
Abstract
Single-port laparoscopic appendectomy (SPLA) has become a good alternative to the traditional surgical treatment of acute appendicitis, due to its advantages of small incision, mild postoperative pain, short hospital stay, and good cosmetic effect. However, the further application of SPLA has been restricted by its relatively long operating time, high level of operating difficulty, and increased equipment and technical requirements. Clinical teams worldwide have attempted to improve and optimize SPLA technical protocols and equipment to maintain stable intraoperative pneumoperitoneal pressure, improve the ‘triangle relationship’ of operating angles, and develop new surgical procedures with less trauma and higher cost-effectiveness. Here, new SPLA techniques reported over the past decade are reviewed and compared, with the aim of providing new insights into technical improvements, equipment upgrades and clinical studies in the coming years.
Keywords
Introduction
Acute appendicitis is a major health issue worldwide, and in particular, the coronavirus disease 2019 pandemic has been associated with a significant increase in the proportion of patients with complicated appendicitis.1,2 Although the roles of medical or surgical interventions remain controversial, early surgery is considered an effective option and has been widely adopted.3–5 With socioeconomic development and increasing demands on cosmetic appearance and minimally-invasive surgery, more minimally-invasive surgical procedures (e.g., endoscopic surgeries) without creating an incision in the abdominal wall, have emerged. 6 However, their applications have been limited due to the high levels of operating difficulties and equipment requirements, and long learning curves. In contrast, since George Kelling described laparoscopy in 1901, 7 laparoscopic surgery has been increasingly applied in clinical settings due to its relatively simple operation, short learning curve, and feasibility for comprehensive abdominal exploration. Compared with the traditional three-port approach, single-port laparoscopy has been confirmed to be effective and safe in the treatment of acute appendicitis, along with many other advantages, including less trauma, less pain, shorter hospital stay, and improved cosmetic effect.8–14
Nevertheless, is single-port laparoscopic appendectomy (SPLA) truly perfect and curative for various types of appendicitis? Unfortunately, the single-port laparoscopic technique is known to depend highly on specialized instruments and is difficult to perform due to parallel angles, which increases the cost of hospitalization, prolongs the learning curve, and ultimately limits the adoption of this technology. All of these factors should be addressed in further studies, because only by improving the equipment and techniques, and achieving better clinical outcomes, will single-port laparoscopic surgery be widely accepted. 15
Unlike previous reviews or meta-analyses that focused on comparisons with conventional three-port laparoscopic appendectomy, the aim of the present narrative review was to summarize the novel, minimally invasive techniques of SPLA reported in articles published in the PubMed, Medline, and Cochrane Library databases over the past decade, and to compare the research methods, surgical instruments, and clinical outcomes between different technical protocols, in an attempt to provide evidence in the improvement, upgrading and promotion of the SPLA technique.
Materials and methods
The PubMed, Medline, and Cochrane Library databases were searched for articles published up to 31 October 2022, using the keywords ‘single port’, ‘single incision’ and ‘appendectomy’ and the search restriction ‘PUBLICATON DATE-10 years’. Adult, paediatric and pregnant patients were all included in the current review. Articles published in a language other than English or unrelated to the topic of interest were excluded. The literature search and data collection were executed independently by four reviewers (ZF, XZ, XF, and JL), and any inconsistent results were resolved by the participation of a fifth reviewer (JY). The current review followed the PRISMA 2020 guideline. 16
Results
A total of 1341 potentially relevant articles were identified through searching the PubMed, Medline, and Cochrane Library databases, of which, 1321 articles that were found to be duplicates, or unrelated to the topic of interest, published in a language other than English, or other reasons, were excluded. In addition, three case reports that lacked sufficient clinical evidence and reliability were also excluded. Finally, 17 research articles or case series on SPLA, from the Republic of Korea, China, India, Spain, and other countries, were included in the present review.17–33 Most articles were from the Republic of Korea (n = 6), followed by China (n = 4), India (n = 3), Vietnam (n = 1), Argentina (n = 1), Egypt (n = 1), and Spain (n = 1). There were eight retrospective studies, six prospective studies, and three case series (Figure 1). Surgical techniques, equipment, and devices, including magnet-assisted single trocar (MAST), needle grasper (Endo Relief)-assisted single-incision laparoscopic appendectomy (NASILA), and SPLA using a needle-type grasping forceps (SLAN) are summarized (Table 1).17–33 The performance of each technique was also compared in terms of clinical outcomes (Table 2).

Flowchart of the selection of studies included in the current review of single-port laparoscopic appendectomy.
Summary of 17 studies of single-port laparoscopic appendectomy included in the current review.

