
Abstract
Study Design:
Retrospective cohort study.
Objective:
To examine the risk of undergoing another cervical spine surgery after single-level posterior cervical foraminotomy (PCF) and analyze the costs of such reoperations.
Methods:
Using the PearlDiver database, we created database algorithms to identify cohorts of patients who underwent single-level PCF and also had various reoperations of interest, within 1, 2, and 4 years of follow-up. We also identified the per-patient average charge (PPAC) for each reoperation cohort.
Results:
In the Medicare cohort, the incidence of any reoperation was 8.3%, 9.8%, and 10.5% within 1, 2, and 4 years of follow-up, respectively. The PPAC was $8520 for the initial PCF procedure. When a second cervical surgery was performed, the PPAC was $70 349 for anterior fusion, $15 760 for posterior decompression alone, and $77 976 for posterior decompression and fusion. In the UnitedHealth cohort, the incidence of any reoperation was 13.6%, 16.7%, and 17.0% within 1, 2, and 4 years of follow-up, respectively.
Conclusions:
The overall incidence of another cervical spine operation was slightly higher in the Medicare population to that in previous literature, but much higher in the UnitedHealth population. The most common reoperation after PCF varied between the Medicare and UnitedHealth datasets, and costs varied widely based on the procedure performed. This study provides pertinent information that surgeons can use to discuss the risk of reoperation with their patients.
Keywords
Introduction
Cervical radiculopathy is a common symptom of degenerative cervical disease or lateral disk herniations. It has a wide range of treatment options, including observation, physical therapy, targeted injection, and surgical decompression. When conservative management options fail, patients will most commonly undergo anterior cervical discectomy and fusion (ACDF). 1 –3 Recently, more attention has been drawn to nonfusion methods of alleviating cervical radiculopathy in the hopes of avoiding consequences of anterior cervical fusion such as decreased range of motion or adjacent segment disease. Therefore, patients and surgeons may opt for posterior cervical foraminotomy (PCF), a common decompression procedure with reported advantages over fusion, including lower cost, preserved spine kinematics, no risk of damage to anterior neck structures, and decreased adjacent segment disease. 3 –9
PCF has demonstrated high success rates and may produce similar outcomes to ACDF, but if symptoms recur or fail to improve, patients may need to undergo another surgery. 10 –15 While recent literature has suggested that the rate of revision surgery after ACDF and PCF is similar, 15 –18 the majority of the data comes from retrospective cohort studies from a limited number of surgeons, and thus may not represent the results seen more generally in practice. In the present study, we aimed to examine the reoperation rate after single-level PCF as reported in a national database and to identify the per-patient average charge (PPAC) associated with each reoperation cohort. To the best of our knowledge, no previous study has looked at a cohort of such size for 4 years after undergoing PCF.
Methods
This retrospective cohort study was deemed exempt from institutional review board review as all patient information was de-identified and we did not receive individual patient information. We used the PearlDiver patient records database (PearlDiver Inc, Warsaw, IN), a national database made up of 2 independent sets of insurance billing records. The first dataset is based on Medicare patients, made up of roughly 45 million patients each year, and their billing records between 2005 and 2012. The second set is from private payer insurance companies, with the biggest input from UnitedHealth Group (UnitedHealth, Minnetonka, MN), with roughly 20 million patients each year from 2007 to 2011. As a whole, PearlDiver is made up of standard analytical files of accrued patient data from 2 datasets over various years as defined by the creators of the database. PearlDiver data includes details such as patient gender, age range, region in the United States, length of stay, and total average charges. Using these datasets, we queried Current Procedural Terminology (CPT) and International Classification of Diseases, ninth edition (ICD-9) procedure codes to identify patients who underwent procedures of interest.
