
Abstract
Study Design:
Technical report.
Objective:
Dorsolumbar vertebral dislocations, with or without associated fractures, occur secondary to very high velocity trauma. The reduction procedures and techniques, which may be adopted in these situations, have been multifariously discussed in the literature. Our objective was to assess the outcome of a novel reduction maneuver, using parallel rods which we have employed in reduction of high-grade thoracolumbar fractures to achieve precise sagittal balance as well as accurate vertebral alignment with minimal soft tissue damage.
Methods:
The study included a total of 11 cases of thoracolumbar dislocations, who had presented to our emergency spine services following high-velocity trauma. After appropriate systemic stabilization and necessary investigations, all patients were surgically treated using the described technique.
Results:
There were no surgical complications at 2-year follow-up. Radiographs showed good reduction and maintained sagittal balance.
Conclusion:
We believe that this technique is an excellent means of achieving safer, easier, and accurate reduction for restoration of sagittal/coronal balance and alignment in high-grade thoracolumbar dislocations. It is easily reproducible and predictable.
Introduction
Dislocations of the dorsal and lumbar vertebrae, with or without associated fractures, occur secondary to very high velocity trauma involving concomitant, multidirectional, compressive and distractive forces across various elements of the spinal column. 1 –6 Such dislocations have been considered as the most apocalyptic injuries and are often associated with devastating lesions of the spinal cord. These injuries frequently involve gross violations of all 3 columns of the spine, resulting in major spinal instabilities. 7 Therefore, such spines need to be reduced and stabilized appropriately without an undue delay. 8 –10 The reduction procedures and techniques, which may be adopted in these situations, have been multifariously discussed so far in the literature. 1 –14 The current article discusses a novel reduction maneuver, which we have employed in these circumstances and achieved precise sagittal balance as well as vertebral alignment with minimal soft tissue damage. The technical intricacies, benefits and pitfalls of this maneuver, detailed stepwise procedure involved and a brief literature review on alternative maneuvers employed hitherto, have been discussed elaborately.
Materials and Methods
The study includes a total of 11 consecutive cases of thoracolumbar dislocations, who had presented to our emergency spine services following high-velocity trauma. All the patients were initially managed in accordance with ATLS (Advanced Trauma Life Support) protocol and immobilized appropriately. After appropriate radiological (X-ray, magnetic resonance imaging [MRI,] and computed tomography [CT] scans, as appropriate) (Figures 1–3) and blood investigations, the patients were planned for surgical intervention and stabilization (based on the fracture pattern and classification). On neurological examination, 7 patients were graded as ASIA (American Spinal Injury Association) A, 1 patient as ASIA B in 1 patient, and 3 patients as ASIA C. All patients were operated within 12-24 hours of injury. Each patient was graded according to thoracolumbar injury classification system. Demographic details of patients are given in Table 1. Associated injuries were treated accordingly. The surgical procedure, which was performed in these patients, to obtain intervertebral reduction and anatomical alignment, has been expatiated upon below. No patient was lost to follow-up.
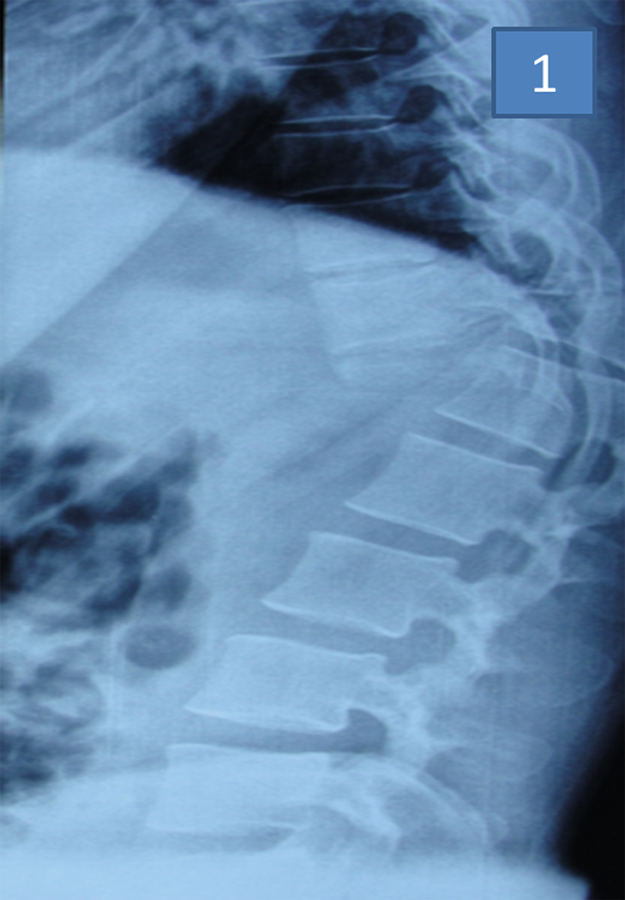
Thoracolumbar radiograph showing T11-T12 level fracture dislocation.
