
Abstract
Study Design:
Retrospective multicenter case series.
Objective:
To assess the rate of perioperative vision loss following cervical spinal surgery.
Methods:
Medical records for 17 625 patients from 21 high-volume surgical centers from the AOSpine North America Clinical Research Network who received cervical spine surgery (levels from C2 to C7) between January 1, 2005, and December 31, 2011, inclusive, were reviewed to identify occurrences of vision loss following surgery.
Results:
Of the 17 625 patients in the registry, there were 13 946 patients assessed for the complication of blindness. There were 9591 cases that involved only anterior surgical approaches; the remaining 4355 cases were posterior and/or circumferential fusions. There were no cases of blindness or vision loss in the postoperative period reported during the sampling period.
Conclusions:
Perioperative vision loss following cervical spinal surgery is exceedingly rare.
Introduction
Perioperative vision loss is a known, albeit rare, complication of spinal surgery. Ischemic optic neuropathy (ION) and central retinal artery occlusion (CRAO) are the 2 most common causes of blindness following nonocular surgery. Perioperative visual loss after nonocular surgery is uncommon; a study looking at 5.6 million patients from the Nationwide Inpatient Sample (NIS) found rates of 8.64, 3.09, and 0.12 per 10 000 patients in those undergoing cardiac, spinal, or appendectomies, respectively. 1 Posterior ION (PION), a rare cause of blindness in the community, is nevertheless the most common cause of visual loss following spine procedures in the prone position (Figures 1 and 2). For spinal procedures, additional risk factors for perioperative visual loss have been reported by some to consist of prone position, obesity, male sex, use of Wilson frame, duration of case, volume of blood loss, anemia, use of large volumes of crystalloids, and intraoperative hypotension. 2 -6 Most studies have addressed the incidence of visual loss in thoracolumbar fusions as these cases tend to be long with higher blood loss compared to most cervical spine surgery. There are, however, a number of case reports documenting visual loss following cervical spine surgery. 7 -9 These have involved use of horseshoe-type headrests with potential for direct impaction of the globe or by inducing changes in periorbital perfusion through enhancement of periorbital edema. However, the incidence of vision loss during cervical spine surgery has not been studied formally in a systematic fashion. This study aims to address the prevalence of blindness following cervical spine surgery.
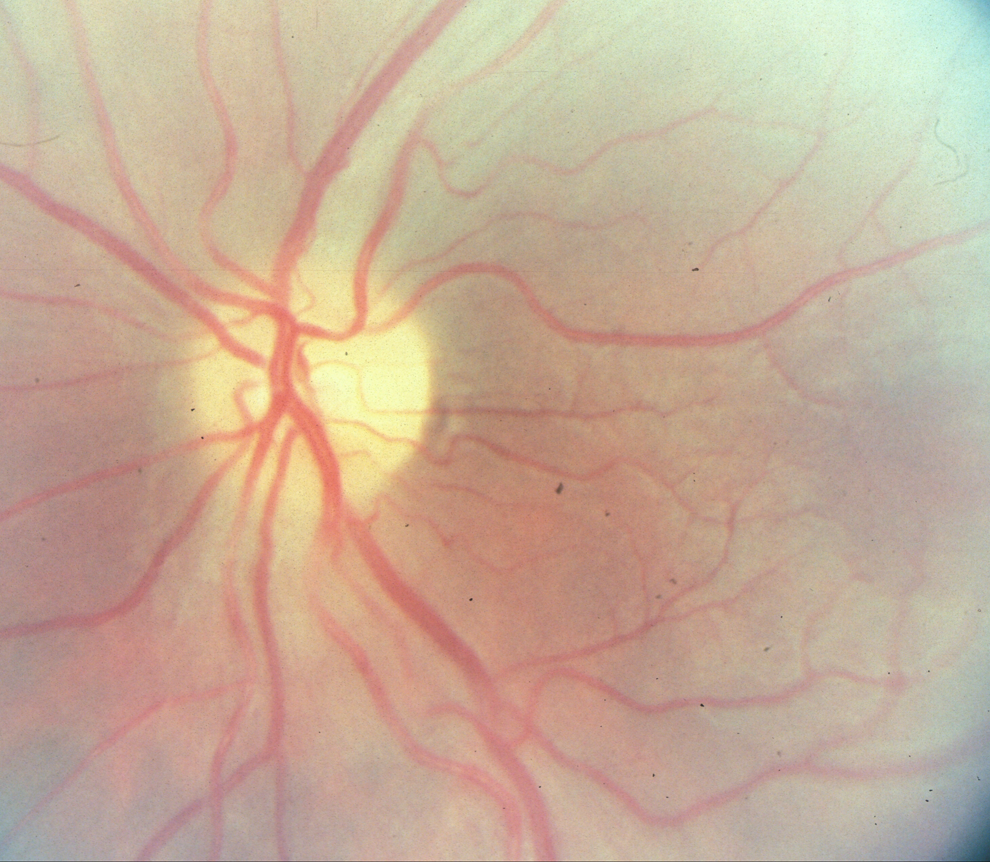
Fundoscopy showing normal optic nerve without evidence of posterior ischemic optic neuropathy.