Using coding commands, each dataset was queried for patients who underwent single-level PCF and whose data was in the database for 1, 2, or 4 years, while excluding those who underwent multiple-level cervical foraminotomy (Table 1). Inherently, we would then expect fewer patients with 4-year follow-up, as these patients would only be included if they had been in the database from 2005 to 2008 for Medicare and in 2007 for UnitedHealth, allowing these patients to be followed for 4 years. Similarly, we expect more patients with 1 year of follow-up as they may have been in the Medicare dataset in 2005, 2006, 2007, 2008, 2009, 2010, or 2011 to be followed for 1 year. We then narrowed our search results by forming cohorts of patients who also underwent another reoperation, not on the same day as the PCF, but within 1, 2, and 4 years of the PCF. The reoperations shown in Table 1 are the only ones we included; modifiers were not included to assure that all patients undergoing PCF would be included in the study. As such, we are unable to discern between unilateral and bilateral PCF. We used the same data to analyze the PPAC of each reoperation cohort. The PPAC averages the total patient charges, including surgeons’ fees and hospital charges. The PPAC was not analyzed in the UnitedHealth dataset because the charges from this dataset may not accurately represent inpatient and outpatient charges. Data analysis was completed using Microsoft Excel (Microsoft, Seattle, WA) and SPSS statistical software (SPSS, Inc, Chicago, IL). We set the significance level at α = .05, and Fisher exact test and 2-tailed P values were used to compare data. Due to patient privacy and contractual agreements with PearlDiver Inc, we are unable to report data on cohorts with less than 11 patients.
Reoperations and Associated Billing Codes.
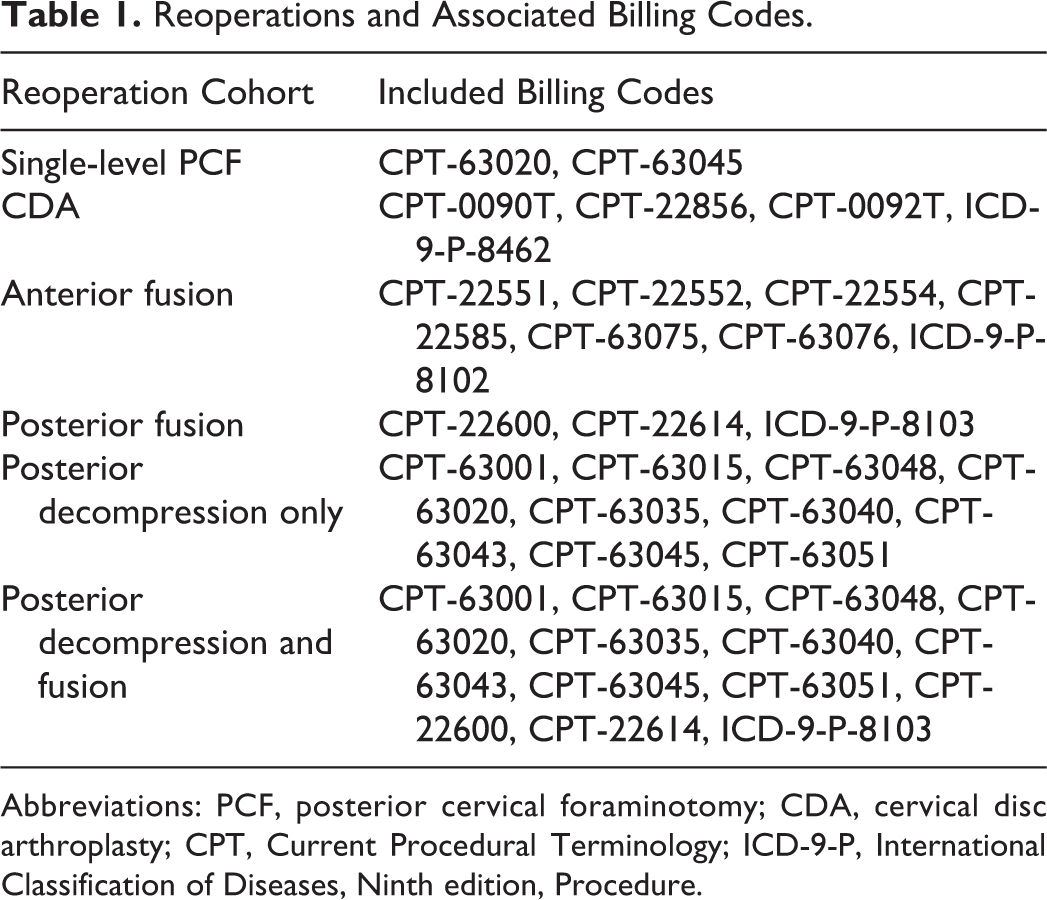
Abbreviations: PCF, posterior cervical foraminotomy; CDA, cervical disc arthroplasty; CPT, Current Procedural Terminology; ICD-9-P, International Classification of Diseases, Ninth edition, Procedure.
