
Abstract
Study Design:
Retrospective study.
Objective:
Anterior fixation of odontoid fracture has been associated with high morbidity and mortality in small, single institution series. Identifying risk factors may improve risk stratification and highlight factors that could be optimized preoperatively. The objective of this study was to determine the 30-day complication rate following anterior fixation of odontoid fractures and to identify associated risk factors among patients in a large national database.
Methods:
Patients who underwent anterior fixation were identified in the American College of Surgeons National Quality Improvement Program database (ACS NSQIP) from 2007 to 2012. Patient demographics, medical comorbidities, perioperative complications, and postoperative complications up to 30 days were analyzed by univariate and multivariate analysis.
Results:
Overall, 103 patients met criteria for the study. The average age was 73.9 years and patients were predominantly white (85.4%). Cardiac comorbidity was common (66.0%), as were dependent functional status (14.6%) and bleeding disorders (13.6%). Complications occurred in 37.9% of patients, and mortality was high (6.8%). Age, white race, and history of bleeding disorders were independently predictive of complications in the multivariate analysis. The postoperative hospital stay was >5 days for 45.6% of patients.
Conclusion:
In a large, multicenter database study, anterior fixation of odontoid fracture was associated with high morbidity and mortality. Although advanced age was associated with increased risk of complications, patients undergoing anterior fixation were older, on average, than in prior studies. Bleeding disorder was a potentially modifiable risk factor for complications that could be optimized prior to surgery.
Keywords
Introduction
The odontoid process or dens of the C2 vertebrae restricts translational movements in the most mobile segment of the cervical spine, the C1-C2 complex. 1 Fractures of the odontoid process result from forceful flexion or extension of the cervical spine, which commonly occurs in motor vehicle accidents in younger patients or simple falls in the elderly. 2 The odontoid process is the most common site of fracture in the cervical spine, accounting for 9% to 15% of cervical spine fractures. 3 –7 These injuries can cause neck pain and cervical instability that put patients at risk for catastrophic spinal cord compromise. 8 –11
The treatment of odontoid fractures depends primarily on fracture pattern, the degree of displacement, and patient age. 4,12 Treatments include cervical collar immobilization, rigid bracing with halo vest, posterior fusion of C1-C2, and anterior fixation with compression screws. 4,5,12
Rigid bracing in the elderly has been associated with unacceptably high morbidity and mortality 13 and lower rates of fusion, prompting some surgeons to advocate for early surgical intervention. 4,14 Surgical intervention provides earlier patient mobilization and higher likelihood of successful fusion.
Anderson and D’Alonzo classified odontoid fractures into Type I through the tip of the dens, Type II through the base of the dens, and Type III extending into the body of the axis. Grauer later subclassified Type II fractures based on the direction of the fracture line, with Type IIb or posterior oblique fractures being most amenable to anterior screw fixation. Studies of anterior fixation of Type II and III fractures have consistently shown high fusion rates of 83% to 100%. 1,2,4,5,9,11,12,15 –23 An alternative approach to surgical correction, posterior arthrodesis of C1-C2, can be achieved by either Gallie and Brooks wire fixation, transarticular screw placement, or screws placed into the vertebra and connected by rods. In contrast to posterior arthrodesis, anterior screw fixation has the benefit of preserving rotation at C1-C2 and potentially providing a more reliable fusion in Type IIb injuries. Although anterior fixation is believed to preserve rotation at C1-C2, this was true for only a minority of patients in the study by Jeanneret et al. 24 Anterior fixation remains controversial due to high rates of morbidity and mortality reported in the literature. 15,16,25,26 Complications from surgical procedures lead to worse outcomes for patients, lower patient satisfaction, and increased hospital and patient expenditure. Although previous studies have reported surgical complications with anterior fixation, risk factors other than patient age have not been studied.
The purpose of this study is to describe the 30-day complications associated with anterior fixation of odontoid fractures in a large multicenter cohort and to identify patient characteristics and preoperative comorbidities that are risk factors for these complications.