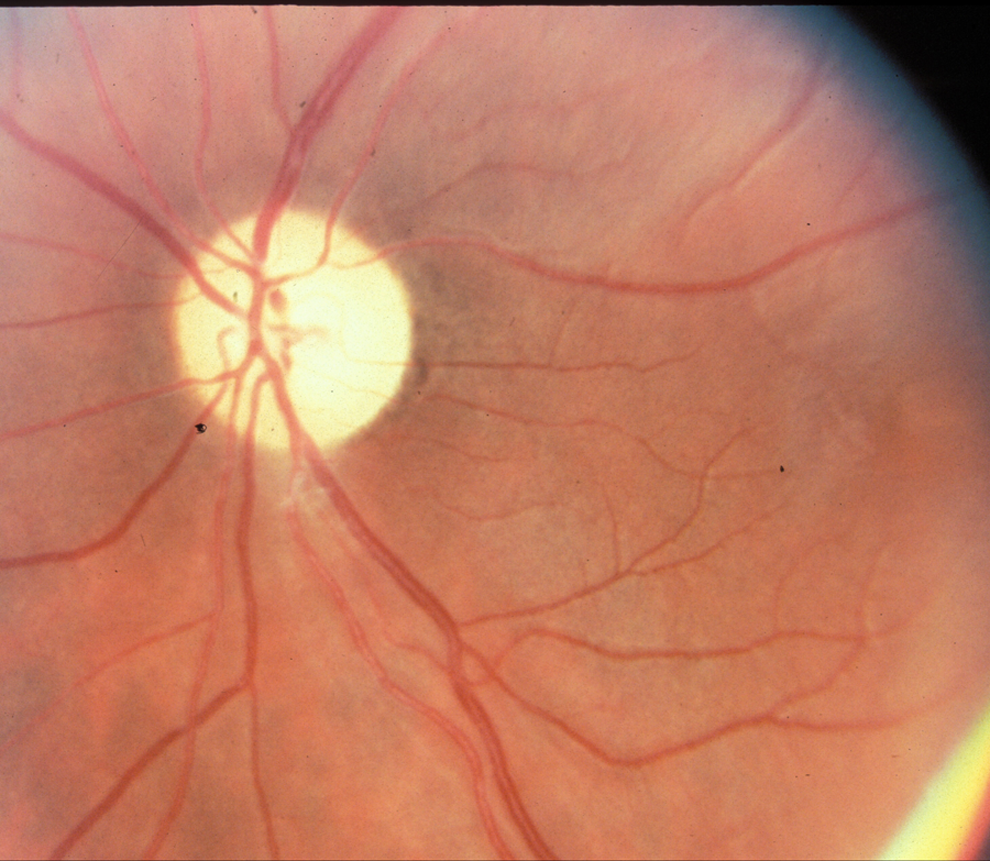
Fundoscopy showing evidence of posterior ischemic optic neuropathy.
Methods
We have conducted a retrospective multicenter case series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network, selected for their excellence in spine care and clinical research infrastructure and experience. Medical records for 17 625 patients who received cervical spine surgery (levels from C2 to C7) between January 1, 2005, and December 31, 2011, inclusive, were reviewed to identify occurrence of 21 predefined treatment complications. The complications included reintubation requiring hematoma evacuation, esophageal perforation, epidural hematoma, C5 palsy, recurrent laryngeal nerve palsy, superior laryngeal nerve palsy, hypoglossal or glossopharyngeal nerve palsy, dural tear, brachial plexopathy, blindness, graft extrusion, misplaced screws requiring reoperation, anterior cervical infection, carotid artery injury or cerebrovascular accident, vertebral artery injuries, Horner’s syndrome, thoracic duct injury, tetraplegia, intraoperative death, revision of arthroplasty, and pseudomeningocele. Trained research staff at each site abstracted the data from medical records, surgical charts, radiology imaging, narratives, and other source documents for the patients who experienced one or more of the complications from the list. Data was transcribed into study-specific paper case report forms. Copies of case report forms were transferred to the AOSpine North America Clinical Research Network Methodological Core for processing, cleaning, and data entry.