Results
Medicare Dataset
Between 2005 and 2012, 2905 patients underwent single-level PCF and had 1 year of follow-up, 2287 had 2 years of follow-up, and 1335 had 4 years of follow-up. Of those who underwent single-level PCF, 241 (8.3%), 225 (9.8%), and 140 (10.5%) had any reoperation within 1, 2, and 4 years, respectively (Figure 1a). Specific reoperations within 1, 2, and 4 years of PCF, respectively, were as follows: 130 (4.5%), 139 (6.1%), and 92 (6.9%) had an anterior fusion reoperation; 36 (1.2%), 42 (1.8%), and 28 (2.1%) had a posterior decompression; and 126 (4.3%), 98 (4.3%), and 57 (4.3%) had a posterior decompression and fusion (Table 2).
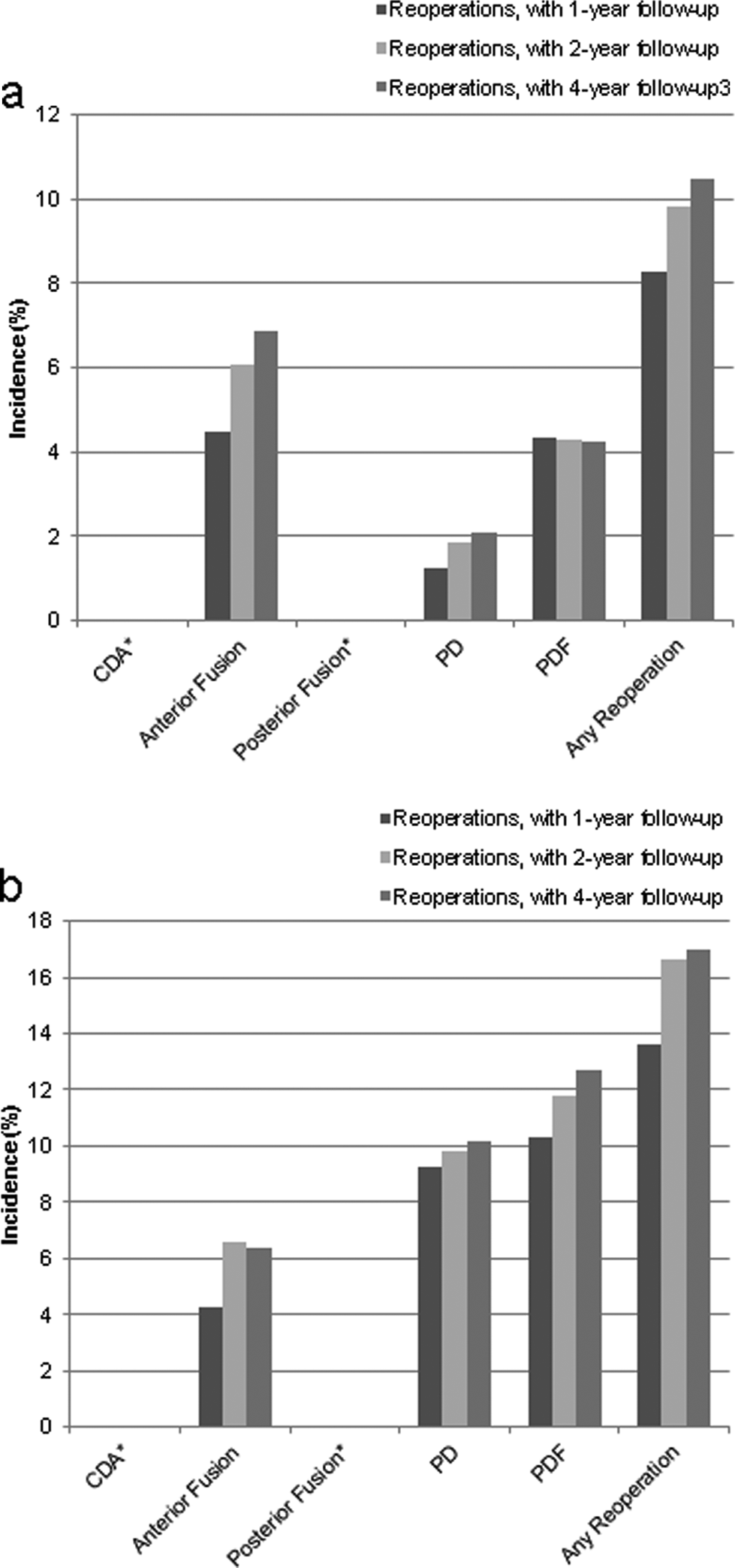
Incidence of reoperation after PCF in the (a) Medicare data set and (b) UnitedHealth data set.
