
Abstract
Emotion-regulation difficulties are implicated as a risk factor for suicidal thoughts, yet little is known about how adults with suicidal thoughts regulate emotions in daily life or which deficits are specific to suicidality versus shared across psychopathology. In two ecological-momentary-assessment studies (Study 1: N = 396; Study 2, recruited online: N = 195), we compared adults with current suicidal thoughts with adults with past or no suicidal history (Study 1) and with psychiatric and healthy control participants (Study 2). Participants with current (vs. past) suicidal thoughts reported greater substance use and self-injury to regulate emotions (Study 1). Compared with psychiatric control participants, participants with suicidal thoughts reported higher regulatory effort and substance use, and compared with healthy control participants, they additionally reported greater distraction and rumination and lower regulatory success (Study 2). Self-injury and substance use uniquely predicted momentary suicidal thinking (Study 2). Findings highlight substance use, self-injury, and heightened regulatory effort as potentially distinct emotion-regulation processes associated with suicidal thoughts.
Keywords
Suicide is a leading cause of death, claming the lives of more than 700,000 people in 2019 (World Health Organization [WHO], 2021). Suicidal behaviors are typically preceded by suicidal thoughts, with approximately 30% of people who think about suicide who go on to attempt suicide (Nock et al., 2008). Emotion-regulation difficulties are highlighted as a risk factor for suicidal thoughts (Colmenero-Navarrete et al., 2022; Raudales et al., 2020). Specifically, theories of suicide suggest that feeling hopeless about one’s ability to control distressing mental states plays a key role in the development of suicidal thinking (Baumeister, 1990; Beck et al., 1975). Because emotion regulation involves an attempt to control emotional distress (Gross, 2015), hopelessness about one’s ability to regulate emotions may heighten the risk of suicidal thoughts (Miranda et al., 2013). Consistent with this idea, previous research has found that approximately 95% of individuals who experience suicidal thoughts regard the desire to escape negative emotions as a primary reason for contemplating suicide (May et al., 2020; May & Klonsky, 2013). Therefore, in some cases, suicidal thoughts might reflect a perceived inability to regulate emotions using any other means but ending one’s life. This highlights the critical role of emotion regulation in understanding suicidal thoughts. Accordingly, there is accumulating evidence for relationships between suicidal thoughts and emotion-regulation difficulties, especially in selecting emotion-regulation strategies (for a meta-analysis, see Rogier et al., 2024).
Suicidal thoughts were associated with reports of heightened use of strategies that are typically considered maladaptive in the long-term, such as rumination, which involves repetitively thinking about causes and consequences of negative emotional experiences (Rogers et al., 2022). Suicidal thoughts were also associated with avoidance from emotional-eliciting situations and with expressive suppression, which involves concealing the outward expression of emotion (Rogier et al., 2024; Ye et al., 2024). With respect to strategies that are typically considered more adaptive in the long-term, suicidal thoughts were associated with reduced use of problem solving (i.e., situation modification) and with reduced use of cognitive reappraisal, which involves reinterpreting the emotional-eliciting situation (Franz et al., 2021; Jenkins et al., 2025; Ong & Thompson, 2019; Rogier et al., 2024). Other studies, using the Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004), have found evidence for concurrent and prospective relationships between reported emotion dysregulation and suicidal thoughts over 6-month and 2- to 3-year follow-up periods (Hatkevich et al., 2019; Miranda et al., 2013; Raudales et al., 2020). Still, research on emotion regulation and suicidal thoughts is constrained by several limitations.
First, there is a need for more theoretically guided and systematic research that differentiates and targets multiple stages of emotion regulation. Emotion regulation is a multistage process, activated by the goal to change the intensity, duration, or quality of emotions through the implementation of emotion-regulation strategies (Gross, 2015; Sheppes et al., 2015). It contributes to better professional, social, and emotional well-being by helping people align their emotional reactions with their personal goals and values (English et al., 2012; Martín-Brufau et al., 2020). The first stage of regulation involves identifying the need to regulate and attempting to change one’s emotional state in a desired direction (identification stage; Raugh & Strauss, 2022). In the second stage of regulation, people select which emotion-regulation strategies to use to attain their regulatory goal (selection stage; Matthews et al., 2021). Next, people implement the strategies they have selected (implementation stage; Shafir et al., 2015), which can involve varying degrees of perceived effort and regulatory success (Scheffel et al., 2021; Wylie et al., 2023). Finally, people monitor the ongoing regulatory process to determine whether they need to adjust the strategies they use or discontinue regulation (Dorman Ilan et al., 2019). Most of the evidence for the link between suicidal thoughts and emotion-regulation deficits has focused on the selection stage of regulation (i.e., use of strategies; see Rogier et al., 2024), far fewer studies have examined deficits in the implementation stage (Jenkins et al., 2025; Kudinova et al., 2016), and no studies that we are aware of have tested the identification or monitoring stages. Many other studies have focused on general deficits that could map onto several regulatory stages (e.g., items such as “When I’m upset, I believe there is nothing I can do to make myself feel better,” which could map onto the identification, selection, or implementation stage; Hatkevich et al., 2019; Miranda et al., 2013; Raudales et al., 2020). To gain a more accurate understanding of emotion regulation in suicidal populations, there is a need to differentiate between those stages and assess for deficits in each stage individually (Sheppes et al., 2015). We therefore focused on three stages of regulation. We assessed emotion-regulation attempts (identification stage), the use of eight emotion-regulation strategies (selection stage), and perceived regulatory success and effort (implementation stage). We also tested whether each emotion-regulation strategy is associated with momentary suicidal thoughts (Stanley et al., 2021).
Another primary limitation in current research on emotion regulation and suicidal thoughts is restricted ecological validity. The majority of studies on emotion regulation and suicidal thoughts have used questionnaires (Colmenero-Navarrete et al., 2022; Franz et al., 2021; Hatkevich et al., 2019; Morrison & O’Connor, 2008; Neacsiu et al., 2018; Pisani et al., 2013). These studies revealed associations between suicidal thoughts and reports of overall emotion dysregulation (Brausch et al., 2022; Rajappa et al., 2012; Raudales et al., 2020), higher trait rumination and expressive suppression (Morrison & O’Connor, 2008), or reduced use of cognitive reappraisal (Ong & Thompson, 2019). Although informative, recent findings question the relevance of global self-report questionnaires to the same processes in daily life (Koval et al., 2023). Specifically, Koval et al. (2023) investigated the relationship between global self-report measures and daily diary or experience-sampling measures completed by the same participants. They found only weak to moderate correlations between global self-reports and the average daily self-reports of emotion-regulation-strategy use (i.e., cognitive reappraisal, expressive suppression, and rumination). This led the authors to conclude that global questionnaires assessing emotion-regulation strategies may not strongly and uniquely predict individual differences in daily selection of these strategies (Koval et al., 2023). Indeed, global self-report measures of emotion regulation are primarily designed and validated to capture habitual or trait-level use of strategies, making them less suitable for evaluating state emotion regulation (Boemo et al., 2022; Medland et al., 2020). Although trait-level data provide a broad approximation of a person’s average or most typical emotion-regulation patterns, state-level data more accurately capture actual experiences in the moment and their within-persons variability (Blalock et al., 2016). Accordingly, there is a growing body of research testing emotion regulation in daily life, offering new insights into how people regulate emotions across different contexts (e.g., uncertainty; Moeck et al., 2024), the variability of strategy use (Blanke et al., 2020), and key predictors of regulatory processes (e.g., emotion differentiation; Kalokerinos et al., 2019). Consequently, it remains unclear whether questionnaire-based findings generalize to everyday emotion regulation among individuals with suicidal thoughts. Furthermore, because questionnaires typically assess emotion regulation retrospectively at a single time point, they are especially vulnerable to memory biases and provide a lower-resolution picture of emotion regulation (Chang et al., 2018).
A handful of studies used behavioral or neurological measures to assess emotion-regulation processes in the lab, focusing on the implementation stage of regulation. Miller et al. (2018), for example, used functional MRI (fMRI) to assess the ability of youths with and without a history of suicidal thoughts to decrease emotional reactions to negative images. They found no group differences in reported negative affect after regulation. However, youths with a history of suicidal thoughts had greater activity in the dorsolateral prefrontal cortex during regulation, which may reflect greater regulatory effort. An electroencephalogram study with a small sample of participants with a history of suicidal thoughts (N = 10) found reduced ability to implement cognitive reappraisal to decrease negative emotion as indicated by higher late positive potentials after regulation compared with participants with no suicidal thought history (Kudinova et al., 2016). Recently, an fMRI study that measured prefrontal activation during a cognitive-reappraisal task found that lower activation in the ventrolateral prefrontal cortex moderated the association between childhood trauma and current suicidal thoughts (Jenkins et al., 2025). These studies provide valuable information suggesting that people with suicidal thoughts may experience less success or more perceived effort when regulating emotions. At the same time, laboratory studies can also be limited in capturing emotion regulation in naturalistic settings (Shiffman et al., 2008). This is because laboratory studies typically involve artificial static stimuli as opposed to dynamic and personally relevant events (Heiy & Cheavens, 2014).
