
Abstract
Study Design:
Retrospective radiographic study.
Objective:
The optimal radiographic modality for assessing cervical foraminal stenosis is unclear. Determination on conventional axial cuts is made difficult due in part to the complex, oblique orientation of the cervical neuroforamen. The utility of 3-dimensonal (3D) computed tomography (CT) reconstruction in improving neuroforaminal assessment is not well understood. The objective of this study is to determine inter-rater variability in grading cervical foraminal stenosis using 3 different CT imaging modalities: 3D CT surface reconstructions (3DSR), 2D sagittal oblique multiplanar reformations (2D-SOMPR), and conventional 2D axial CT imaging.
Methods:
Pretreatment CT scans of 25 patients undergoing surgery for cervical spondylotic radiculopathy were analyzed at 2 levels: C5-C6 and C6-C7. Simple interrater agreement and kappa-Fleiss coefficients were calculated for each imaging modality and stenosis grade. Image reviewers (attending spine surgeon, attending neuroradiologist, spine fellow) interpreted each CT scan in 3 different formats: axial, 2D-SOMPR, and 3DSR. Four cervical foramina at 2 spinal levels were graded as normal (no stenosis), mild (≤25% stenosis), moderate (25%-50% stenosis), or severe (>50% stenosis).
Results:
Across all imaging modalities, interrater reliability was fair when grading foraminal stenosis (κ < 0.4). Agreement was lowest for the axial images (κ = 0.119) and highest for the 3D CT reconstructions (κ = 0.334). 2D-SOMPR images also led to improved interrater reliability when compared with axial images (κ = 0.255).
Conclusion:
Grading cervical foraminal stenosis using conventional axial CT imaging is difficult with low interrater reliability. CT modalities that provide a circumferential view of the cervical foramen, such as 2D-SOMPR and 3D CT reconstruction, had higher rates of interobserver reliability in grading foraminal stenosis than conventional axial cuts, with 3D having the highest. As these 3D reconstructions can be obtained at no additional cost or radiation exposure over a conventional CT scan, and because they can provide useful information in determining levels being considered for surgical decompression, we recommend they be utilized when evaluating cervical foramina.
Introduction
Cervical radiculopathy is relatively common and affects an estimated 83 per 100 000 Americans each year. 1 In cases of refractory pain or neurologic involvement, cervical radiculopathy is treated surgically. However, a sine qua non of successful operative care is the proper identification of the causative root level(s). Unfortunately, the classic triad of history, physical examination, and imaging (including X-rays, magnetic resonance imaged [MRIs], and computed tomography [CT] scans) may not allow for definitive, confident identification of the causative level(s) in many cases.
Accurate assessment of foraminal stenosis with commonly used imaging modalities in the axial and sagittal plane may be imperfect for 3 primary reasons. First, the cervical foramina are obliquely oriented relative to the sagittal plane, thus preventing consistent assessment of foraminal diameter between multiple imaging reviewers using standard axial 2-dimensional (2D) imaging analysis. 2,3 Second, the current “gold standard” for diagnosis of foraminal stenosis is MRI, but images are typically obtained only in the axial and sagittal plane, rather than in the oblique sagittal plane of the neuroforamina. Third, there are no universally accepted criteria to define foraminal stenosis radiographically. Strict numerical cutoffs increase the number of false-positive readings, because asymptomatic individuals frequently exhibit foraminal diameter narrowing in at least one 2D plane along the oblique axis. 4,5 For this reason, clinicians typically assign the diagnosis of foraminal stenosis based on their clinical experience in recognizing normal anatomic variation on spinal imaging.
CT imaging data is frequently interpreted by clinicians with the help of various postacquisition imaging analysis protocols. Most common are 2D slices of anatomic interest in any of the cardinal anatomical planes: coronal, sagittal, and axial. New protocols have allowed for postacquisition generation of 3D surface reconstructions, which provide virtual 3D anatomic structures. Studies utilizing 3D reconstruction of 2D CT imaging data are promising, and the utility of this imaging technology has been demonstrated in the diagnosis of rotational and shear vertebral fractures, 6 assessment of congenitally abnormal pedicles, 7 and also establishment of safe entry points for pedicle screws in corrective scoliosis surgeries. 8
However, there are currently no studies evaluating the utility of 3D CT reconstruction in assessing cervical neuroforaminal stenosis. The purpose of this study was to determine the utility of 3D surface reconstructed (3DSR) CT scans in assessing cervical foraminal stenosis, by comparing the reliability of this modality versus 2D sagittal oblique multiplanar reformations (2D-SOMPR) and conventional 2D axial CT imaging.
