
Abstract
Study design:
Technical report on cadavers.
Objective:
To evaluate preliminary feasibility and safety of lumbar sagittal alignment correction with anterior hyperlordotic cages used to overpower previous posterior spinal instrumentation.
Methods:
Hyperlordotic 30° anterior lumbar interbody fusion (ALIF) cages were inserted in collapsed L5-S1 disc space of 2 cadavers to overpower prior posterior L5-S1 pedicle screws and rod constructs. A distinct technique of opening up the disc space and creation of intersegmental lordosis was employed using a large endplate distractor and transforaminal lumbar interbody fusion (TLIF) paddle distractor. Assessment of increase in the intersegmental lordosis (ISL) was made using lateral fluoroscopic imaging. Postprocedural computed tomography (CT) scans were obtained to evaluate any failure of posterior instrumentation and to serve as a surrogate marker for bone quality.
Results:
The 2 cadavers selected (from an available number of 10) were males: 82 and 84 years of age, respectively. Both had marked L5-S1 disc space collapse. The ISL achieved with hyperlordotic cages was 27.6° for the first cadaver (up from 4.9°) and 23.1° for the second one (up from 4.6°). No obvious screw-rod failure or cutout of instrumentation occurred. Postprocedure CT scans did not reveal any loosening of screws or cutout through endplates. Hounsfield unit values calculated on axial CT cuts were 73.50 (osteoporosis) and 80.70 (osteopenia) respectively for the 2 cadavers.
Conclusion:
Based on the results of the cadaveric experiment, overpowering of posterior instrumentation can be effectively achieved. Biomechanical and clinical studies are indicated to further evaluate the suitability and safety of this technique.
Keywords
Introduction
The importance of restoration of sagittal spinopelvic alignment in adult spinal deformity (ASD) is well established. 1 -4 Sagittal malalignment secondary to flatback deformity, presenting in patients with previous posterior spinal instrumentation and fusion, is of major concern. Management of these cases is challenging and requires meticulous planning for restoration of overall spinal alignment and balance. Three-column osteotomies (pedicle subtraction osteotomy and vertebral column resections) have been popularized over the past 2 decades for posterior correction of lumbar flatback deformity. However, apart from being technically demanding, they are associated with a very high complication rate; as is being increasing reported in the literature. 5 -8 Alternatively, alignment correction from the front, in the presence of intact posterior instrumentation, has been classically described by a 3-stage back-front-back approach. Here, removal of posterior instrumentation is required before attempting correction from the front, followed by reinstrumentation from the back again. This adds significantly to the length and the complexity of the surgery with the need for repeated patient repositioning, if done under a single anesthesia event. Instead, the authors propose the use of hyperlordotic anterior lumbar interbody fusion (ALIF) cages to overpower posterior instrumentation, without it’s prior removal. The authors report their experience with this novel technique on two cadavers, and evaluate its preliminary feasibility.
Materials and Methods
Cadavers from the human tissue lab from the manufacturer of hyperlordotic cages (Nuvasive Inc, San Diego, CA) were selected with the following criteria: age more than 70 years and collapsed 5/1 disc space. Exclusion criteria were previous compression fractures or evidence of previous lumbar spine surgery.
Lateral C-arm fluoroscopy was used to screen lumbar spines on all cadavers available at the time of the study. Based on the outlined criteria, 2 suitable cadavers were found from a total of 10 available ones. Both of them had marked disc height collapse at L5-S1 level, with loss of intersegmental lordosis (ISL) at that level.
Key steps of the surgical technique performed on both cadavers are outlined below.
A standard posterior midline exposure was done for instrumentation at L5-S1 level. Polyaxial 6-mm titanium pedicle screws were inserted and connected securely with 5.5 titanium rods. The L5-S1 ISL was measured on lateral C-arm fluoroscopy after placement of the posterior instrumentation construct.
