
Abstract
Study Design:
Retrospective analysis of prospectively collected data.
Objectives:
Adult spinal deformity (ASD) surgery is a highly complex procedure that has high complication rates. Risk stratification tools can improve patient management and may lower complication rates and associated costs. The goal of this study was to identify the independent association between American Society of Anesthesiologists (ASA) class and postoperative outcomes following ASD surgery.
Methods:
The 2010-2014 American College of Surgeons National Surgical Quality Improvement Program database was queried using Current Procedural Terminology and International Classification of Diseases, Ninth Revision, codes relevant to ASD surgery. Patients were divided based on their ASA classification. Bivariate and multivariate logistic regression analyses were employed to quantify the increased risk of 30-day postoperative complications for patients with increased ASA scores.
Results:
A total of 5805 patients met the inclusion criteria, 2718 (46.8%) of which were ASA class I-II and 3087 (53.2%) were ASA class III-IV. Multivariate logistic regression revealed ASA class to be a significant risk factor for mortality (odds ratio [OR] = 21.0), reoperation within 30 days (OR = 1.6), length of stay ≥5 days (OR = 1.7), overall morbidity (OR = 1.4), wound complications (OR = 1.8), pulmonary complications (OR = 2.3), cardiac complications (OR = 3.7), intra-/postoperative red blood cell transfusion (OR = 1.3), postoperative sepsis (OR = 2.7), and urinary tract infection (OR = 1.6).
Conclusions:
This is the first study evaluating the role of ASA class in ASD surgery with a large patient database. Use of ASA class as a metric for preoperative health was verified and the association of ASA class with postoperative morbidity and mortality in ASD surgery suggests its utility in refining the risk stratification profile and improving preoperative patient counseling for those individuals undergoing ASD surgery.
Keywords
Introduction
As the elderly population in the United States continues to rise and is projected to nearly double by 2050, 1 adult spinal deformity (ASD) is becoming increasingly prevalent. The United States Bone and Joint Initiative estimates a total of $75.8 billion in hospital discharge costs related to spinal deformity disorders, with 65% of that cost being derived from scoliosis, spondylolisthesis, and other spondylopathies. 2 Additionally, conservative estimates of complications from ASD surgery tally to $5.4 billion, with complication rates ranging from 13% to 59%. 3 Although there are continued developments in techniques, instrumentation, and anesthesia in the realm of ASD surgery, 3,4 the increasing emphasis on cost containment and restructuring of compensation schemes have prioritized the utility of potential risk stratification tools to predict complications and improve perioperative planning and management.
The American Society of Anesthesiologists (ASA) Physical Status classification system was originally developed as a variable for statistical tabulations. 5 The original goal of the ASA class system was to assess overall preoperative physical status of the patient and not surgical risk per se because it does not include the impact of surgery on the patient’s outcomes. However, since then, multiple studies have demonstrated and emphasized its potential as a useful proxy for judging patients’ operative risk and as a predictor for postoperative complications, particularly in spinal surgeries. 6 –13 Because the score is assigned preoperatively based on the patient’s preoperative health, ASA classifications have the potential to be an accessible tool for surgeons to gauge patient risk for postoperative complications.
Prior literature exploring the utility of preoperative factors, especially ASA class, in ASD surgery has conflicting results (Table 1). Schwab et al conducted a multicenter, retrospective study of ASD patients and found no significant differences in ASA class between the cohorts with complications and without complications. 14 However, Tang et al identified ASA class to be an independent risk factor for major complications in ASD surgery, while Pateder et al also found an association between a higher ASA class ranking and patient mortality. This study seeks to help resolve these conflicts from previous works by investigating the capability of ASA class to predict adverse postoperative events using the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database.
Prior Literature Overview for ASA Class Utility in ASD Surgery.