Populations and Methods
Patient and Reviewer Populations
Twenty-five consecutive patients who underwent anterior cervical discectomy and fusion (ACDF) at C5-6 and/ or C6-7 for the treatment of cervical spondylotic radiculopathy from January 1, 2010 to December 31, 2013, and who had preoperative CT scans of adequate quality, were chosen for this study. Patients having surgery for soft disc herniation were excluded in order to focus on those having bony foraminal narrowing. Patients were identified through a review of the electronic medical record. Exclusion criteria included a past medical history of trauma to the cervical spine, malignancy, congenital cervical spine anomalies, and known rheumatic disease.
Image reviewers included a graduating fellow in orthopedic spine surgery, an attending neuroradiologist, and a practicing fellowship-trained attending orthopedic spine surgeon. The institutional review board approved this study design and a waiver of consent was obtained. Once the eligible cervical spine studies were identified, the identifying information was removed and the data from the images was logged in a completely deidentified database. Reviewers were blinded to all patient identifiers, medical histories, and patient inclusion criteria for this study.
Methods
Study candidates were identified using the SurgiNet EMR application, and imaging files were acquired using GE PACS software. Twenty-five pretreatment CT scans were converted to the DICOM (digital imaging and communications in medicine) file format and downloaded to local computer hard disk for processing using OsiriX workstation software version 4.1.2. DICOM files were formatted to three separate imaging modalities: 2D axial slices, 2D Sagittal Oblique MPR (2D-SOMPR) slices, and 3D surface reformation (3DSR).