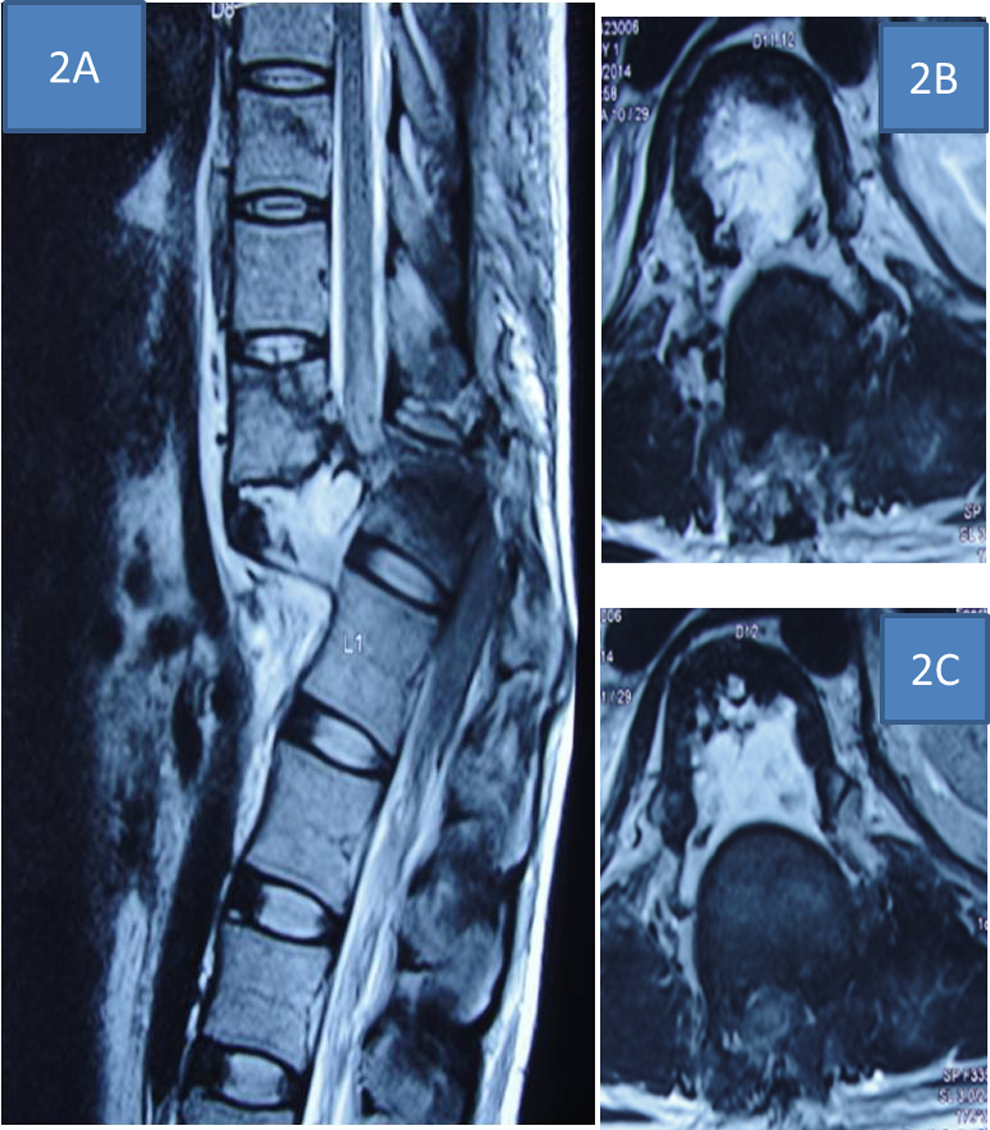
(A, B, C) Magnetic resonance images (sagittal and axial) showing cord transaction at T11-T12 level.