To our knowledge, no study thus far has compared reports of emotion regulation in daily life between adults with and without suicidal thoughts using naturalistic methods. In the current studies, we used participants’ smartphones to collect high-resolution data in their natural environment (ecological momentary assessment [EMA]). This type of data is obtained by measuring reports on emotion regulation multiple times per day over several days, enabling greater reliability and fine-grained information on state-level emotion regulation. EMA also reduces memory biases and maximizes ecological validity because it evaluates psychological processes in real-world contexts (Shiffman et al., 2008). Consequently, there is a growing acknowledgment of the benefits of using EMA to reveal the nature and dynamics of suicidal thoughts (Hallensleben et al., 2018; Sedano-Capdevila et al., 2021). EMA-based assessments have yielded new insights into the variability and proximal predictors of suicidal thoughts, highlighting their fluctuations over time and their contextual triggers (Hallensleben et al., 2018; Sedano-Capdevila et al., 2021). In this study, we aim to leverage the advantages of EMA to better understand the relationships between suicidal thoughts and reports on emotion regulation in real time.
Finally, an additional limitation pertains to the specificity of findings to suicidal populations. Suicidal thoughts are usually accompanied by a wide range of transdiagnostic psychiatric symptoms (Xu et al., 2023). Previous studies have typically compared people with either current or a history of suicidal thoughts to control participants that were not matched on psychiatric symptoms (Brausch et al., 2022; Decker et al., 2021; Khazem & Anestis, 2016; Miranda et al., 2013; Rajappa et al., 2012). These comparisons do not allow for distinguishing patterns of regulation that are unique to suicidal thoughts from patterns that characterize high levels of psychopathology regardless of suicidality. Furthermore, some studies have included participants with either current or past suicidal thoughts interchangeably (Khazem & Anestis, 2016; Kudinova et al., 2016), making it hard to distinguish between the acute stage of suicidal thinking and trait-like patterns of regulation that characterize people with past suicidal thoughts.
To pinpoint the emotion-regulation challenges that are specifically associated with the presence of suicidal thoughts, we used a two-study investigation with three comparison groups. In Study 1, we used a general-population sample and compared people with current suicidal thoughts, people with past suicidal thoughts, and people with no history of suicidal thoughts. In Study 2, we recruited people with current suicidal thoughts, people with comparable levels of psychiatric symptoms but no history of suicidal thoughts (i.e., psychiatric control participants), and people with low levels of symptoms and no history of suicidal thoughts (i.e., healthy control participants).
The goal of this investigation was mainly exploratory, designed to test associations between distinct stages of emotion regulation and suicidal thoughts while addressing limitations pertaining to low ecological validity and low specificity to suicidal populations. However, based on previous findings (see Jenkins et al., 2025; Kudinova et al., 2016; Miller et al., 2018; Rogier et al., 2024), we expected that people with current suicidal thoughts would experience difficulties in the selection stage of regulation such that they would report using strategies that are typically considered less adaptive to a greater extent (e.g., rumination, expressive suppression, self-injury, substance use) and strategies that are typically considered more adaptive to a lesser extent (e.g., cognitive reappraisal, situation modification). We also expected participants with current suicidal thoughts to experience difficulties in the implementation stage of regulation, which would manifest in less perceived success and greater perceived effort in regulating emotions. We had no a priori predictions with respect to the identification stage (i.e., regulation attempts).
Study 1
We used a general-population sample to compare people with current suicidal thoughts, people with past suicidal thoughts, and people with no history of suicidal thoughts. Participants completed a weeklong EMA period assessing their reports on emotion-regulation attempts and strategies and perceived regulation success.
Transparency and openness
Study 1 was not preregistered. Data, materials, and code are publicly available on the OSF at https://osf.io/f9hjd/. All study procedures were approved by the Harvard University-Area Institutional Review Board (No. 22-0128). We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Method
Data were collected as part of a larger research project (see Millgram et al., 2023). For a list of all measures, see the Supplemental Material available online.
Participants
The sample size was determined based on a power analysis described in Millgram et al., 2023 (see the Supplemental Material). To ensure that this sample was sufficient to detect group differences in emotion-regulation variables, we conducted a post hoc power analysis using the simr package in R (Green & MacLeod, 2016) with 100 simulations, α = .05, considering an average of 14 time points with negative emotion per participant. We estimated power to detect differences between three groups. The power analysis indicated that a sample of 396 participants would enable the detection of a small effect for between-groups differences, marginal R2 = .005 and conditional R2 = .18 with 88.0% power, 95% confidence interval [CI] = [79.98, 93.64]. Participants were 401 residents of the United States, ages 18 and above, recruited online through Prolific (Palan & Schitter, 2018). Prolific is an online research platform for participant recruitment. It includes a large pool of participants from diverse demographic backgrounds and includes tools to prescreen participants and monitor participant engagement. Prolific was shown to produce high-quality data, and it is widely used in psychological research (Douglas et al., 2023).
Out of the 401 participants who completed the study, one participant failed two attention checks in the baseline survey, and four participants failed more than 10% of attention checks embedded in each EMA survey (see preregistration for Millgram et al., 2023), resulting in a final sample of 396 participants. During the baseline survey, participants completed an online, self-report version of the Columbia–Suicide Severity Rating Scale (C-SSRS; Posner et al., 2008), which was used to determine their group status. Forty-three participants reported current suicidal thoughts during the past month, 129 participants reported past suicidal thoughts, and 224 participants reported no lifetime history of suicidal thoughts (for demographic and clinical characteristics, see Table 1; for a flowchart depicting participant-recruitment procedure, see Fig. 1). The gender identities in the sample were 205 female; 183 male; four genderqueer, nonbinary, or gender-fluid; one transgender; one unsure; and two who preferred not to say. The racial and ethnic identities in the sample were 298 White, 34 Black/African American, 28 Asian, 22 Hispanic/Latino, three Middle Eastern or North African, one Native American/American Indian, nine identified as “other,” and one who preferred not to say. Participants were paid $3.50 for a baseline survey with an additional $0.25 for each EMA survey and a $1 bonus for any day they completed more than four surveys. The maximum amount participants could earn was $21.
Demographics and Clinical Characteristics
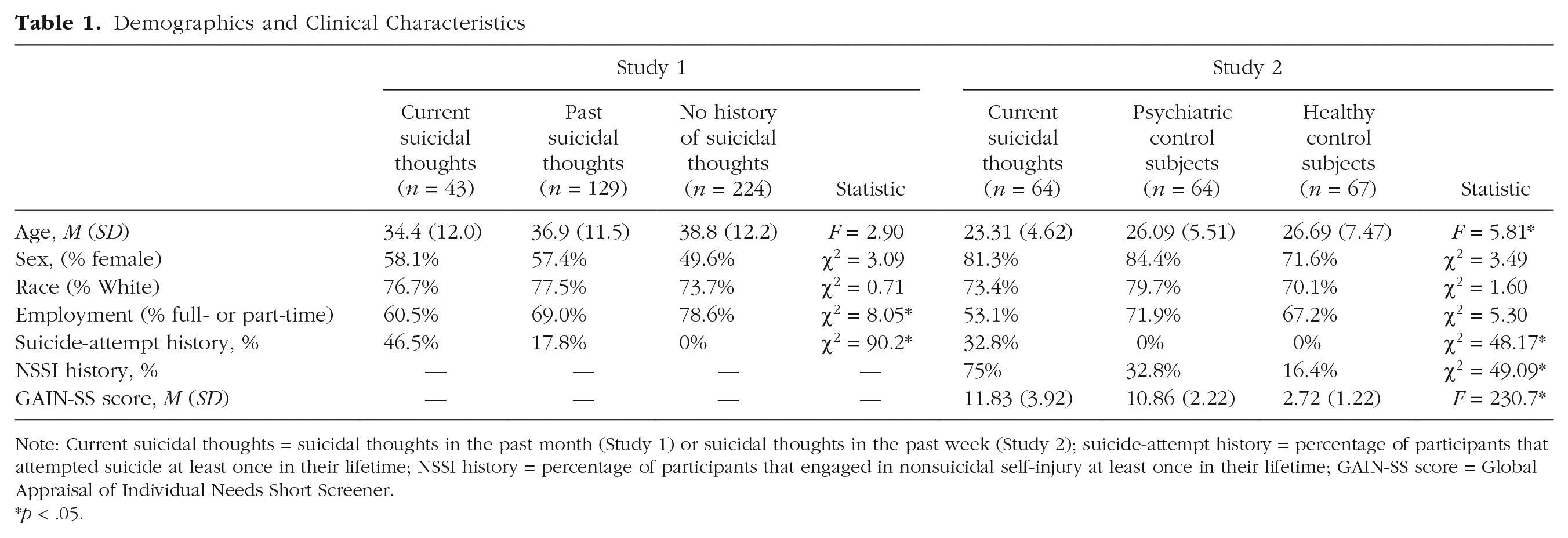
Note: Current suicidal thoughts = suicidal thoughts in the past month (Study 1) or suicidal thoughts in the past week (Study 2); suicide-attempt history = percentage of participants that attempted suicide at least once in their lifetime; NSSI history = percentage of participants that engaged in nonsuicidal self-injury at least once in their lifetime; GAIN-SS score = Global Appraisal of Individual Needs Short Screener.
p < .05.