For each 2D axial CT study, all slices containing imaging data for C5-C7 were compiled into a Microsoft Powerpoint presentation, which allowed users to scroll through the deidentified images in a manner similar to the conventional imaging workstation. A representative 2D-SOMPR imaging window is depicted in Figure 1. Quicktime desktop capture video software was used to record scrolling through these images along the longitudinal axis of the C5-C7 neuroforamina (red arrows), as highlighted with the orange line. An exemplary 3DSR image with a spatial orientation key is shown in Figure 2. In a similar fashion, desktop capture video software was used to record complete manipulation of the surface models in all angles and orientations centered around the longitudinal axis of the neuroforamina. When viewing these movies, users could simulate toggling through the original imaging modalities in the native OsiriX software by adjusting the navigation bar as seen in Figure 2. A representative spinal segment is illustrated in each imaging modality in Figure 3 along with the corresponding user agreement.
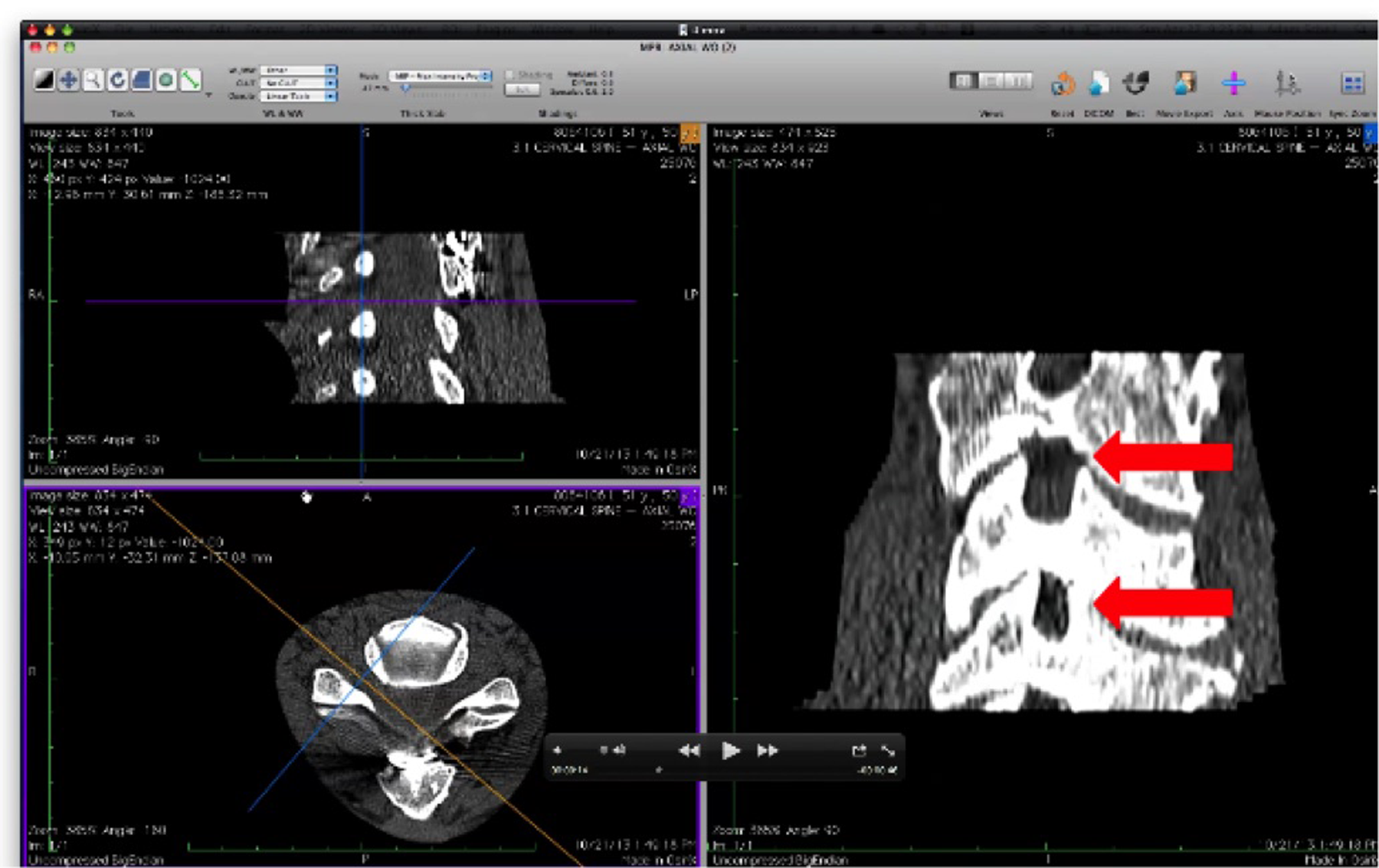
Two-dimensional sagittal oblique multiplanar reformations (2D-SOMPR) viewing window. Bottom left window: axial orientation of the sagittal oblique slices, which are taken perpendicular to the longitudinal axis represented by the orange line in that window. The blue line is coplanar to each sagittal oblique slice. Right: A representative sagittal oblique slice taken along the longitudinal axis of the neuroforamen. The red arrows indicate the location of the left C5-C6 (upper) and left C6-C7 (lower) neuroforamen.
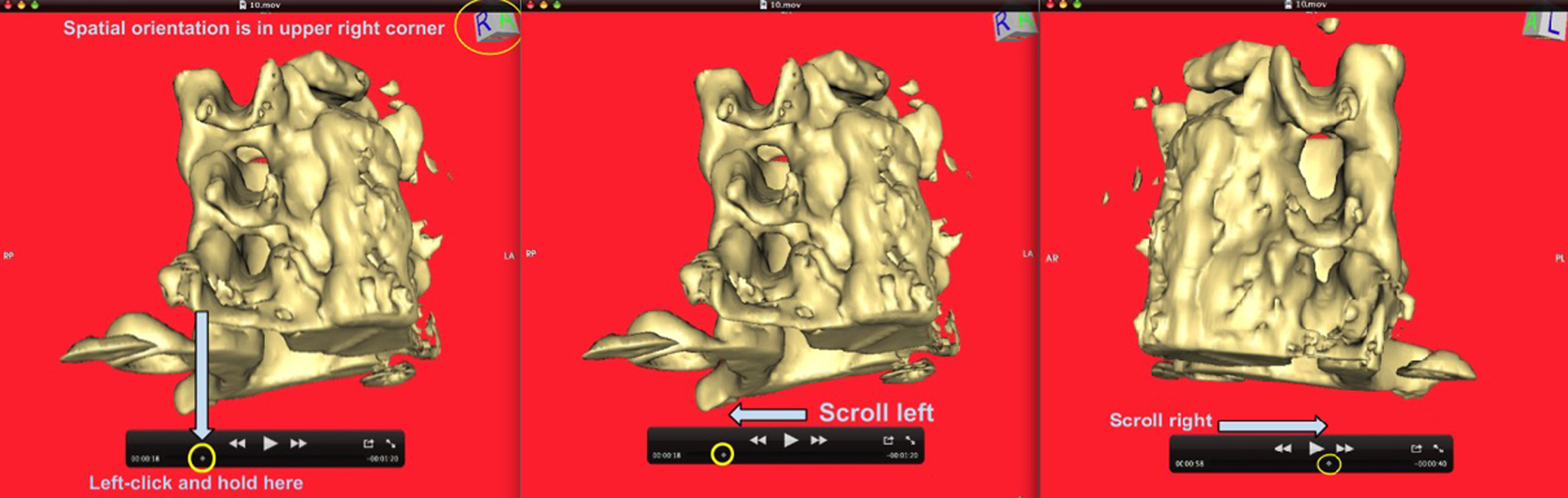
Three-dimensional surface reconstruction (3DSR) of a C5-C7 vertebral segment. Reviewers use the spatial orientation cube (top left, large yellow circle) and the navigation bar to toggle directionality of 3DSR and view each foramen down its longitudinal axis.