The cadavers were then flipped for the ALIF procedure. An anterior retroperitoneal approach was done to access the L5-S1 disc from the front. Distraction of the disc space and desired ISL was achieved by complete release of the anterior longitudinal ligament (ALL) and extensive discectomy back to the posterior longitudinal ligament (PLL), with further release of the PLL. A large paddle endplate distractor was used for this purpose, after the discectomy release, to pry open the disc space gradually. In order to give more power to the distractor, small transforaminal lumbar interbody fusion (TLIF) flat bullet nose distractors were inserted in between the large distractor paddle blades and rotated 90° in place, clockwise and counterclockwise, to further open up the disc space (refer to Figure 1 demonstrating the technique in the first cadaver). The TLIF flat bullet nose distractor started at 8 mm of height going up progressively to 12. Also, the large paddle endplate distractor was inserted deep and as far as possible up to the posterior rim of the endplates; to avoid breaking the end plates during distraction and to bring about gradual controlled overpowering of posterior instrumentation. Hyperlordotic cage (HLC) template was then inserted in order to further open up the disc space before the final HLC was set in with screws through the endplates. The system used was Nuvasive Brigade HL ALIF System (30° hyperlordotic PEEK ((polyetheretherketone) cage with 20 mm anterior height and 8 mm posterior height). Lateral C-arm fluoroscopy images were obtained to measure the increase in L5-S1 ISL following the procedure.
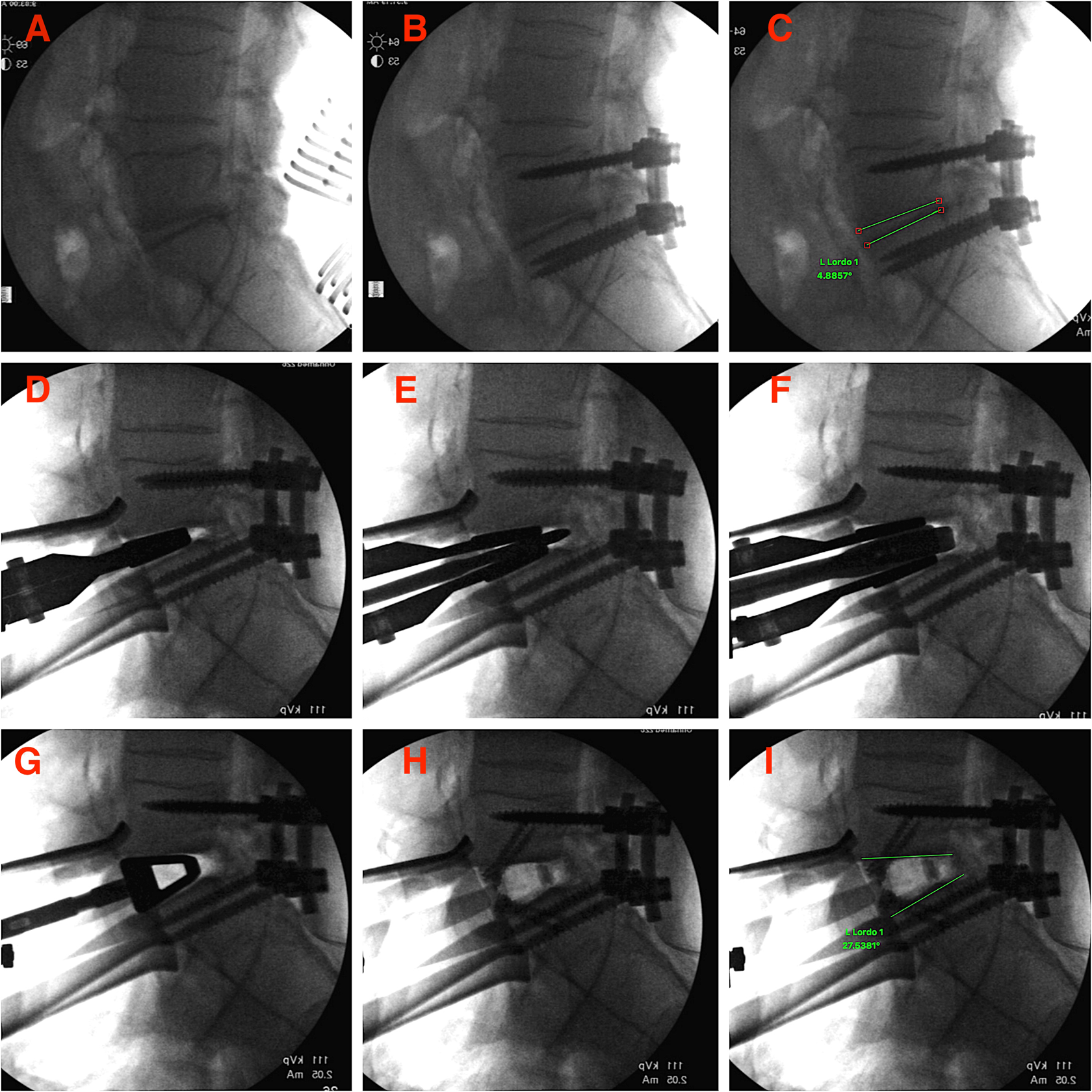
Sequential steps in the technique of “overpower” for cadaver 1 as demonstrated on fluoroscopy. (A) Posterior exposure of L5-S1 level. (B) Pedicle screws with rods inserted. (C) L5-S1 lordosis measured at 4.9°. (D) Insertion of the large endplate distractor. (E) TLIF paddle distractor inserted in between the blades of the endplate distractor. (F) TLIF distractor rotated 90° to pry open the disc space. (G) Insertion of trial device for the hyperlordotic cage. (H) Thirty degree hyperlordotic PEEK cage inserted and secured with endplate screws. (I) Final L5-S1 lordosis obtained measured at 27.6°. PEEK, polyetheretherketone; TLIF, transforaminal lumbar interbody fusion.