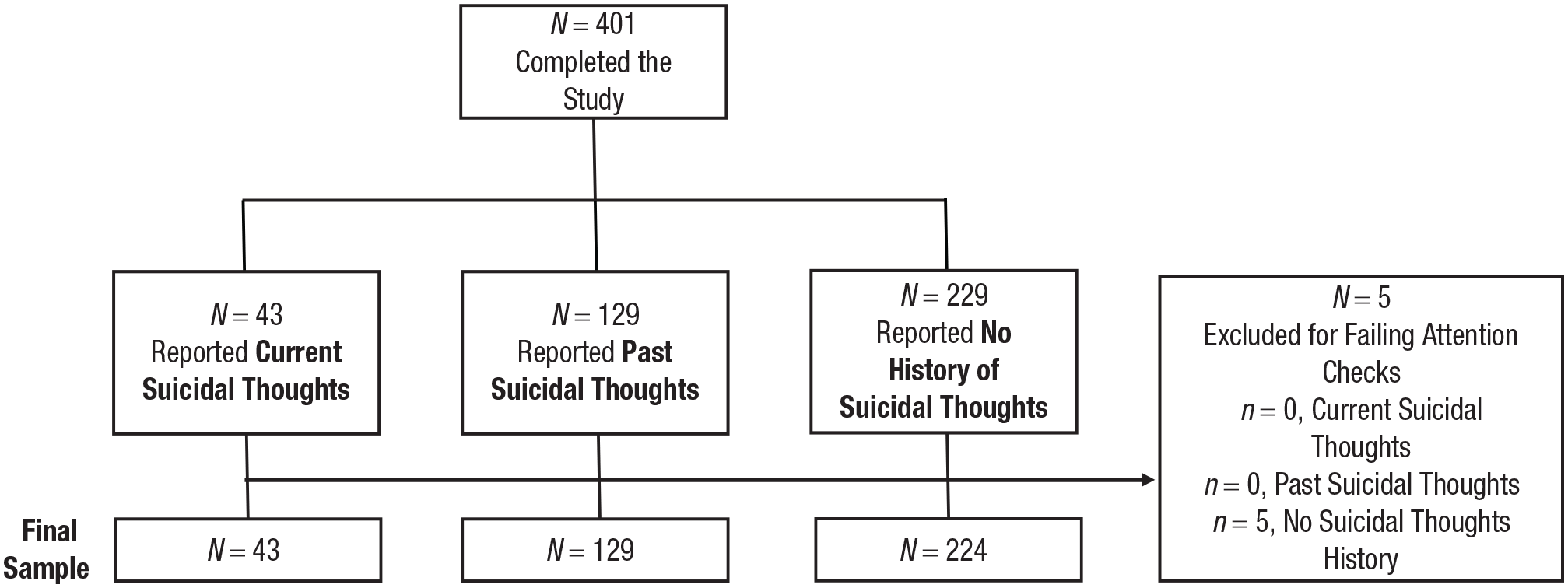
Flow diagram of the process of screening participants in Study 1.
Procedure
Study 1 included a baseline survey followed by a 7-day EMA period. For the EMA, participants downloaded a smartphone-based app (Metricwire). Following recommendations by Eisele et al. (2022), the app sent participants six surveys per day. Five surveys were sent at random times at least 90 min apart between 9 a.m. and 6:30 p.m. and stayed open for 1 hr. The last survey each day was sent at a random time between 8 p.m. and 9 p.m. and remained open for 6 hours.
Measures
Baseline survey
We used an electronic self-report version of the C-SSRS (risk-assessment version; Posner et al., 2008) to assess past-month and lifetime history of suicidal thoughts. The C-SSRS is an established and widely used measure (Mundt et al., 2013), and the electronic administration of the C-SSRS has demonstrated comparable psychometric properties and predictive validity (Greist et al., 2014; Gwaltney et al., 2017). For descriptives and psychometrics of the C-SSRS in the current sample, see the Supplemental Material.
EMA
At the beginning of each survey, participants reported on their negative emotions in the past hour (“In the past hour, how much did you experience negative emotions?”; 0 = not at all, 10 = extremely; for convergent validity, showing correlations between this measure and discrete negative emotions assessed at baseline, see the Supplemental Material). Next, participants reported on their emotion-regulation attempts (“In the past hour, how much did you
Analytic approach
We ran multilevel models (measurements nested within persons) using the lme4 package in R (Bates et al., 2015); p values were calculated using lmerTest (Kuznetsova et al., 2017). We included a random intercept for participants and random slopes for negative emotional reactivity. Following Barr et al. (2013), when models did not converge, we removed the random effect explaining the least variance. Continuous Level 1 predictors were person-mean centered, and continuous Level 2 predictors were grand-mean centered. Because of the exploratory nature of this investigation, we adjusted p values for multiple comparisons using false-discovery rate, applying Benjamini-Hochberg corrections (Benjamini & Hochberg, 1995; Thissen et al., 2002). We report both the original and the adjusted p values. Following Nakagawa and Schielzeth (2013), we calculated marginal R2 (R2M), which estimates the proportion of variance explained by the fixed effects, and conditional R2 (R2C), which estimates the proportion of variance explained by both fixed and random effects, using the MuMIn package in R (Barton, 2009). To ensure that any group differences were not driven by differences in participants’ initial emotional reactions rather than their regulation of these reactions, in all analyses, we controlled for negative emotions in the past hour (emotional reactivity; see also Raudales et al., 2020).
Results
The total number of completed surveys was 12,132. The average number of surveys completed per person was 35.05 (SD = 7.86; 83.5% compliance, Mdn = 90.5%). Groups did not differ in compliance, F(2, 393) = 0.65, p = .525 (82.9%, 83.4%, and 83.6% compliance for participants with current and past suicidal thoughts and no history of suicidal thoughts, respectively). We used all available data and report analyses with the original data. For missingness patterns and analyses with imputed data to account for missingness, see the Supplemental Material.
Identification stage: emotion-regulation attempts
We ran a multilevel regression model including only surveys when participants reported negative emotions in the past hour (nonzero responses; n = 5,466 surveys). Group (no suicidal-thoughts history, past suicidal thoughts, current suicidal thoughts) was entered as a Level 2 predictor, and regulation attempts were entered as the dependent variable. We controlled for emotional reactivity in the past hour. The random slope for emotion reactivity was removed because the model did not converge when including it. Participants with suicidal thoughts (M = 4.12, SD = 2.08) did not differ from participants with no suicidal-thought history in their regulation attempts (M = 4.20, SD = 1.82), b = −0.08, SE = 0.32, t(330.7) = −0.23, p = .816 (adjusted p = 9.79), R2M = .004, R2C = .39. They also did not differ from participants with past suicidal thoughts (M = 4.02, SD = 1.53), b = 0.10, SE = 0.34, t(324.9) = 0.30, p = .768 (adjusted p = 6.91), R2M = 0.004, R2C = 0.39. There was also no difference between participants with past suicidal thoughts and no history of suicidal thoughts, b = −0.18, SE = 0.22, t(337.3) = −0.80, p = .425 (adjusted p = 1.18), R2M = .004, R2C = .39.
Selection stage: emotion-regulation strategies
We repeated the previous analysis with each strategy as the dependent variable, including only surveys when participants indicated some level of regulation attempts (nonzero responses; n = 4,613 surveys). The models for rumination and expressive suppression included no random slope for emotional reactivity because these models did not converge when including it. For a summary of the results, see Table 2. Participants with current suicidal thoughts reported using more self-injury and substances (alcohol, drugs) to regulate emotions compared with the other two groups (see Fig. 1). Both participants with current and past suicidal thoughts reported using distraction and rumination to a greater extent compared with participants with no history of suicidal thoughts. Participants with current suicidal thoughts also reported using more expressive suppression compared with participants with no suicidal-thought history. Groups did not differ in their use of cognitive reappraisal, situation modification, social support, body relaxation, and emotional eating. For descriptives and zero-order correlations between emotion-regulation strategies, see Table S3 in the Supplemental Material.
