
Abstract
Study Design
Retrospective cohort study.
Objectives
To identify predictors for early mortality following traumatic spinal cord injury (TSCI), as recognition of factors associated with early mortality is essential for public resource allocation and optimized acute care.
Methods
Retrospective Analysis of SCI patients admitted to the acute SCI ward from 2003 to 2022 was performed. Days elapsing from the date of injury to date of death established the survival time. Early mortality was defined as survival time ≤ 365 days. Multivariable logistic regression was used in modeling of early death following TSCI with age, gender, neurologic deficit, type of neurologic injury, ventilation status, and count of complications as covariates.
Results
Simple logistic regression indicated a significant association of early mortality with the number of complications (P < .0001), neurological deficit (P < .0001), complete neurological injury (P < .0001), ventilation status (P < .0001), and age group (P < .0003). After adjusting for other covariates, complete neurological injury (OR: 1.75, P < .0001), ventilation (OR: 2.80, P < .0001), and Age group (over 60 OR: 17.71, P < .0001) were significantly associated with early mortality. The multivariable model showed a good overall fit (Hosmer-Lemeshow P = .315; AUC 0.85).
Conclusions
Predictors of early mortality after TSCI are high complete spinal cord injury, age, number of complications, and the need for ventilation. Identification of high-risk patients is crucial to rationalize and improve acute care to potentially reduce mortality rates.
Keywords
Introduction
Traumatic spinal cord injury (TSCI) is a catastrophic event that imposes a considerable health and economic burden on the patient and society.1-4 The incidence of TSCI ranges from 3.6 to 195.4 patients per million population around the world and is higher in low-income countries compared to high-income countries.5,6 Most studies on TSCI have analyzed patient cohorts from first-world countries.7-10 Particularly, African countries lack adequate TSCI mortality studies as limited resources restrict data availability and quality. 5 Research findings cannot directly be transferred, because the epidemiological and clinical characteristics of TSCI may differ depending on the country’s development status.11,12 In high-income countries the average age of acquiring TSCI has increased, reflecting demographic changes, and the main etiology has shifted from motor vehicle crashes (MVC) to falls, with an increasing proportion of elderly female patients.11,13-15 In developing countries TSCIs continues to primarily affect young males involved in civilian crime or MVC.6,11,12,16 Prior TSCI research has focused on neurological recovery and long-term therapeutic strategies,16-23 but evidence on early mortality is limited.24-29 Recognition of factors associated with early mortality can help rationalize and improve acute TSCI patient care. The present study aims to identify predictors for early mortality in TSCI patients in South Africa.
Materials and Methods
Data Source and Study Population
The Acute Spinal Cord Injury (ASCI) unit database of Groote Schuur Hospital, Western Cape, Cape Town, South Africa was searched for patients admitted between January 2003 and December 2022. This database includes pure SCI patients without other injuries, polytraumatized patients are not admitted to the ASCI unit. The post-discharge mortality status and if applicable, cause of death was validated by matching the patient’s ID numbers with the South African medical research council (MRC) Rapid Mortality Surveillance (RMS) death registry. 30 Patients with prior SCI unrelated to trauma, tumor, or chronic neurological impairment were excluded.
Definitions
The main outcome variable was early mortality status. Early mortality was defined as a survival time equal to or less than 365 days. Survival time was defined as the number of days elapsed from the date of TSCI acquisition to the date of death. Severity of the neurological deficit was based on the American Spinal Injury Association (ASIA) motor Score and categorized into high quadriplegic (ASIA motor Score 0-4), low quadriplegic (ASIA motor Score 5-50), and paraplegic patients (ASIA motor Score >50). Ventilation status (ventilation required yes vs no) and type of neurological injury (complete vs incomplete) were considered as binary variables. In the univariable analysis age was treated as a continuous variable, patients were categorized in age groups: >20, >30, >40, >50, and >60 years. In the multivariable regression model Age groups ≤20, 20-30 (over 20 up to and including 30), 30-40 (over 30 up to and including 40), 40-50 (over 40 up to and including 50), 50-60 (over 50 up to and including 60) and > 60 were formed. The most frequent age group 20-30 was used as the reference group. The odds of age group 20-30 were reported compared to ≤20. In case of no significant association odds ratio with ≤20-year-olds as a reference group were added. Further categorization was based on complication count: 0, ≥1, ≥2, and ≥3 complications. Evaluated complications included respiratory complications (e.g. bronchopneumonia, pulmonary embolism), gastrointestinal complications (e.g. gastrointestinal bledding, ileus, gastritis, gastrointestinal ulcer), urologic (e.g. urinary tract infections, urethral injury), hematologic (e.g. anaemia, deep vein thrombosis, thrombophlebitis), cardiovascular (e.g. arrhythmia, hypotension, cardiac failure), orthopaedical (e.g. failed reduction, implant or construct failure, surgical wound infection), decubitus ulceration (grad II or more), and other complications (miscellaneous complications that do not fall into the before described categories, e.g. severe metabolic disturbance, delirium, meningitis).