Once the procedure was performed, the cadavers were flipped and the posterior instrumentation was inspected for any gross loosening or failure of the construct. Postoperative computed tomography (CT) scan were ordered to evaluate any loosening at the bone-screw interface and end plate changes or subsidence, as well as to assess the degree of osteoporosis. Hounsfield unit (HU) measurements were done at the level of L3 vertebral bodies to evaluate osteoporosis. Three measurements from 3 different levels of axial cuts at L3 vertebral body of each cadaver were averaged out, according to the technique described by Schreiber et al. 9,10
Results
Both cadavers chosen in accordance with the criteria listed above were males. The ages of the cadavers, as found to be on record with the laboratory, were 82 and 84 years, respectively.
Cadaver 1 (82 years age): The ISL in the first case increased from 4.9° to 27.6° (Figure 1). There was no gross change in the posterior instrumentation after the insertion of the HLC. No loosening at the bone screw interface or endplate impaction was found on the postprocedure CT scan (Figure 2). The mean HU value obtained at the L3 level was 73.50 (which correlated with osteoporosis).
Cadaver 2 (84 years age): In view of a large bridging anterior osteophyte, access to the L5-S1 disc space was more challenging in the second case. An osteotomy was performed to take down the osteophyte in order to reach the disc space. Also, mild impaction of the posterior aspect of the L5 inferior endplate occurred during disc space preparation with the paddle distractor. This, however, did not preclude the placement of HLC and overpowering the posterior pedicle screw construct could be achieved. The ISL in this case increased from 4.6° to 23.1° (Figure 3). Inspection of the posterior instrumentation after the insertion of the HLC showed intact instrumentation. Postprocedure CT scan (Figure 4) did not demonstrate any loosening at the bone-screw interface; however, mild L5 inferior endplate impaction, as noticed on the lateral C-arm fluoroscopy was evident. The mean HU value calculated at the level of L3 body was 80.70 (correlating with osteopenia).
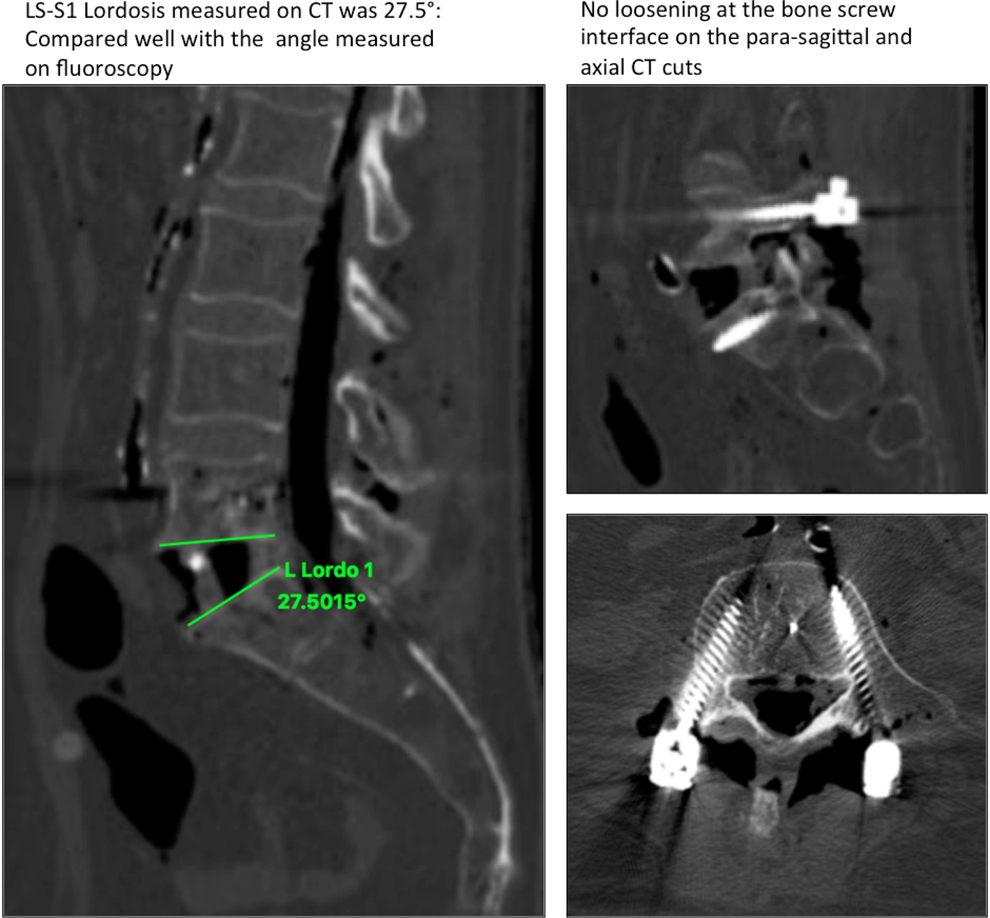