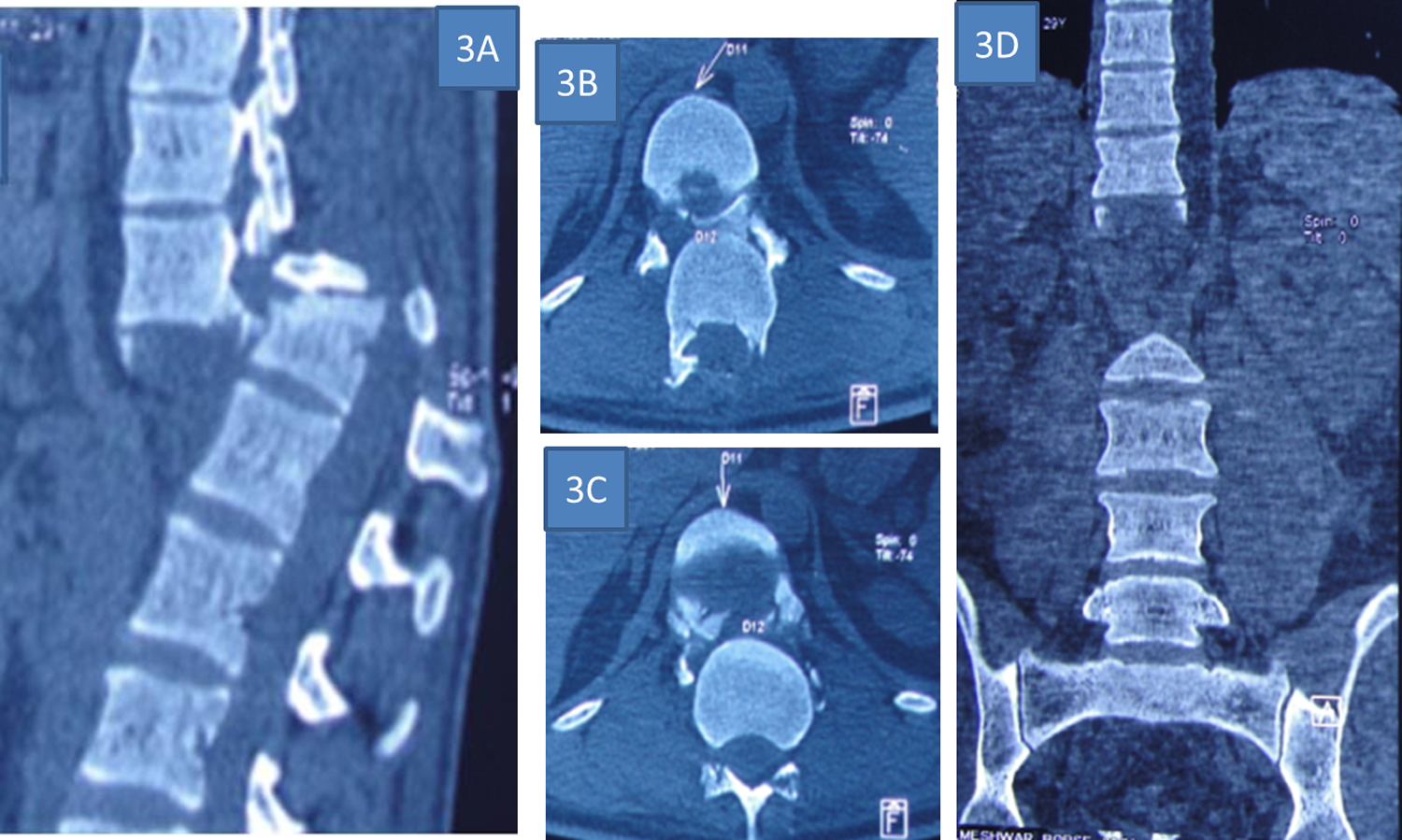
(A, B, C, D): Computed tomography (sagittal, axial, and coronal) scans showing T11-T12 dislocation.
Demographic Details of Patients.