Statistical Analysis
Descriptive data are presented as mean ± standard deviations (SD) or counts and percentages (%), age as median and range. To evaluate univariable associations with early mortality simple logistic regression type III Wald tests were used to obtain an unadjusted odds ratio (ORs) with 95% confidence interval (CIs) for each predictor variable.
To identify independent predictors of early mortality, a multivariable regression model was used including all demographic and clinical covariates which are available at admission. Model fit was confirmed using the Homer-Lemeshow goodness-of-fit test, and the model’s predictive capacity was assessed using receiving operating characteristic (ROC) area under the curve. All analyses were performed using IBM SPSS Statistics (Version 27.0, IBM Corporation, Armonk, USA). Tests were two-sided and statistical significance was accepted at the P < 0.05 level.
Results
The search of the computerized medical records ASCI database identified 3223 patients admitted between January 2003 and December 2022. The post-discharge survival status was obtained in 2210 patients who were linked on the RMS death registry. Application of the exclusion criteria left a final dataset of 2204 unique patients. 168 patients deceased within 1 year after acquiring TSCI with 81 in-house deaths. The median age of all patients was 35 (range 9 to 93, Figure 1) and 87% were male patients. Mean ASIA motor Score was 51.6 ± 34.8. Frequency distribution of patients with traumatic spinal cord injury n = 2204.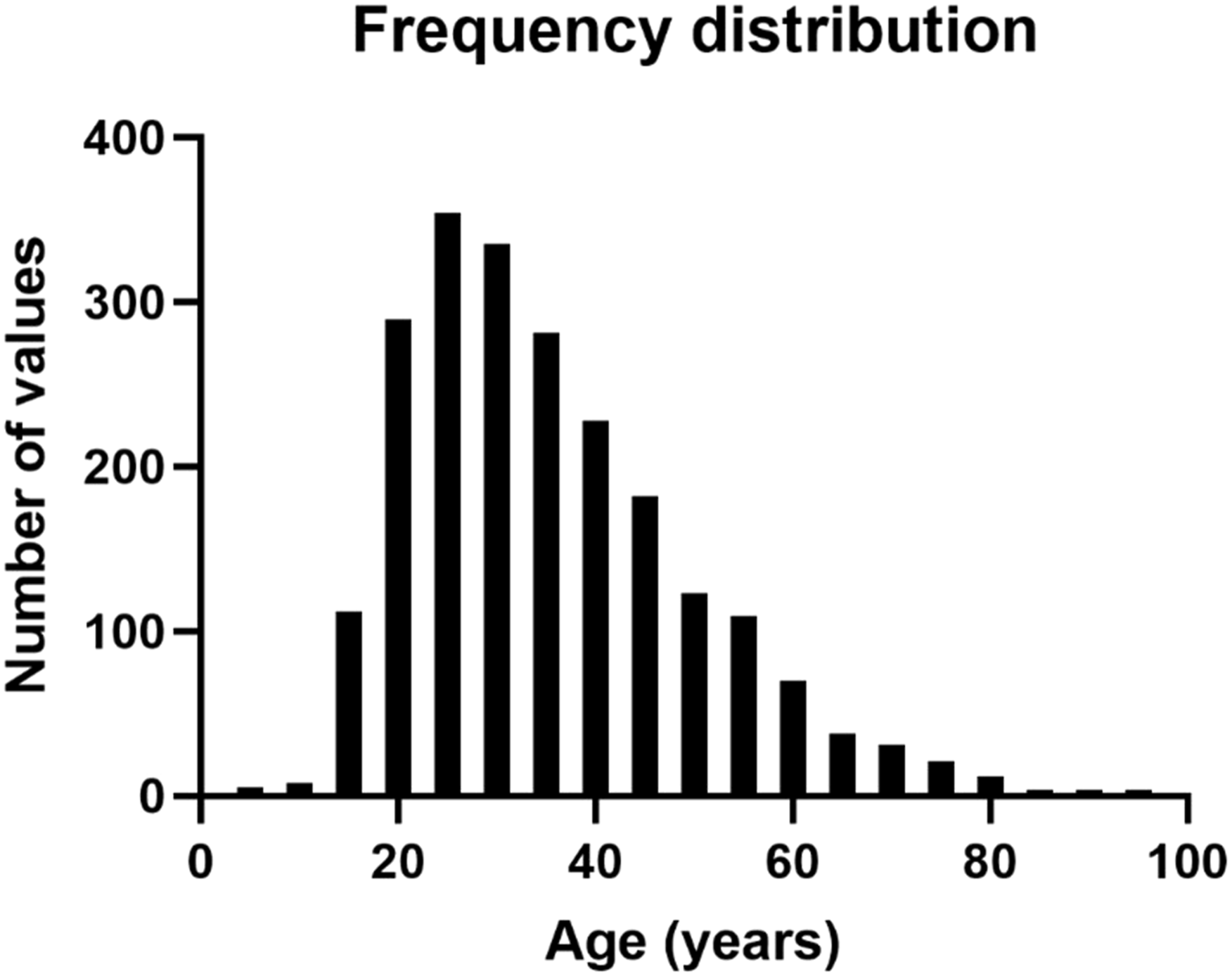
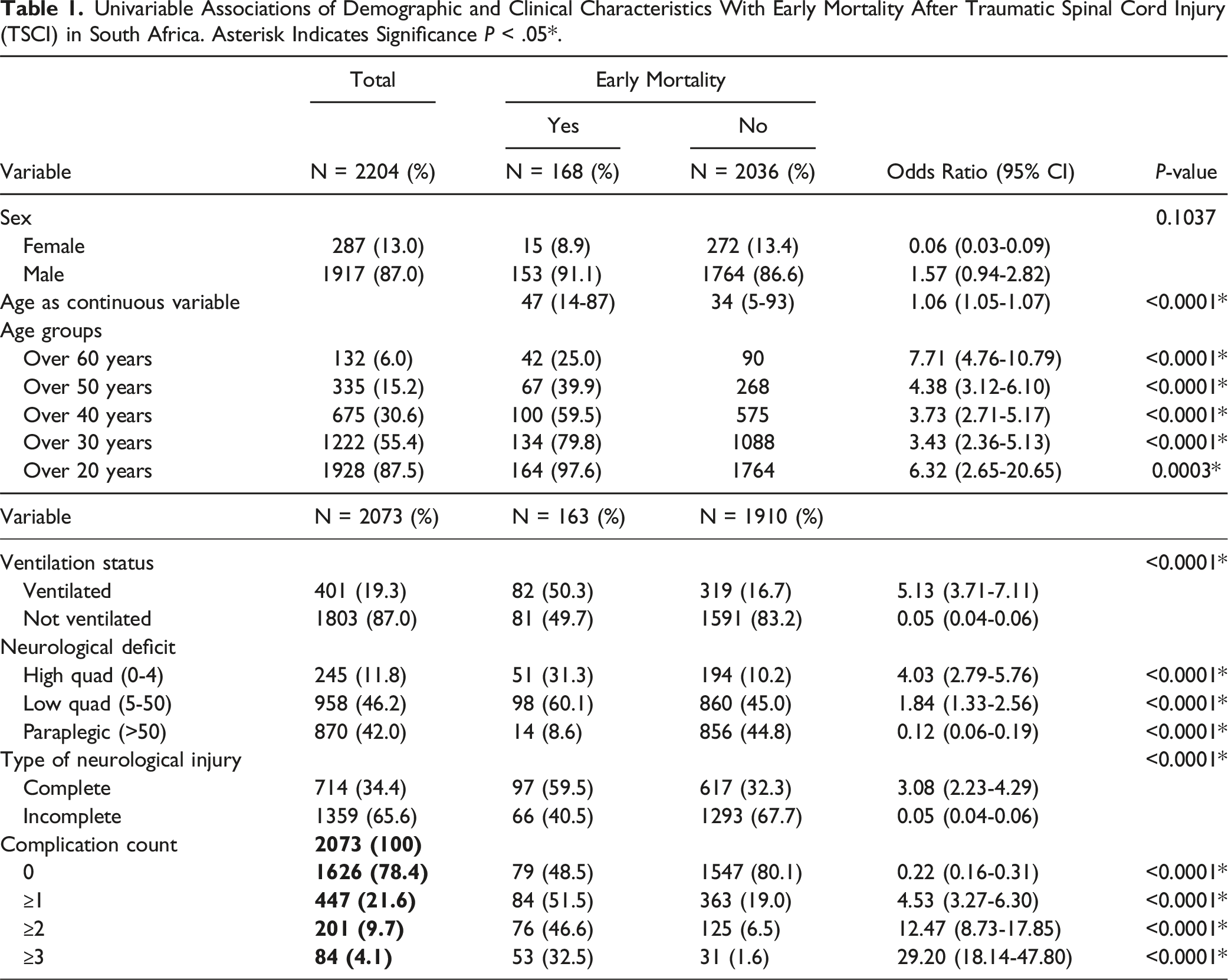
Univariable Associations of Demographic and Clinical Characteristics With Early Mortality After Traumatic Spinal Cord Injury (TSCI) in South Africa. Asterisk Indicates Significance P < .05*.
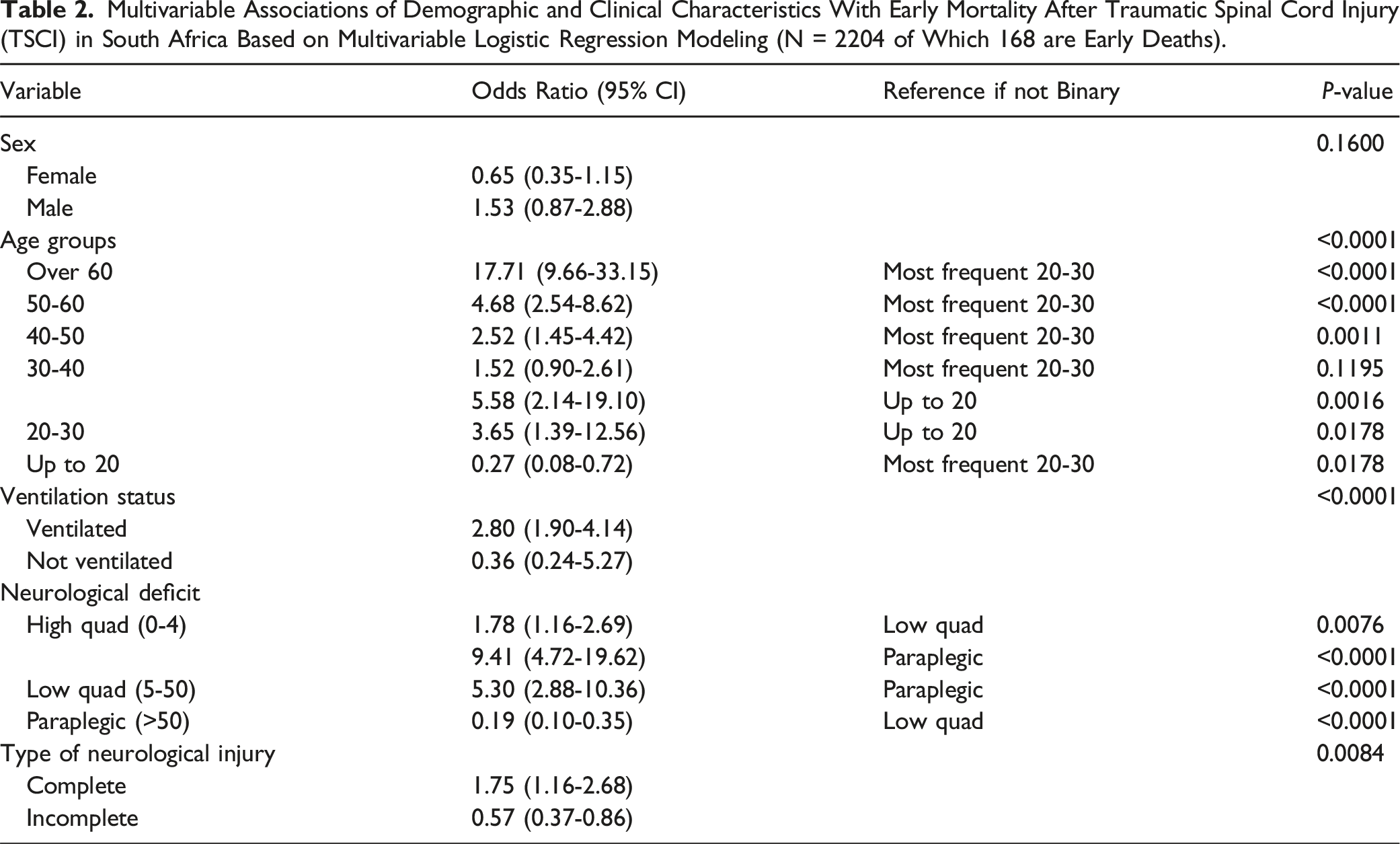
Multivariable Associations of Demographic and Clinical Characteristics With Early Mortality After Traumatic Spinal Cord Injury (TSCI) in South Africa Based on Multivariable Logistic Regression Modeling (N = 2204 of Which 168 are Early Deaths).