Methods
Data Acquisition and Patient Selection
The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) collects more than 150 variables from surgical cases at participating hospitals in the United States. Certified reviewers collect hospital patient data as well as morbidity and mortality data in the 30-day postoperative period. The accuracy of this data is confirmed by routine audits, which have demonstrated interrater error rates of less than 2%. 27 The ACS NSQIP database is composed of HIPAA compliant, de-identified data that includes patient demographics, comorbidities, procedure codes, and 30-day perioperative outcomes. The ACS NSQIP database is validated for use in observational studies of short-term surgical outcomes, 28 and investigators have used it in many studies of spine surgery to date. 29 –34 Since all ACS NSQIP records are de-identified, this study was exempt from review by the institutional review board.
Patients undergoing anterior fixation of odontoid fractures were identified from 2007 to 2012 ACS NSQIP participant use files by Current Procedural Terminology (CPT) codes 22318 and 22319. Both CPT codes are used for “open treatment and/or reduction of odontoid fracture(s) and or dislocation(s) (including os odontoideum), anterior approach, including placement of internal fixation,” with 22318 corresponding to procedures without grafting and 22319 to procedures with grafting. 35 We assessed mortality and morbidity in these patients and divided them into 2 cohorts, one consisting of patients who experienced any complication and one with no complications. The following complications were included in the analysis: wound complications; sepsis; renal, central nervous system, cardiac, or pulmonary complications; venous thromboembolism; and unplanned reoperation. Detailed definitions of each of these complications can be found in the appendix.
Statistics
Demographics, comorbidities, and operative variables were compared in the complication and no complication groups using univariate analysis. Independent t tests were performed for continuous variables and χ2 or Fisher’s exact tests were performed for categorical variables. Median and interquartile ranges were reported for operative time and length of stay. Complications within 30 days of surgery were analyzed by univariate analysis. Complications that reached significance and preoperative variables that had P values <.1 in the univariate analysis were analyzed by multivariate logistic regression in order to determine which variables were independent predictors of morbidity. P values, odds ratios (ORs), and 95% confidence intervals (CIs) were reported for the analyses. All P values were 2-tailed with a cutoff value of P < .05. All statistical analyses were performed using SPSS v20 (Chicago, IL).
Results
The ACS NSQIP database returned 103 patients who underwent anterior fixation of odontoid fractures between 2007 and 2012. Grafting was used in only 4 of these cases (3.9%). The average age was 73.9 years, with a majority of patients above age 65 years (Figure 1). Gender was 61.2% female, race was 85.4% white, and the average body-mass index was 25.7. In terms of comorbidities, there was a high rate of cardiac comorbidity (66.0%), dependent functional status (14.6%), bleeding disorders (13.6%), smoking (12.6%), and diabetes (11.7%; Table 1). Cardiac comorbidity includes congestive heart failure, history of myocardial infarction, percutaneous cardiac intervention, cardiac surgery, angina, and medicated hypertension. Bleeding disorders are defined by ACS NSQIP as any condition that places the patient at risk for excessive bleeding requiring hospitalization due to a deficiency of blood clotting elements. Median operative time was 80 minutes (interquartile range = 48 to 124.5). Median length of stay was 5 days (interquartile range = 3 to 8.5).
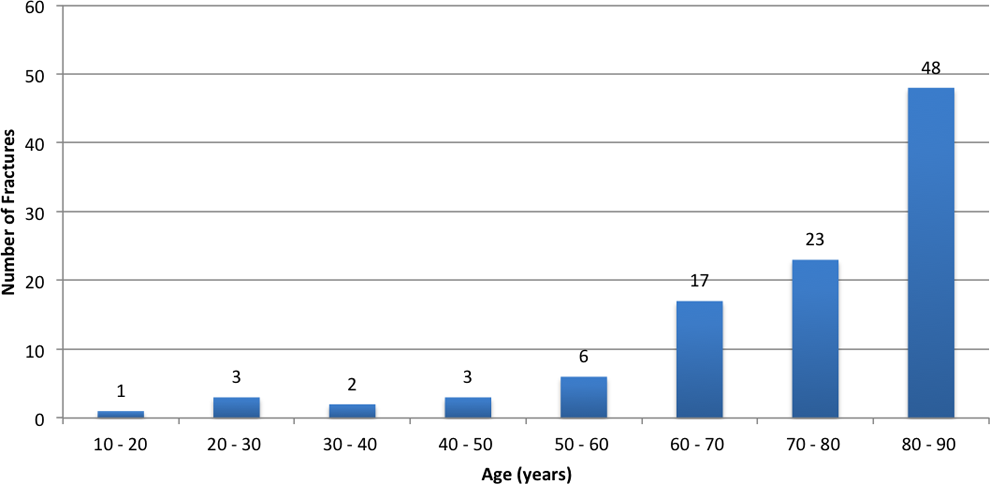
Age of patients undergoing anterior fixation of odontoid fractures.