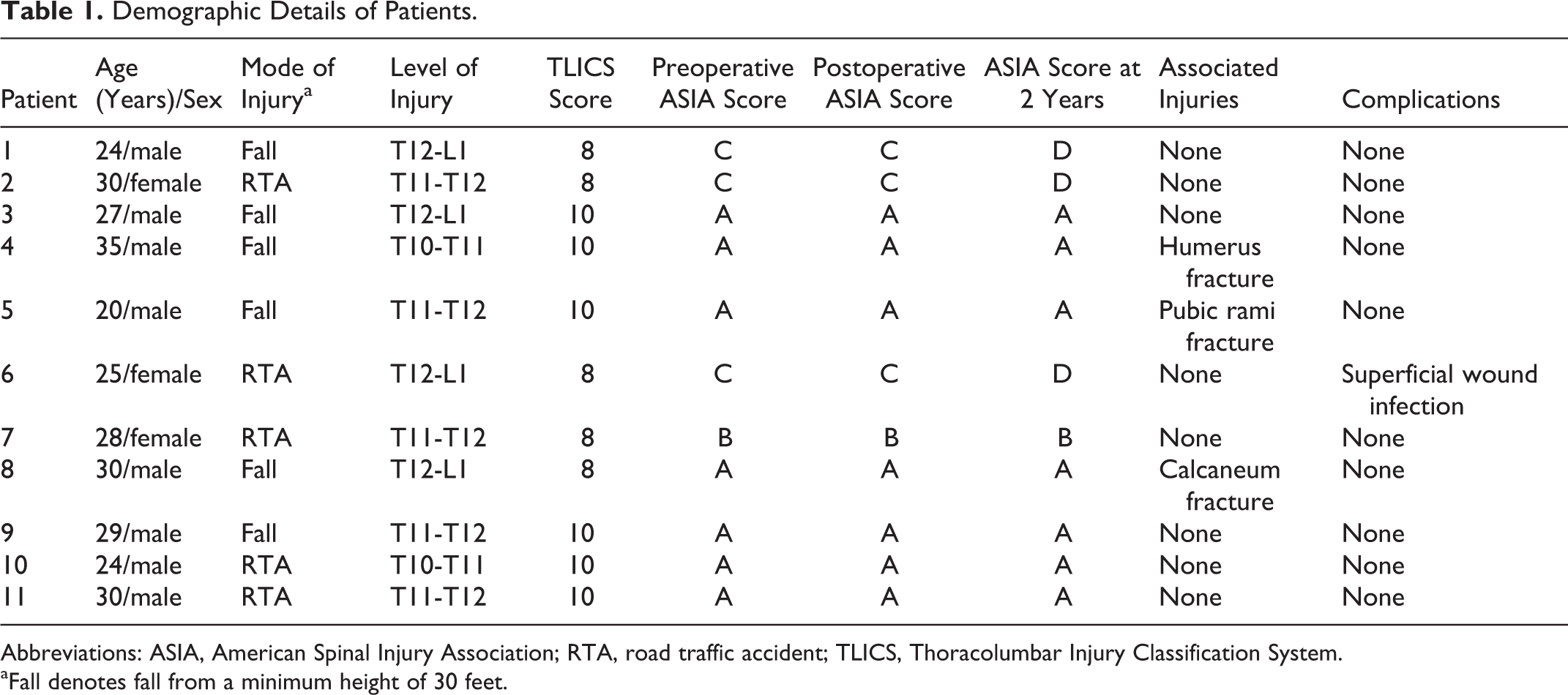
Abbreviations: ASIA, American Spinal Injury Association; RTA, road traffic accident; TLICS, Thoracolumbar Injury Classification System.
aFall denotes fall from a minimum height of 30 feet.
Surgical Technique
Patient Position
Prone position (proper patient positioning with appropriate lordosis may aid in achieving partial vertebral reduction in a proportion of patients).
Approach
Posterior midline approach—midline skin incision is performed and paraspinal muscles are gradually raised from their insertions. The posterior vertebral elements including laminae and spinous processes are exposed. Care should be taken, as there is injury to posterior elements and laminectomy defects. Care should be taken at the level of fractured vertebrae, so as to avoid any violation of the spinal canal and vital neural elements, which might be transgressed at the time of initial injury itself. The vertebral facets and transverse processes are exposed at the appropriate levels.