CLA, conventional laparoscopic appendectomy; CMLA, conventional multiport laparoscopic appendicectomy; MAST, magnet-assisted single trocar; NA, needlescopic appendectomy; NASILA, needle grasper (Endo Relief)-assisted single-incision laparoscopic appendectomy; SILA, single-incision laparoscopic appendectomy; SILACI, single-incision laparoscopic appendectomy using conventional multiport laparoscopic instruments; SILACIG, single-incision laparoscopic appendicectomy with conventional instruments and glove port; SLAN, single-port laparoscopic appendectomy using a needle-type grasping forceps; SPA, single-port laparoscopic appendectomy; SPLS, single-port laparoscopic surgery; SSILA, suprapubic single-incision laparoscopic appendectomy.
Comparison of patient demographics and clinical outcomes associated with novel single-port laparoscopic techniques used in various studies.
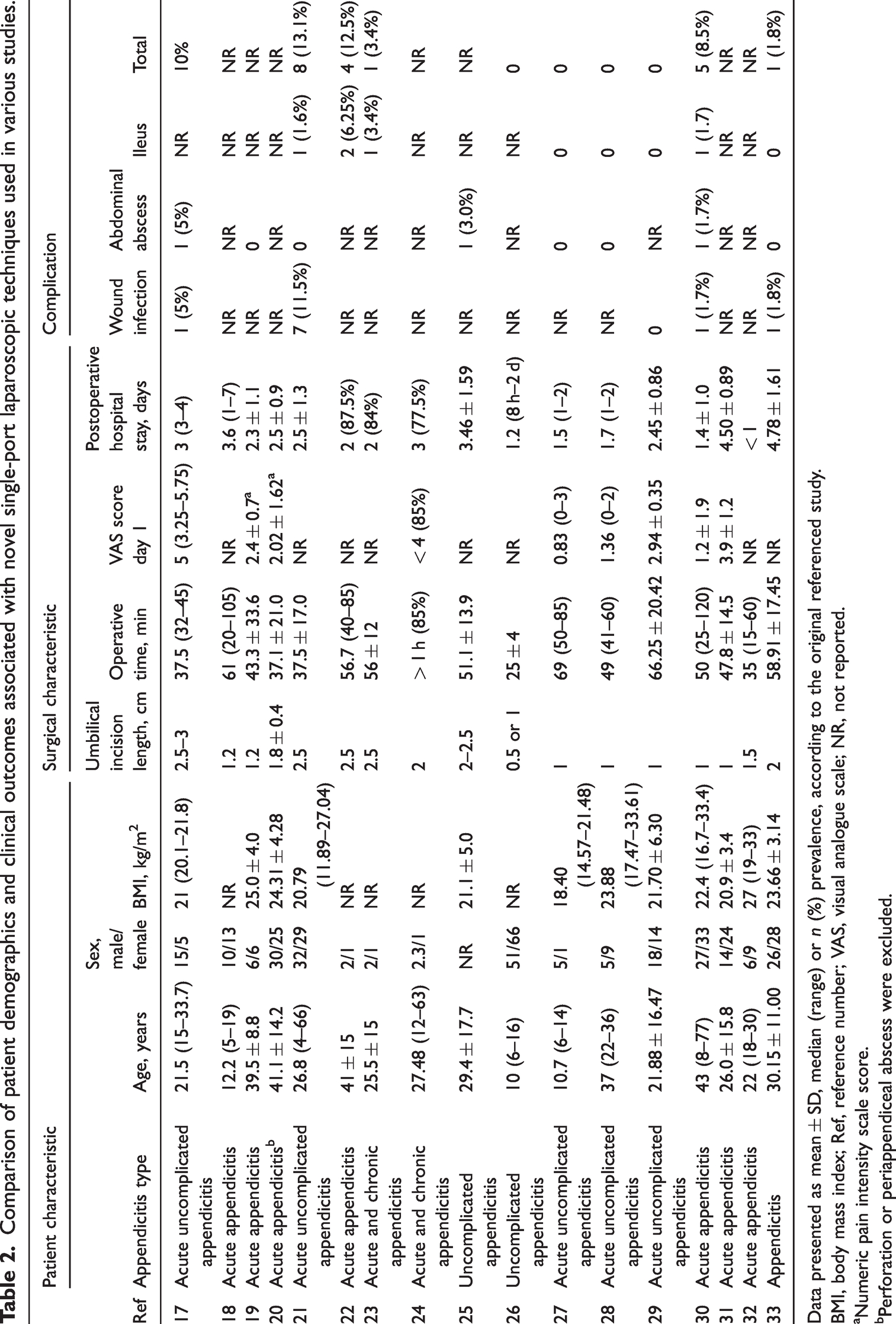
Data presented as mean ± SD, median (range) or n (%) prevalence, according to the original referenced study.