Demographics and Preoperative Patient Characteristics.
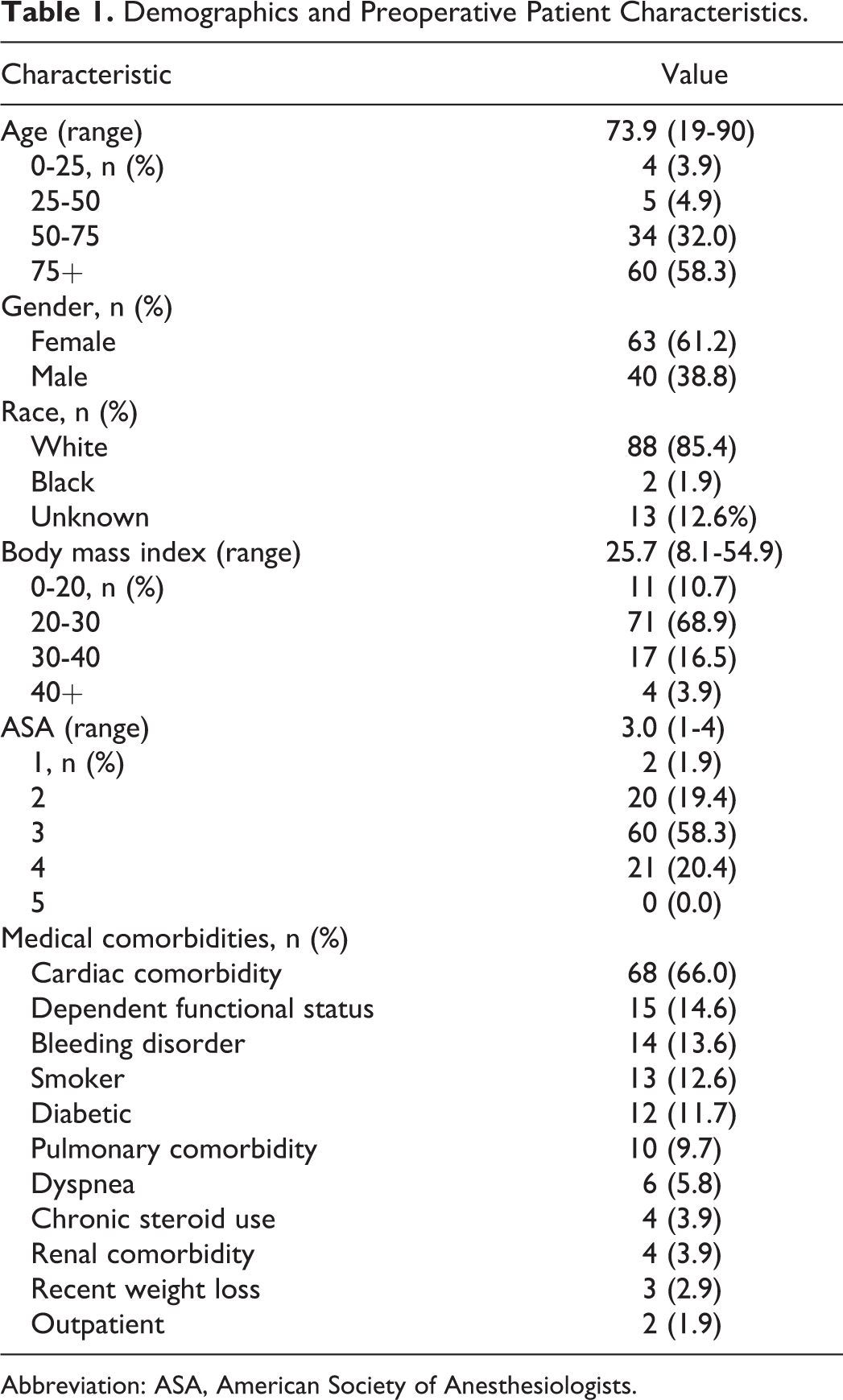
Abbreviation: ASA, American Society of Anesthesiologists.