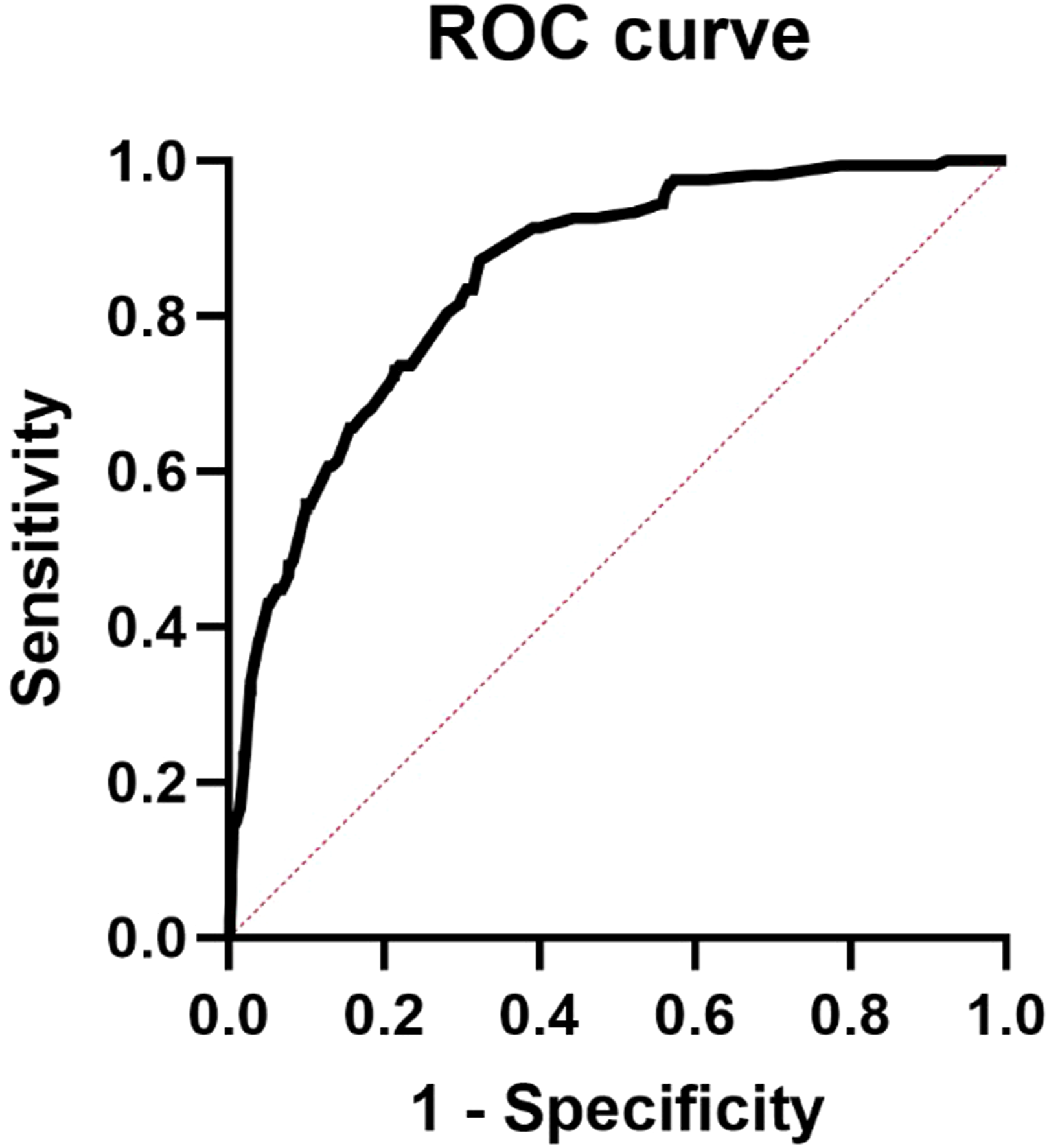
ROC Analysis to assess the multiple logistic regression model fit. Area under the ROC curve 0.85, 95% CI (0.82-0.88, P < .0001).
Demographic Variables
Age increased the odds ratio (OR) of early mortality and a linear relationship between the logit of odds of early mortality and age was identified. Up to age twenty, the relationship between the predicted probability of early mortality and age was linear but relatively flat (Figure 3). There was a stepwise increase of the odds of early mortality from age group over 30 to the older age groups: over 30 years OR = 3.43 (2.36-5.13, P < .0001), over 40 years OR = 3.73 (2.71-5.17, P < .0001), over 50 years OR = 4.38 (3.12-6.10, P < .0001), and over 60 years OR = 7.71 (4.76-10.79, P < .0001). OR of age group over 20 was disproportionately high 6.32 (2.65-20.65, P = .0003), as the age group under 20 was small (N = 276) and showed only 5 early deaths. The univariable association between