Emotion-Regulation Strategies in Daily Life as a Function of Group (Study 1)
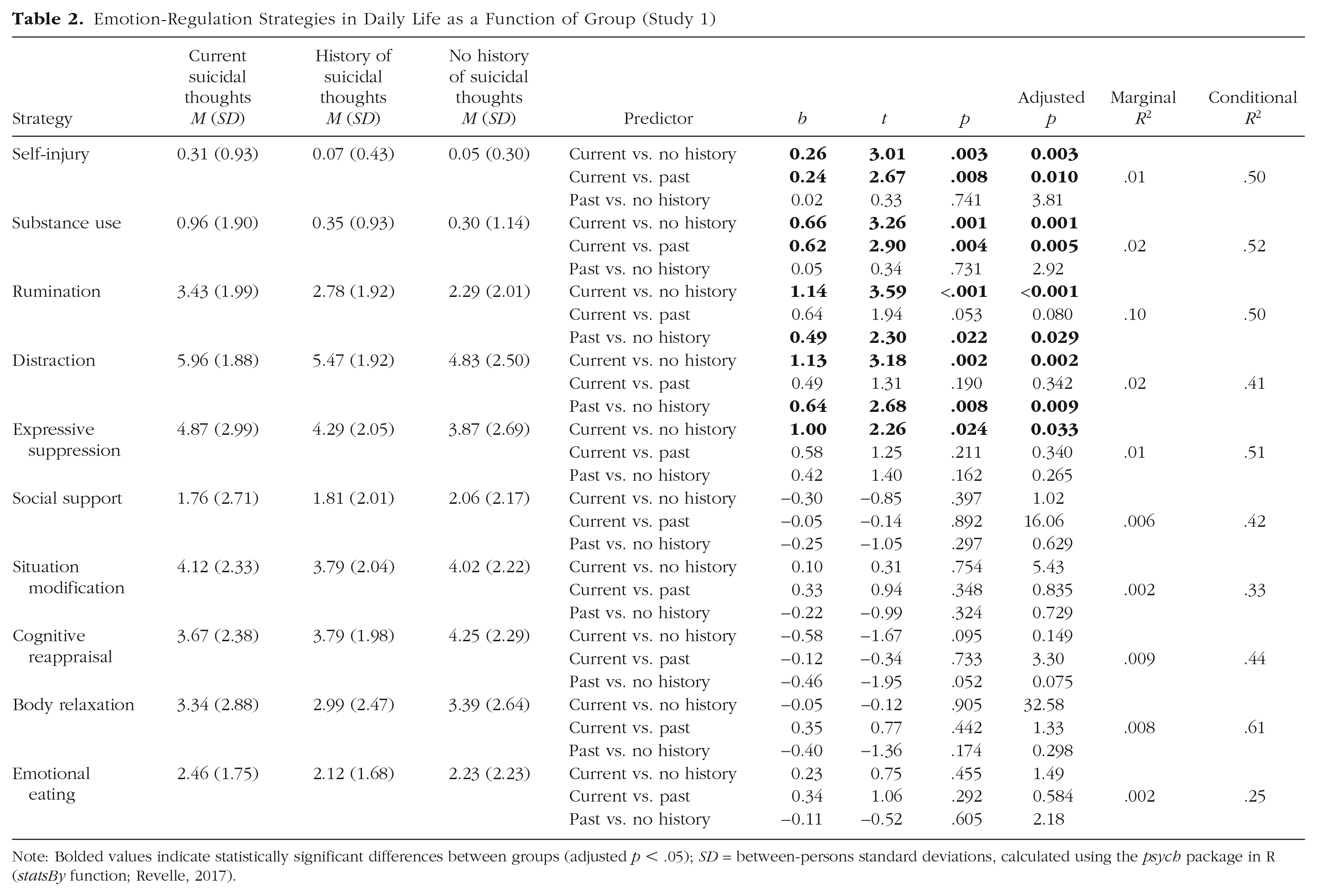
Note: Bolded values indicate statistically significant differences between groups (adjusted p < .05); SD = between-persons standard deviations, calculated using the psych package in R (statsBy function; Revelle, 2017).
Implementation stage: perceived emotion-regulation success
We repeated the previous analysis with perceived emotion-regulation success as the dependent variable. Participants with both current (M = 4.43, SD = 2.03) and past suicidal thoughts (M = 4.54, SD = 1.71) perceived themselves as less successful in regulation compared with participants with no history of suicidal thoughts: (M = 5.17, SD = 2.02), b = −0.74, SE = 0.31, t(317.6) = −2.38, p = .018 (adjusted p = 0.023), R2M = .07, R2C = .48 for current versus no suicidal thoughts and b = −0.63, SE = 0.21, t(312.4) = −3.02, p = .003 (adjusted p = 0.003), R2M = 0.07, R2C = 0.48 for past versus no suicidal thoughts. Participants with current suicidal thoughts did not differ from participants with past suicidal thoughts, b = −0.11, SE = 0.32, t(312.6) = −0.32, p = .746, (adjusted p = 4.48), R2M = .07, R2C = .48.
Study 2
In Study 2, we compared people with current suicidal thoughts with psychiatric control participants (i.e., participants matched on psychiatric symptoms) and healthy control participants. To broaden the focus on the implementation stage of regulation, we also assessed emotion-regulation effort (Miller et al., 2018). Finally, we tested whether each emotion-regulation strategy predicted momentary suicidal thinking.
Transparency and openness
Study 2 was not preregistered. Data, materials, and code are publicly available on OSF at https://osf.io/f9hjd/. All procedures were approved by the Harvard University-Area Institutional Review Board (No. 21-0422). We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Method
Data were collected online as part of a larger research project (see Millgram et al., 2025). For a list of all measures, see the Supplemental Material.
Participants
The sample size was determined based on a power analysis described in Millgram et al. (2025; see the Supplemental Material). To ensure this sample size was sufficient for detecting between-groups differences in emotion-regulation variables, we conducted a post hoc power analysis using the simr package in R (Green & MacLeod, 2016) with 100 simulations, α = .05, and considering an average of 14 time points with negative emotion per participant. We estimated power to detect a small effect size for differences between three groups (R2M = .008, R2C = .13). The analysis indicated that a sample of 195 participants (65 participants per group) would enable the detection of such effect with 82.0% power, 95% CI = [73.05, 88.97].
Participants were recruited based on their responses to a screening survey assessing their lifetime and past-week suicidal thoughts and a well-validated measure for past-year psychiatric symptoms (Global Appraisal of Individual Needs Short Screener [GAIN-SS]; Dennis et al., 2006). Participants rated the item “Have you ever seriously thought about killing yourself for longer than a few minutes?” (0 = no, 1 = yes). Next, participants rated the item “When was the last time you seriously thought about killing yourself?” (1 = in the past 7 days, 2 = 2 weeks ago, 3 = 4 weeks ago, 4 = 8 weeks ago [1–2 months ago], 5 = 12 weeks ago [2–3 months ago], 6 = 3–6 months ago, 7 = 6 months–1 year ago, 8 = more than 1 year ago). These types of items have been used in past research to measure active suicidal ideation (Millner et al., 2015).
Psychiatric symptoms were assessed using the GAIN-SS (α = .90 in the current sample; Dennis et al., 2006). Because suicidal thoughts are transdiagnostic (Caudle et al., 2024; Nock, Hwang, et al., 2009), we selected the GAIN-SS, which taps into four psychiatric-symptom dimensions, all of which were previously associated with suicidality (Giugovaz et al., 2024; Ilgen et al., 2010; Soto-Sanz et al., 2019). Specifically, the screener includes 20 items; five items comprise an internalizing-disorder subscreener (α = .88 in the current sample), five items comprise an externalizing-disorder subscreener (α = .78 in the current sample), five items comprise a substance-disorder subscreener (α = .86 in the current sample), and five items comprise a crime/violence subscreener (α = .66 in the current sample). Psychometric assessments of the GAIN-SS demonstrated high internal consistency (α = .96), excellent sensitivity (90% or more) for identifying the presence of a psychiatric disorder, and excellent specificity (92% or more) for correctly ruling out the presence of a psychiatric disorder (Dennis et al., 2006). It has been used in both clinical services and research (Bruffaerts et al., 2018; Conrad et al., 2012) and a variety of populations (primary care, criminal-justice system, homeless populations, college populations, and general-population samples; Mortier et al., 2015; Sacks, 2008; Shinn et al., 2007; Truman et al., 2011). The GAIN-SS has also been used in the past to assess mental health among people with suicidal thoughts and behaviors (Mortier et al., 2015, 2017).
For a flowchart depicting participants’ screening process, see Figure 2. The screening survey was distributed on Prolific (N = 1,747). Eligible participants were invited to the main study beginning the next day. Eligibility for the suicidal-thoughts group included seriously thinking about suicide during the past week (n = 137). Eligibility to the psychiatric-control group included reporting comparable levels of past-year psychiatric symptoms as the suicidal thoughts group (GAIN-SS≥7) but reporting no history of suicidal thoughts (n = 175). Eligibility for the healthy-control group included low symptom levels (GAIN-SS≤3) and no history of suicidal thoughts (n = 247). Out of the total 559 eligible participants who were invited to participate, 234 participants completed the main study. During the main study, suicidal thoughts were assessed again using the Self-Injurious Thoughts and Behaviors Interview (SITBI; Fox et al., 2020). To ensure the reliability of group assignments, we removed participants with inconsistent responding (Klimes-Dougan et al., 2022): 10 participants who were recruited to the suicidal-thoughts group but reported no past-week suicidal thoughts in the main study, six participants who were recruited to the psychiatric-control group but reported a history of suicidal thoughts in the main study, and five participants who were recruited to the healthy-control group but reported a history of suicidal thoughts in the main study. Eighteen additional participants were excluded for failing one or more of three attention checks embedded in the EMA surveys on Days 3, 5, and 7. Results remained identical when including these participants in the analyses (for details, see the Supplemental Material).