Of the 103 patients, 64 experienced no complications while 39 experienced perioperative or postoperative complications within 30 days of the procedure (Table 2). The overall rate of major complications was 17.5%, which included death (6.8%), unplanned reoperation (5.8%), failure to wean from ventilator or re-intubation (4.9%), myocardial infarction (1.9%), stroke (1.9%), sepsis (1.9%), cardiac arrest (1.0%), and septic shock (1.0%). Minor complications occurred in 28.2% of patients, which included blood transfusion (22.3%), pneumonia (3.9%), and urinary tract infection (2.9%).
Thirty-Day Complications and Other Adverse Outcomes.
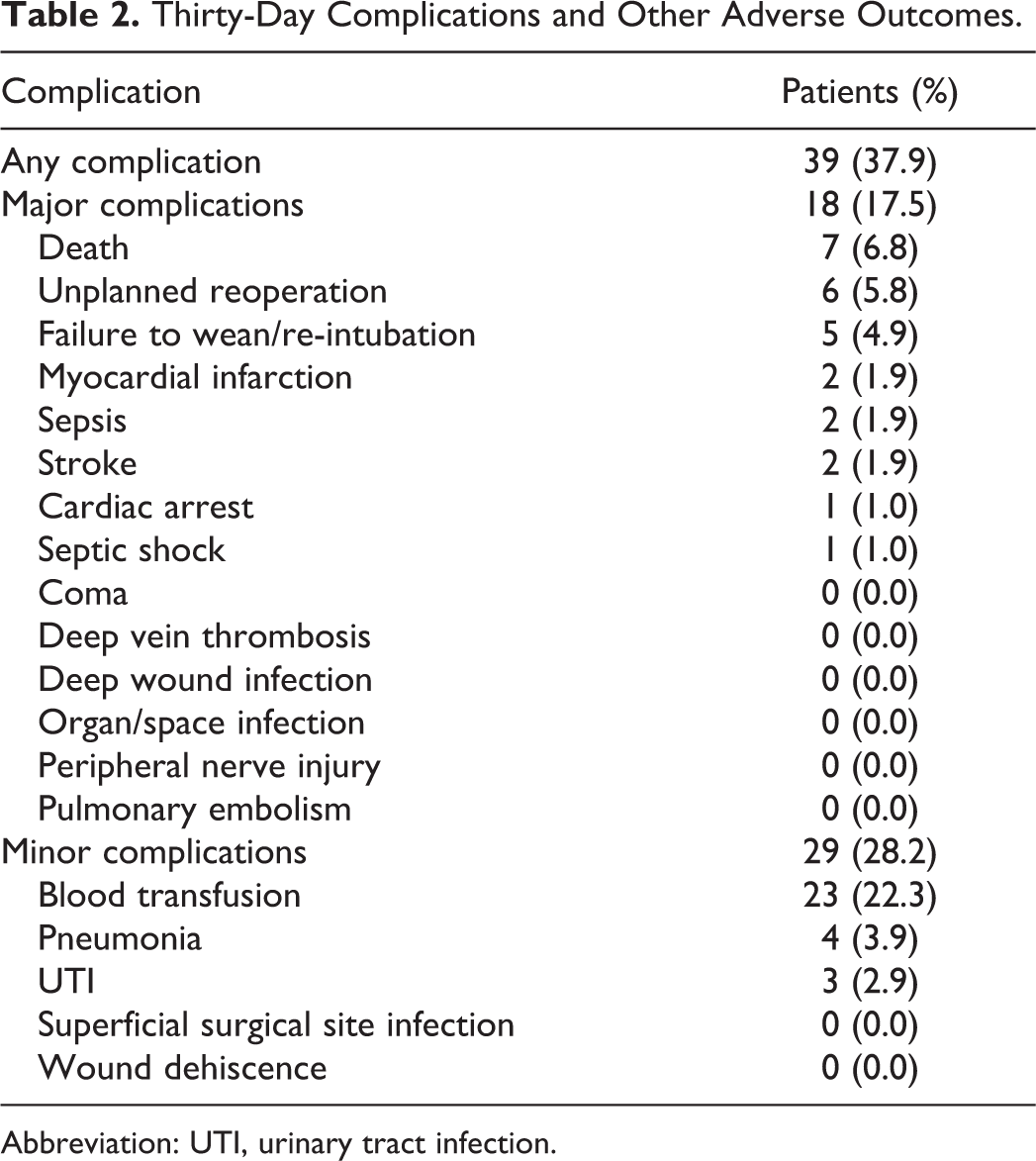
Abbreviation: UTI, urinary tract infection.
