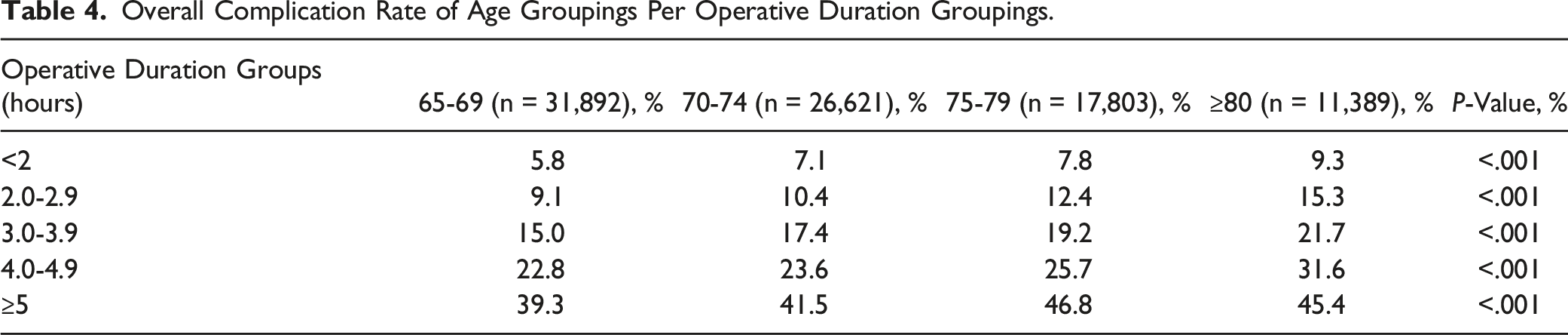
Overall Complication Rate of Age Groupings Per Operative Duration Groupings.
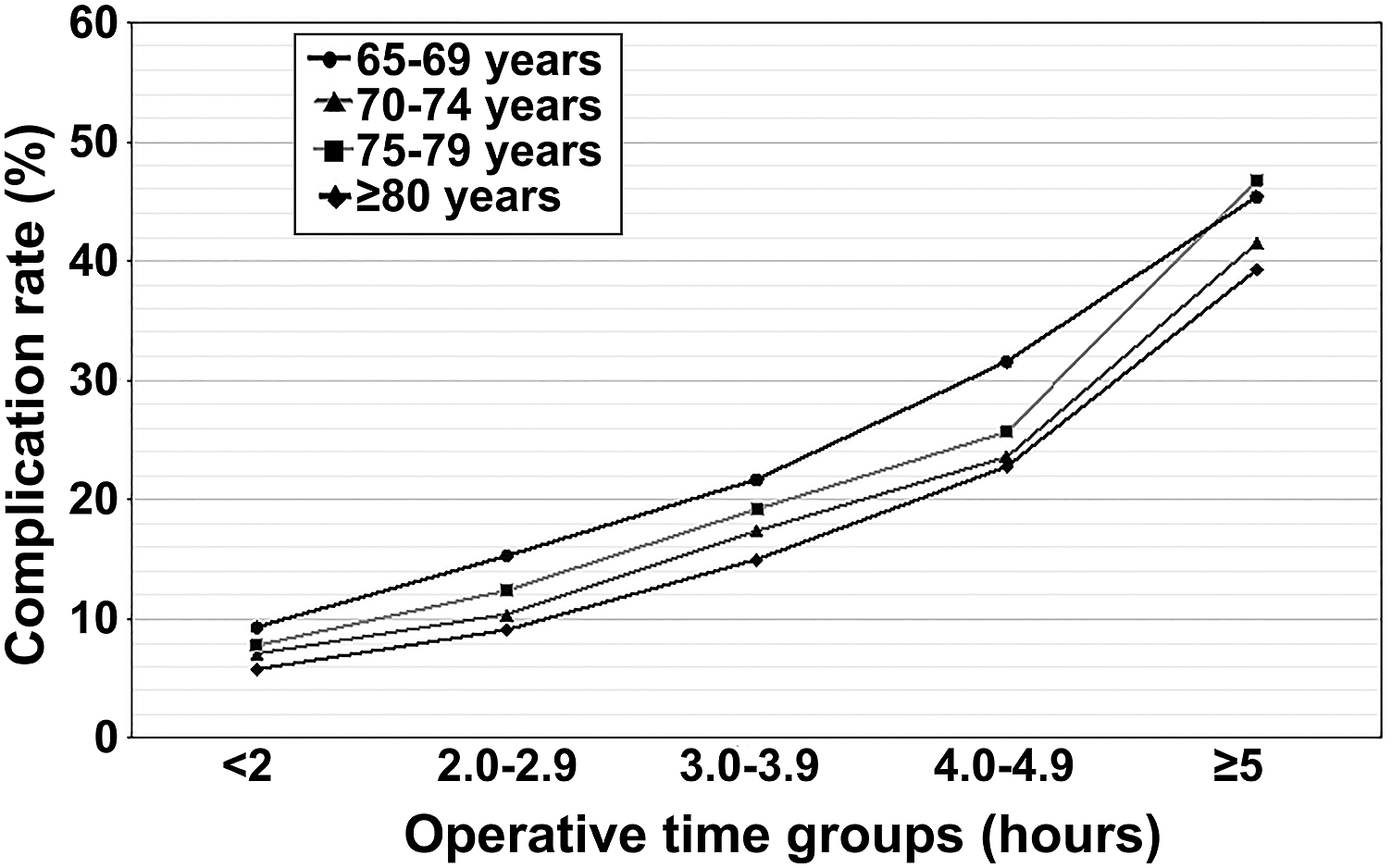
Generalized linear model of overall complication rates (%) stratified by age group and operation duration group. The differences between age groups per operative time group are fairly similar with no age-specific inflection points detected.