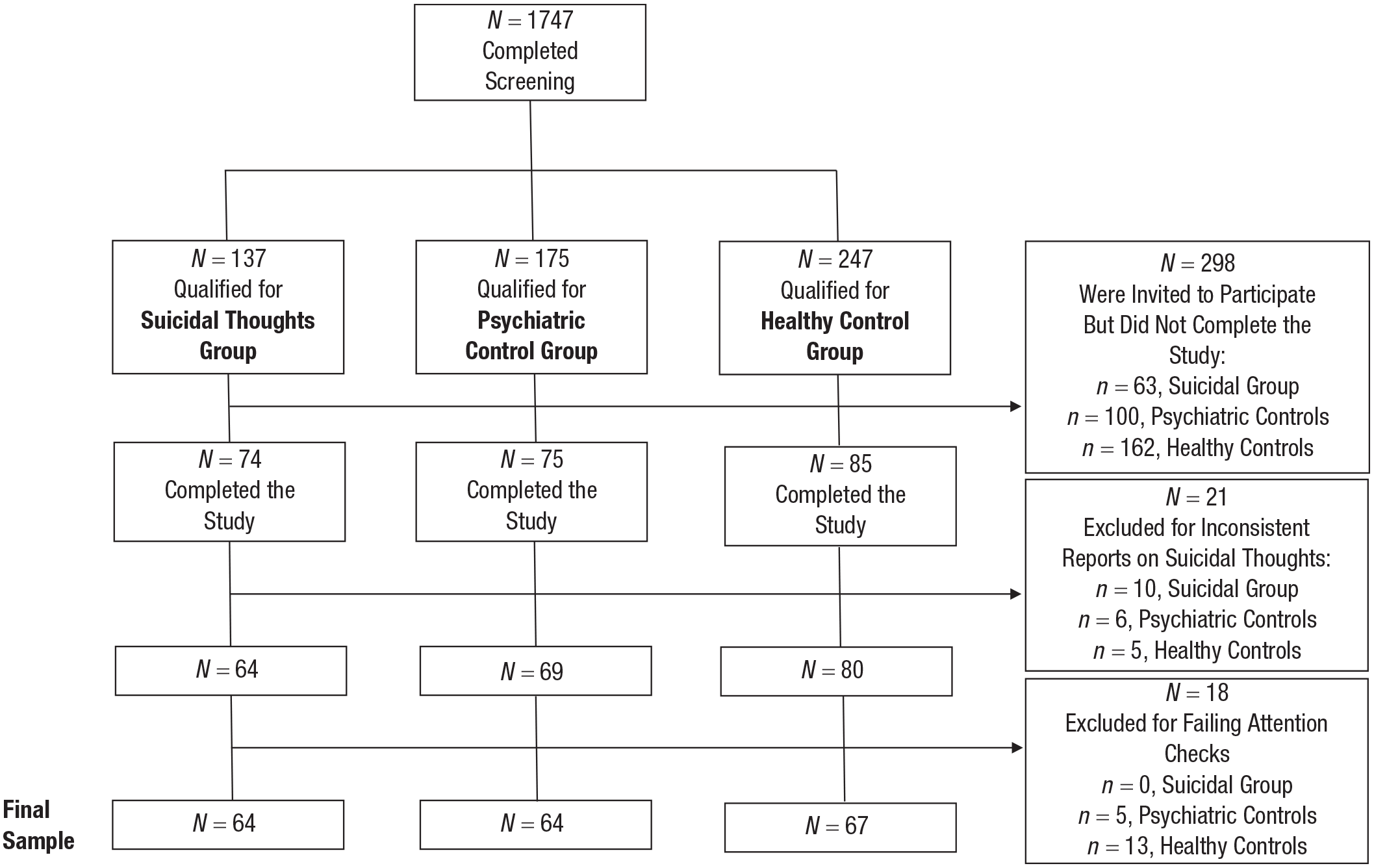
Flow diagram of the process of screening participants in Study 2.
The final sample included 195 participants. Sixty-seven healthy control participants (GAIN-SS: M = 2.72, SD = 1.22), 64 psychiatric control participants (GAIN-SS: M = 10.86, SD = 2.22), and 64 participants who reported suicidal thoughts within the past week (GAIN-SS: M = 11.83, SD = 3.92). Groups differed in their psychiatric symptoms, F(2, 192) = 230.7, p < .001, such that healthy control participants reported significantly fewer symptoms compared with the other two groups (95% CI = [8.01, 10.22], p < .001 compared with participants with suicidal thoughts; 95% CI = [7.04, 9.25], p < .001 compared with psychiatric control participants). As intended, psychiatric control participants and participants with current suicidal thoughts did not differ in their symptom levels, 95% CI = [−0.15, 2.09], p = .104, but differed with respect to experiencing suicidal thoughts (for demographic and clinical characteristics, see Table 1). The gender identities in the sample were 140 female; 40 male; 14 genderqueer, nonbinary, or gender-fluid; and one transgender. The racial and ethnic identities were 145 White, 13 Black/African American, 13 Asian, 16 Hispanic/Latino, two Middle Eastern or North African, one Native American/American Indian, and five identified as “other.”
Procedure
The study included a baseline survey followed by a 7-day EMA period. Participants downloaded the same app used in Study 1 (Metricwire) and were sent six surveys per day. Five surveys were sent at random times at least 90 min apart between 9 a.m. and 7 p.m. and stayed open for 1 hr. The last survey each day was sent at a random time between 8 p.m. and 9 p.m. and remained open for 6 hr. Participants were paid $15 for the baseline survey. The payment structure for the EMA was identical to Study 1. At the end of each survey, participants were provided with resources for treatment and safety (for more details about risk management, see the Supplemental Material).
Measures
Baseline survey
To assess suicidal thoughts in the main study, participants completed an online self-report version of the Self-Injurious Thoughts and Behaviors Interview (SITBI; Fox et al., 2020). The SITBI is widely used and has established predictive and convergent validity for online administration (Fox et al., 2020; Nock et al., 2007).
EMA
The EMA measures were identical to Study 1 with the following exceptions. There were slight differences in the items assessing rumination (“I concentrated and dwelled on the situation”) and expressive suppression (“I tried not to express my negative feelings”). Study 2 did not include items assessing emotional eating and body relaxation. To assess regulatory effort, if participants tried to decrease their negative emotions, they rated how effortful it was for them (“Overall, how much effort it took for you to decrease your negative emotions?”; 0 = not at all, 10 = a lot; for discriminant validity between this measure and the item for regulation attempts, see the Supplemental Material). Finally, similar to Kleiman et al. (2017), to assess momentary suicidal thoughts, participants rated their current suicidal desire (“Right now, how strong is your desire to die?”; 0 = not at all, 10 = very strong) and intent (“Right now, how strong is your intent to kill yourself?”; 0 = not at all, 10 = very strong), between: ω = .72, 95% CI = [.66, .78]; within: ω = .66, 95% CI = [.64, .68].
Analytic approach
Our analytic approach was identical to Study 1.
Results
The total number of completed surveys was 3,725. The average number of surveys completed per person was 28.26 out of 42 surveys (SD = 11.32; 67.3% compliance, Mdn = 76.2%). Groups did not differ in their compliance rate, F(2, 192) = 1.78, p = .172 (61.4%, 66.4%, and 72.6% for participants with suicidal thoughts and psychiatric and healthy control participants, respectively). We used all available data and report analyses with the original data. For missingness patterns and analyses with imputed data to account for missingness, see the Supplemental Material.
Identification stage: emotion-regulation attempts
We ran a multilevel regression model including only surveys when participants reported negative emotions in the past hour (nonzero responses; n = 1,780 surveys). Group (suicidal thoughts, psychiatric control participants, healthy control participants) was entered as a Level 2 predictor, and regulation attempts was entered as the dependent variable. We controlled for emotional reactivity. We did not find group differences between participants with suicidal thoughts (M = 3.44, SD = 1.79) and healthy control participants (M = 4.09, SD = 2.09), b = −0.65, SE = 0.38, t(179.3) = −1.70, p = .091 (adjusted p = 0.137), R2M = .03, R2C = .40, or psychiatric control participants (M = 3.81, SD = 1.62), b = −0.36, SE = 0.35, t(154.2) = −1.04, p = .301 (adjusted p = 0.710), R2M = .03, R2C = .40. There was also no difference between healthy and psychiatric control participants, b = −0.29, SE = 0.39, t(184.9) = −0.74, p = .459 (adjusted p = 1.26), R2M = .03, R2C = .40
Selection stage: emotion-regulation strategies
We repeated the previous analysis with each strategy as the dependent variable, including only surveys when participants indicated some level of regulation attempts (nonzero responses; n = 1,327 surveys). For a summary of the results, see Table 3. Participants with suicidal thoughts differed from psychiatric control participants only in their reported use of substances, such as alcohol and drugs, to regulate emotions (see Fig. 3). Both participants with suicidal thoughts and psychiatric control participants reported using distraction to a greater extent compared with healthy control participants. People with suicidal thoughts also reported using more rumination and substances compared with healthy control participants. With respect to self-injury, we found that participants with suicidal thoughts used more self-injury compared with healthy control participants, but this difference was no longer significant when correcting for multiple testing. Groups did not differ in their reported use of cognitive reappraisal, situation modification, social support, and expressive suppression. For descriptives and zero-order correlations between emotion-regulation strategies, see Table S7 in the Supplemental Material.