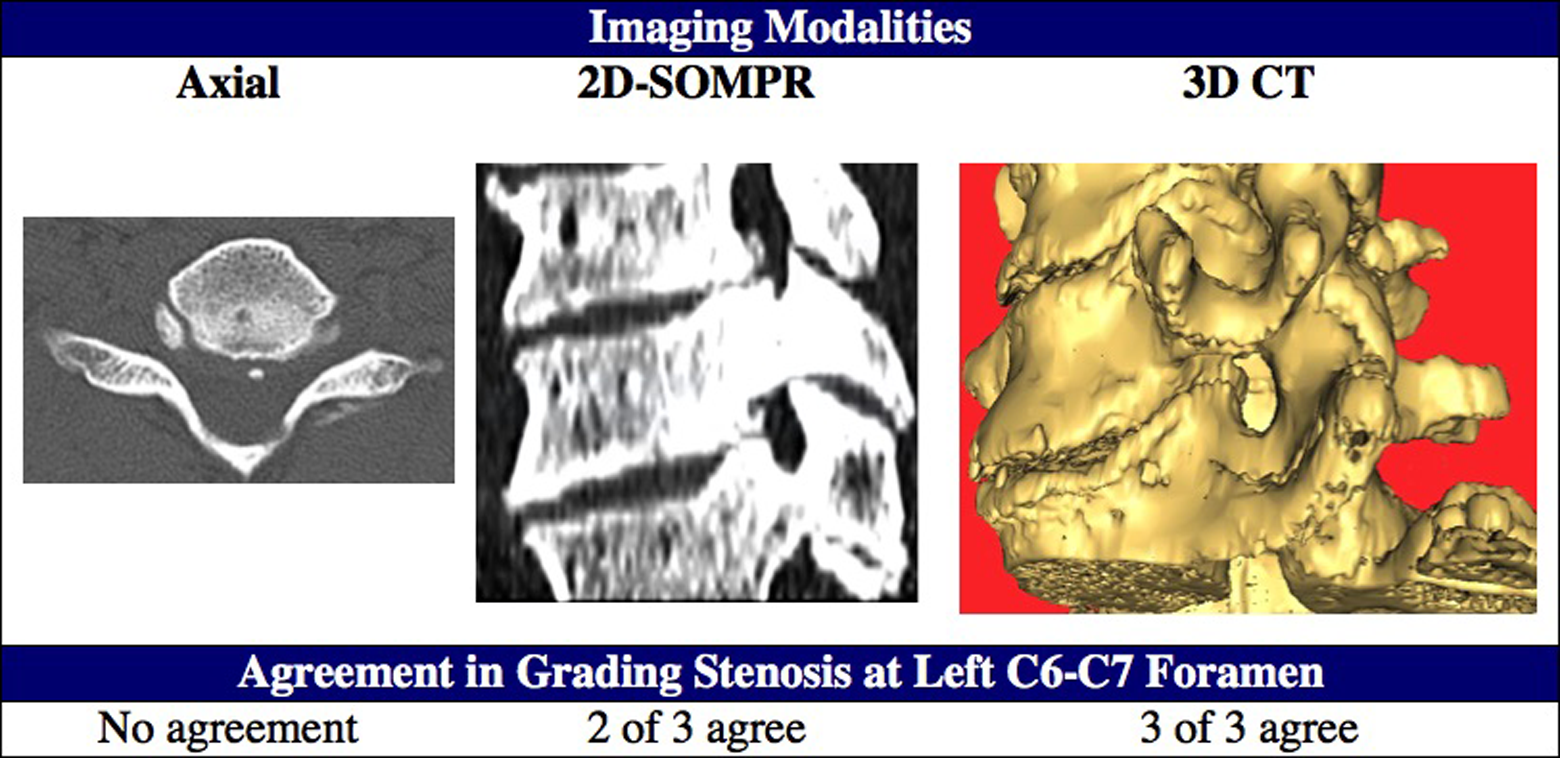
Images of a representative spinal segment using each of 3 modalities. The left neuroforamen elicited 3 different levels of agreement and demonstrated improved consensus when 3-dimensional computed tomography (3D CT) surface reconstructions were utilized.