Univariate Analysis
Elderly patients (age ≥65 years) were significantly more likely to experience complications (P = .003), as were white patients (P = .007) and patients with bleeding disorders (P = .028). Use of graft was not associated with increased risk of complications (P = .625), although the sample size of only 4 grafted patients limits the utility of comparisons between grafted and nongrafted groups.
Multivariate Analysis
Age, white race, American Society of Anesthesiologists score ≥3, and bleeding disorder were all found to have P value <.1 in the univariate analysis and were therefore carried into the multivariate logistic regression (Table 3). Advanced age was found to be an independent risk factor for complications within 30 days (OR = 7.8; 95% CI = 1.5-39.4) as were white race (OR = 11.2; 95% CI = 1.3-96.2) and bleeding disorders (OR = 4.4; 95% CI = 1.0-18.2; Table 4).
Univariate Analysis of Risk Factors for Any Complication Following Anterior Fixation of Odontoid Fracture.
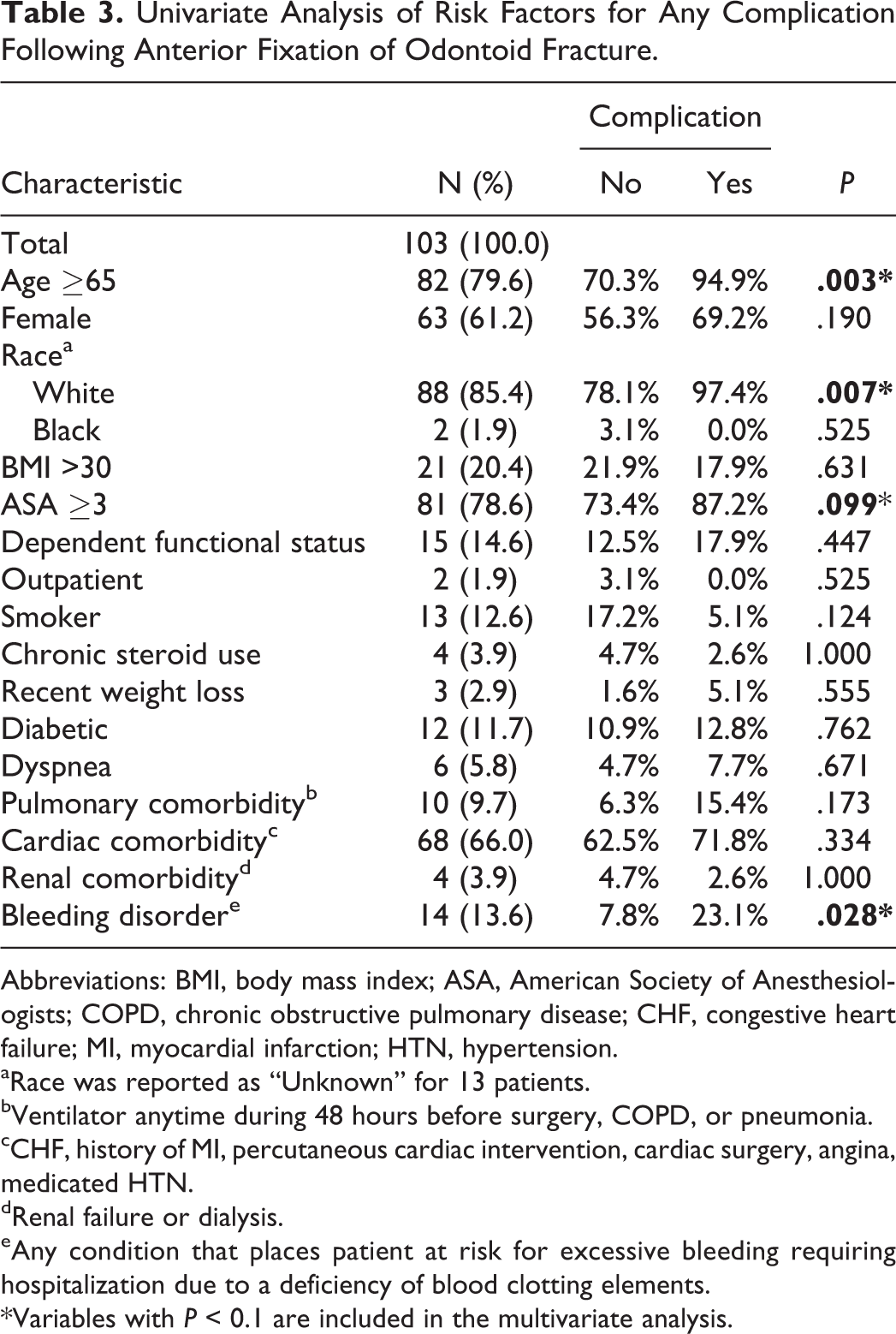
Abbreviations: BMI, body mass index; ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; MI, myocardial infarction; HTN, hypertension.