Incidence of Reoperation in the Medicare Versus UnitedHealth Data Sets.
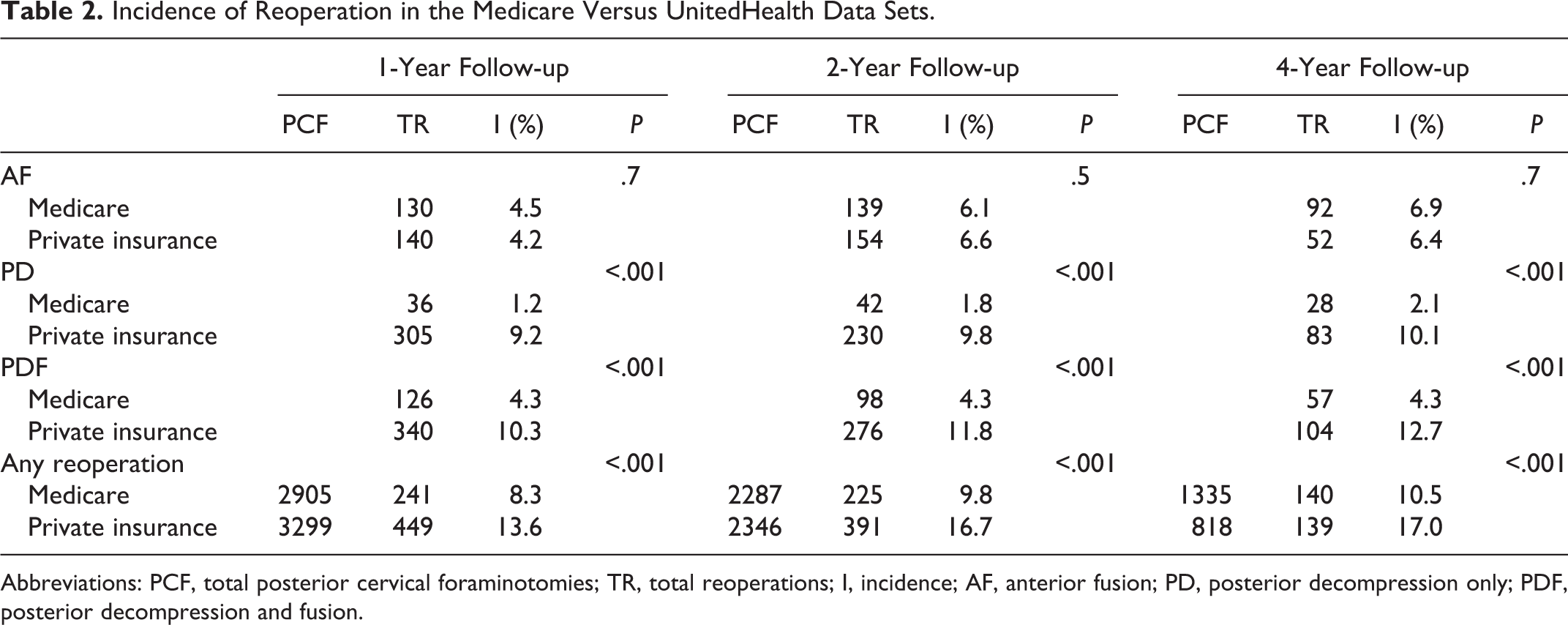
Abbreviations: PCF, total posterior cervical foraminotomies; TR, total reoperations; I, incidence; AF, anterior fusion; PD, posterior decompression only; PDF, posterior decompression and fusion.
Table 3 shows the demographics of PCF and risk of reoperation stratified by age, sex, and region. Within 2 years of PCF, 13.4% of those <65 years of age underwent a reoperation, versus 8.2% of those ≥65 years of age (P < .001). The difference in sex was not statistically significant, although the trend was toward a higher incidence of reoperation in females. The incidence of reoperation was highest in the Northeast at 1-year follow-up (12.5%, P = .004) and 2-year follow-up (13.5%, P = .03) follow-up, and highest in the West at 4-year follow-up (14.1%, P = .1).