BMI, body mass index; Ref, reference number; VAS, visual analogue scale; NR, not reported.
Numeric pain intensity scale score.
Perforation or periappendiceal abscess were excluded.
Current techniques review and comparison of technical programs and clinical outcomes between different single-port laparoscopic surgery procedures
Maintaining stable pneumoperitoneal pressure and rational selection of surgical instruments is essential to ensure adequate laparoscopic exposure of the operating field and smooth surgical process. In view of this, the selection of equipment and devices may differ between various international surgical teams, resulting in different clinical outcomes.
A variety of homemade surgical gloves were found to be widely used, because they are easy-to-make, effective, and, more importantly, affordable.17,23–25,31,33 In order to prevent surgical site infection, studies from Vietnam and the Republic of Korea described the application of an ALEXIS XS wound retractor (Applied Medical, Rancho Santa Margarita, CA, USA) during surgery.17,31 Other incision protecting measures (e.g., homemade wound protector ring) have also been reported.23–25,33 Nevertheless, surgical site infection still occurred after single-incision laparoscopic appendectomy (SILA) performed through a handmade surgical-glove port (n = 1, 5.0%), 17 or after suprapubic single-incision laparoscopic appendectomy (SSILA; n = 1, 1.8%). 33 The highest incidence of surgical site infection after SILA was reported by Chong et al., 21 reaching 11.5% (n = 7). Therefore, the principle of aseptic operation should always be emphasized. The percutaneous organ-holding device (Suture Grasper Closure Device; Mediflex Surgical Products, Islandia, NY, USA), as described by Lee et al., 31 was also applied in the single-port needlescopic appendectomy (NA) by Ismail et al, 26 and exhibits a good auxiliary role in clamping the appendix and tying knots, thus avoiding the creation of more surgical incisions; in addition, its 1-cm tiny umbilical incision offers a minimally-invasive and aesthetic solution, which is quite similar to the needle forceps used by the current team. In addition, the venous access cannula and homemade microdiathermy needle used by Ismail et al. 26 can achieve sharp separation of the appendix without creating additional surgical incisions, which facilitates the realization of single-port laparoscopic surgery. The use of traditional three-port laparoscopic trocars and operating instruments to complete a single-port laparoscopic surgery has also been reported in India, Korea, and China.23–25,33 Compared with the traditional three-port laparoscopic surgery, this new technique does not increase hospitalization costs and therefore is more affordable. Among these techniques, the protocol designed by Que Son et al. 17 had the shortest mean operating time (37.5 min), which may be explained by the following: the use of an ALEXIS XS Wound retractor (Applied Medical) combined with surgical-glove port effectively maintains stable pneumoperitoneal pressure and the use of a percutaneous organ-holding device (Suture Grasper Closure Device; Mediflex Surgical Products) effectively improves the parallel operating angles of traditional single-port laparoscopic surgery, ensuring a smooth surgical operation.
Traditional laparoscopic trocars have also been used by many teams.18,22,26–29 Among them, both the single-incision laparoscopic appendectomy using conventional multiport laparoscopic instruments (SILACI), completed by Uday et al., 22 and the SLAN designed at the present authors’ centre (Chaoyang Central Hospital),27–29 were completed using the traditional three-port laparoscopic instruments. Notably, SLAN showed a smaller mean incision length than SILACI (1 cm versus 2.5 cm), which may have been due to needle forceps used at Chaoyang Central Hospital to assist the operation, during which only two 5-mm trocars were required for entry, observation and operation. In contrast, SILACI requires a slightly shorter average operating time than SLAN (56.7 min versus 66.25 min), which may be associated with the soft texture of the needle grasping forceps used in SLAN, insufficient stability of pneumoperitoneal pressure, and difficulty of operation due to small incision length. SLAN will be further optimized in both design and practice based on the currently available techniques and our clinical experience. Some specially-designed surgical instruments have also been described.18,26 The MAST appendectomy uses the Dominguez magnetic grasper, 18 which effectively reduces the number of incisions through magnet adsorption. However, single-port NA using Mediflex showed many advantages, 26 including smaller incisions (0.5 or 1 cm versus 1.2 cm), shorter average operating time (25 min versus 61 min), and shorter average postoperative hospital stay (1.2 days versus 3.6 days), which may be because the use of venous access cannula, homemade microdiathermy needle, and percutaneous organ-holding device (Suture Grasper Closure Device; Mediflex Surgical Products) is more adaptable to the operating procedure of traditional three-port laparoscopic surgery, which helps to lower the surgical difficulty and shorten the learning curve.