Emotion-Regulation Strategies in Daily Life as a Function of Group (Study 2)
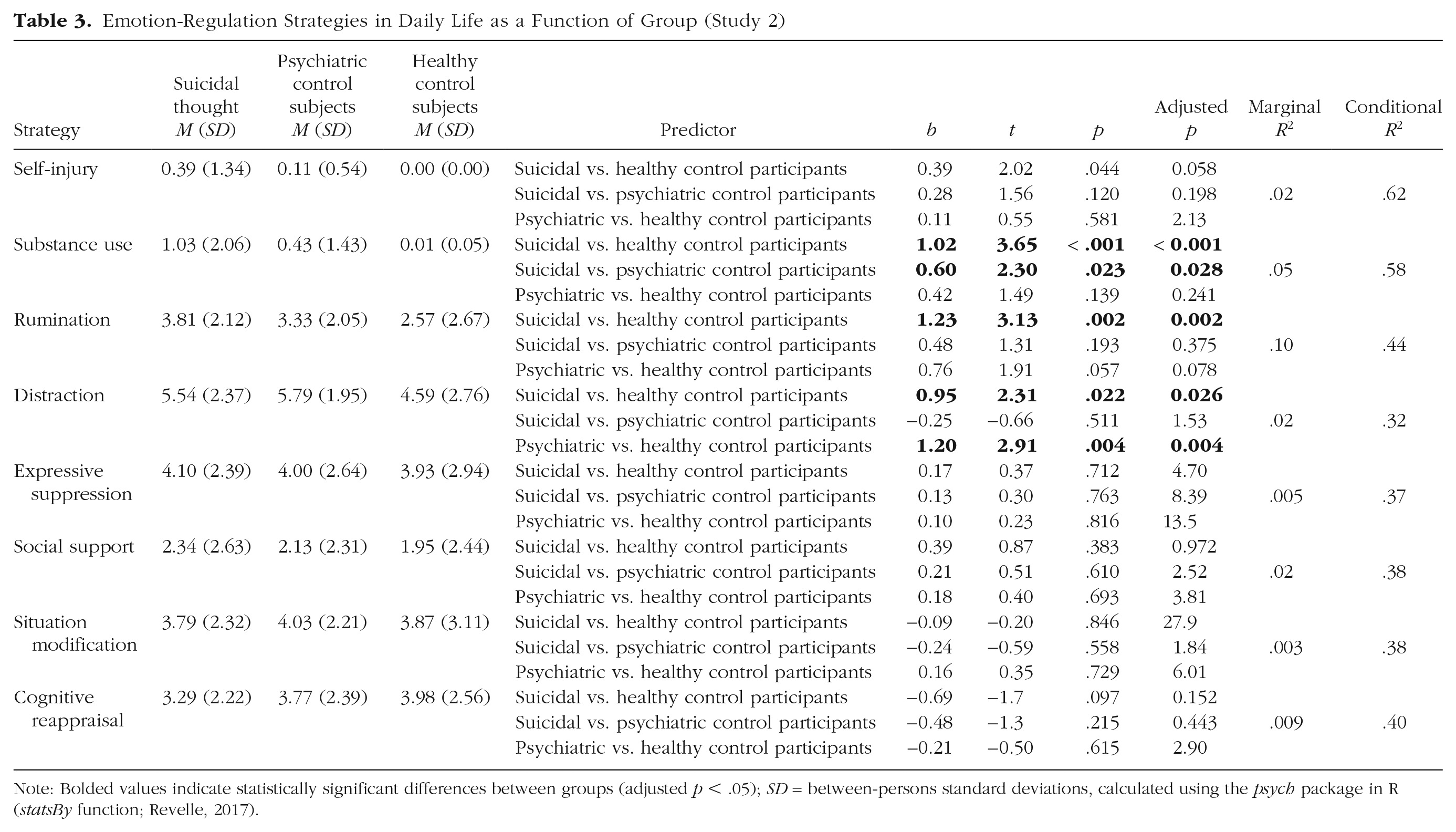
Note: Bolded values indicate statistically significant differences between groups (adjusted p < .05); SD = between-persons standard deviations, calculated using the psych package in R (statsBy function; Revelle, 2017).
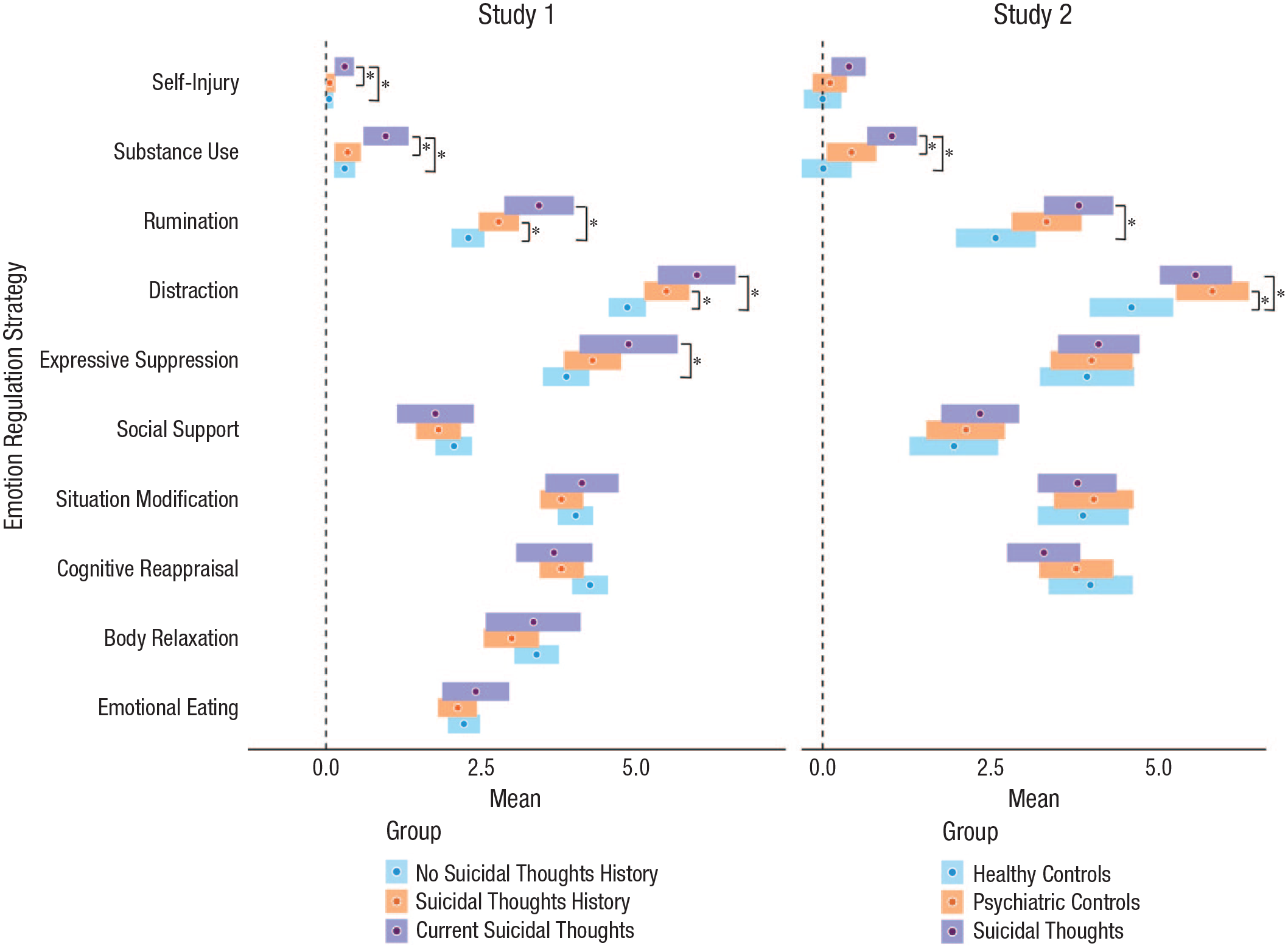
Differences in emotion-regulation-strategy use in daily life as a function of group. Participants with current suicidal thoughts used more substance use, rumination, distraction, and self-injury compared with healthy control participants or people with no history of suicidal thoughts. They differed from psychiatric control participants only in their use of substances (alcohol, drugs) to regulate emotions and from people with past suicidal thoughts in their use of self-injury and substances. Error bars represent 95% confidence intervals around the mean. Asterisk indicates adjusted p < 0.05.
Implementation stage: perceived emotion-regulation success and effort
We repeated the previous analysis with perceived emotion-regulation success and effort as dependent variables. When predicting perceived success, we removed the random slope for emotional reactivity because the model did not converge when it was included. Participants with suicidal thoughts reported less success in regulation (M = 3.97, SD = 1.93) compared with healthy control participants (M = 4.95, SD = 2.05), b = −0.98, SE = 0.35, t(164.4) = −2.81, p = .006 (adjusted p = 0.007), R2M = .04, R2C = .38. Psychiatric control participants (M = 4.56, SD = 1.84) did not significantly differ from people with suicidal thoughts, b = −0.59, SE = 0.33, t(148.8) = −1.82, p = .072 (adjusted p = 0.103), R2M = .04, R2C = .38, or healthy control participants b = −0.39, SE = 0.35, t(164.8) = −1.11, p = .269 (adjusted p = 0.592), R2M = .04, R2C = .38 (see Fig. 4a).