Demographic Stratification of Reoperations in Medicare Dataset.
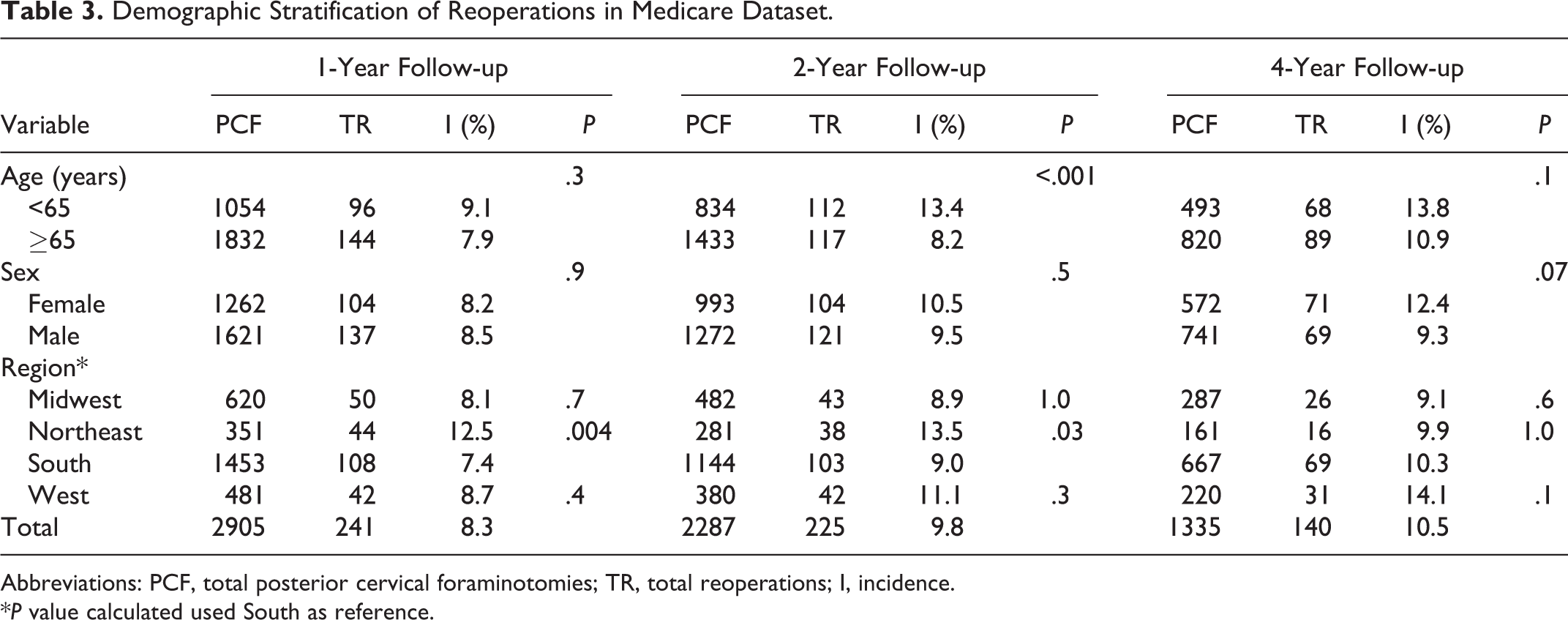
Abbreviations: PCF, total posterior cervical foraminotomies; TR, total reoperations; I, incidence.
*P value calculated used South as reference.
For the index procedure (PCF), the PPAC was $8520. The PPAC was $70 349 for the anterior fusion cohort, $15 760 for the posterior decompression alone cohort, and $77 976 for the posterior decompression and fusion cohort.
UnitedHealth Dataset
Between 2007 and 2011, 3299 patients underwent single-level PCF with 1 year of follow-up, 2346 with 2 years of follow-up, and 818 with 4 years of follow-up. Of those who underwent single-level PCF, 449 (13.6%), 391 (16.7%), and 139 (17.0%) had any reoperation within 1, 2, and 4 years, respectively (Figure 1b). Specific reoperations within 1, 2, and 4 years of PCF, respectively, were as follows: 140 (4.2%), 154 (6.6%), and 52 (6.4%) had an anterior fusion reoperation; 305 (9.2%), 230 (9.8%), and 83 (10.1%) had a posterior decompression; and 340 (10.3%), 276 (11.8%), and 104 (12.7%) had a posterior decompression and fusion (Table 2).
