
Abstract
Having more social connections is related to better quality of life in people with psychosis. However, little is known about the nature of these social connections or whether the personal significance of social connections matters for quality of life. We aimed to fill this gap by surveying 200 people with psychosis using social identity mapping (SIM), which allows people to name their groups, roles, and relationships and how they feel about these. SIM names were categorized into 10 groups, with “activities” (39%) and “family” (14%) being most common; “patient” (3%), “politics” (2%), and “local residence” (1%) were least common. Hierarchical regression revealed that the only variable associated with better quality of life was having a greater number of highly important connections. This was mediated by self-esteem. Clinicians and researchers should examine the potential of social identification, the internalization of social connections, as a means of improving quality of life.
Keywords
Psychotic disorders such as schizophrenia affect 2% to 3% of the global population; that is 20.9 million people worldwide (Charlson et al., 2018; World Health Organization [WHO], 2004). Common symptoms of psychotic disorders include distressing experiences, such as hallucinations or hearing and seeing things that other people cannot see and hear. Other common symptoms are paranoid delusions: the distressing and unfounded belief that other people want to harm you (Fusar-Poli et al., 2022; McCarthy-Jones et al., 2013). Psychotic disorders are associated with a high burden of disease, a significantly reduced life span, and low quality of life (Chang et al., 2023 ; Cloutier et al., 2016; Dingle et al., 2014; Hjorthøj et al., 2017; Millier et al., 2014; Oakley et al., 2018; Walker et al., 2015). Many people with psychotic disorders also describe being dissatisfied with their social relationships (Dong et al., 2019; Jerome et al., 2023; Tee et al., 2022; Watson et al., 2018). Furthermore, people with psychosis have described distress related to changes in their social lives and in their sense of identity when they developed psychosis (Conneely et al., 2021; H. Cooper, 2022).
Experiencing a psychotic episode, and continued symptoms, and receiving support from services for psychosis can bring about important changes in people’s relationships, group memberships, and roles that have a profound impact on how people understand themselves (i.e., their sense of social and personal identity; Conneely et al., 2021; Hogg et al., 2022; Kraepelin, 1913; Nevarez-Flores et al., 2022; Nordgaard et al., 2018; Parnas & Handest, 2003; Parnas & Jansson, 2015; Watson et al., 2018). Research has shown that after a psychotic episode, people’s social world has an important impact on their health and happiness, their psychotic symptoms, and their recovery (Badcock, Di Prinzio, et al., 2020; Badcock et al., 2019, 2021; Gayer-Anderson & Morgan, 2013; Palumbo et al., 2015). Researchers assess social connectivity by counting contacts in social networks and by asking people about the number of friends they have or how their time is used/how much time is spent alone compared with in social, structured activities (D. Fowler et al., 2017; Palumbo et al., 2015; for a more detailed review, see next section). However, little is known about the nature of these social connections, the personal meanings people with psychosis attach to these social connections, and whether this matters for supporting better quality of life. This research fills that gap by aiming to (a) use social identity mapping (SIM) to describe the nature of people’s social connections and (b) examine associations between features of social identity maps and people’s quality of life. Specific analyses explore the relationship between social connections and quality of life, considering not simply the number but also the personal meanings attached to these social connections (e.g., how important and positive people feel each connection is).
To do this, we draw on the social identity approach to health (SIAH; Haslam, Cruwys, et al., 2019; Haslam et al., 2012, 2018, 2021; Jetten et al., 2017) and use SIM, which allows people to create a personal map of their groups, roles, and relationships—social connections—while also measuring how important and positive each of these are. We propose that having a larger number of connections that are considered personally important and thereby internalized to a greater degree into people’s sense of self would be associated with better quality of life. In line with the expectations from the SIAH, we propose that this stronger social identification will be related to how people see and appraise themselves (better self-esteem) and how satisfied they are with their lives (better subjective quality of life).
Social Connections and Psychosis
Social connections have been conceptualized in a variety of ways. This includes as relationships, networks, and a source of social support (Christakis, 2004; House et al., 1988; Perkins et al., 2015). Often, social connections are measured by assessing the specific number of social contacts a person has (e.g., number of friends, whether one has a romantic partner; Giacco et al., 2021; Vogel et al., 2021) or through evaluations of how satisfied people are with the quantity and/or the quality of their interpersonal relationships (Badcock, Adery, & Park, 2020). Research suggests not only that having many social connections is important for individuals’ happiness over time but also that they play a key role in improving health, reducing distress, and reducing risk of mortality (J. H. Fowler & Christakis, 2008; Granovetter, 1973; Holt-Lunstad et al., 2010; House et al., 1988; Putnam, 2001; Thoits, 1995). Social connections help, in part, because other people are important sources of support that can help individuals to manage the minor and major events in their lives, including illness (Cohen & Wills, 1985; Thoits, 2011). However, there are likely other mechanisms through which social connectedness affects health outcomes, including through social identification (Haslam et al., 2022).