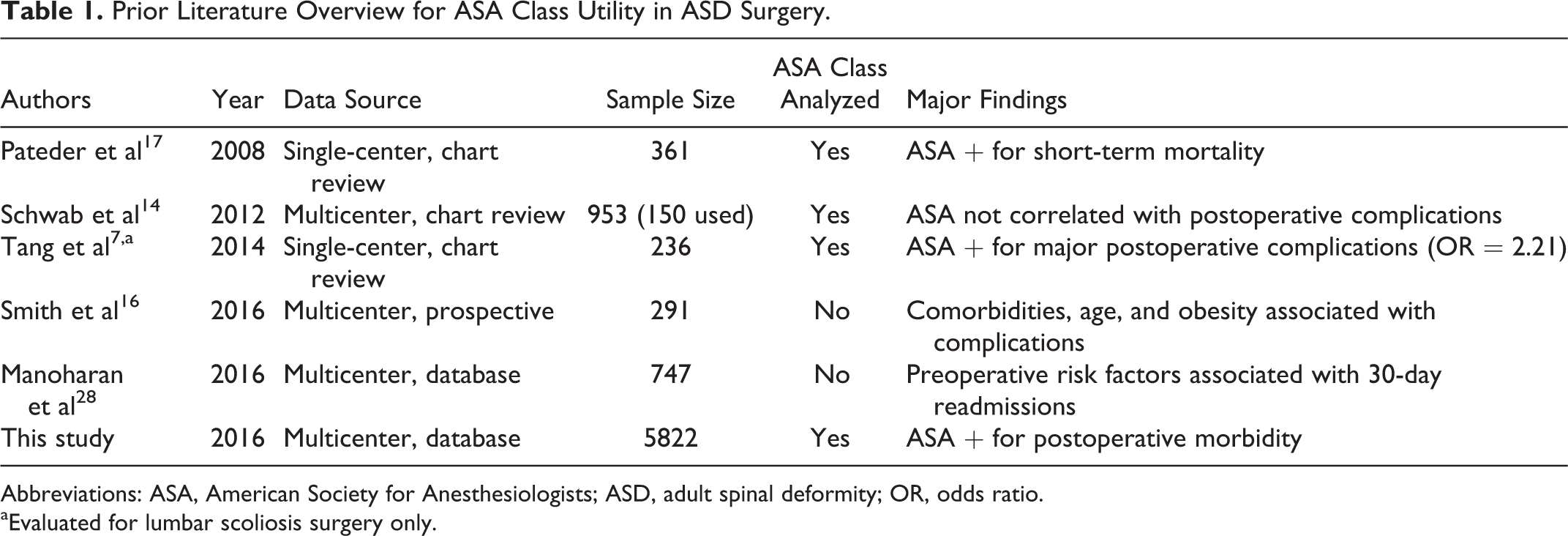
Abbreviations: ASA, American Society for Anesthesiologists; ASD, adult spinal deformity; OR, odds ratio.
aEvaluated for lumbar scoliosis surgery only.
Materials and Methods
This was a retrospective study of prospectively collected data in the 2010-2014 ACS-NSQIP database. NSQIP is a large national database with risk-adjusted 30-day postoperative morbidity and mortality outcomes. More than 500 hospitals that vary in size, socioeconomic location, and academic affiliation contributed data to the 2010-2014 ACS-NSQIP database. 15 NSQIP data is collected prospectively by dedicated clinical abstractors at each institution on more than 150 demographic, preoperative, intraoperative, and 30-day postoperative variables. These on-site surgical clinical reviewers stringently maintain the fidelity of the NSQIP database, and they conduct ongoing internal auditing processes to analyze interrater reliability and to ensure accuracy of data collection.
Inclusion Criteria
The NSQIP database from 2010 to 2014 was used in this study. Adult patients (≥18 years) undergoing spinal fusion for deformity were identified based on Current Procedural Terminology (CPT) codes 22 800, 22 802, 22 804, 22 808, 22 810, 22 812, 22 818, and 22 819. CPT codes 22 843, 22 844, 22 846, or 22 847 were also included to capture long, multilevel fusion constructs. Patients with CPT codes 22 842 and 22 845 were included if they had an ICD-9 (International Classification of Diseases, Ninth Revision) diagnosis for spinal deformity (including 737.1, 737.2, 737.3, 737.4, 737.8, and 737.9). Cases with missing preoperative data; emergency cases; patients with a wound class of 2, 3, or 4; an open wound on their body; current sepsis; current pneumonia; prior surgeries within 30 days; cases requiring cardiopulmonary resuscitation prior to surgery; any patients undergoing a nonelective procedure; or cases with diagnoses of cervical spine, trauma or injury to spine, or neoplasm of spine were excluded in order to reduce the risk of confounding variables.
Variable Definition
Patient demographic variables included sex, age (≥65 years old), and race (white, black, Hispanic, and other). Other race included American Indian, Alaska Native, Asian, Native Hawaiian, Pacific Islander, or unknown/not reported. Preoperative variables included operation year, obesity (body mass index ≥30 kg/m2), diabetes (non–insulin-dependent diabetes mellitus or insulin-dependent diabetes mellitus), current smoking (within 1 year of surgery), dyspnea (≤30 days prior to surgery), functional status prior to surgery (independent or dependent/partially dependent ≤30 days prior to surgery), pulmonary comorbidity (ventilator dependent ≤48 hours prior to surgery or history of chronic obstructive pulmonary disease ≤30 days prior to surgery), cardiac comorbidity (use of hypertensive medication or history of chronic heart failure ≤30 days prior to surgery), renal comorbidity (acute renal failure ≤24 hours prior to surgery or dialysis treatment ≤2 weeks prior to surgery), steroid use for chronic condition (≤30 days prior to surgery), ≥10% loss of body weight (in the last 6 months), bleeding disorder (chronic, active condition), and preoperative transfusion of ≥1 unit of whole/packed red blood cells (RBCs; ≤72 hours prior to surgery).