aRace was reported as “Unknown” for 13 patients.
bVentilator anytime during 48 hours before surgery, COPD, or pneumonia.
cCHF, history of MI, percutaneous cardiac intervention, cardiac surgery, angina, medicated HTN.
dRenal failure or dialysis.
eAny condition that places patient at risk for excessive bleeding requiring hospitalization due to a deficiency of blood clotting elements.
*Variables with P < 0.1 are included in the multivariate analysis.
Multivariate Analysis of Risk Factors for Any Complication.a
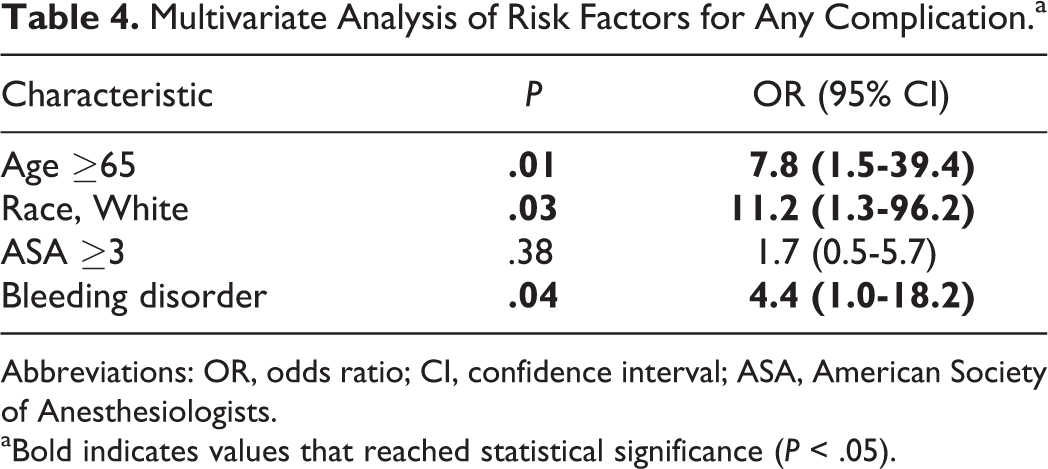
Abbreviations: OR, odds ratio; CI, confidence interval; ASA, American Society of Anesthesiologists.
aBold indicates values that reached statistical significance (P < .05).
Discussion
In this study, we tested the hypothesis that anterior fixation of odontoid fractures is associated with high morbidity and mortality in a large cohort using the ACS NSQIP database. Due to the rarity of anterior fixation of odontoid fractures, our 103-patient sample is one of the largest studies of this procedure to date. We showed that patients tended to be older (79.6% ≥65 years), predominantly white (85.4%), and had significant burden of cardiac disease (66.0%). Anterior fixation of odontoid fracture was associated with high 30-day mortality (6.8%), and patients suffered complications at a rate of 37.9%. Unplanned reoperations occurred in 5.8% of patients. Age, white race, and bleeding disorders were independent predictors of complications following anterior fixation of odontoid fractures. Confidence intervals were wide for each of these risk factors; therefore, a larger study of odontoid fracture repair is needed to confirm these findings. Unsurprisingly, grafting was seen in a small minority of cases (4 of 103). The specifics of this rare technique are not available from the ACS NSQIP database; therefore, it would be helpful if authors using grafting with anterior fixation described their indications and technique in the literature.