Descriptive statistics were provided for baseline patient characteristics. Paired t test was used to analyze changes in clinical outcomes at follow-up compared to preoperative status.
Results
Of the 17 625 patients in the registry, there were 13 946 patients assessed for the complication of blindness. There were 9591 cases that involved only anterior surgical approaches; the remaining 4355 cases were either posterior and/or circumferential fusions. There were no cases of blindness in the perioperative period reported during the sampling period.
Discussion
There are several large studies that have assessed risk factors for vision loss following spinal surgery (see Table 1). The study by Chang and Miller postulated that anemia, hypotension, long surgical duration, and significant intraoperative hydration were all risk factors for vision loss. 8 On multivariate analysis, another study found pediatric and elderly patients (>84 years) were at higher risk for vision loss; additionally, non-ION and non-CRAO visual loss risk factors included peripheral vascular disease (PVD), hypertension, and blood transfusion, whereas ION-related vision loss risk factors included hypotension, PVD, and anemia. 11
Review of Sentinel Studies Assessing Blindness as a Risk Factor Following Spinal Surgery.
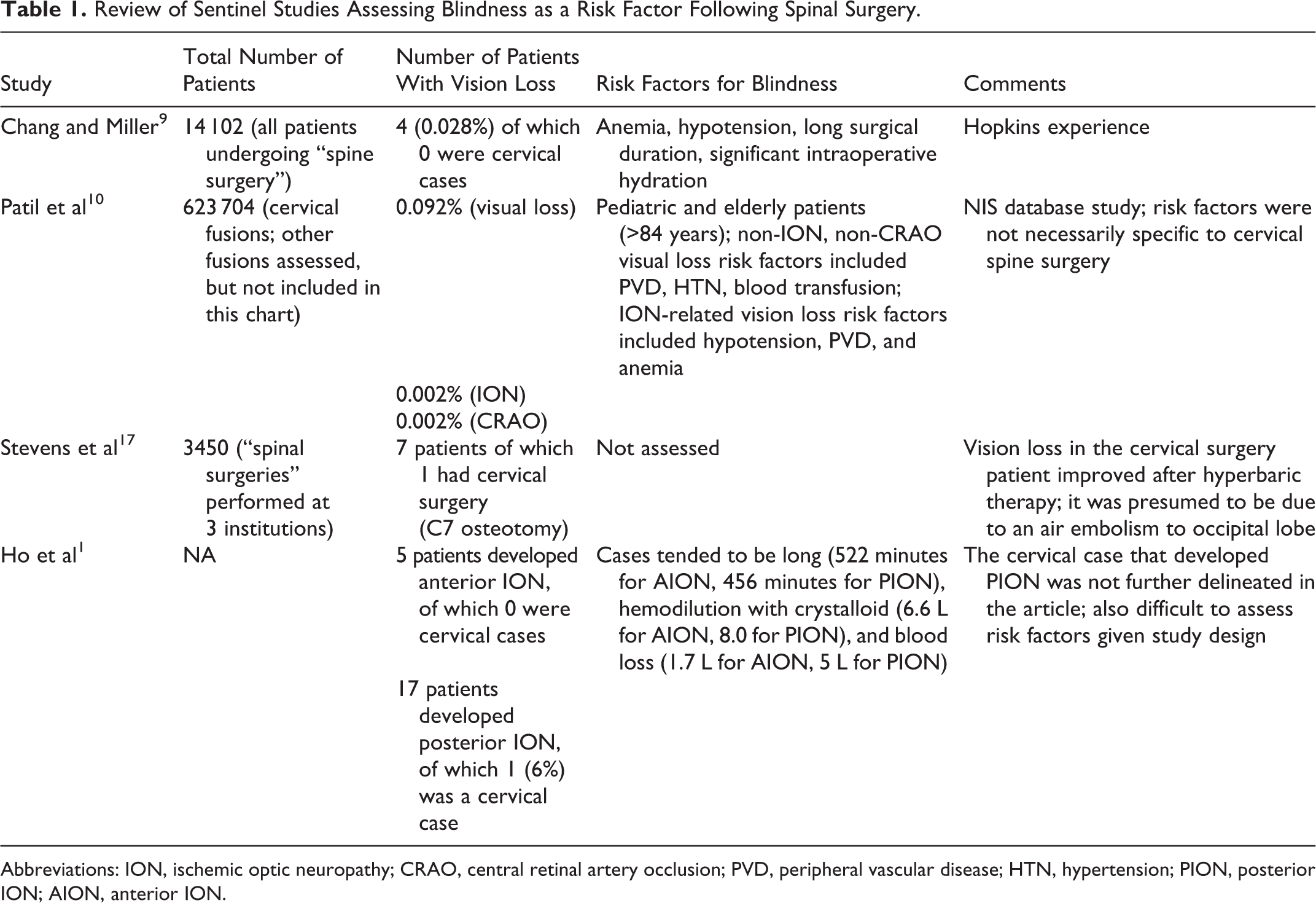
Abbreviations: ION, ischemic optic neuropathy; CRAO, central retinal artery occlusion; PVD, peripheral vascular disease; HTN, hypertension; PION, posterior ION; AION, anterior ION.