The Emory University Institutional Review Board approved this study. Reviewers were blinded to all patient identifiers, medical histories, and patient inclusion criteria for this study. All imaging files were completely de-identified and stored on a remote drive, where each imaging reviewer could access at his leisure. The four cervical foramina at the specified vertebral levels were then graded by each reviewer according to the following subjective scale: normal (no stenosis), mild (≤25% stenosis), moderate (25%-50% stenosis), or severe (>50% stenosis). Reviewers also indicated whether surgical decompression should be considered at each foramen assuming the subject was experiencing radiculopathic symptoms on that side.
Statistics
Simple percentage agreements in the aforementioned categories were determined for each imaging modality. The kappa-Fleiss coefficient and standard error was then determined for each imaging modality overall and subsequently stratified according to assigned foraminal stenosis grade. Kappa-Fleiss coefficients and standard errors were also calculated to compare reviewers’ surgical decisions. The Landis-Koch score was used to interpret kappa-Fleiss coefficients in the following manner: no agreement (<0), slight (0.01-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and excellent (0.81-1.00). 9 Chi-square analysis was used to analyze absolute agreement using the likelihood ratio test. Contingency plots were also generated for comparing absolute agreements.
Sample size was determined using the method of Sim et al. 10 We anticipated a kappa coefficient of approximately 0.4 based on similar studies in the literature. 11 With a significance α = .05 and an expected power of (1 − β) = 0.9, a sample size requirement of at least n = 66 neuroforamina was identified using a 2-tailed distribution calculation. Therefore, 100 neuroforamina (4 neuroforamina in 25 patients) were evaluated. All statistical analysis was performed using JMP SAS pro statistical software (version 10.0.0; SAS Institute, Cary, NC), with statistical significance defined as P < .05.
Results
Of the 25 patients included in the study, there were 17 females (68%) and 8 males (32%), ages 41 to 75 years (mean 56.6 years). A total of 75 unique CT imaging files depicting a total of 100 neuroforamina were analyzed by each reviewer. When all 3 imaging modalities were compared, the mean absolute inter-method agreement was 25.6% (18%-34%) indicating low absolute agreement among reviewers (Table 1). Both 2D-SOMPR and 3DSR enabled increased absolute agreement when compared with 2D axial images (34% and 25% vs 18%, respectively). Chi-square analysis of absolute agreement between methods revealed a statistically significant increase when 3DSR images were analyzed (df = 4, χ2 = 9.67, P = .046), and a contingency table illustrating differences in absolute agreement across imaging modalities is depicted in Figure 4.
Summary of Absolute Agreement and Kappa Coefficients When All 3 Reviewers Were Compared for Each Imaging Modality.a
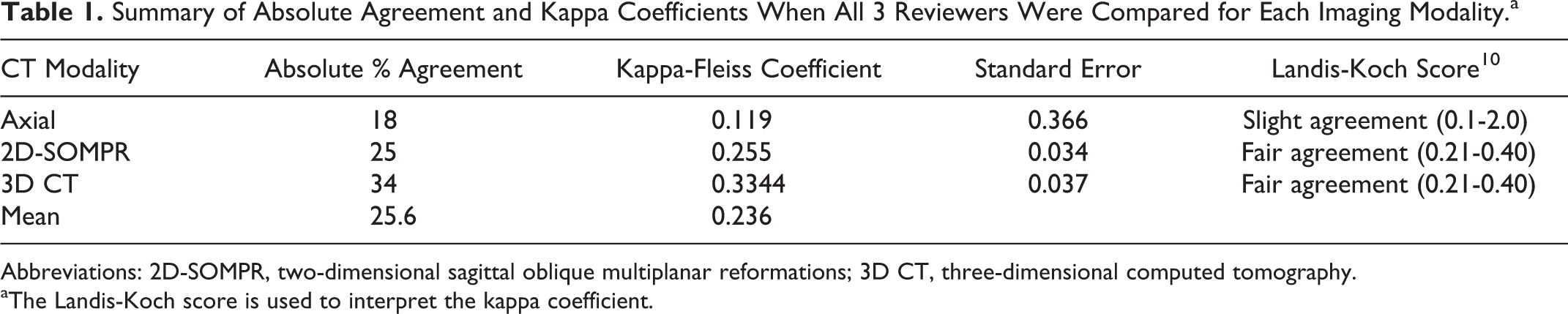
Abbreviations: 2D-SOMPR, two-dimensional sagittal oblique multiplanar reformations; 3D CT, three-dimensional computed tomography.
aThe Landis-Koch score is used to interpret the kappa coefficient.