People diagnosed with psychotic disorders report smaller social networks than the general population, and their roles and relationships often change as a result of their symptoms and their involvement with services (Gayer-Anderson & Morgan, 2013; Laxhman et al., 2017; Michalska da Rocha et al., 2017; Palumbo et al., 2015; White et al., 2021). The loss of social connections and social roles can thus accompany psychotic disorders and may partially account for individuals’ reported dissatisfaction with their social world (Boeing et al., 2007). Indeed, an analysis of large-scale national data in Australia suggested that people diagnosed with psychotic disorders experience both dissatisfaction with social connections and loneliness, both of which are associated with higher levels of service use and an increased risk of suicide (Badcock, Adery, & Park, 2020; Badcock, Di Prinzio, et al., 2020; Badcock et al., 2019, 2021). Many people with a psychotic disorder also report wanting more social connections: In a sample of more than 500 people with schizophrenia-spectrum diagnoses, 68% said they would like to increase the size of their social networks (Tee et al., 2022). There is evidence to suggest that having more social contact with friends in the first year after the onset of a first episode of psychosis, is a significant predictor of symptom remission, whereas less contact with friends is associated with more severe symptoms and lower quality of life (Degnan et al., 2018).
It is clear that social connections matter: Who one knows and how many of these connections are available can determine whether an individual has access to tangible supports (e.g., advice, comfort, information, finances) during difficult times (Smith & Christakis, 2008). Yet, an understudied aspect of social connections, is that they can also help people to make sense of who they are. That is, social connections are also an important source of identity that affects how individuals feel about themselves and their lives. There is little evidence as to the types of social connections people with psychosis have, or how they feel about these. To better understand whether and specifically how this psychological internalization of social connections as social identities may influence outcomes, we draw on the SIAH (Haslam, Cruwys, et al., 2019; Haslam et al., 2012, 2018, 2021; Jetten et al., 2017).
The SIAH: Theory and Applications
The SIAH combines insights from social identity theory (Tajfel & Turner, 1979) and self-categorization theory (Turner et al., 1987) to understand the nature and implications of group dynamics for health. According to this approach, individuals come to understand who they are through their group memberships (Haslam et al., 2012, 2018; Jetten et al., 2014). Group memberships can reflect the social categories that define people, including age or gender; social roles, such as being a parent or sibling; interpersonal relationships, such as friendships or romantic relationships; affiliations; and activities, such as political parties, teams, or clubs (Haslam et al., 2012, 2018). Through these group memberships, individuals can share experiences with others and feel a sense of connectedness and belonging that can facilitate access to tangible and intangible resources, including social support (Jetten et al., 2014, 2017). Critically, individuals can identify with these group memberships to various degrees. Here, identification includes the extent to which a group is considered important to who one is, how positively it is evaluated by the person, or whether an individual feels bonded to or acts with other individuals in the group (Leach et al., 2008). Identification matters because as it increases, it can unlock access to psychological resources, such as self-esteem and a sense of control, that can contribute to trust in others, quality of life, and well-being (Greenaway et al., 2016; Jetten et al., 2015; Tajfel & Turner, 1979).
There is now considerable research attesting to the benefits of having a number of group memberships and stronger identification with a given group, for various health and well-being outcomes, including depression, social anxiety, and addiction (Beckwith et al., 2015; Best et al., 2016; Dingle et al., 2019; Haslam, Best, et al., 2019; Meuret et al., 2016). There has also been increased interest in applying these ideas to clinical populations with different diagnoses. For instance, a recent investigation found that identifying with an “autism identity” was positively associated with personal self-esteem and quality of life (K. Cooper et al., 2017; R. Cooper et al., 2021). Other work in a nonclinical groups suggests that group memberships and identification may be related to one of the most common symptoms associated with psychotic disorders: paranoia (Elahi, 2017; Greenaway et al., 2015). Here, cross-sectional data from a large household survey in the northwest of England suggested that neighborhood identification, defined here as participants’ sense of belonging to their immediate neighborhood (“your street or block”), was associated with lower paranoia in the general population (McIntyre et al., 2021). National identification was cross-sectionally associated with less paranoia for a community sample of British people from African and African Caribbean backgrounds who had had primarily positive experiences with White British people 1 (McIntyre et al., 2021). In another cross-sectional study of subclinical paranoia, greater identification with one’s family was associated with lower paranoia in students (Sani et al., 2017). Although promising, this research has focused on subclinical symptoms of psychosis rather than people diagnosed with a psychotic disorder and imposed a preset choice of social identification: identification with nation (McIntyre et al., 2021), neighborhood, or friends (McIntyre et al., 2018). Given the focus on subclinical paranoia in the existing literature, it is unclear whether similar relationships between identification and well-being may be observed among individuals who have been diagnosed with a psychotic disorder in which paranoia and other symptoms are more severe. One might expect, for example, that in cases in which paranoia is more severe, social identification does not make any difference to quality of life because the influence of psychotic symptoms may be the most important factor determining quality of life. Previous work has measured social identification with specific, imposed groups, such as neighborhood, nationality, or friends, including manipulation to increase identification with a specific group, such as nationality (Greenaway et al., 2019). These approaches have significant limitations: The measures described above risk missing the range of social connections that might be important to an individual. One might have strong social identifications with groups other than the nationality of a country, none of which would be captured by a measure solely assessing strength of national identification. To address these issues, in the present research, we extended the SIAH to individuals with a diagnosis of a psychotic disorder and used an ecologically valid means of assessing social connections and identification that allows participants the freedom to come up with and name their own groups, roles, and relationships in a way that is creative, self-driven, and self-reflective: SIM (Cruwys et al., 2016).