Intraoperative variables included fusion length (long fusion is ≥4 levels during an anterior approach and ≥7 levels during a posterior approach), surgical approach (posterior, anterior, or combined), bone graft, fusion to pelvis, osteotomy, operative time (≥4 hours), and total relative value units. Thirty-day postoperative outcome variables include mortality, any postoperative complication, length of stay (LOS; ≥5 days), wound complication (superficial or deep surgical site infection, organ space infection, or wound dehiscence), pulmonary complication (pneumonia, unplanned reintubation, or duration of ventilator-assisted respiration ≥48 hours), venous thromboembolism (pulmonary embolism or deep vein thrombosis), renal complication (progressive renal insufficiency or acute renal failure), urinary tract infection (UTI), peripheral nerve injury, cardiac complication (cardiac arrest requiring cardiopulmonary resuscitation or myocardial infarction), intra-/postoperative transfusion, sepsis, central nervous system complication (cerebrovascular accident or coma), reoperation (related to initial procedure), and unplanned readmission (related to initial procedure). ACS-NSQIP provides further information on variable characteristics. 16
Patients were split up into 4 cohorts according to their assigned ASA classification score of 1, 2, 3, and 4. Exclusion criteria discussed above removed any instances of ASA classes 5 or 6 and so was not considered.
Statistical Analysis
Bivariate analyses were performed on patient demographic, preoperative, intraoperative, and postoperative characteristics using Pearson’s χ2 test. Fischer’s exact test was used where appropriate. Multivariable logistic regression analysis, with stepwise entry and removal criteria set to a significance level of .05, was performed to identify postoperative outcomes with which the higher ASA classes were associated. The c-statistic, which is the area under the receiver operating characteristic curve, was also retrieved from the predictors of postoperative outcomes models and determined the accuracy of this model. The area under this curve measures the ability of the model to correctly classify those with the complication and those without. SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC) was used for all statistical analysis.
Results
Study Population
A total of 5803 patients met the inclusion criteria for the study, of which 155 (2.7%) patients were ASA class I, 2561 (44.1%) patients were ASA class II, 2927 (50.4%) patients were ASA class III, and 160 (2.8%) patients were ASA class IV (Table 2). Patients with ASA class IV were more likely to be male, ≥65 years of age, black, obese, diabetic, dyspneic, partially or totally functionally dependent, pulmonary comorbid, cardiac comorbid, renal comorbid, smokers, use steroids, have recent weight loss, bleeding disorder, longer operation times, osteotomy, fusion to pelvis, longer fusion lengths, and posterior surgical approach.
Patient Demographics, Comorbidities, and Intraoperative Variables (N = 5803).a
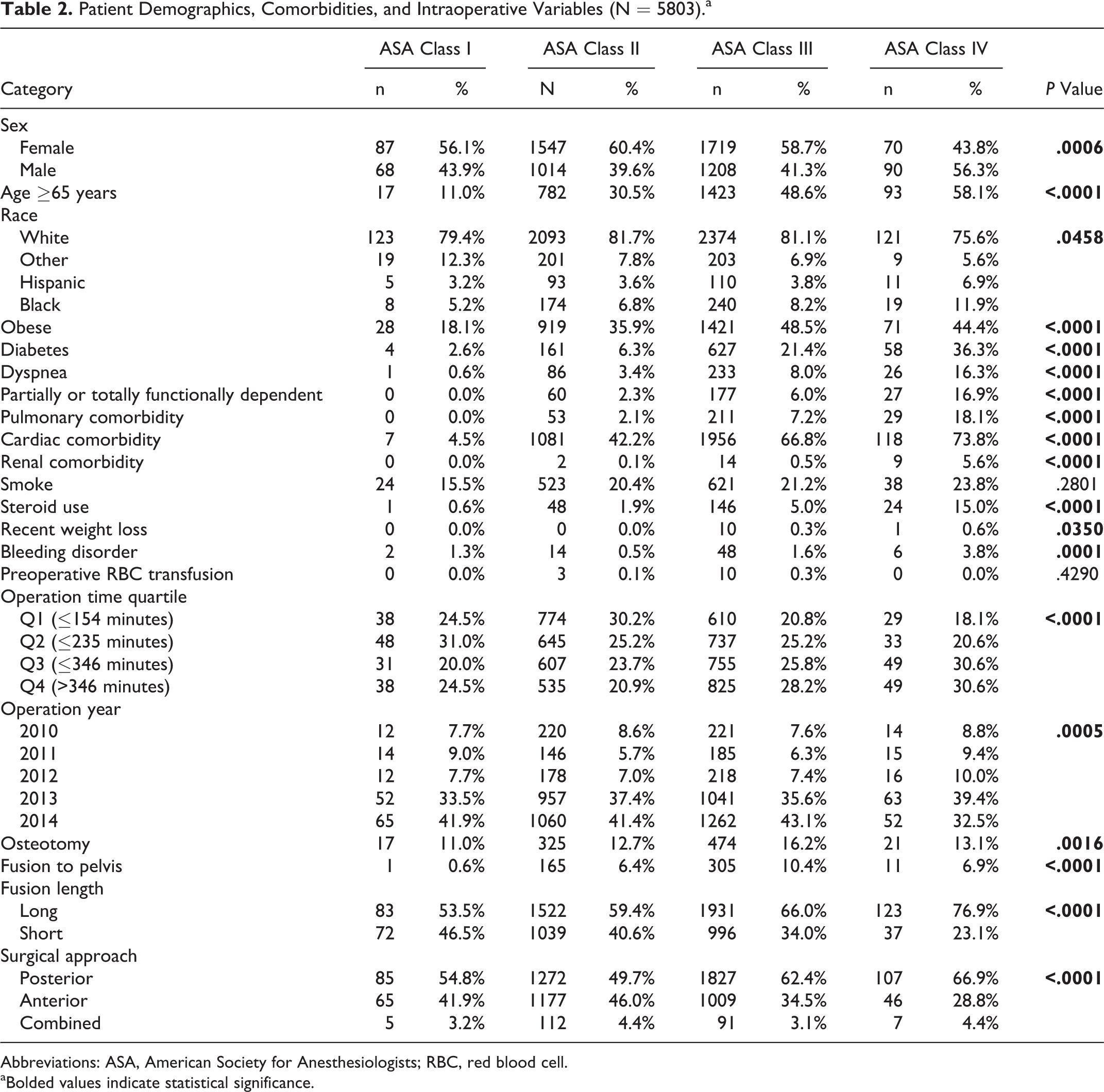
Abbreviations: ASA, American Society for Anesthesiologists; RBC, red blood cell.