sex and early mortality was not significant (P = .1037) and neither was the adjusted association (P < .1600). Logistic regression curve of the predicted probability (2a, bottom) and log odds (2b, top) of early mortality versus age. The tick marks indicate the distribution of events (early deaths) by age.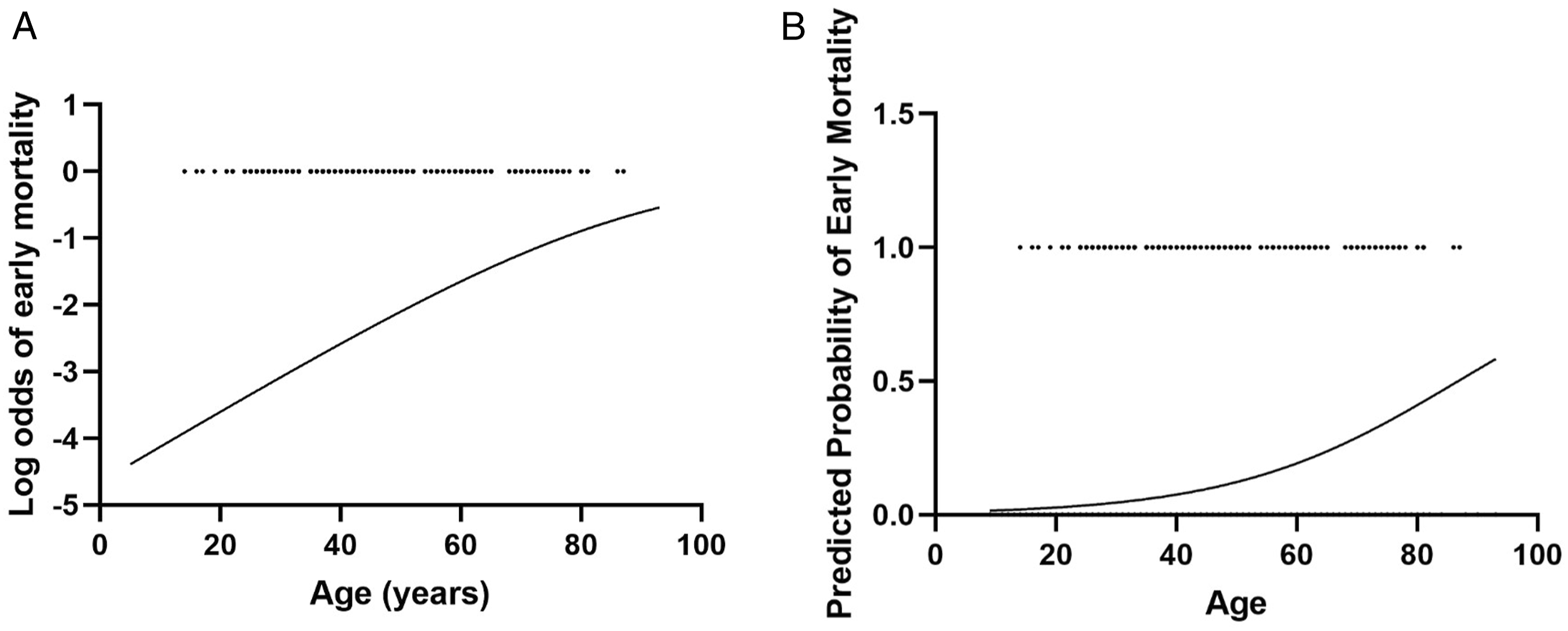
Clinical Variables
Univariable analysis indicated that a complication count of ≥3 significantly increased the odds of early mortality (OR = 29.20, 95% CI (18.14-47.80), P < .0001), as well as a positive ventilation status (OR = 5.11, 95% CI (3.11-7.33), P < .0001). There was a significant association between severity of neurological deficit and the type of neurological injury and early mortality: high quadriplegia (0-4 ASIA motor Score points) increased the odds significantly (OR = 4.03, 95% CI (2.79-5.76), P < .0001), followed by low quadriplegia (OR = 1.84. 