Anterior fixation of odontoid fracture is a relatively uncommon procedure. A survey by Clark and White of 26 providers reported a total of only 11 cases of anterior fixation. 25 The highest frequency of anterior fixation in the literature was reported by Apfelbaum et al in their study of 147 cases at 2 hospitals over a 13-year period. 11 Our series of 103 cases reported by hospitals participating in NSQIP over a 6-year period suggests an even lower frequency of anterior fixation cases than previous studies. However, given the technical complexity of anterior fixation of odontoid fracture, it is likely that only a handful of hospitals participating in NSQIP actually perform this procedure.
The risks of anterior fixation were considered low in Bohler’s seminal paper describing the technique, 2 although several studies after Bohler have shown high rates of morbidity and mortality, particularly among elderly patients. Muller et al showed a mortality of 40% among elderly patients with this approach, although the sample size was just 5 patients. 36 Our study captures one of the largest and most diverse samples to date, which, in contrast to the single institution studies that dominate the current literature, may provide a truer representation of preoperative comorbidities and the postoperative complications of anterior fixation.
The findings of our large multicenter study reinforce the assertion that the elderly are at increased risk for perioperative complications. Furthermore, we show that the elderly comprise a majority of patients undergoing anterior fixation of odontoid fractures at hospitals participating in ACS NSQIP. This is a surprising finding given that expert opinions by Hsu and Anderson 4 and Konieczny et al 37 favor posterior fusion or cervical immobilization in this demographic. The increased morbidity and mortality in the elderly has been shown previously in single-center studies. A recent study by Platzer et al 26 comparing outcomes in 69 young patients and 41 elderly patients undergoing anterior fixation showed significantly higher rates of complications (8% vs 22%) and perioperative mortality (1% vs 9%) in the elderly group, which is consistent with our results. Given that only 20.4% of patients in our study were <65 years of age, further study is needed to clarify the increased risk of complications with age.
Patients in our study were older than patients in previous studies of anterior fixation (mean 73.9 years, 79.6% ≥65 years), with a majority being older than 75 years of age. Patients studied by Bohler were an average age of 44.8 years of age. The 2 largest studies of anterior fixation, authored by Apfelbaum et al 11 and Platzer et al, 26 report outcomes in cohorts whose average age is 50.1 and 54 years, respectively. The reason for this difference in average patient age is unclear. Perhaps it is related to a difference in patient populations (hospitals across the United States participating in ACS NSQIP versus Vienna, Austria; Salt Lake City, Utah; and Budapest, Hungary) or a trend toward broader patient selection criteria for anterior screw fixation. Unfortunately, none of the aforementioned studies describes its criteria for patient selection, so an explanation cannot be further elucidated.
In the literature, mortality with anterior fixation ranges from 0% to 14%. 11,15,16,23,26,36 –38 Mortality of 6.8% in our study is high but within the reported range. We capture all deaths within 30 days of the procedure, which encompasses most all surgery-related deaths. In long-term follow-up studies by Apfelbaum and Platzer, all surgery related deaths occurred within 32 days of the primary procedure. Several authors have raised concerns about high mortality among elderly patients, which ranges from 6% to 11%. 23,26,38 Muller’s frequently cited mortality rate of 40% among 5 elderly patients treated with anterior fixation is an outlier in a small sample and may be less representative. Henry showed that 89% of deaths in their study occurred in patients ≥79 years of age. In our study, one death occurred in a 65-year-old patient, and 6 deaths (86%) occurred in patients ≥82 years of age.
Reintubation or failure to wean occurred in 4.9% of patients. Hematoma, severe pneumonia, and pharyngeal edema are in line with other literature that have examined complications of anterior fixation of odontoid fractures, 15,23,26,36 and these may have contributed to reintubations in our study. Patients and their families may benefit from counseling on the likelihood of this outcome prior to surgery.