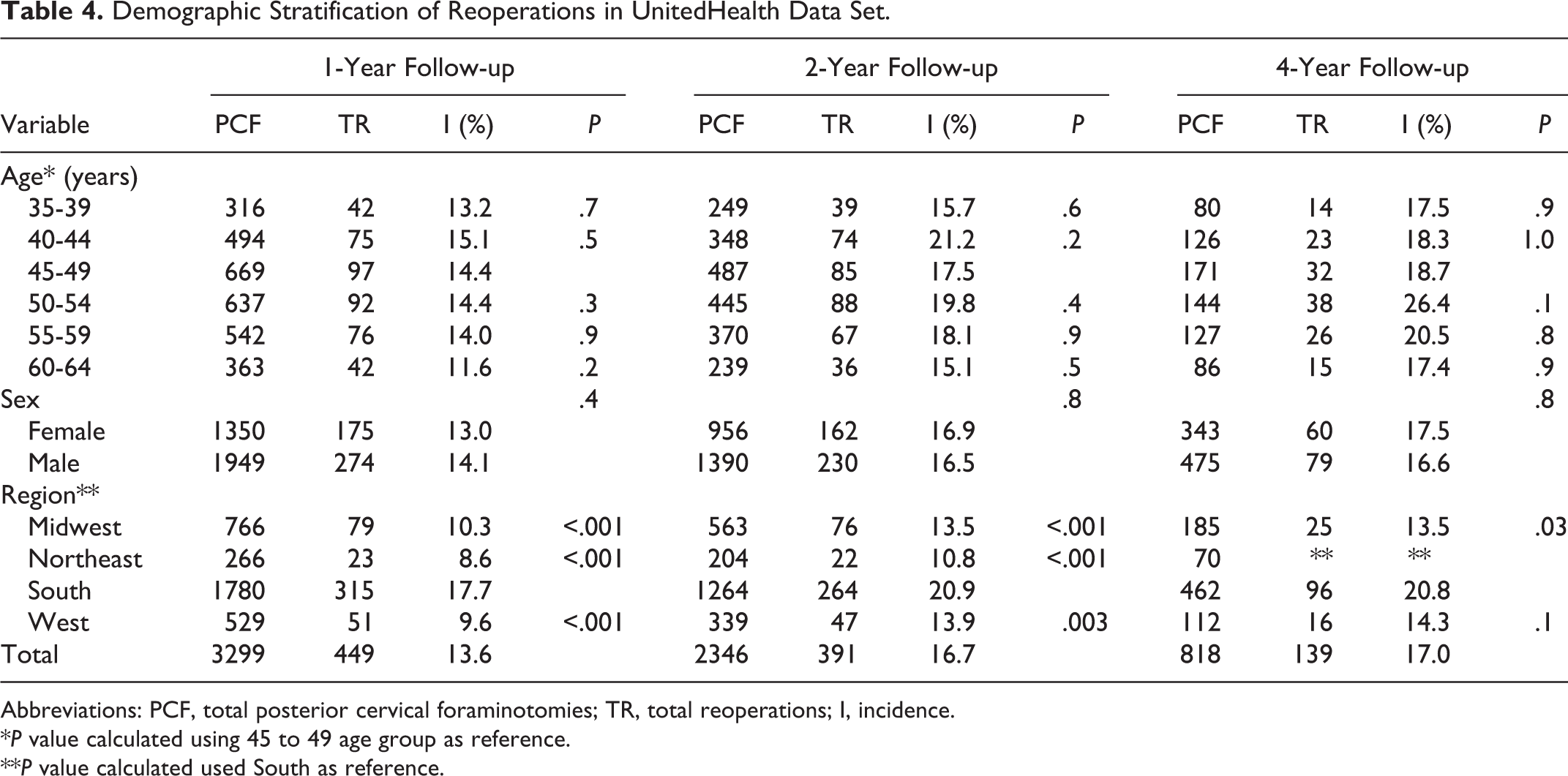
Table 4 shows the demographics of PCF and risk of reoperation stratified by age, sex, and region. Not all age groups are included as several included cohorts of less than 11 patients. The 45 to 49 age group had the most number of index procedures, although the incidence of reoperation was highest in the 40 to 44 group at 1 year (15.1%) and 2 years (21.2%), and in the 50 to 54 group at 4 years (26.4%). The incidence of reoperation was higher in females at 4-year follow-up (17.5% vs 16.6%, P = .8). The incidence of reoperation was highest in the South at 1-year follow-up (17.7%, P < .001), 2-year follow-up (20.9%, P < .05), and 4-year follow-up (20.8%, P = .03).