Steps
Pedicles screws are inserted at 2 levels above and below the level of dislocation bilaterally (eg, in D11 D12 dislocations, pedicle screws are inserted into D10 and D11 vertebrae proximally, as well as D12-L1 vertebrae distally) (Figure 4A).
Two small rods are inserted into the pedicle screws: One rod is applied proximal to the injury site (eg, D10 and D11 vertebrae) and the other distally D12 and D11 vertebrae) (Figure 4B).
After confirming the levels and positions of the pedicle screws under fluoroscopy, 2 vice grips are applied to hold the rods on either side of the injury site (Figure 4C).
Then, the operating surgeon holds the 2 vice grips carefully and performs the following 3-stepped reduction maneuver: The surgeon initially applies gradual, gentle, and sustained distraction across the dislocated vertebrae. Then, with maintained distraction, the surgeon pushes the anteriorly displaced proximal vertebrae further anteriorly (considering the common situation, where the proximal column is subluxated anteriorly, in relation to the distal one); and pulls the distal vertebrae in an posterior direction; thereby enhancing the displacement further, leading to unlocking and disimpaction of the dislocated vertebrae. It is important to cautiously perform this maneuver after distraction to aid reduction. Maintaining these sustained forces, the facets are completely unlocked; and further reductive forces are provided in the diametrically opposite directions (proximal column is now pulled backward and the distal one forward), so as to achieve a congruent reduction of the facets bilaterally. Care should be taken to avoid any jerky, violent thrusts while performing these maneuvers. Additional rotational manipulations may be required in selected cases to achieve reduction.
All these manipulations should be carried out in as gentle a manner as possible. Unnecessary forceful maneuvers, which may be detrimental to vital structures, should be strictly avoided. If there is any restriction to achievement of smooth reduction, the surgeon should carefully assess the soft tissue and bony structures, which may hinder the facetal relocation and get rid of them before further attempts.
As the operating surgeon maintains the reduction thus achieved with continued forces in the direction of reduction, an assistant applies a rod on the opposite side across the pedicle screws and temporarily fixes the vertebrae in reduced position.
The temporary short rods, initially applied, are then removed; and another long rod is applied on the other side too. The reduction, alignment and stabilization are verified under fluoroscopy and a final tightening of the screws carried out.
We prefer to preserve a protective layer posterior to the cord till these manipulative procedures are completed; thereby obviating any further evitable injuries to the neural elements and dural breaches resulting from inadvertent slippage of the instruments.
Complete decompression of the cord is then finally performed (with removal of spinous processes and bilateral laminectomies) at the injured level. Performing laminectomies is difficult in such situations and utmost care should be taken to prevent neural injuries (cerebrospinal fluid leak, etc). The dural elements are then thoroughly envisaged and checked for any defects and appropriate repairs are carried out, as required. A gelfoam or a fascial pad is placed posteriorly to cover the open neural elements (Figure 4D). Performing decompression before stabilizing the spinal column is technically challenging and can have high chances of neural injuries. Moreover, any event of cerebrospinal fluid leak encountered can be difficult to address in an unstable spinal column, so we prefer to perform laminectomy after spinal stabilization.
A transverse cross-link is then applied to provide additional strength and stability to the construct. Autologous graft materials, consisting of the leftover bones procured from laminectomy together with additional graft from iliac crest, are then placed in the lateral gutter at the intertransverse zones to facilitate and enhance fusion (Figure 4E).