The main causes of perioperative visual loss, CRAO and posterior ION, are caused by different mechanisms. CRAO is generally caused by direct compression of the eye leading to an increase in ocular pressure with resultant ischemia. Although the optic nerve head is capable of autoregulation, available human studies suggest that this mechanism is not robust, and there is significant variation among healthy individuals. 12,13 Furthermore, autoregulation is likely lost when intraocular pressure exceeds a threshold value. 14 In contrast, in posterior ION, venous congestion likely plays a significant role resulting in ischemia, with change in blood pressure playing a more minor role. 3 -5
The largest study specifically assessing vision loss in patients undergoing cervical spinal surgery was done by Patil et al. 11 They assessed 623 704 patients in the NIS database who had undergone cervical spinal fusion. They found an incidence of 0.077% following cervical spine surgery compared to 0.28%, 0.14%, and 0.09% for scoliosis cases, posterior fusions, and anterior fusions, respectively. In addition, the incidence of ION was also lowest in the cervical spine patient cohort at 0.004%, compared to 0.02%, 0.017%, and 0.009% of scoliosis cases, posterior fusions, and anterior fusions. Not surprisingly, cervical spine patients had the lowest frequencies of anemia (1.1%), hypotension (0%), and transfusion (0.6%), all of which have been cited as risk factors for vision loss postoperatively.
Although the article by Patil et al is the largest series assessing vision loss after cervical spinal surgery, it has several limitations. As they pointed out, the duration of surgical intervention, and perhaps more importantly the permanence and severity of the vision loss, cannot be assessed by the NIS database. The extremely large number of patients assessed is a strength of the article, but the absence of more specific vision data makes drawing conclusions difficult. Although our article does not have as many patients, we were also able to show that the rate of vision loss after cervical spinal surgery is exceedingly low.
The Johns Hopkins experience published by Chang et al also assessed a large number of patients. 10 In their series of 14 102 patients, 4 patients developed vision loss postoperatively; none of these cases were related to cervical spine surgery. Although a large study, it is limited by the fact that patients were chosen based on having had “spine surgery.” Our study has a similar number of patients and was limited to cervical spinal cases only. Our study group, like the Hopkins group, has also found that the prevalence of vision loss following cervical spinal surgery approximates zero.
A review published by Ho et al divided vision loss into anterior or posterior ION. In their review of the literature, they found 5 patients who developed anterior ION, of which zero were cervical cases, and 17 patients who developed posterior ION, of which only one case was related to cervical spinal surgery. 2 Unfortunately, that case is not discussed in greater detail in their study. Regardless, similar to the studies by Patil and Chang, as well as our data, the incidence of vision loss following cervical spinal surgery appears to be exceedingly low.