Demographic Stratification of Reoperations in UnitedHealth Data Set.
Abbreviations: PCF, total posterior cervical foraminotomies; TR, total reoperations; I, incidence.
*P value calculated using 45 to 49 age group as reference.
**P value calculated used South as reference.
Comparison of Medicare and UnitedHealth Datasets
The overall risk of reoperation was significantly higher in the UnitedHealth dataset than the Medicare dataset, at 1-, 2-, and 4-year follow-up (P < .001; Table 2). The difference between the 2 datasets was also significant when further analyzing the data (Table 2). There was a significantly higher rate of posterior decompression following PCF in the UnitedHealth dataset compared to the Medicare dataset, at 1-, 2-, and 4-year follow-up (P < .001). There was also a significantly higher rate of posterior decompression and fusion following PCF in the UnitedHealth dataset compared to the Medicare dataset, at 1-, 2-, and 4-year follow-up (P < .001). However, there was no significant difference between the 2 datasets in the incidence of anterior fusion after PCF (P = .7, P = .5, P = .7, at 1, 2, and 4 years of follow-up, respectively).
In both datasets, after PCF, less than 11 patients underwent cervical disc arthroplasty or posterior fusion alone, and due to contractual limitations detailed above, the data is not reported here.
Discussion
Previous literature has shown promising results after PCF and that patients can expect relief of radiculopathy. 10 –16 However, patients may eventually need a second surgery. In our study, the overall risk of reoperation after single-level PCF in the Medicare dataset was 8.3%, 9.8%, and 10.5% within 1, 2, and 4 years of follow-up, respectively. This is comparable to a study by Bydon et al, 16 which reported a 9.9% reoperation rate in 151 patients, occurring at an average of 2.4 years after PCF. In the same study, however, 80% of the patients underwent an ACDF as the reoperation, which is higher than both datasets in this study. Similarly, Davis 17 reported a 6% reoperation rate after PCF in 170 patients, all occurring at the same level, which is nearly half the rate found in our study. Wang et al 15 reported that 5% of 178 patients in their study underwent an ACDF after PCF, which is comparable to the rate of anterior fusion after PCF in the Medicare and UnitedHealth datasets.
It should be noted that all of the previous literature regarding cervical spine reoperation rates after PCF reported rates much lower than the UnitedHealth group in the current study. Furthermore, our results revealed the risk of reoperation after single-level PCF was significantly higher in the UnitedHealth dataset compared to Medicare (P < .001). This may be attributable to patients younger than 65 making up a majority of the UnitedHealth dataset, especially considering that younger patient age was reported by Wang et al 15 to be a risk factor for revision ACDF following PCF. Interestingly, the difference in total reoperation rates seems to be completely accounted for by an increased utilization of posterior cervical surgeries following the index PCF in the UnitedHealth group, while the rates of anterior fusion following PCF were similar in the 2 datasets. Overall, ACDF following PCF rates in the Medicare and UnitedHealth datasets were similar to what has already been reported in the literature, while posterior revision procedures were significantly higher in the UnitedHealth dataset. Thus, explaining why, while total revision rates were only slightly higher in the Medicare dataset compared to the previous literature, the UnitedHealth dataset had a much higher rate of reoperation.
When looking at the risk of reoperation after ACDF, studies have shown revision rates to be 4% to 8%. 8,15 In a randomized study of 72 patients, Wirth et al 9 found similar rates of revision surgery after ACDF versus PCF, although the numbers were quite high (24% reoperation rate after ACDF vs 27% after PCF). Using a propensity-matched analysis, Lubelski et al 18 reported the reoperation rates in 188 patients who underwent ACDF versus 140 who underwent PCF. Follow-up was 2 years, and there was no statistically significant difference in revision surgery between the 2 procedures (4.8% after ACDF vs 6.4% after PCF, P = .7). It should be noted that most previous studies reporting reoperation following PCF are from single-institution studies and/or major tertiary referral centers. The data obtained for this study is accumulated from a mix of academic and private practitioners with varying degrees of experience. Thus, the types of surgeries performed and rates of reoperation following PCF in these 2 bases may be more representative of the “average” spine practice in the United States. Despite the limitations of this study detailed below, this data can be helpful when counseling patients preoperatively.