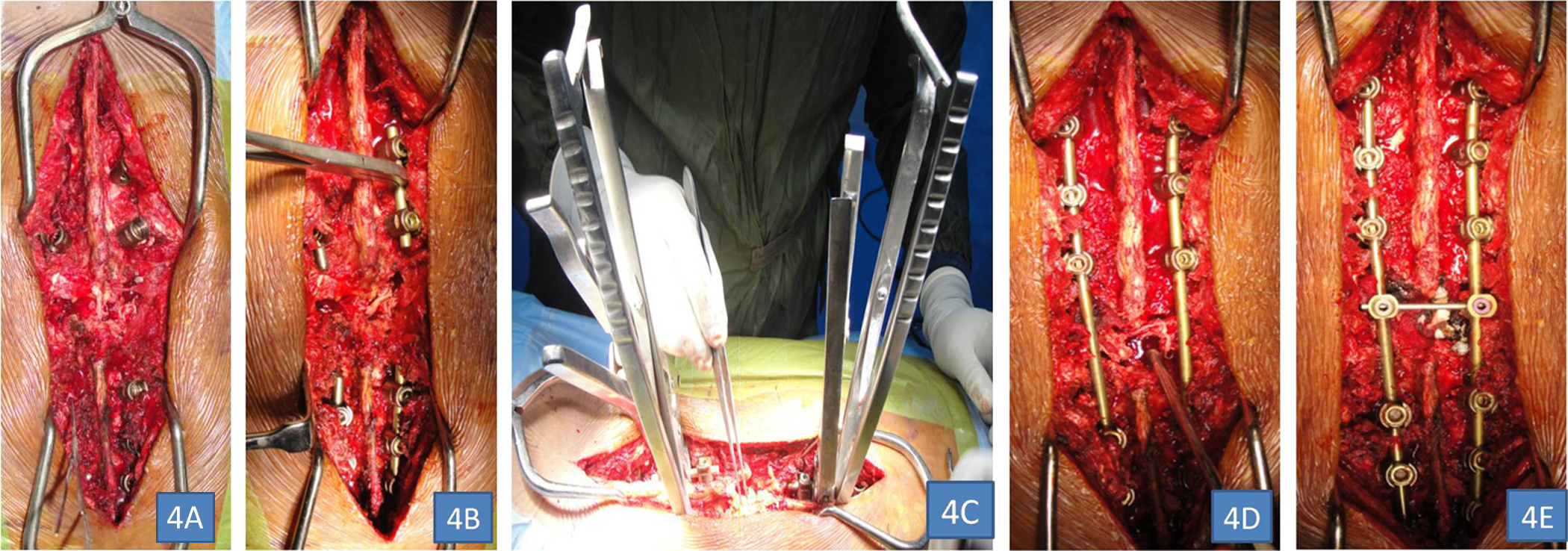
Intraoperative photographs showing steps in reduction maneuver: (A) pedicle screw insertion above and below the level of fracture dislocation, (B) 4 rods inserted (2 above and 2 below) on either side of fracture, (4) vice grips applied to the rod on either side to perform reduction maneuver, (D) permanent rods applied replacing the temporary small rods and decompression done at site of injury, and (E) interlink applied.
Postoperative Protocol
All patients were gradually mobilized on the second postoperative day with appropriate orthotic aid. Routine physiotherapy protocols, including gradual strengthening of the core muscles, wheel chair mobilization in paraplegics, and walking with appropriate aids, were systematically carried out in all patients. Patients were followed up for minimum 24 months and radiographs were obtained to ensure thoracolumbar reduction and alignment.
Results
Postoperative radiographs showed good reduction with maintained sagittal balance in all cases (Figure 5A and B). There were no neurological deteriorations (ASIA B and ASIA C) or surgery-related complications in postoperative period in any of our cases. Complications associated with prolonged immobilization especially in paraplegics like chest infection, urinary tract infection, bed sores, and so on, were managed appropriately. Outcome was assessed radiologically and checked for maintenance of reduction in sagittal and coronal plane. Fusion was assessed using radiographs at follow-up. At 2-year follow-up, radiographs show maintained sagittal/coronal alignment and no hardware-related complications (Figure 6A and B).

Postoperative radiographs.