aBolded values indicate statistical significance.
Unadjusted Analysis
There were statistically significant differences in 30-day unadjusted morbidities and mortality between the 4 ASA cohorts (Table 3). Patients in the ASA IV cohort, compared to the ASA I cohort, experienced a higher rate of mortality (3.8% vs 0.0%), any complication (51.9% vs 17.4%), LOS ≥5 days (55.0% vs 20.6%), wound complication (4.4% vs 0.6%, P = .0005), pulmonary complication (11.9% vs 0.6%), UTI (3.1% vs 0.6%, P = .0095), cardiac complication (4.4% vs 0.0%), intra-/postoperative RBC transfusion (41.3% vs 15.5%), sepsis (6.3% vs 0.0%), reoperation (9.6% vs 0.7%), and unplanned readmission (12.3% vs 3.5%). All P values are <.0001 unless otherwise stated.
Unadjusted Outcomes (N = 5803).a
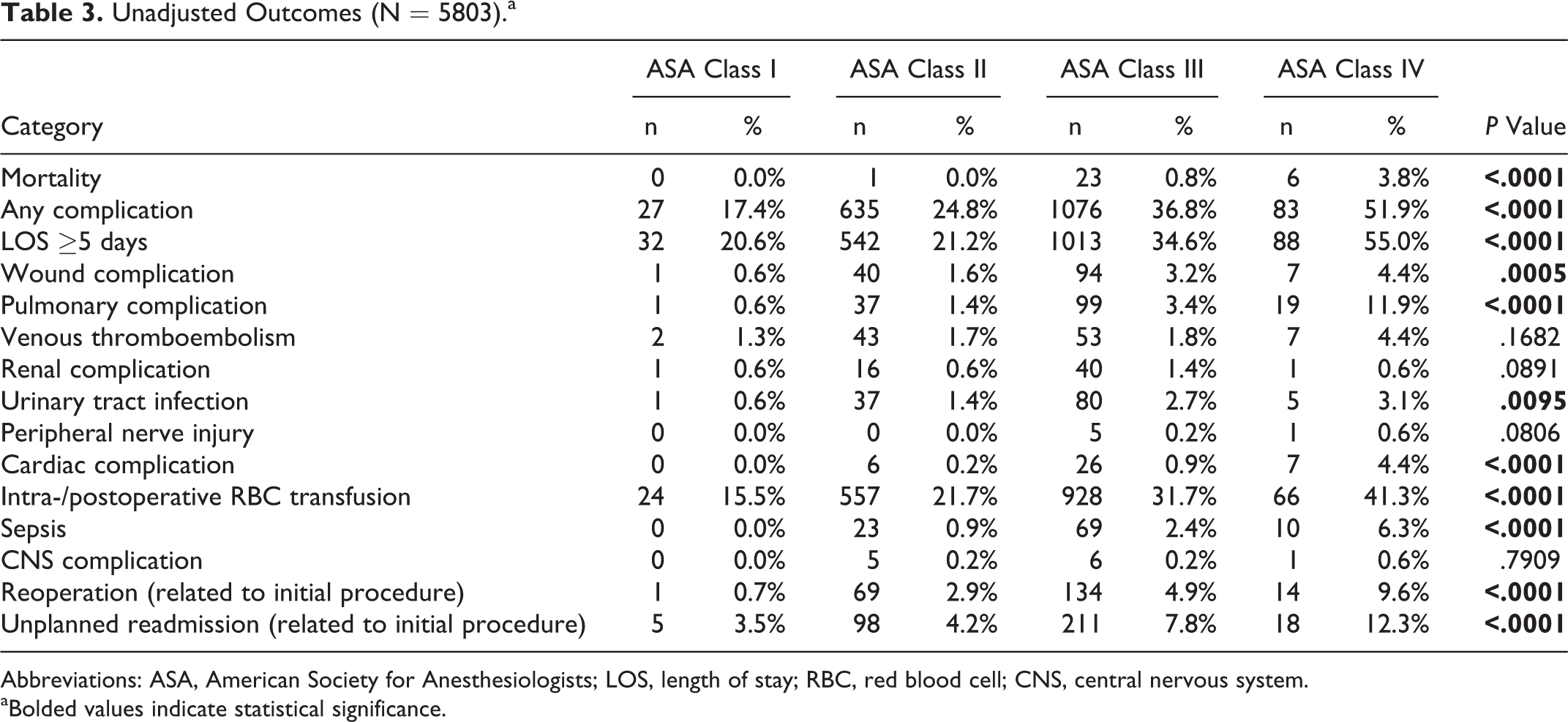
Abbreviations: ASA, American Society for Anesthesiologists; LOS, length of stay; RBC, red blood cell; CNS, central nervous system.
aBolded values indicate statistical significance.