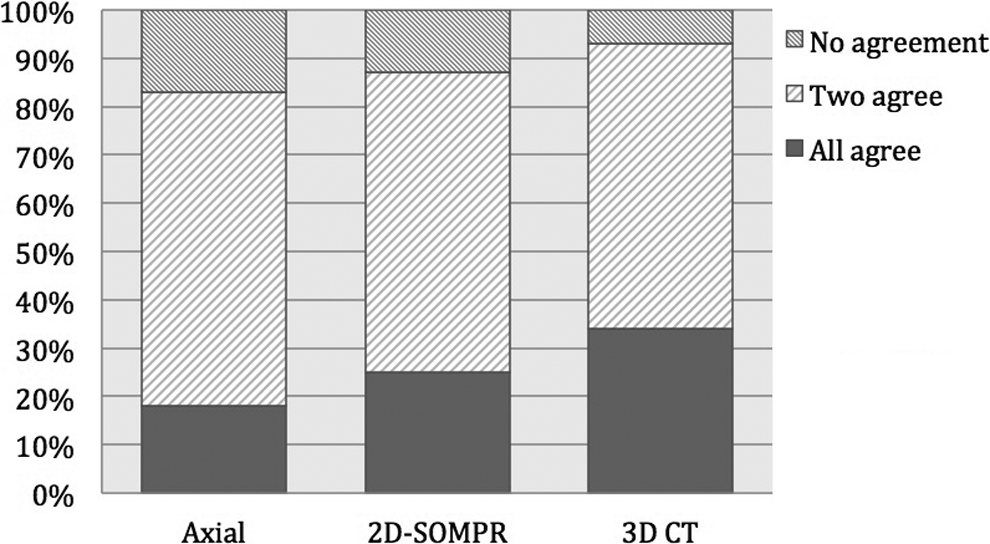
Contingency plot stratified by imaging modality and depicting the frequency of each possible agreement scenario in the assignment of foraminal stenosis grades: no users agree, 2 users agree, or all users agree. The frequency of 2 or more users agreeing was highest when 3-dimensional computed tomography (3D CT) reconstruction was utilized (χ2 = 9.67, P = .0464).
According to the Landis-Koch score, interrater reliability was “fair” when grading foraminal stenosis across all imaging modalities (κ < 0.4). Overall agreement was “slight” when 2D axial images were read (κ = 0.119) and “fair” when 2D-SOMPR (κ = 0.255) and 3DSR (κ = 0.334) images were reviewed (Table 1). Moreover, agreement was lowest in the axial images (κ = 0.119) and highest in the 3D CT reconstructions (κ = 0.334). Sagittal oblique MPR images also led to improved interrater reliability when compared with axial images (κ = 0.255). When interuser agreement was stratified according to assigned foraminal stenosis grade, 3DSR images provided the highest agreement for both “mild” and “moderate” stenosis (Figure 5). Both 3DSR and 2D-SOMPR provided improved agreement in these categories when compared with 2D axial images. Across all imaging modalities, agreement was highest when assigning “normal” stenosis grades, and 2D-SOMPR enabled the maximum agreement in this category (κ = 0.582). Agreement in the assignment of “severe” stenosis was notably higher when 3DSR images were used (κ = 0.326) in comparison with 2D-SOMPR (κ = 0.228) and 2D axial images (κ = 0.1852).