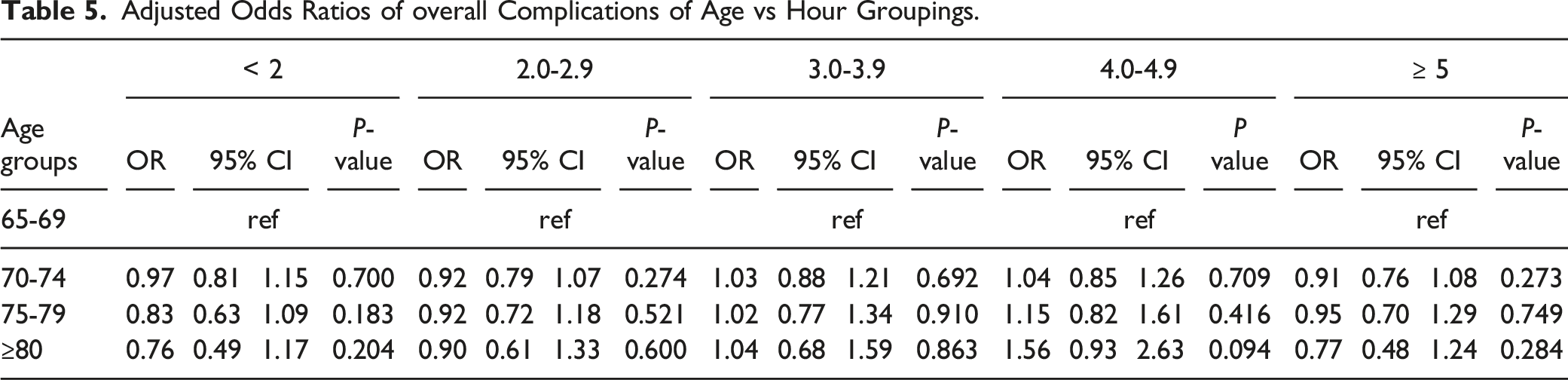
Adjusted Odds Ratios of overall Complications of Age vs Hour Groupings.
Tertiary Objective: Effect Size of Operative Duration vs Age on Complication Rates
Effect Sizes of Age and Operation Duration Factored Independently and Combined.

Discussion
Because of the increased degenerative risks of patient age, surgeons must carefully weigh the benefits derived from invasive surgical procedures against potential harms, with the goal to minimize distress and maximize meaningful outcomes. Thus, in order to expand effective clinical decision-making practice for elective spine procedures, we used a large multi-institutional database to explore the influence of operative duration and age on complication rate in an elderly population. Specifically, we were interested in a simple clinical rubric that might guide decisions for patients of advanced age. We sought to identify whether there are thresholds for operative duration or age that portend excess risk. We detected a distinct increase in complication rates between surgeries lasting 4.0-4.9 hours and those ≥5 hours in length, suggesting a threshold of 5 hours. Importantly, we detected no clinically impactful differences in preoperative comorbidies among any of the operative duration groups. Thus, operation duration proved to be a robust independent risk factor for adverse postoperative outcomes, although increased age was found to carry no independently increased complication risk regardless of operative time. Although age and operative time both were associated with statistically significant differences in overall complication rates, operative duration had a notably larger effect than age.
Primary Objective: Identify Operative Time Threshold for Excess Complications
Before adjusting for risk factors, a strong association with an increasing incidence of overall complications, medical complications, and surgical complications was observed as operation duration increased (Table 2). More notably, overall complications and medical complications demonstrated a distinct inflection point between 4-4.9 hours and ≥5 hours, followed by increased trajectory (Figure 1). Adjusting for confounders, operative duration proved to be a robust independent risk factor for overall complications and medical complications (Table 3). These results suggest that operations lasting ≥5 hours demonstrate substantially increased risk in the elderly population. Therefore, we suggest that spine surgeons should carefully weigh the anticipated benefits for elective surgeries requiring more than 5 hours against the potential for excessive risk.