Subgroup Analysis Between ASA Class II and III
A bivariate subgroup analysis was performed between ASA class II and ASA class III (Table 4). Patients in the ASA class III cohort were more likely to be ≥65 years of age, obese, diabetic, dyspneic, partially or totally functionally dependent, pulmonary comorbid, cardiac comorbid, renal comorbid, use steroids, have recent weight loss, bleeding disorder, operation time ≥4 hours, osteotomy, fusion to pelvis, longer fusion lengths, and posterior surgical approaches.
Subgroup Bivariate Analysis Between ASA II and ASA III Patients for Patient Characteristics (N = 5488).a
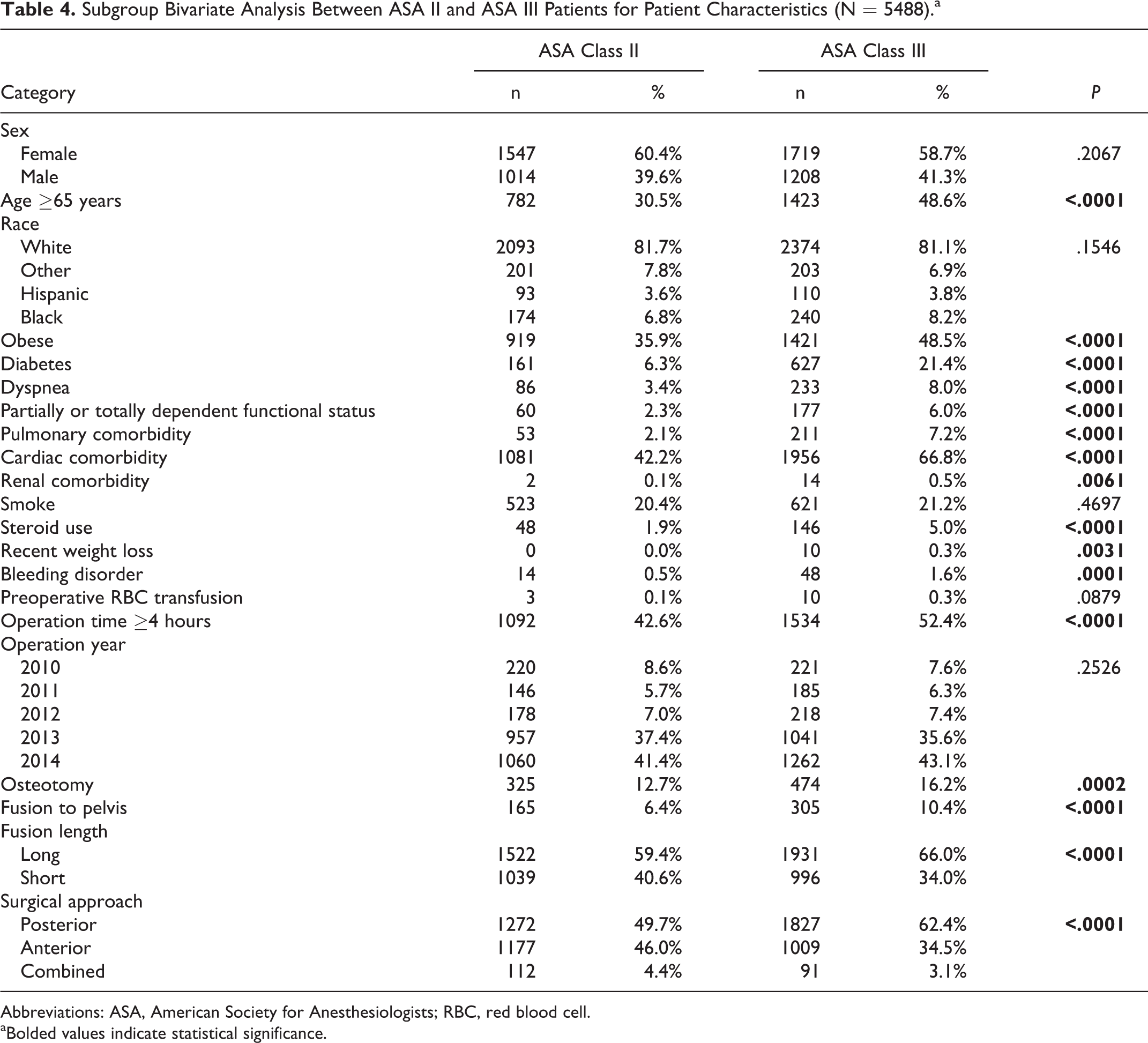
Abbreviations: ASA, American Society for Anesthesiologists; RBC, red blood cell.
aBolded values indicate statistical significance.