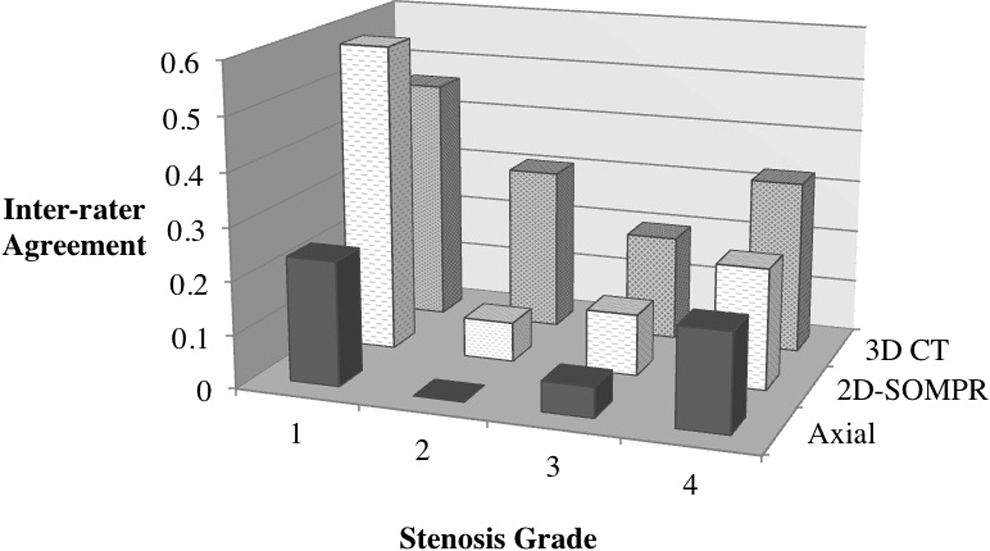
Interrater agreement was evaluated using the kappa value for each imaging modality and stratified according to the assigned stenosis grade.
The spine fellow and the attending spine surgeon were asked to evaluate the need for surgical decompression at each neuroforamen, under the assumption that the patient was experiencing radiculopathic symptoms on that side. Notably, interrater agreement was “slight” when 2D axial images were used (κ = 0.064; Figure 6). Agreement was considered “moderate” when either 3DSR or 2D-SOMPR was used. Moreover, there was enhanced agreement when either 3DSR or 2D-SOMPR were compared with 2D axial images.
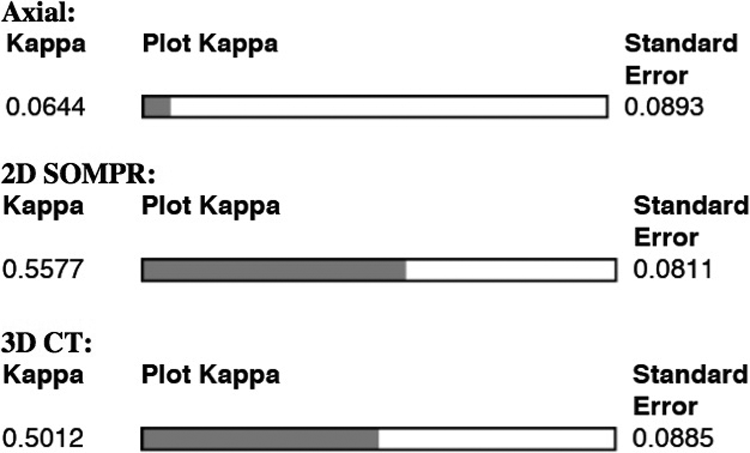
Interrater agreement in whether or not to recommend surgery was evaluated using the kappa value for each imaging modality. Only the surgeons are compared in this analysis.
Discussion
In the present study, we evaluated the utility of 3DSR CT scans in the assessment of cervical foraminal stenosis by comparing interrater reliability with other established CT modalities. When evaluating cervical foraminal stenosis, 3DSR had the highest inter-rater agreement, 2D-SOMPR had the second highest, and 2D axial images had the lowest. Interrater agreement on the need for surgical decompression was also greater with 3DSR and 2D-SOMPR than with axial cuts. Therefore, we conclude that the addition of 3DSR images is beneficial in the CT assessment of cervical foraminal stenosis for patients undergoing surgical decompression.
Imaging of the cervical spine plays an important role in the evaluation of patients with radiculopathic pain in the upper extremities. Although MRI remains the gold standard for evaluating pathology in this anatomic region, 3 MRI has its limitations. Chief among these limitations is slice width, which can limit the resolution with which MRI may define the small cervical neuroforamina. In addition, MRI artifact has been shown to distort small bony anatomy by overestimating bony contributions to foraminal stenosis. 4 Although they can be, MRI scans are also not routinely obtained in the oblique sagittal plane of the neuroforamina in most radiology departments. Furthermore, they cannot readily be reformatted in such a plane postacquisition, unlike CT scans. Finally, the presence of metallic hardware in patients who had undergone prior spinal surgeries may lead to distortion artifacts, rendering MRI images of patients in this population difficult to interpret.