Our findings corroborate numerous studies that demonstrate correlation between longer operation duration and increased rates of adverse postsurgical outcomes.7,10-16,20,21 The mechanisms underlying this relationship likely vary depending upon surgical discipline, anatomic location, and complication type. 14 However, contributing variables routinely encountered in elective spine surgery include compromised surgical site sterility, retractor-induced tissue ischemia, increased wound desiccation, greater anesthesia exposure, surgical team fatigue, blood stasis, and blood loss.14,15,21-27 Considering the significantly increased complication risk associated with prolonged operations, surgeons, hospitals, and policy-makers should seek every opportunity to safely reduce operative duration. Optimizing operative skill and efficiency, improving surgical team communication, limiting the ratio of surgical trainees to attending surgeons, staging complex surgeries, and deployment of safe, yet efficient emerging technologies are established means whereby operative times could be streamlined.15,28-31 In the meantime, as spine surgeons consider the hazards and benefits in providing elective surgical care to their elderly spine patients, the present study warns that surgeries lasting ≥5 hours demonstrate significantly greater rates of complication.
Secondary Objective: Identify Age Threshold for Excess Overall Complications
We similarly sought to identify the presence of age thresholds within our established operation duration groupings beyond which patients experienced significantly increased complications. To the best of our knowledge, no such analysis has been reported in the spine surgery literature. After further stratifying our preexisting operative time cohorts into 4 age groupings (65-69, 70-74, 75-79, ≥80), univariate analysis showed steady increases (all P < .001) in overall complication rates as age increased across each operative duration grouping (Table 4). However, no distinct inflection point was detected. Upon multivariate analysis, no significantly increased risk of complication was noted between any age comparison among any of the hour groupings (Table 5). It warrants consideration that we recorded notably increased rates of several medical comorbidities among the most elderly patients (Table 1). For example, rates of hypertension increased nearly 10% (68.7 vs 78.3%) and the percentage of patients with dependent functional status more than doubled (2.2 vs 5.4%) across age groups. Thus, we hypothesize that the increased complication rate associated with increased age (Table 4) was possibly more influenced by the progressively increased comorbidity burden of elderly age than by advanced age itself. 32 If true, this would corroborate other studies that report that age alone is a less useful risk factor than comorbidity profiles in calculation of complication risks among elderly spine patients.33-39
Tertiary Objective: Effect Sizes of Operative Duration vs Age in Overall Complication Rates
To the best of our knowledge, the individual and combined effect sizes of prolonged operative duration and increased age on overall complication rates among elderly spine surgery patients have not been investigated. Using a GLM, and in conjunction with our earlier findings, we found that both operation duration and age were significant factors. Operative duration exerted a medium effect on overall complication rates (F = 1575.914, P < .001, η2P = .067) whereas increased age exerted only a small effect (F = 79.673, P < .001, η2P = .003) 19 (Table 6). When factored compositely, age and operative time remained significantly associated with increased overall complication rates, but the measured the effect size was minimal (F = 3.917, P < .001, η2P = .001). It is possible this diminished combined effect is due to unexplained variablitiy within the interaction terms of the model. In light of these findings, surgeons should consider operative duration more heavily than age when conducting surgical risk assessment.
Limitations
Using the ACS-NSQIP database introduces several limitations. Most importantly, this is a retrospective database that implicitly reflects surgeons’ decisions for operative treatment. For example, the fact that age did not show an independent association with increased complications may represent overall clinical judgement. Compared with age, comorbidities may have exerted greater influence, although this was not directly tested. Moreover, comorbidities appear nonspecific to operative duration, suggesting that healthier patients were not selected for longer procedures. Nonetheless, the silent effect of surgeon selection is not tested in this research, nor is it ethical or feasible to test this effect. Other specific limitations include that the database only records outcomes 30 days postoperatively, limiting our ability to understand the long-term consequences of surgical intervention. Another limitation of the NSQIP database is its use of generic standardized definitions, which limits the availability of some pertinent neurosurgical variables. Lastly, although large datasets have the advantage of increased statistical power, such analyses are vulnerable to problems with data interpretation and application, 40 particularly when using statistical techniques that compare the mean differences among groups such as the Pearson χ2 and ANOVA tests. 41 Thus, the high rate of statistically significant results reported from our univariate analysis may be influenced or overemphasized by the large nature of the dataset.
Conclusion
To the best of our knowledge, this is the most rigorous investigation to date regarding the relationship between prolonged operative duration and postoperative adverse outcomes in elderly patients undergoing many types of elective spine surgery. Our analysis demonstated that longer operative duration is strongly associated with postoperative complications and that the rate of complications among elderly patients dramatically increases in operations lasting ≥5 hours. Additionally, the effect of operative duration on surgical outcomes was more influential than that of age. Therefore, surgeons should strongly consider the operative time requirements of spinal surgical interventions in assessment of the anticipated benefits from surgery for patients aged ≥65 years.
Supplemental Material
Supplemental Material - Identification of an Operative Time Threshold for Substantially Increased Postoperative Complications Among Elderly Spine Surgery Patients
Supplemental Material for Identification of an Operative Time Threshold for Substantially Increased Postoperative Complications Among Elderly Spine Surgery Patients by Matthew C. Findlay, Robert B. Kim, Wesley S. Warner, Brandon A. Sherrod, Seojin Park, Marcus D. Mazur, and Mark A. Mahan in Global Spine Journal
Footnotes
Acknowledgments
We thank Kristin Kraus, MSc, for editorial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.