There are a number of case reports that have documented vision loss after cervical spinal surgery. Many of these cases have blamed the vision loss on faulty positioning. Manfredini reported a case of prolonged compression of the eyeball during surgical fixation of a C5-C6 subluxation that resulted in blindness. 8 Abraham et al reported a case of unilateral vision loss presumed to be ION after fixation of an atlanto-axial dislocation in the prone position; they hypothesized that the patient’s vision loss could have been due to a combination of factors including malpositioned horseshoe head rest and surgery in the prone position. 7 Bekar also reported a case of CRAO as a result of cervical spine surgery in the prone position using a horseshoe head holder; they believed that prolonged ocular pressure caused the arterial occlusion. 9 In a case by Kasodekar et al, a patient underwent a C3-C6 laminectomy and was positioned prone on a horseshoe head holder. Postoperatively the patient had painless vision loss and was found to have CRAO on fundoscopy. The etiology was unclear in this case, but believed to be due to a hypercoagulable state from a carcinoma of the mandible. 17 Overall, these case reports provide little specific evidence beyond mere association that vision loss is a specific risk factor in patients undergoing cervical spinal fusion and that prone position on a horseshoe head holder may be a contributing factor. 7 –9,15 –17
One limitation of this paper is that only blindness was assessed. Patients who suffered from other forms of partial vision loss (ie, anopsias, decreased visual acuities, etc) were not included in the analysis. It has been shown that perioperative vision loss can, in fact, be partial. 1,2 –4 Patients with partial vision loss may have been missed in our analysis. However, given that blindness represents the most extreme form of vision loss, it is also reassuring that there were no cases recorded in our series.
Although rare, vision loss following spinal surgery is a potentially devastating event. Some studies have shown that visual acuity can return to baseline levels, but this seems to be the exception rather than the rule. Our study specifically assessed the risk of vision loss following cervical spinal surgery through our analysis of 13 946 patients. This, combined with a literature review of large series, has shown the risk of vision loss after cervical spinal surgery to be statistically negligible. Regardless of this exceedingly low risk, care should still be taken to avoid the known risk factors associated with blindness in other types of spinal surgery. This includes placing the head of the patient at or above heart level if at all possible. It is also not desirable to place the patients’ face in a dependent fashion on a hardened structure such as the padded bar of a horseshoe headrest. Unfortunately, our database was unable to assess the type of head holder used, and whether this has any bearing on the rate of vision loss. In terms of volume replacement, larger volume resuscitation over a longer period of time may increase periorbital edema and decrease perfusion pressure of the optic nerve.
Finally, in light of the major impact that blindness has on affected patients, surgeons may consider including a discussion of a theoretical risk of perioperative vision loss in their consenting process. While the data in the current registry is quite reassuring, the presence of past reports of blindness underscores the theoretical potential for its occurrence from a variety of etiologies beyond optic neuropathies, such as stroke. Therefore, and in light of its impact on patient quality of life, a discussion of risks surrounding cervical spine surgery should also include a discussion of perioperative blindness as rare, but potentially high impact complication.
Footnotes
Authors’ Note
This study was ethically approved by the Institutional Ethics Committees (IEC) at all participating sites.
Acknowledgements
For use of fundoscopic images showing PION: Neil R. Miller, MD, Professor of Ophthalmology, Neurology, and Neurosurgery, Wilmer Eye Institute, Johns Hopkins Hospital.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brandon C. Gabel reports grants from AOSpine North America during the conduct of the study; Jens Chapman reports grants from AOSpine North America during the conduct of the study; Rod J. Oskouian Jr reports grants from AOSNA during the conduct of the study; Ahmad Nassr reports grants from AOSNA during the conduct of the study; Bradford L. Currier reports grants from AOSpine North America during the conduct of the study, personal fees from DePuy Spine, personal fees from Stryker Spine, personal fees from Zimmer Spine, other from Zimmer Spine, other from Tenex, other from Spinology, other from LSRS, other from AOSNA, outside the submitted work; Arjun S. Sebastian reports grants from AOSpine North America during the conduct of the study; Steven R. Hamilton reports grants from AOSpine North America during the conduct of the study; Michael G. Fehlings reports grants from AOSpine North America during the conduct of the study; Thomas E. Mroz reports other from AOSpine, grants from AOSNA during the conduct of the study, personal fees from Stryker, personal fees from Ceramtec, other from Pearl Diver, outside the submitted work; and K. Daniel Riew reports personal fees from AOSpine International, other from Global Spine Journal, other from Spine Journal, other from Neurosurgery, personal fees from Multiple Entities for defense, plantiff, grants from AOSpine, grants from Cerapedics, grants from Medtronic, personal fees from AOSpine, personal fees from NASS, personal fees from Biomet, personal fees from Medtronic, nonfinancial support from Broadwater, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AOSpine North America Inc, a 501(c)3 nonprofit corporation.