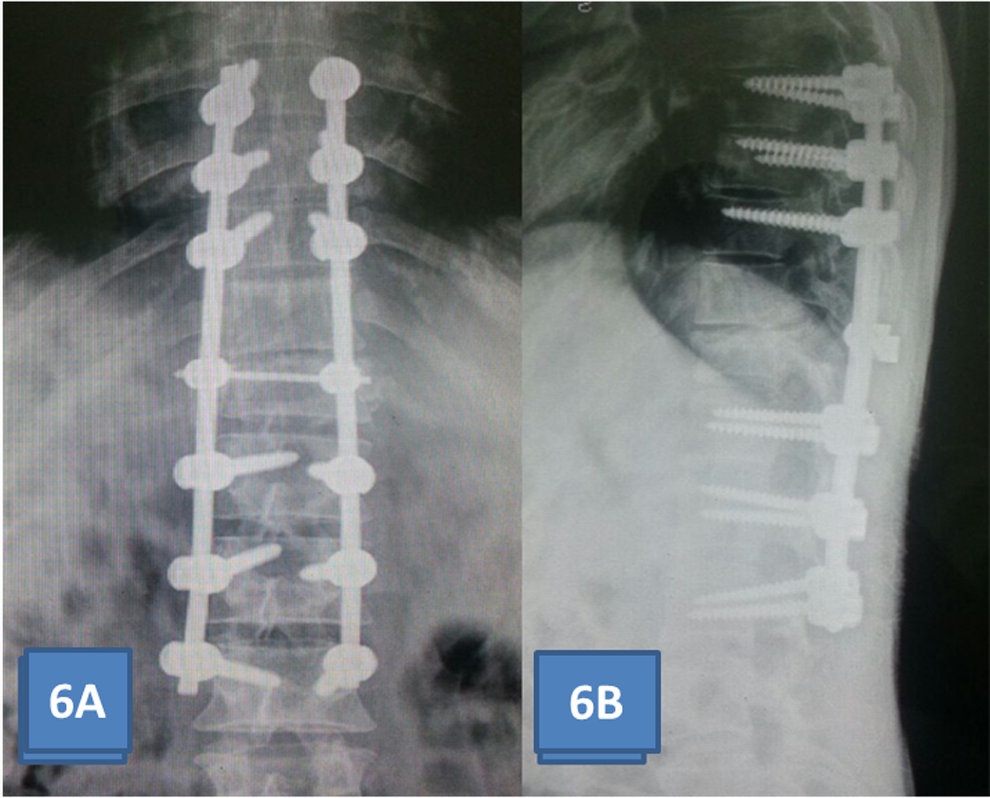
(A, B) Radiographs at 2-year follow-up.
Discussion
Vertebral dislocations are high-energy lesions, which have especially been described at the highly mobile, high-stress junctional segments of the vertebral column, including the cervical vertebrae, thoracolumbar junctions, and lumbosacral junctions. 1,2,13,14 Literature has also described a few cases of mid-lumbar vertebral dislocations, involving unilateral and bilateral displacements of the facetal articulations. 5 These injuries have usually ensued high-velocity road traffic accidents or falls from heights, although certain underlying conditions, such as spinal bifida or rheumatoid arthritis may facilitate these injuries, even in situations of less violent trauma. 15,16 Various theories 1,8 have been purported in the literature to explain the underlying mechanisms involved, including a combination of flexion-distraction forces; simultaneous hyperflexion–rotation–lateral translation–shearing–compression forces; or significant hyperextensile forces 6 (as originally described by Watson-Jones 6 in lumbosacral dislocations). Nevertheless, the major dislocating mechanism predominantly involves a rotational vector at cervical and lumbosacral levels (with coronally oriented facets) and hyperflexional elements at the majority of other levels (with sagittal facet orientation), especially in those situations where these dislocations are not accompanied by significant bony fractures. 1,6,8
These are annihilating injuries, and are often accompanied by complete cord transections and significant neurological damages. 5 However, the association with other grievous systemic injuries, including vascular, abdominal, and thoracic visceral lesions (especially, as observed following direct trauma in seat-belt syndromes), renal contusions and other pelvic visceral and bony injuries needs to be fore grounded. 17 –20 These patients thence need adequate monitoring and systemic stabilization, prior to any specific radiological investigations and surgical planning. Plain roentgenograms, MRI and CT scans form important components of surgical planning and aid in understanding the specific fracture morphologies. 17 –20
The reduction technique described in our article is a novel method of achieving relocation of these displaced vertebrae, with observed benefits, including minimal risks for additional neurological insults, lesser iatrogenic soft tissue disruptions, and relative preservation of biomechanically crucial structures. It is based on the concept that in these grossly dislocated spines, the proximal and distal segments behave like separate entities, which have undergone anteroposterior and lateral shifts, tilts, and displacements, with simultaneously associated significant overlaps in the longitudinal plane. The technique includes sequential manipulations, with initial establishment of proximal and distal anchorage to the spinal columns, using 2 short pedicle screws-rods constructs. Further maneuvering is performed by an experienced surgeon, who controls the 2 disjunct segments, with appropriate grasps using vice grips applied on the rods on either side. The 3-step reduction maneuver is performed, with traction forming the most important initial, disimpacting manipulation, which helps in overcoming the overlap. The successive maneuver includes partly exaggerating the displacement by gradual, controlled mobilization of the segments in the same direction as their postinjury shifts. These 2 disimpacting maneuvers are crucial; as if unreasonable coercion is applied during these manipulations, inadvertent, secondary, iatrogenic damage to the cord and neural elements may ensue. The final stage of reduction involves application of force in the direction antagonistic to the initial direction of slip and maintaining the position of reduction with sustained, nonjerky pressure. It should be cautioned that initial maneuver of exaggeration of deformity can cause further narrowing of canal and there is risk of pulling bone fragments or disc material while performing the reduction. Also, anterior vascular structures can be jeopardized due to stretching. Therefore, one has to be gentle, steady, and graded in performing the maneuver. In one of our cases, we preferred to apply the initial, pedicle screw-rod construct on diagonally opposite sides (one on the right and the other on the left), as we felt it would provide us with a biomechanically sounder frame in that specific situation. We had significantly large lateral translational and rotational components of displacement in that patient, which forced us to try this alternative assembly. Though this construct significantly aids in easing out the reduction in these difficult situations, it becomes technically difficult to perform the final stabilization by replacing this temporary fixation (on either side) with the longer rod.