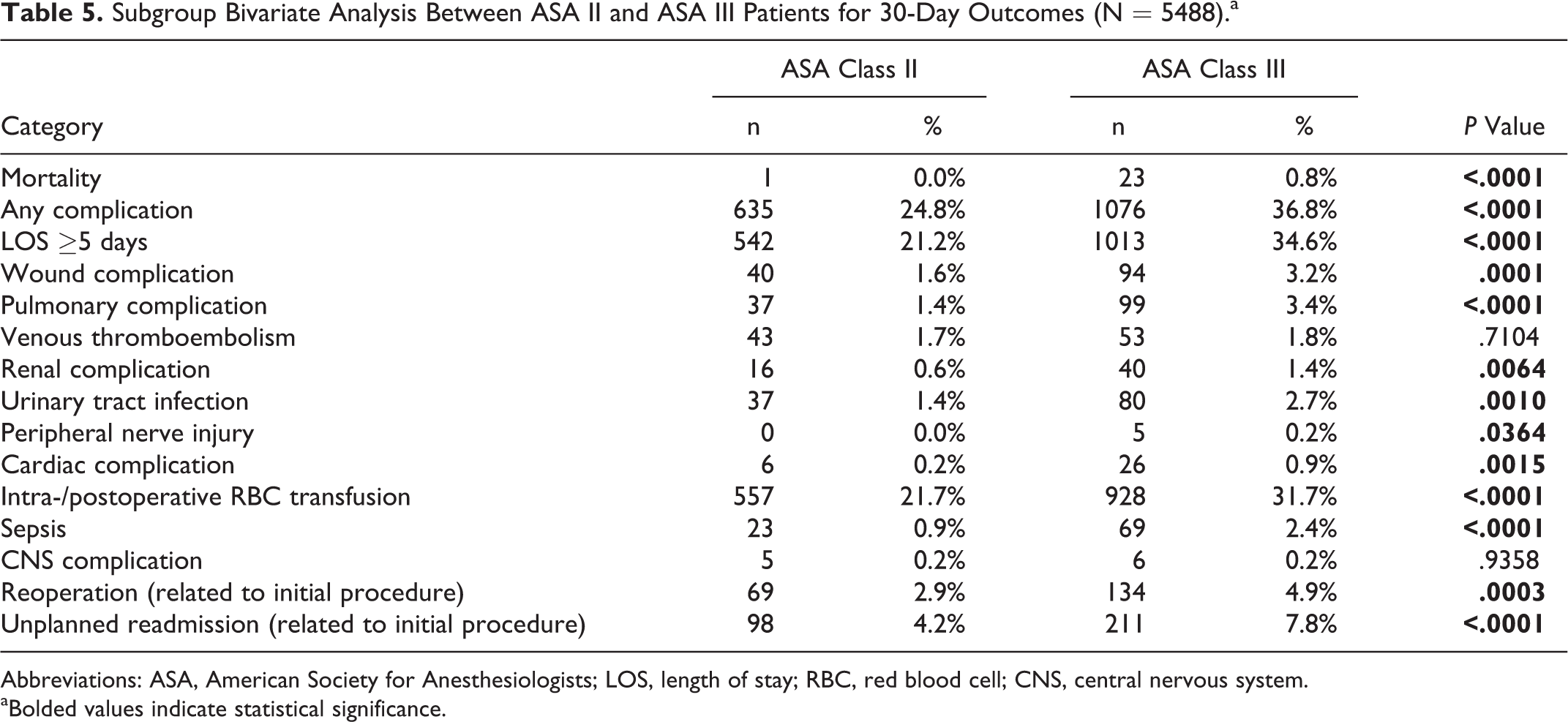
There were statistically significant differences in 30-day unadjusted morbidities and mortality between the ASA II and ASA III cohorts (Table 5). ASA III patients experienced a higher rate of mortality (0.8% vs 0.0%), any complication (36.8% vs 24.8%), LOS ≥5 days (34.6% vs 21.2%), wound complication (3.2% vs 1.6%, P = .0001), pulmonary complication (3.4% vs 1.6%), renal complication (1.4% vs 0.6%), UTI (2.7% vs 1.4%, P = .0010), peripheral nerve injury (0.2% vs 0.0%, P = .0364), cardiac complication (0.9% vs 0.2%, P = .0015), intra-/postoperative RBC transfusion (31.7% vs 21.7%), sepsis (2.4% vs 0.9%), reoperation (4.9% vs 2.9%, P = .0003), and unplanned readmission (7.8% vs 4.2%). All P are <.0001 unless otherwise stated.
Subgroup Bivariate Analysis Between ASA II and ASA III Patients for 30-Day Outcomes (N = 5488).a
Abbreviations: ASA, American Society for Anesthesiologists; LOS, length of stay; RBC, red blood cell; CNS, central nervous system.
aBolded values indicate statistical significance.