Postprocedure computed tomography scan on cadaver 1 showing calculated lordosis and no evidence of screw loosening or cutout on the parasagittal and axial cuts.
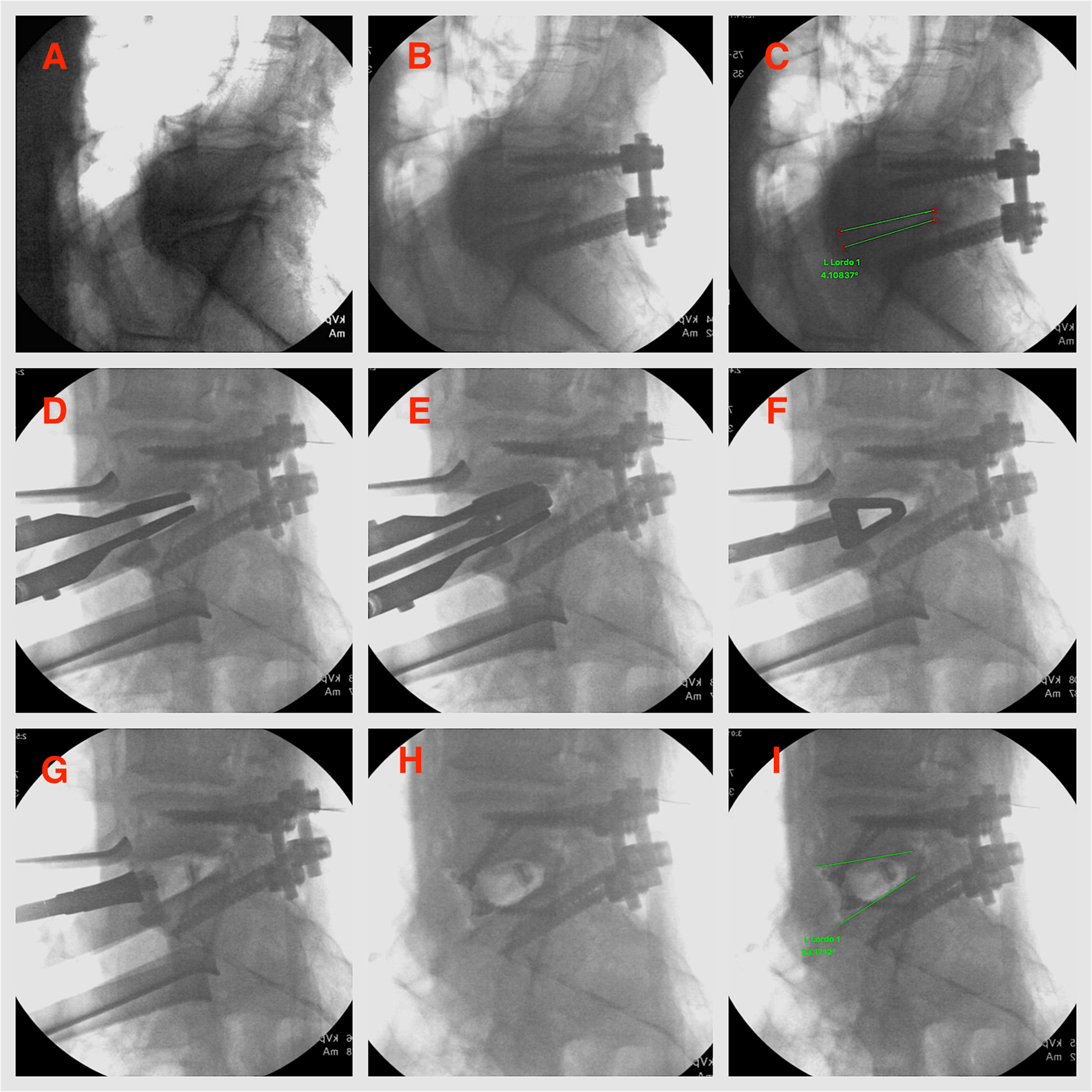
Sequential steps in the technique of “overpower” for cadaver 2 as demonstrated on fluoroscopy. Notice the bridging anterior osteophyte at L5-S1. (A) Posterior exposure of L5-S1 level. (B) Pedicle screws with rods inserted. (C) L5-S1 lordosis measured at 4.6°. (D) Insertion of the large endplate distractor. (E) TLIF paddle distractor inserted in between the blades of the endplate distractor and rotated 90° to pry open the disc space. (F) Insertion of the trial device. Notice mild inferior L5 endplate impaction. (G) Insertion of the 30° hyperlordotic PEEK cage. (I) Hyperlordotic PEEK cage secured with endplate screws. (I) Final L5-S1 lordosis obtained measured at 23.1°. PEEK, polyetheretherketone; TLIF, transforaminal lumbar interbody fusion.
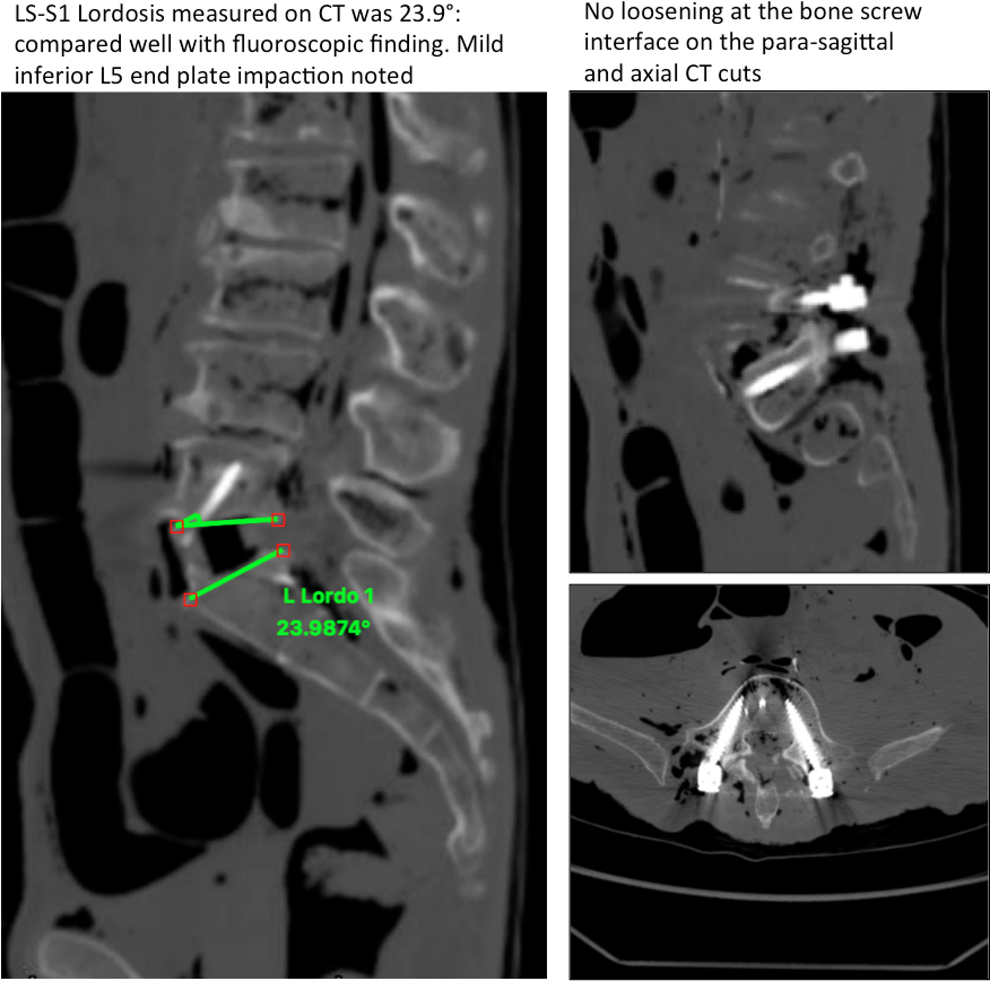
Postprocedure computed tomography scan on cadaver 2. Notice the mild inferior endplate impaction of the L5 body. There is no evidence of screw loosening or cutout.