There have been other methods described in literature to effect reduction in these injuries. A three-staged closed reduction technique was described by Bohler involving lumbar hyperlordosis, using a Cotrel frame. 21 –23 However, the current emphasis is on open reduction in all these patients through a posterior approach. This approach enables complete, direct, posterior decompression of the nerve roots and helps in achieving posterolateral fusion with intertransverse bone graft. There have been suggestions that use of halobifemoral traction 24,25 during the preoperative period may aid in achieving easier and safer reduction intraoperatively. Nevertheless, this practice of closed pre-operative traction is fraught with possible complications resulting from overstretching of lumbar roots or brachial plexus; or as a consequence of immobilization (eg, deep vein thrombosis). 5 Diverse open reduction maneuvers have been broadly discussed, including direct manual reduction by applying traction to the spinous processes, 5 applying distraction using interspinous laminar spreaders, 26 –29 or using small curettes 13 to maneuver the superior jumped facet out of the locked position (especially in the subaxial cervical spine). Notwithstanding, these manipulations have a significant rate of failure in achieving reduction, which may necessitate more invasive procedures, such as partial facetectomies and laminectomies and resection of ligamentum flavum or other soft-tissue or bony remnants (which may hinder the reduction). 5 With our technique, we did not need to perform facetectomy or excessive resection of bony structures in any of our patients. With a good grip of the proximal and distal vertebrae (using the screw-rod construct at 2 levels above and below the dislocated level) and sequential, gentle manipulations as described, the reduction could be achieved, with minimal insult to the vital neural elements and relative preservation of the critical stabilizing bony components of the vertebrae (especially the facets). Nonetheless, care should be taken to avoid unduly jolty and excessively forceful handlings during the reduction. If there is any difficulty in mobilizing and maneuvering the vertebrae, the procedure must be temporarily aborted, possible elements obstructing the reduction should be assessed, release of necessary structures coming in the way of reduction (including, facet capsule, ligamentum flavum, loose bony fragments, etc) must be considered, as required and then the procedure gently repeated all over. Complete, posterior decompression of the nerve roots is then carried out.
We believe that the technique, thus described is an excellent means of managing thoracolumbar dislocations with or without associated fractures. If performed the right way, it can help in achieving safer, easier, and accurate reduction and sagittal balance restoration. The importance of achieving good alignment and reduction even in patients with complete cord damage (in whom neurological recovery may not be feasible) needs to be emphasized on, as the reduced spine helps in vital restitution of its biomechanical stability, thereby facilitating easy rehabilitation and recuperation of paraplegics. However, we would like to emphasize on the importance of adequate experience and expertise on part of the operating surgeon, as inadvertent violations of nervous tissues can occur if proper care is not taken. In these situations, the need for a stable construct with long segment stabilization and augmentation with additional transverse cross-links following reduction cannot be understated. 5 This technique adds to armamentarium of treating surgeons if standard techniques are unable to get reductions. It is easy to understand, perform, and is reproducible.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.