Initially, it appears that there was a significant loss of follow-up in the 2 datasets—that only 46% of the patients had a 4-year follow-up in the Medicare dataset and 25% in the UnitedHealth dataset. As a retrospective cohort, however, only patients from 2005 to 2008 were selected to be followed for 4 years in the Medicare dataset because the data is only included through 2012. Similarly, 4-year follow-up in the UnitedHealth dataset was only selected in patients in 2007 because the dataset stops in 2011, and this would be the only way to assure 4 years of follow-up. Thus, it is expected to have more patients with 1-year follow-up than 4-year follow-up. It should also be noted that we are unable to comment on the rates of cervical disc arthroplasty or posterior fusion following PCF. Both cohorts had less than 11 patients in them and thus we cannot report absolute values due to restrictions of the database intended to protect patient privacy.
A paucity of studies exist examining the cost-effectiveness of PCF. 4 However, a systematic review in 2014 revealed that PCF was economically more beneficial than ACDF as the former was cheaper and led patients to return to work sooner. 4 The current study found the PPAC to Medicare for the initial PCF to be $8520. Another aspect of cost involves the durability of a surgery and costs associated with future treatments. We found that more than 10% of Medicare patients who underwent a single-level PCF would require at least one further cervical spine surgery within 4 years. The PPAC varied widely dependent on the type of surgery performed with posterior decompression and fusion being associated with the highest charges at $77 976, while posterior decompression alone was charged at $15 760. A limitation of using PPAC is that it may not accurately reflect the reimbursements or actual cost to the patient, which is generally a fraction of what is charged. 4 The use of spine implants and longer inpatient stays generally associated with fusion procedures naturally involve higher costs and likely attributed to the higher PPAC seen in patients undergoing fusion. 19
Our study has several limitations. The retrospective nature of the study introduces biases that are avoided in a prospective study. Furthermore, the ICD-9 and CPT codes merely describe the surgeries performed and do not tell us about the surgeon, or whether or not the “reoperation” was a true reoperation, or another cervical spine surgery at an adjacent region. However, previous studies have shown that reoperation within the first few years after PCF is mostly undergone at the same level. 16,17 Finally, in an aim to protect patient privacy, the database limits the data we receive, particularly when the patient population is below 11 patients, which precludes us from various statistical analyses that can control for potential confounding factors or provide insight on the reason behind reoperation after PCF. Nevertheless, PearlDiver has distinct advantages, allowing us to longitudinally follow patients, and its use in orthopedics has been extensively validated. 20 –22
Conclusions
The risk of reoperation after single-level PCF may be higher than previously reported. Furthermore, the risk of reoperation in the UnitedHealth dataset was significantly higher than the risk in the Medicare dataset, indicating that there are other factors that determine revision surgery after PCF. In addition, posterior cervical surgery following a PCF may be much more common than previously reported. Thus, the data from this study may be helpful to clinicians as it gives information regarding the expected rates of any further cervical surgeries following PCF. Further investigation is warranted to accurately determine the causes of reoperation following PCF, and the associated morbidities and cost.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Financial activities outside of the submitted work: Zorica Buser—Xenco Medical (consultancy), AO Spine (consultancy, past). Patrick C. Hsieh—Consulting: DePuy Synthes Spine, Medtronic; Speaking and/or Teaching Arrangements: Siemens. Jeffrey C. Wang—Royalties: Aesculap, Biomet, Amedica, Seaspine, Synthes; Stock Ownership: Fziomed; Private Investments: Promethean Spine, Paradigm spine, Benevenue, NexGen, Vertiflex, electrocore, surgitech, expanding orthopaedics, osprey, bone biologics, curative biosciences, pearldiver; Board of Directors: North American Spine Society (nonfinancial, reimbursement for travel for board meetings, courses, etc.), North American Spine Foundation (nonfinancial), Cervical Spine Research Society (nonfinancial, reimbursement for travel for board meetings), AO Spine/AO Foundation (honorariums for board position); Fellowship Support: AO Foundation (spine fellowship funding paid to institution).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.