Thus, overpowering of the posterior pedicle screw instrumentation could be successfully achieved in both cadavers, with significant restoration of ISL. The gain in the ISL was, however, slightly less in the second cadaver, due to mild inferior end plate impaction at L5. No loosening at the bone-screw interface, or cutout of the screws though the endplates or rod failures were noticed in either case.
Discussion
Sagittal malalignment associated with flatback deformity, either primary or iatrogenic, is one of the major indications for spine surgery in the aging population. 11 To deal with iatrogenic flatback deformity in presence of previous posterior instrumentation, 2 conventional strategies are described. Posterior only approach (with either simple Smith Petersen osteotomies or 3-column osteotomies) or combination of anterior and posterior approaches. 12,13
Posterior osteotomies allow removal of previous instrumentation and correction through the same approach. They also allow for a large angular correction at a single level. However, the main drawback is that they require extensive work around epidural scar tissue, which is an inherently risky task. Complication rates as high as 42% have been reported with 3-column osteotomies in the literature. 5
The second option is a combination of anterior and posterior approaches and often involves a “back-front-back” procedure. This requires removal of posterior instrumentation with posterior releases, repositioning the patient for anterior surgery, performing anterior lumbar interbody fusion and then flipping the patient prone again to finalize the posterior instrumentation with contoured rods. Obvious pitfalls of this approach are significant increase in procedural time, cumbersome repositioning (if attempted under a single anesthesia event) and potentially higher blood loss. The risk of having kick out of the anterior cages, during the posterior correction at the time of finalizing the posterior instrumentation is another potential issue. An alternative solution lies in the use of anterior HLCs (locked in with endplate screws) to overpower posterior instrumentation from the front; thus converting it to a simpler front-back procedure instead of a 3-stage procedure. Anterior correction with HLCs can also avoid the need for extensive 3-column osteotomies in the scar tissue posteriorly.
The thought of overpowering posterior spinal instrumentation inherently brings a few biomechanical concerns in the reader’s mind. Failure of the posterior rods and screws with breakage and cutout, endplate damage, vertebral body fractures, neurological injury are some of the prominent complications that may arise if a meticulous and gradual correction technique is not followed. The authors in this article aimed to investigate whether overpowering of posterior constructs with anterior HLCs, can be safely performed from a technical perspective without encountering or minimizing the aforementioned complications.
Cadavers with collapsed L5-S1 disc levels were selected, as the impact on overall sagittal plane is maximum, when lordosis is corrected as distally as possible in the lumbar spine. This is also in accordance with the concept that two-thirds of lumbar lordosis should be anatomically distributed from L4-S1 levels. 14 Additionally, cadavers with advanced age were chosen to determine if this technique could be safely applied in osteoporotic/osteopenic spines, as would be an expected finding in the geriatric population.
A unique disc space distraction technique using a TLIF distractor (flat bullet nose distractor) rotated in between the blades of a large endplate paddle distractor was employed. This enabled us to gradually and safely crack open the PLL and achieve controlled distraction to accommodate the HLC. Significant lordosis correction could be attained in both cadavers with this technique, as was discussed in the results. The endplate impaction that occurred in the second cadaver was likely due to the large paddle distractor not being positioned far enough posteriorly in the disc space. The authors highly recommend that distraction be attempted with the paddle blades seated deeply inside the disc space with maximum endplates contact, to allow a larger area of force dissipation.