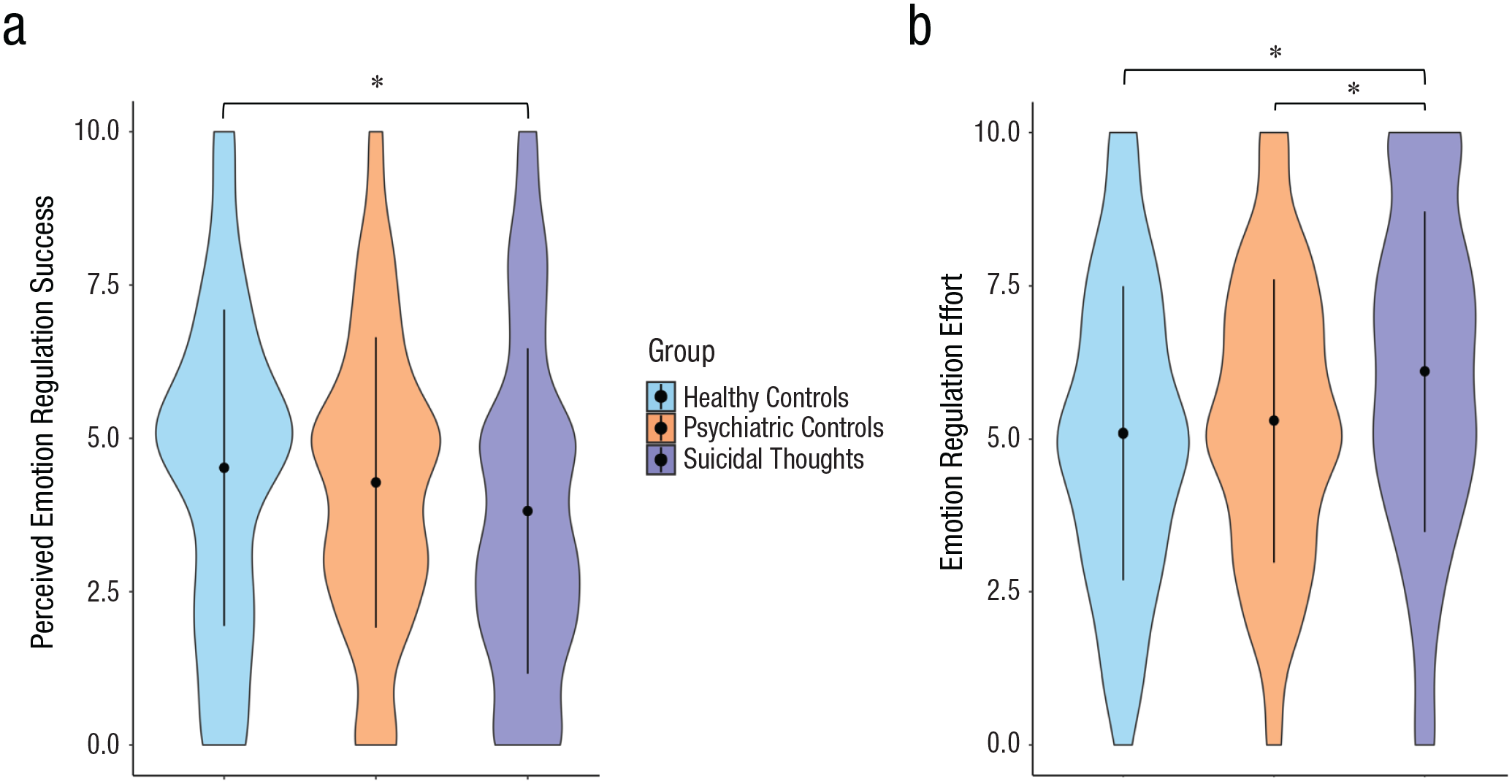
Differences in (a) perceived emotion-regulation success and (b) effort as a function of group (Study 2). Participants with current suicidal thoughts reported emotion regulation to be less successful and more effortful compared with healthy control participants. They differed from psychiatric control participants in their reported emotion-regulation effort but not in their perceived success in regulation. Error bars represent ±SD from the mean. Asterisk indicates adjusted p < 0.05.
Participants with suicidal thoughts also reported more effort in regulation (M = 5.91, SD = 1.89) compared with healthy control participants (M = 4.86, SD = 1.97), b = 1.05, SE = 0.31, t(155.8) = 3.37, p < .001 (adjusted p < 0.001), R2M = .13, R2C = .42, and psychiatric control participants (M = 5.29, SD = 1.63), b = 0.62, SE = 0.29, t(138.3) = 2.14, p = .034 (adjusted p = 0.043), R2M =.13, R2C = .42, even after accounting for the intensity of the negative emotions being regulated (see Fig. 4b). There was no difference in effort between psychiatric and healthy control participants, b = 0.43, SE = 0.31, t(154.2) = 1.39, p = .167 (adjusted p = 0.306), R2M = .13, R2C = .42. As an additional analysis, we tested whether perceived effort in regulation reflects the number of emotion-regulation strategies used. We tested the correlation between reported effort and the number of emotion-regulation strategies that were reported at the same time point. We found moderate positive correlations at the within-persons, r(1,327) = .300, p < .001, and the between-persons, r(195) = .227, p = .002, levels (for more details, see the Supplemental Material).
Prediction of momentary suicidal thoughts
We ran models with each emotion-regulation strategy (rated with respect to the past hour) as the independent variable and the intensity of current suicidal thoughts (rated with respect to the present moment) as the dependent variable, including only participants in the suicidal-thoughts group. We controlled for past-hour negative emotion and for suicidal thoughts at the previous time point (i.e., lagged suicidal thoughts).
The lagged-suicidal-thoughts variable was computed for each time point by drawing the intensity of suicidal thoughts in the previous time point. Because we did not expect suicidal thoughts rated at the last survey of the day to predict suicidal thoughts at the following day, we did not include overnight lags. Thus, lagged suicidal thoughts were computed only for time points occurring in the same day as the current time point. The model for situation modification did not converge when including a random slope for negative emotion, so it was removed from the model.
A summary of the results appears in Table 4. Substance use and self-injury predicted elevated suicidal thoughts above and beyond past-hour negative emotion and previous suicidal thoughts. Cognitive reappraisal, situation modification, social support, distraction, rumination, and expressive suppression did not predict suicidal thoughts after accounting for negative emotions and previous suicidal thoughts.
Prediction of Suicidal Thoughts in Real Time by Emotion-Regulation Strategies
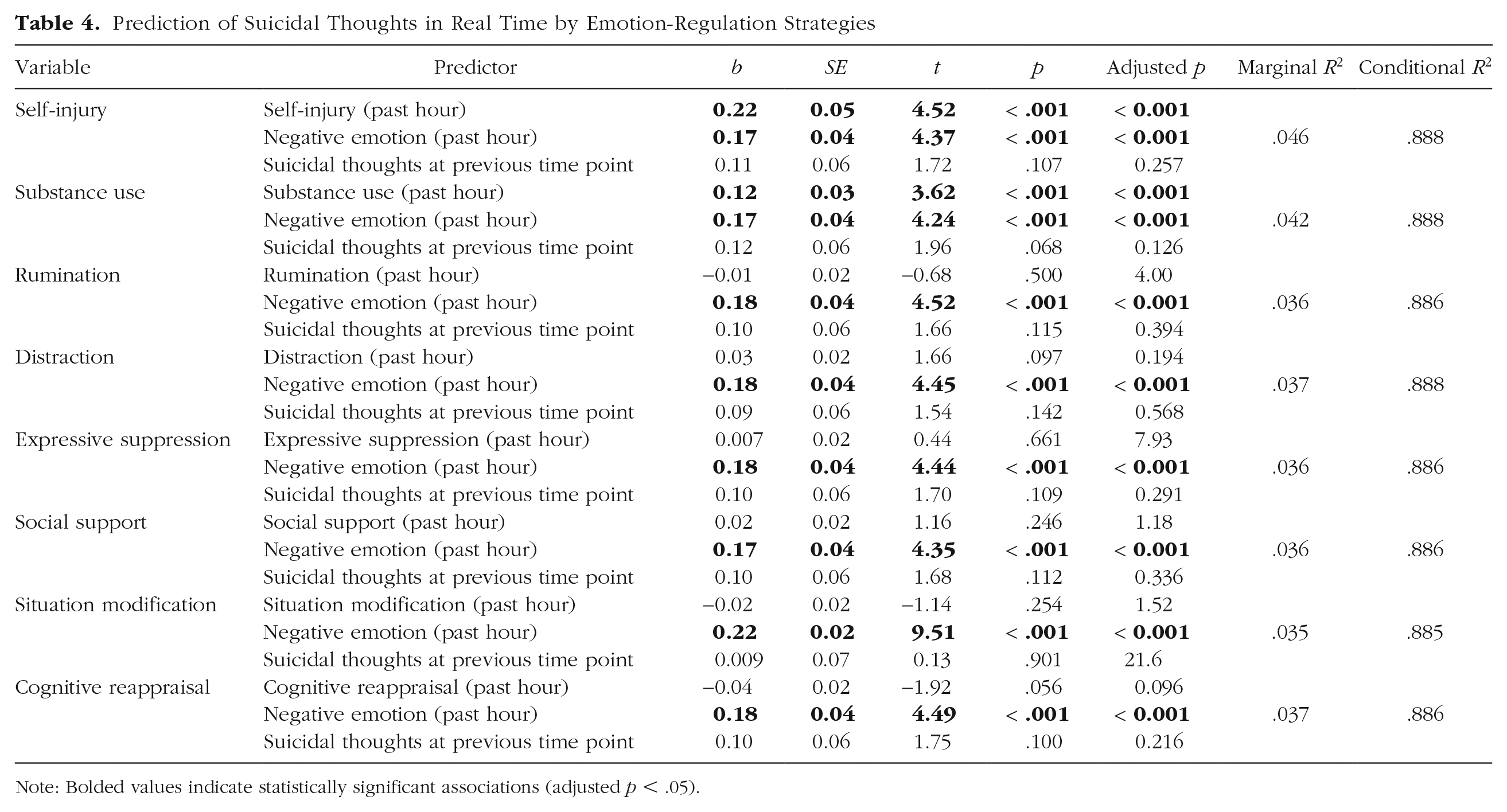
Note: Bolded values indicate statistically significant associations (adjusted p < .05).