95% CI (1.33-2.56), P < .0001), whereas paraplegia significantly reduced the odds of early mortality (OR = 0.12, 95% CI (0.06-0.19), P < .0001). The adjusted analysis showed attenuated associations. The need for ventilation remained a significant predictor (OR = 2.80, 95% CI (1.90-4.14)). In the multivariable analysis paraplegia reduced the odds of early mortality compared to low quadriplegia (OR = 0.189, 95% CI (0.10-0.35)) and high quadriplegia significantly increased the odds (OR = 1.78, 95% CI (1.16-2.69)), as well as completeness of the neurological injury (OR = 1.75, 95% CI (1.16-2.68)). The strongest independent predictor in the multivariable model was Age group over 60 (OR = 17.71, 95% CI (9.66-33.15)) and Age group up to 20 decreased the odds of early death (OR = 0.27, 95% CI (0.08-0.72)), with the most frequent age group 20-30 selected as a reference.
Discussion
To date, large scale data on early mortality of TSCI patients in developing countries is lacking as previous research has focused on data from industrialized nations and long-term mortality. The aim of the present study was to help bridge this gap. Predictors of early mortality after TSCI in South Africa are high complete spinal cord injury, age, number of complications, and the need for ventilation. A predictive multivariable model was developed including the characteristics which are available at admission to help assess the risk of early mortality. Identification of high-risk patients is essential for public resources allocation and improving care to potentially reduce mortality rates.
Among all factors, Age over 60 was found to be the strongest predictor of early mortality followed by number of complications, and ventilation status. A correlation of Age group and complications and mortality is consistent with prior research.7,15,31 Ventilation status has been identified before as an independent predictor for early mortality.32-35 The need for ventilation indicates not only respiratory impairment, but also severe high spinal cord injury, or concomitant thorax trauma. Ventilation status is a simple characteristic readily available at the bedside at no additional cost.