Multivariate Analysis
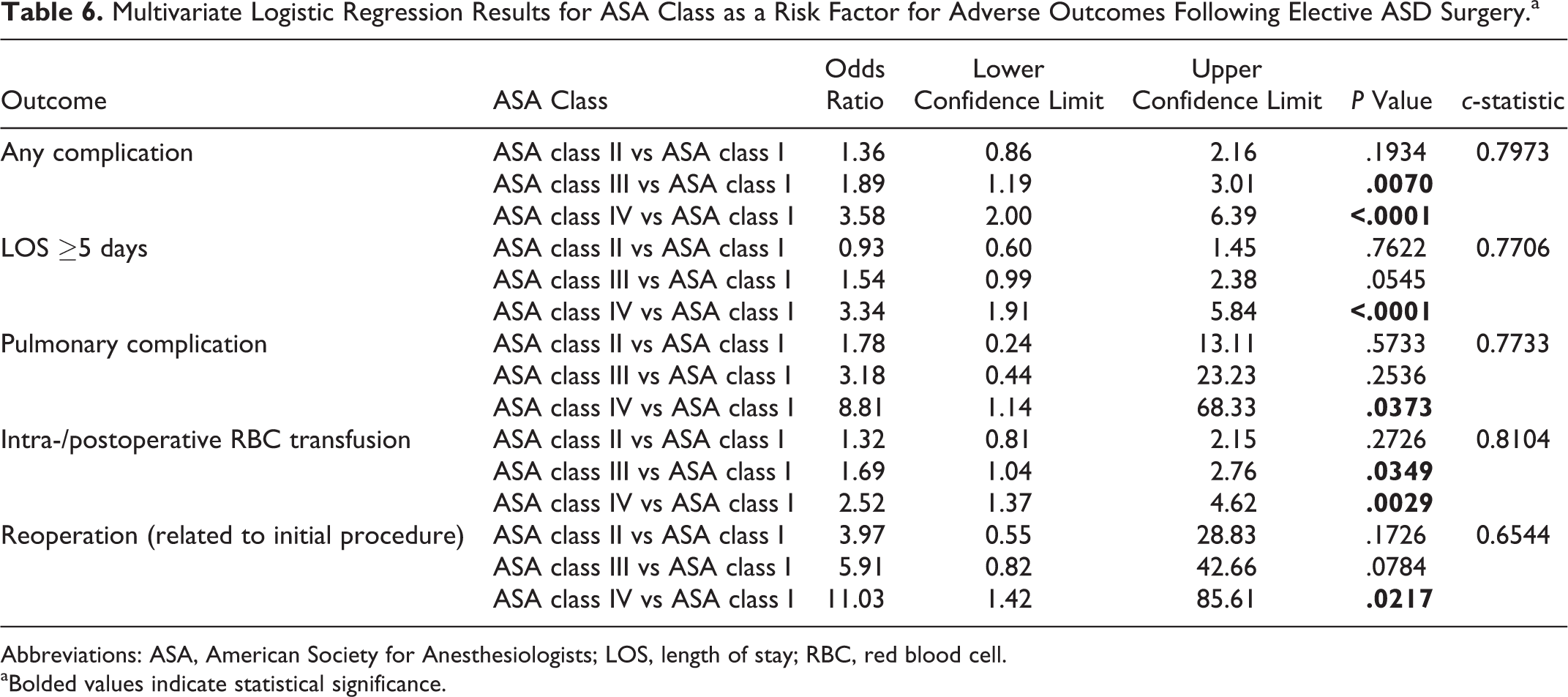
Multivariate logistic regression analysis (Table 6) revealed ASA classes II, III, and IV, compared to ASA class I, to be a significant, independent risk factor for several acute complications. Patients experienced an increased risk of any complication (ASA class III: odds ratio [OR] = 1.89, confidence interval [CI] = 1.19-3.01, P = .0070; ASA class IV: OR = 3.58, CI = 2.00-6.39; c-statistic = 0.7973), LOS ≥5 days (ASA class IV: OR = 3.34, CI = 1.91-5.84; c-statistic = 0.7706), pulmonary complication (ASA class IV: OR = 8.81, CI = 1.14-68.33, P = .0373; c-statistic = 0.7733), intra-/postoperative RBC transfusion (ASA class III: OR = 1.69, CI = 1.04-2.76, P = .0349; ASA class IV: OR = 2.52, CI = 1.37-4.62, P = .0029; c-statistic = 0.8104), and reoperation (ASA class IV: OR = 11.03, CI = 1.42-85.61, P = .0217; c-statistic = 0.6544). P values are <.0001 unless otherwise stated.
Multivariate Logistic Regression Results for ASA Class as a Risk Factor for Adverse Outcomes Following Elective ASD Surgery.a
Abbreviations: ASA, American Society for Anesthesiologists; LOS, length of stay; RBC, red blood cell.
aBolded values indicate statistical significance.
Discussion
This study explored the role of patient ASA class assignment in improving risk stratification for patients undergoing elective ASD surgery. Higher ASA class assignment was found to be significantly and independently associated with the many acute postoperative outcomes such as any complication, LOS ≥5 days, pulmonary complications, intra-/postoperative RBC transfusion, and reoperation (related to initial procedure).
The bivariate analysis (Table 2) in this study was most useful in illustrating the differences in characteristics of patients between the low and high ASA class cohorts. In patient demographics, old age had a significant correlation with higher ASA. Although ASA class assignment is not dependent on this variable, it may instead function as a confounder. Stratification by age revealed that the incidence of pulmonary and cardiac comorbidities, two leading drivers of higher ASA class assignment, increased with older age in this study’s patient population. This may explain the difference seen in age between these ASA class cohorts.