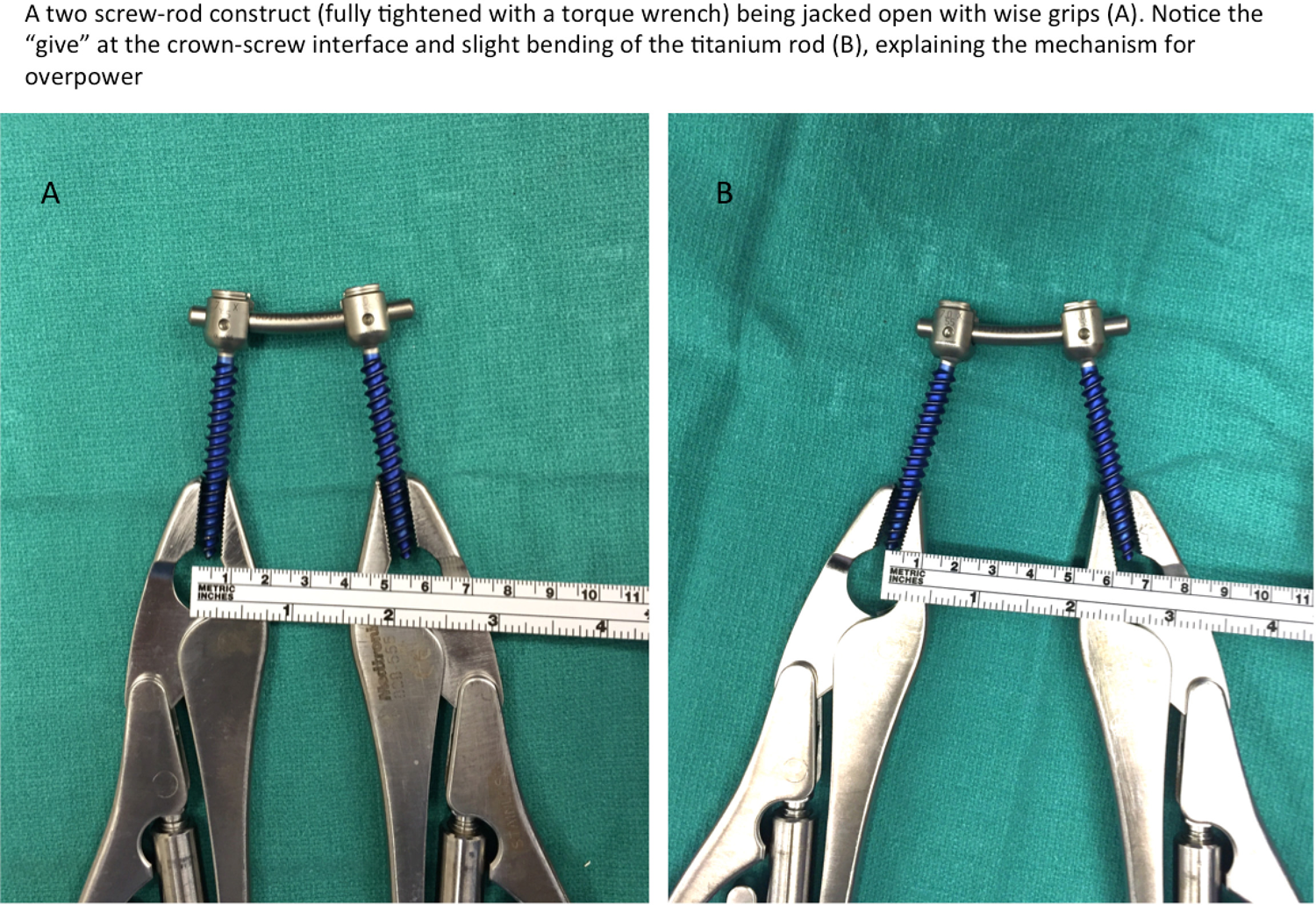
Overpowering of the posterior poly-axial screw-rod construct, in the authors’ opinion, is via the slight angular “give” occurring at the crown-screw interface (as depicted in Figure 5), the slight flexibility of the titanium rods and some minor “give” additionally at the bone screw interface. Six-millimeter polyaxial titanium screws with 5.5-mm titanium rods were chosen for this study as they are commonly used in contemporary adult spine surgery. Monoaxial screws, being far less likely to be used in adult deformity surgery, were not tested in this study. However, with monoaxial screws, it is expected that the correction with overpower technique would be of a much lesser magnitude, since the “give” at the crown-screw interface would not occur. Also, screws or rods made up of other stiffer alloys such as cobalt chrome or stainless steel were not tested. This is an important drawback of the study and the authors also do not recommend their technique when posterior instrumentation consists of these stiffer material constructs. Results with stiffer metal alloys may not be the same as with titanium implants, which have slight elasticity compared with the stiffer alloys.