The paediatric glove port (Nelis Corp., Bucheon, Korea) or glove port (Nelis Corp.) are mainly used in the techniques described by Korean teams.19–21,30 NASILA is performed using a paediatric glove port (Nelis Corp.) in combination with a needle grasper (Endo Relief),19,20 which is similar to the needle forceps used in the present authors’ SLAN technique. Although the average NASILA operating time was shorter than SLAN (37.1 and 43.3 min versus 66.25 min), their average incision was longer (1.2 and 1.8 cm versus 1.0 cm); and other postoperative clinical outcomes showed no significant differences. The protocol described by Chong et al. 21 did not use additional instruments, with lower cost and shorter operating time (37.5 min); however, it resulted in negative clinical outcomes, such as longer surgical incision (2.5 cm) and higher surgical site infection rate (11.5%); notably, postoperative intestinal obstruction was found in one case (1.6%). Thus, this technique still has room for improvement. Kim et al. 30 described the solo-surgery technique, which can be performed by the operator alone without an assistant. The use of a Lone Star retractor (3307G; Cooper Surgical, Trumbull, CT, USA) requires just a 1-cm incision, and the tiny trauma results in mild pain (mean visual analogue scale [VAS] score 1.2 ± 1.9) and short postoperative hospital stay (mean duration 1.4 ± 1.0 days). However, complications, such as surgical site infection (1.7%), intra-abdominal abscess (1.7%), and intestinal obstruction (1.7%), should also be noted. Careful selection of patients may help reduce postoperative complications. In addition, surgical safety and medical disputes may also be concerns during its large-scale promotion.
Similarly, a Spanish team chose to insert the R-port via a 1.5-cm transverse incision above the pubic bone, 32 changing the observation angle of the surgical field; similar to a Caesarean-section incision, the incision is low and hidden, achieving acceptable cosmetic effects. However, the Spanish study was a case series, and further large-scale clinical studies are pending.
Optimal surgical treatment strategy for patients with acute appendicitis
Different types of newly developed minimally-invasive surgical procedures have their own advantages and characteristics, and compared with traditional three-port laparoscopic surgery, they showed positive clinical outcomes in terms of cosmetic effect and patient satisfaction.8–14 However, the use of specialized instruments and parallel approaches increase the cost of hospitalization and the difficulty of surgical procedures and learning curves, therefore, limitations in their clinical application and promotion remain. Tailored intervention protocols based on patient needs and clinical conditions will help improve surgical outcome and patient prognosis.
Given the upgrading of surgical instruments, it seems that age and body mass index (BMI) are no longer limitations for single-port laparoscopic surgery, 34 and technical protocols for novel single-port laparoscopic surgeries have become available for both children and adults with an average BMI of 18.4 kg/m2 to 27 kg/m2. Since a single umbilical incision is created during single-port laparoscopic surgery, no abdominal drain can be placed after the surgery, which may also be one of the reasons for the milder postoperative pain.
Notably, careful selection of patients remains important to ensure maximal safety and feasibility. Preoperative computed tomography may have advantages in assessment of disease conditions, especially in patients with bowel wall thickening, as previously reported. 35 Considering the mild inflammatory status and uncomplicated surgical procedures, SPLA has frequently been performed in patients with uncomplicated appendicitis.17,21,25–29 Conversely, patients with complicated appendicitis are at higher risk of conversion to laparotomy, for whom strict surgical indications should be adopted. 36 In cases where indwelling abdominal drainage tubes are required (e.g., for appendiceal perforation), the selection of single-port laparoscopic surgery becomes limited. Caution should be used in the selection of a single-port laparoscopic technique in patients with perforated appendicitis, and its value still needs to be further explored in clinical studies. The safety and feasibility of single-port laparoscopic surgery during pregnancy have been reported, 37 and this also requires further investigations in large studies.