Bivariate analysis also revealed that patients with a higher comorbidity burden was correlated with higher ASA scores. Since ASA class is dependent on physical status, which is dependent on patient preoperative health, this observed result agrees with ASA class assignment guidelines, as well as other previous literature in spinal surgeries. 6 –13 Interestingly, the prevalence of smoking in the higher ASA class cohort was not significantly different than that of the lower ASA class. ASA guidelines register current smokers automatically into ASA class II, but there is no concrete information on how the degree of smoking, aside from conferred illnesses that more relate to a patient’s current disease states, plays a role in ASA class assignment. Because NSQIP registers patient smoking as binary and fails to capture the degree of smoking, these 2 factors may have led to this result.
Most important, on multivariate analysis, increasing ASA class was identified as an independent risk factor for many postoperative complications. Pateder et al echoed these results in their study, which identified the bivariate association between ASA class and mortality. 17 Smith et al conducted a prospective, multicenter, 2-year follow-up of patients following ASD surgery and found that higher, perioperative (<6 weeks from operation) complication rates (ie, overall morbidity) are associated with patients who have greater preoperative comorbidities. 18 Mannion et al used the Eurospine Spine Tango Registry to create a cohort of patients undergoing spine surgery for degenerative lumbar disorders and found ASA class to be an independent risk factor of surgical and general complication incidence in patients undergoing any spine surgery. 19 Preoperative patient comorbidities have been shown to increase complication rates in spinal surgery. 18,19 Similarly, ASA class is an effective surrogate for patient preoperative comorbidities, and therefore, advanced ASA class acts as a risk factor for postoperative adverse events. This is in line with other studies that have shown ASA class to correlate with and increased incidence of postoperative complications following spine surgery. 6,7,9,12,20
All of the postoperative adverse events where ASA class was identified as a risk factor generally had modest c-statistic values (Table 6). For example, in other spinal surgeries, ASA class has been implicated as a risk factor for wound complications. 10,13 This may be justified by the fact that ASA class encapsulates diabetes and obesity, both of which have been associated with a greater risk of surgical site infections as a result of tissue hypoperfusion and subsequently impaired immunological function. 21 Finally, ASA class is a proxy for patients’ preoperative health and encapsulates multiple comorbidities that are known to be risk factors for cardiac complications, 22 pulmonary complications, 23 postoperative sepsis, 22,24 UTI, 24 and intra-/postoperative transfusion. 25 A greater incidence of these complications can lead to prolonged length of hospital stay.
The key findings from this study were different than the conclusions from Schwab et al, 14 which may have stemmed from differences in study design. Schwab et al divided their patient population into a complication cohort and control cohort. The complication cohort was collected by a nonrandom, retrospective consecutive sampling method, and the control cohort was randomly selected from a time-matched sample. The advantage of using this method, as Schwab et al did, is that the optimization algorithm for multivariate logistic regression will be less likely to generate a model with low sensitivity and specificity (ie, low c-statistic). However, this study ensures that this advantage is mirrored by taking into account c-indices when looking at multivariate regression model accuracies. The differences between this study and Schwab’s, then, stem from the different sampling procedures used. Given that nonrandom sampling has a greater risk of creating a sample that may not be the best representation of the true population, 26 NSQIP, given its much larger data size, is more likely to represent this true ASD population, helping bolster the reliability of outcomes in this study.
However, there are several limitations that must be addressed in this work. Because the NSQIP database classifies cases based on CPT codes, differences between procedural techniques cannot be accounted for in this study. The NSQIP database does not delineate patients by ICD-9 codes, which presents an inherent limitation of the database. We attempted to control for variables that we considered surrogates for case complexity such as operative duration, presence or absence of an osteotomy, pelvic fixation, surgical approach, long fusion lengths, and total relative value units in our multivariate regression analysis. Furthermore, NSQIP offers a large patient size but may overrepresent academic US medical centers. Additionally, long-term complications, radiological outcomes, and other spine-specific variables are not captured in the NSQIP database, which only evaluates complications up to 30 days postoperatively, leading to a potential underestimation of risk. Finally, interrater reliability of ASA class are not perfect, even though ASA class assignment has been known to achieve 98% reliability (±1 class) across different anesthesiologists. 27
Despite these limitations, this is the first study evaluating the role of ASA class in ASD surgery with a large patient database. ASA class can intuitively be appreciated as a tool in patient risk stratification since it inherently captures a large spectrum of patient comorbidities. In this study, this notion was verified, with higher ASA class assignments showing significant and independent correlation with any complications, LOS ≥5 days, pulmonary complications, intra-/postoperative RBC transfusions, and reoperation. These results suggest the utility of ASA class in refining the risk stratification profile and improving preoperative patient counseling for those individuals undergoing ASD surgery.
Footnotes
Authors’ Note
This study was qualified as exempt by the Mount Sinai Hospital Institutional Review Board. This study was previously presented as a “Podium Presentation” at the Lumbar Spine Research Society 2016 Annual Meeting on April 14, 2016, in Chicago, Illinois.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Cho reports personal fees from Stryker and nonfinancial support from Zimmer, outside the submitted work. The remaining authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.