Unplanned reoperations occurred in 5.8% of patients. Reoperations cause distress for families and are associated with morbidity, increased hospital costs, and worse patient outcomes. Earlier studies report reoperations for loose screws, nonunion causing severe pain, postoperative hematoma, and fracture redisplacement. 11,15,36 Platzer et al reported that all reoperations were consequences of procedure-specific complications (eg, instrumentation failures, nonunion) and none from general, systemic complications (eg, cardiac, respiratory). ACS NSQIP is limited to reporting general complications; however, it is reasonable to assume that the causes of unplanned reoperations in our study are similar to earlier studies and, therefore, unplanned reoperations represent major procedure-specific complications that arose in our 103 patient sample. Our reoperation rate was comparable to other reports, which range from 3.4% to 8.7%. 11,26,36 Since our follow-up focuses on 30-day outcomes, the true rate of reoperation in our patient sample is likely higher.
Blood transfusion was a frequent complication, occurring in 22.3% of patients treated with anterior fixation. Blood transfusion is not uncommon in spine surgery. Buerba et al reported transfusion as a complication in 0.4% to 11.1% of patients undergoing cervical spine fusion in a recent ACS NSQIP study. 30 Butler reported transfusions in 25.9% of spine surgery patients in an Irish cohort of younger patients with predominantly cervical spine trauma. 39 In our study, transfusions likely resulted from the combination of trauma in conjunction with anticoagulant and antiplatelet medication use. These medications are prescribed widely among elderly patients with cardiac disease, which was present in 66.0% of patients in this series. In the setting of trauma, surgery may or may not be delayed for these medications to be metabolized and normalization of coagulation labs, so greater blood loss can occur. Risks of allogenic blood transfusion include transfusion reactions, hemolytic reactions, increased infection rates, and disease transmission. This is the first study to report the rate of blood transfusions associated with anterior fixation of odontoid fractures. With this information, patients may be more accurately counseled on the risks of transfusion associated with anterior fixation of odontoid fracture.
Bleeding disorder was a significant risk factor for complications. ACS NSQIP defines bleeding disorders as any condition that places the patient at risk for excessive bleeding requiring hospitalization due to a deficiency of blood clotting elements. Included are patients with vitamin K deficiency, hemophilias, thrombocytopenia, and chronic anticoagulation, while patients on aspirin therapy are excluded. 27 Considering these findings, preoperative optimization of coagulopathies warrants further study as a potential means to reduce complications.
White race has not previously been reported as a risk factor for complications in anterior fixation. Gender is a frequently reported demographic variable, although the variable of race has not been reported in studies of anterior fixation of odontoid fractures to date. The underlying cause of why white race might be associated with increased complications remains unclear. Only 2 patients were identified as black in our cohort, and race was unknown in 13 cases, which raises the question of whether the finding could be spurious. Further research would be needed to establish whether white race is a true risk factor for increased complications in anterior fixation of odontoid fractures.
There are several limitations to this study, many of which are due to the generalized nature of the ACS NSQIP database. For instance, this study reports on the major causes of morbidity and mortality, but procedure-specific outcomes are not available. Dysphagia is a common complication of anterior fixation that would be useful to report; however, dysphagia is not specifically recorded in the ACS NSQIP database so we must look at its sequelae instead, such as pneumonia and other pulmonary complications. Our cohort is one of the largest to date on the subject of anterior fixation of odontoid fractures, yet with a sample of 103 patients, its power for detecting significance among risk factors for complications remains low. Additionally, there is no way of knowing the distribution of cases among the hospitals in the ACS NSQIP database as both patients and hospitals are de-identified. This potentially introduces sampling bias into our results. Last, with the ACS NSQIP data set we cannot appreciate the mechanism of injury, fracture pattern, acute neurologic status, or associated injuries of patients in the study.
Conclusion
Anterior fixation of odontoid fractures was associated with high morbidity and mortality in a large multicenter cohort. Advanced age, white race, and bleeding disorders were significant risk factors for complications within 30 days. Despite recent expert opinions recommending posterior fusion or cervical immobilization over anterior fixation for elderly patients with odontoid fractures, the majority of patients treated with this approach were older than 75 years. Specific complications and their frequencies reported here are valuable statistics for surgeons to use in management, preoperative patient counseling, and risk stratification.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SKC: Stryker Grant; OREF grant not related to the content of this work. All other authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.