General Discussion
Do people with suicidal thoughts differ in whether and how they regulate emotions in daily life? In the current project, we addressed this question by using EMA methods across two adult samples. We found that adults with suicidal thoughts did not significantly differ from healthy or psychiatric control participants in their reported emotion-regulation attempts. We also did not find evidence that they used strategies that are typically considered more adaptive to a lesser extent than healthy or psychiatric control participants (i.e., cognitive reappraisal, situation modification, social support). Instead, compared with healthy control participants, participants with suicidal thoughts reported greater use of distraction, rumination, and substances such as alcohol or drugs to regulate emotions.
Furthermore, people with suicidal thoughts perceived themselves to be less successful in regulation and reported more effort in doing so compared with healthy control participants. These findings point to an effort-success gap in emotion regulation (Gruber et al., 2012) given that participants with suicidal thoughts experienced reduced success despite their greater efforts. These findings also converge with laboratory studies finding evidence for reduced regulation efficacy and heightened effort among people with a history of suicidal thoughts (Kudinova et al., 2016; Miller et al., 2018).
At the same time, we did not find evidence that many of the observed patterns are specific to suicidal thoughts. To test for specificity, we compared people with current suicidal thoughts with people with similar levels of psychiatric symptoms. For several emotion-regulation difficulties, we found no evidence that they were specific to suicidality (e.g., increased reported use of rumination and distraction, reduced perceived success in regulation). However, some unique characteristics emerged. Adults with suicidal thoughts were more likely to report using substances to regulate emotions and experienced greater effort even compared with psychiatric control participants. These findings highlight the use of alcohol or drugs and elevated regulatory effort as emotion-regulation processes that may be specifically associated with suicidal thinking. Furthermore, substance use and self-injury were the only strategies predicting momentary suicidal thoughts in the suicidal-thoughts group. They also differentiated people with current versus past suicidal thoughts in Study 1. This suggests they may reflect state-like characteristics of the acute phase of suicidal thinking, distinguishing them from patterns observed in individuals with past suicidal thoughts (i.e., elevated rumination and distraction), which may represent more stable, trait-like regulatory difficulties. These findings further emphasize the potential role of substance use and self-injury in exacerbating suicidal thinking (Giugovaz et al., 2024; Hamza et al., 2012).
Findings also provide a nuanced examination of deficits at different stages of emotion regulation. We found no support for the hypothesis that suicidal thoughts are associated with deficits in trying to regulate emotions (i.e., emotion-regulation attempts), which is a substep of the identification stage of regulation (Gross, 2015). However, suicidal thoughts were associated with emotion-regulation strategies that are typically considered less adaptive, such as self-injury and substance use (selection stage), and with less success and more effort in implementing strategies (implementation stage). These findings are consistent with behavioral findings showing that adolescents who self-injure were able to generate similar solutions to noninjurers in a problem-solving task but chose to use more negative solutions and had lower self-efficacy in implementing better solutions (Nock & Mendes, 2008).
Therefore, these findings highlight the importance of focusing on both the selection and implementation stages of emotion regulation in clinical and research settings. Clinicians can help patients become more aware of their emotion-regulation strategies and reduce reliance on maladaptive strategies that may exacerbate suicidal thinking, such as substance use (DeCou et al., 2019). Incorporating interventions that improve strategy selection into just-in-time suicide-prevention approaches (Coppersmith et al., 2022) could be particularly beneficial. For example, interventions could suggest which strategies to use during moments of heightened distress (e.g., cognitive reappraisal, situation modification) while discouraging maladaptive responses (e.g., substance use). These interventions could be context-sensitive, tailoring recommendations based on factors such as emotional intensity (i.e., high vs. low distress; Matthews et al., 2021) and situational affordances (e.g., the degree of control over the situation; Troy et al., 2013).
Beyond strategy selection, future research should explore ways to support the effective implementation of emotion-regulation strategies. For instance, repeated training in cognitive reappraisal (Denny & Ochsner, 2014) may reduce the cognitive effort required for regulation and enhance regulatory success over time. Existing treatments that integrate emotion regulation as a core component, such as emotion-regulation therapy (ERT; Mennin & Fresco, 2014) and dialectical-behavior therapy (DBT; Linehan, 1987), have demonstrated efficacy in reducing symptoms of anxiety, depression, and suicidality (e.g., ds = 1.5–4.5 for reducing general-anxiety-disorder symptoms and ds = 1.5–2.0 for reducing depressive symptoms in ERT; Renna et al., 2017; pooled Hedges’s g = 0.622 for reducing suicidal thoughts and behaviors in DBT; Panos et al., 2014). These therapies focus on teaching emotion-regulation skills, including mindfulness, cognitive restructuring, and psychological distancing, alongside exposure-based techniques (Lynch et al., 2006; Mennin & Fresco, 2014). Our findings could further inform these treatments by identifying the specific maladaptive strategies most frequently used by individuals with suicidal thoughts to be targeted in treatment (e.g., distraction, rumination, expressive suppression, self-injury, and substances). Critically, they can point to the strategies most strongly associated with elevations in suicidal thoughts (e.g., substance use, self-injury). In addition, our results suggest that regulatory effort, a factor not explicitly emphasized in existing protocols, may serve as an important intervention target.
Limitations and future directions
In the current project, we provide a descriptive overview of reported emotion regulation in daily life among adults with suicidal thoughts. However, these studies also have several limitations. First, our findings are correlational. Therefore, causal conclusions on the role of emotion regulation in the development of suicidal thinking cannot be drawn. Future research should adopt longitudinal or experimental designs to better clarify causal relationships and account for additional variables apart from negative emotional reactivity that may influence emotion-regulation processes and suicidal ideation.
Second, participants self-reported their emotion regulation at each time point. Although self-reports provide valuable insights, they are susceptible to response biases and can capture only how people perceive their emotion regulation. Future research should consider integrating behavioral measures alongside self-reports to obtain a more comprehensive understanding of emotion-regulation processes. In addition, consistent with previous studies assessing emotion regulation in daily life, we used single items to assess emotion-regulation attempts, strategies, and regulatory success and effort (Gruber et al., 2013; Kalokerinos et al., 2019; Moeck et al., 2024). However, this restricted our ability to test the reliability of those measures. Some items also differed from one another in how they were phrased. Future research should use multiple items to assess each of these constructs while trying to maximize consistency across items.
Third, our studies used community samples that were recruited online and were heterogeneous in terms of psychiatric-symptom profiles. This heterogeneity reflects the transdiagnostic nature of suicidal thoughts and the diverse symptom presentations associated with suicidality. However, it may also obscure distinct emotion-regulation patterns that characterize specific subgroups of individuals with suicidal thoughts who share similar symptoms and potentially reduce statistical power. Future studies should explore the generalizability of our findings to inpatient samples (as opposed to samples recruited online) and examine whether distinct subgroups of individuals with suicidal thoughts (e.g., individuals primarily experiencing internalizing symptoms) demonstrate unique emotion-regulation patterns compared with other subgroups (e.g., individuals primarily experiencing externalizing symptoms) and compared with psychiatric control participants who exhibit the same type of symptoms. It is also important to distinguish between individuals with suicidal thoughts who have attempted suicide and individuals who have not. In this study, we focused on suicidal thoughts and included both individuals with and without a reported suicide attempt (see also Coppersmith et al., 2023; Jenkins et al., 2025; Miller et al., 2018). However, emotion-regulation patterns may differ based on suicide-attempt history, highlighting the need for future research to explore this possibility.
Because this investigation was largely exploratory, replications are needed. In addition, despite post hoc power analyses indicating sufficient power, the studies did not include a priori power analyses specifically tailored to these research questions, further underscoring the need for replications. Moreover, given that Study 2 had a high proportion of female participants, future research should strive for more gender-balanced samples to ensure broader generalizability.
Future research should also further clarify the role of emotion-regulation effort in suicidal thoughts. There is now converging evidence across daily life and neurological assessments that individuals with suicidal thoughts may experience more effort when regulating emotions (Miller et al., 2018). However, it remains unclear what is the exact nature of effort in this context (Wolpe et al., 2024). Our findings suggest that using a higher number of emotion-regulation strategies may contribute to perceived effort, although other factors, such as limited cognitive resources, also warrant investigation (Franz et al., 2023). In addition, future studies should examine how contextual factors influence the link between emotion regulation and suicidal thoughts. Factors such as controllability of the situation, uncertainty, or emotion-regulation goals can shape emotion-regulation processes and potentially moderate the observed effects (Millgram et al., 2019; Moeck et al., 2024; Troy et al., 2013).
To conclude, this study is the first to assess reports on multiple emotion-regulation processes in adults with suicidal thoughts using naturalistic methods. This takes the field a step further in understanding what are the specific emotion-regulation challenges people with suicidal thoughts encounter. Ultimately, this knowledge could help identify how these challenges could be better addressed.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026251349809 – Supplemental material for Emotion Regulation in Daily Life Among Adults With Suicidal Thoughts
Supplemental material, sj-docx-1-cpx-10.1177_21677026251349809 for Emotion Regulation in Daily Life Among Adults With Suicidal Thoughts by Yael Millgram, Daniel D. L. Coppersmith, Gal Sheppes, Rebecca Fortgang, Amit Goldenberg and Matthew K. Nock in Clinical Psychological Science
Footnotes
Acknowledgements
This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Science Foundation or the National Institutes of Health.
Transparency
Action Editor: Aleksandra Kaurin
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.