An illustration depicting the proposed mechanism of “overpower” in polyaxial titanium screw rod constructs.
The presence of posterior fusion masses and fibrous scar tissue are also likely to impede overpowering. These factors could not be accounted for and tested on the cadavers. In the presence of a posterior fusion without instrumentation, overpowering may be still achievable, depending on the extent, the thickness, and the quality of the fusion mass. The thinner and less consolidated the fusion mass, the more the likelihood of achieving correction. As a corollary to this, extensive posterolateral fusion may prove counterintuitive for attempting this technique. Posterior fusion masses along with instrumentation may make overpowering very challenging to achieve, and in the authors’ opinion should not be attempted, unless there are signs of pseudarthrosis on imaging, at the intended levels of overpower. In the clinical scenario, a case-by-case evaluation of the CT imaging to look for the extent and quality of posterior fusion is invariably recommended.
Another drawback of the study was that this technique was tested at only 2 disc space levels in 2 cadavers, both being L5-S1 levels; since only 2 from an available number of 10 cadavers met the inclusion criteria that were outlined for their selection. On the brighter side, we were able to test this technique in the most worst-case scenarios (advanced age of cadavers, severely collapsed disc space, suboptimal bone quality); thus, establishing the feasibility of this technique. As the higher lumbar disc spaces were relatively well preserved in the cadavers, the technique was not attempted at those proximal levels. Additionally, this technique, in the authors’ opinion, may be most suited for the L5-S1 level, as the S1 endplate tends to the densest and strongest endplate in the lumbosacral spine, accommodating very well the stresses during disc space distraction. From the limited experience we had on cadavers, it cannot be predicted if similar correction can also be achieved safely at levels proximal to L5-S1.
Finally, at the conclusion of the procedure, CT scans of lumbar spines were obtained on both cadavers to evaluate signs of posterior instrumentation failure and endplate damage. Although no loosening around the screws or screw cutout was noticed, there was mild endplate impaction of the posterior aspect of the L5 inferior endplate of the second cadaver, as acknowledged and explained above. In spite of this, good correction was achieved, though of a slightly lesser magnitude than in the first cadaver. The measurements of increase in the ISL on fluoroscopy also correlated well with the values calculated on sagittal CT images.
CT also proved to be valuable in establishing osteoporosis/osteopenia in both cadavers through calculations of HU. The L3 level was chosen for this as it was away from the area of dissection and instrumentation and was less likely to be affected by artifacts from the instrumentation below. The measurements of the HUs were done using the method described by Schreiber et al. 9,10 The HU values of 75.50 and 80.70 calculated, respectively, for the 2 cadavers, were in the range of osteoporosis and osteopenia, respectively, as correlated with T scores on dual x-ray absorptiometry (as per the reference data established in the study by Schreiber et al. 9 ). The mean normative value for males in the age group of 81 to 89 years published by Schreiber et al 9 was 90.0 (±25.5). A HU score of 78.5 (±32.4) correlated with osteoporosis (T score less than or equal to −2.5), while a score of 100.8 (±24.5) correlated with osteopenia (T score between −1 and −2.5) in the study by Schreiber et al. Thus, in our case, the first cadaver can be considered osteoporotic (mean HU score 75.50) while the second one bordered on osteoporosis/osteopenia (mean HU score 80.70). This lends further support to the feasibility of the overpowering technique, as it could be performed even in cadavers with presumably poor bone quality.
Conclusion
Based on the experience with cadavers, the technique of overpowering posterior spinal instrumentation and fusion with anterior HLCs can be regarded as an effective one. This may prove to be a valuable addition to the techniques available for managing revision adult spinal deformity cases. When properly planned and carefully executed, it may also be feasible, to some extent, in osteopenic/osteoporotic vertebral bone. However, further biomechanical and clinical studies are required to validate this novel technique and establish its wider applicability.
Footnotes
Acknowledgements
The authors acknowledge Nuvasive Inc for providing access to their cadaver lab for the study and allowing their instrumentation to be used.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.