In the present patient cohort, the majority of TSCI patients were of male sex, but there was no significant association with short-term mortality. Prior studies showed that male sex was significantly associated with more severe concomitant systemic injuries. The present dataset included a higher portion of TSCI caused by civilian violence, in particular gang violence, which may have affected the results. Civilian violence involves more males than females, and a different set of injuries such as stabbings and low-velocity gunshot wounds, which may contribute to different results of the present analysis compared to previous studies from first world countries. The mortality risk of individuals involved in civilian crime is disproportionately elevated,36-39 but this may have a greater impact on the long-term mortality.
The current study identified severity of the neurological injury as an independent predictor of early mortality, specifically severe motor deficit of 0-4 ASIA motor Score and complete spinal cord injury. Prior research on TSCI has indicated a direct correlation of long-term mortality with the degree of neurologic impairment. However, more recent US studies have excluded preserved motor function as a protector against early mortality and the authors suggest improvements in the acute care of TSCI patients as a possible explanation of this shift.15,31 In the present study a less severe motor deficit appeared to be protective against early mortality, likely due to the association with less severe injuries and higher levels of autonomy. Given that our cohort included only pure SCI patients and excluded those with polytrauma, the latter seems to play a particularly important role. In South Africa permanent care facilities are scarce and limited bed capacity shortens rehabilitation to approximately 3 to 6 months. SCI patients are then discharged. 40 With many unable to afford ongoing care, autonomy becomes vital, especially when living in poverty or on the streets.
The median age in the present study was 35 years, which is consistent with prior studies. In the US and Canada mean patient age was reported 33 years in the major trauma outcome study. However, recent studies based on data from developed countries note that the mean age of TSCI patients has increased.41,42 The increase in mean age of TSCI patients in developed countries are most likely due to the demographic change, together with the success of prevention efforts targeted at younger people based on seatbelt, helmet laws and education about impaired driving. However, the frequency distribution of the present dataset showed a clear peak for young adult patients. The differences in the age distribution are most likely also due to the different developmental status of the countries. Locally, crime rates are high and a high proportion of TSCI are related to gang violence. Therefore, prevention strategies in South Africa should not only focus on increasing road safety but further aim at reducing the involvement of young individuals in gangs.
The etiology of TSCI has also been described to be changing. 43 In industrialized countries MVC were identified the leading cause for TSCI in early studies.44,45 In more recent years the proportion of TSCI due to falls has increased. 14 A study from Ontario described a similar proportion of falls and MVC (43.2% falls and 42.8% MVC). 46 Analysis of a Canadian dataset from 2006 found that overall MVC accounted for 35% and falls for 31% of TSCI and identified falls as the primary cause of TSCI in 57% of patients older than 60 years and 89% of those older than 80 years. 47 In the present dataset the proportion of stab and gunshot wounds is comparatively high. This further emphasizes substantial differences and need for analysis of mortality data analyses from developing countries.
Limitations
The present study inherits limitations. First, deaths at the scene of the accident are not included in these data and patients with less severe TSCI or transient deficits might not be coded as TSCI. Second, direct causality cannot be determined. This is why the present paper did not distinguish natural and unnatural deaths. Cases recorded as unnatural death in South Africa include homicides, suicides and accidents, while natural causes refer to medical causes of death. Even if the causes of death are a consequence of the TSCI, under South African law, once patients are discharged from acute medical care, these complications become regarded as natural death occurrences. Thus, in this series, the natural deaths recorded were likely caused by complications from the TSCI. Third, the impact of surgical management on early mortality was not analyzed. Including surgical management as a predictor in the present study would have introduced considerable heterogeneity and blurred the results. To adequately examine the effects of surgical management SCIs, types of surgery need to be assessed separately, with the dataset stratified by injury mechanism.
Further research should investigate the predictors of 2-year, 5-year, or long-term mortality after injury respectively post discharge. It needs to be analyzed how management, specifically different types of surgical procedures, impact outcome, early, and long-term mortality.
Conclusion
Predictors of early mortality after TSCI are high complete spinal cord injury, age, number of complications, and the need for ventilation. Identification of high-risk patients is crucial for public resources allocation and optimized care to potentially reduce mortality rates.
Footnotes
Acknowledgments
The authors thank Ria Laubscher (Biostatistics) and Pamela Groenewald (Specialist Scientist) from SAMRC for patient survival data linking.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data and materials are available on reasonable request.