Using concealed incisions, decreased numbers of incisions, and shortened incision length can achieve satisfactory cosmetic outcome. Among the technical protocols reviewed, SLAN, designed by the present authors’ team, and the techniques described by Ismail et al., 26 Kim et al., 30 and Lee et al., 31 all used an incision of no more than 1 cm in length. For paediatric patients, single-port NA with Mediflex used only a 0.5-cm umbilical incision, 26 through which a 5-mm laparoscope was inserted to complete the operation; the mean operating time was only 25 min and the mean postoperative hospital stay was 1.2 days; no complication was reported in all 117 patients, suggesting that this technique was the least invasive method to date. Notably, these findings were obtained from a high-quality multi-centre prospective clinical study. 26 Garijo et al. 32 reported using a 1.5-cm concealed transverse incision on the pubic bone that provided a good surgical field. Although single-port laparoscopic surgery has been shown not to increase the risk of surgical site infection, 38 its long-term cosmetic outcome remains controversial and needs to be validated in long-term follow-up studies. 39
Lowering surgical cost may reduce the economic burden of patients and improve cost-effectiveness. The techniques described by Uday et al.,22,23 Muneef et al., 24 and Lee et al. 25 may also be performed using conventional instruments, which are more acceptable in price, however, incisions of 2–2.5 cm don’t satisfy the requirements of modern minimally-invasive surgeries. Similarly, Chong et al. 21 directly applied the instruments and methods of three-port techniques to single-port laparoscopic surgery, during which a comfortable ‘triangle relationship’ angle was created. This new technique reduces the learning curve, but its high rate of complications (13.1%) remains a concern. The 2.5-cm umbilical incision also needs to be improved.
Future technique optimization and evidence-based research
The development of minimally invasive surgical techniques highly depends on improvements in instruments and methods. The past decade has shown many innovative advances in new equipment and methods for laparoscopic appendectomy, including homemade gloves, and the paediatric glove port and glove port (both Nelis Corp.), which have effectively improved the maintenance of stable pneumoperitoneal pressure during surgery. The use of a venous access cannula, homemade microdiathermy needle, and percutaneous organ-holding device (Suture Grasper Closure Device, Mediflex Surgical Products) helps to lower the surgical difficulty and shorten the incision length. However, as reported in some studies, issues of long incisions, multiple complications, high cost, and low quality of clinical studies still need to be addressed. The future development of new surgical procedures for SPLA should be based on patient demand for cosmetic appearance and minimally-invasive approaches. New surgical protocols that can handle the parallel operating angles, maintain stable pneumoperitoneal pressure, reduce surgical trauma, and increase patient comfort should be actively explored while upgrading equipment. Although studies have proposed that single-port laparoscopic surgery can be used in internship programs,40–42 we suggest that this procedure remains a highly challenging technique, 43 which may also be one of the reasons for the longer operating time.44,45 Furthermore, postoperative complications, such as abdominal abscess and incision hernia, may also occur.40,46 Therefore, before the adoption of a new technique in clinical practice, careful patient selection and intensive professional training are necessary to reduce postoperative complications; for obese patients or patients with complex conditions, including perforated appendix occurring during the procedure, conversion to the traditional three-port technique or open surgery should be considered in a timely manner. 47
There is no doubt that surgeons pay close attention to improvements in clinical practice, especially the research and development of new surgical techniques, which may add a stronger sense of professional success. However, clinical studies, particularly evidence-based high-quality studies, may yield more effective and reliable evidence to justify current clinical work, optimize clinical protocols, and avoid inappropriate clinical decisions and/or unnecessary sacrifices and waste.48–50 At present, clinical studies on SPLA are generally of low quality, and most that were published over the past decade were case reports and retrospective studies. Future high-quality, prospective, randomized controlled trials should be actively carried out to further validate the safety and efficacy of new technologies and to assess long-term clinical outcomes.
In summary, although a variety of new types of single-port laparoscopic techniques can be searched in the literature, few procedures were proved to be perfect by comprehensive and reliable clinical evidence, and studies were not performed as widely and globally as three-port laparoscopic appendectomy for treatment of various types of appendicitis. Therefore, there is still a long way to go.
Conclusion
Over the past decade, advances in surgical equipment and protocols for SPLA have greatly benefited patients with acute appendicitis in terms of hospital costs, number of surgical incisions, and postoperative hospital stay. However, issues of longer single-incision length, higher complication rates, and longer operative time still need to be addressed in most technical procedures. Considering the limitations of the single-port laparoscopic technique in specific device applications, and the inability to retain laparoscopic drainage tubes, surgical instruments and techniques should be rationally chosen based on disease status and patient needs. Unfortunately, the quality of currently available clinical studies is generally low, and high-quality prospective randomized controlled trials on equipment upgrading and procedure improvement are warranted.
Footnotes
Author contributions
YC and SG: conception and design. ZF, XZ, XF, JL, and JY: literature search and selection, and data collection and analysis. YC: manuscript writing. All authors reviewed and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by grants from the Natural Science Foundation of Liaoning province, China (No. 2023-MS-354), and the Science and Technology Project for Youth of Chaoyang Central hospital, Liaoning province, China.