Three-dimensional CT reformation is an imaging tool that has recently been validated in a variety of applications to the practice of spine surgery. This form of postacquisitional CT image processing has been demonstrated to reduce interuser variability in the diagnosis of rotational and shear vertebral fractures, 6 assessment of congenitally abnormal pedicles, 7 and also establishment of safe entry points for pedicle screws in corrective scoliosis surgeries. 8 This study represents the first application of 3DSR to assessing foraminal stenosis in patients presenting with cervical radiculopathy. The modern radiology “workstation,” which is the software suite used to process imaging data in routine clinical practice, provides spine practitioners with a wide array of postacquisition imaging tools to enhance their interpretation of routine radiology studies. Generating 3DSRs is fast, easy, and requires no additional medical costs or radiation to the patient in cases where a CT has already been obtained. Methodologies that improve image interpretation are of great value to spine surgeons, who must often make decisions regarding operative levels in the face of clinical symptoms that do not match a “textbook” pattern.
The primary outcome of interest in this study was interrater reliability in the assessment of cervical foraminal stenosis. Interpreting cervical spine images in this manner is a difficult task, and the low absolute agreement demonstrated in this study confirms this fact. However, the data presented in this study demonstrates an advantage to using 3DSR, because interrater reliability was maximized relative to the other 2 imaging modalities examined. While users tended to agree more frequently overall when 3DSR was used, 3DSR had greatest agreement when evaluating “mildly” to “moderately” stenosed foramina. This finding potentially suggests greater value to 3DSR in evaluating subtler degrees of stenosis, where decision making is even more difficult than when evaluating the obvious, “severe” case.
While this novel application of 3DSR to diagnosing foraminal stenosis appears to be a useful clinical tool, this data also demonstrates the utility of 2D-SOMPR. Both 3DSR and 2D-SOMPR notably enhanced interrater reliability when compared with 2D axial imaging. The obliquely oriented sagittal slices provided by 2D-SOMPR are described in the literature but not as frequently utilized in clinical practice. 3 The apparent advantages of 3DSR and 2D-SOMPR over 2D axial imaging are likely due to the longitudinal view of the cervical foramen that these modalities provide. This view of the neuroforamen is sometimes described as a “down the barrel” perspective, where the cervical foramen is conceptualized as a cylinder into which the reviewer may directly peer. This vantage point may allow for an intuitive assessment of stenosis, where the reviewers may directly view the space available for the nerve roots exiting the foramen. In contrast, 2D axial images may not transect the foramen evenly due to normal cervical spine lordosis altering the ideal slice angle, thus making a true foraminal diameter difficult to ascertain.
A secondary outcome of this study was interrater reliability in the recommendation to offer surgical decompression for any particular foramen. The advantages of 3DSR and 2D-SOMPR were born out in this analysis as well. While 3DSR did not provide increased agreement compared with 2D-SOMPR in determining the need for surgery, both modalities were markedly better than 2D axial slices in this regard.
One limitation of this study is that it pertains to the evaluation of foraminal stenosis due to bony rather than soft tissue pathology. When evaluating foraminal narrowing due to soft disc, ligamentous, or annular etiologies, MRI is the preferred option. Thus, this study relates to those clinical circumstances in which MRI provides incomplete assessment of bony foraminal narrowing, and CT is obtained for further evaluation of foraminal dimensions. These are frequently situations in which surgical decision-making is made more difficult than simply identifying an obviously herniated disc.
In conclusion, grading cervical foraminal stenosis using conventional axial CT imaging is a challenging task with only fair interrater reliability. CT modalities that provide a “down the barrel” view of the cervical foramen, such as sagittal oblique MPR and 3D CT reconstruction, may provide additional information to imaging reviewers, leading to increased interrater reliability when grading stenosis and deciding on surgical levels. No additional radiation is necessary in those whom a CT scan has already been obtained, as the reformation can be performed postacquisition. This imaging technology is readily applied to any CT image using ubiquitous workstation software. The routine use of 3DSR should be considered in CT evaluation of patients with cervical radiculopathy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John M. Rhee earns royalties from Biomet Zimmer Spine and Lippincott, is a consultant for Biomet Zimmer Spine, is a speaker for Depuy Spine, is a board member of the Cervical Spine Research Society, and holds stock in Phygen/Alphatec.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.