The Current Study
To date, no research has examined the relationship between social identification and quality of life quantitatively in the clinical sample of people diagnosed with a psychotic disorder. SIM offers a way of measuring the number of connections that people have and how they feel about these connections (Bentley et al., 2020; Cruwys et al., 2016). This method allows participants to reflect on, and list, all of their social connections: group memberships, roles, and relationships. Because some of these are not groups but relationships, in the current study, we refer to them as “connections.” Participants are then guided through a process in which they evaluate the importance, positivity, and amount of activity associated with each of the connections listed on the map. In this way, SIM enables a fuller examination of the nature of people’s connections. Individuals are given agency in detailing and evaluating their links to others and a way that captures their personal perception and experience of how positive the groups are and how important they are for their sense of self.
Based on the SIAH, higher identification with a given group and/or having a greater number of groups would be associated with better self-esteem and better quality of life (Haslam et al., 2018, 2021; Sani et al., 2012, 2015a, 2015b; Tajfel, 1978). However, when it comes to SIM, existing research has not shown consistent patterns between the features measured in the maps and quality of life or well-being (Bentley et al., 2020; Cruwys et al., 2016). In some instances, the overall number of groups is positively related to well-being. In other instances, it is the number of positive groups that is associated with greater satisfaction with life and better self-esteem (Cruwys et al., 2016, Study 1). In another study, it was the number of important groups that was positively associated with quality of life (Bentley et al., 2020; Cruwys et al., 2016, Studies 1 and 3). Because there is no definitive pattern in the associations between social identity features and various well-being outcomes when assessed using social identity maps and because this study represents the first use of the SIM tool with a sample of individuals with a diagnosis of a psychotic disorder, we were unable to make specific hypotheses. The current study had two exploratory aims: (a) to use SIM to describe the nature of social connections among a sample of individuals with a diagnosis of psychotic disorder and (b) to examine associations between features of social identity maps and quality of life.
Method
Transparency and openness
Within the limitations of the protocol that received ethical approval from the Health Research Authority (HRA) and of working with a clinical sample recruited from National Health Services (NHS), this study adheres to the guidelines set out in the Transparency and Openness Promotion community working group (Nosek et al., 2015). Supplementary materials (i.e., consent form, participant information sheet, SIM tool, measures, information on the internal piloting phase, additional details on analyses, including missing data and assumption testing) are available online at https://osf.io/ctdhy/. The actual data cannot be deposited publicly because it would be in breach of the HRA ethical approval that was granted. We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Participants and design
Participants were 200 individuals with a diagnosis of a psychotic disorder (gender: male, n =113, female, n = 67; age: M = 37.80 years, SD = 12.53) recruited from inpatient wards, Early Interventions Services, and outpatient clinics within East London NHS Foundation Trust (ELFT). Participants were eligible to take part in the study if they were at least 18 years old, had the capacity to provide informed consent, and had received a diagnosis of a psychotic disorder according to the International Classification of Diseases (ICD-10: F20, F21, F22, F23, F24, F25, F28, F29; WHO, 2004). The most common diagnosis was schizophrenia (47.5%), followed by schizoaffective disorder. When they took part in the study, 73% of participants were unemployed, 57% were inpatients, and of these individuals, 55.5% were voluntary patients (i.e., they were not detained under a section of the Mental Health Act). Sixty percent of the sample were born in the United Kingdom. The sample had a mix of ethnic categories that reflects the diversity of the area where data were collected (i.e., Black/Black British–African: 18.5%; White British: 17%; Asian/Asian British–Bangladeshi: 16%; Black/Black British–Caribbean: 12.5%; White other: 6.5%; other ethnic group: 4.5%; other Black/Black British background: 3.5%; mixed/multiple ethnic groups–White and Black Caribbean: 2.5%; mixed/multiple ethnic groups–White and Black African: 1%; other Asian/Asian British background: 2%; White Irish: 1%; Asian/Asian British–Chinese: 1%; mixed/multiple ethnic groups–White and Asian: 0.5%; missing: 1.5%). Ninety-nine participants were within the first 5 years since diagnosis, and 101 had been diagnosed for 5 years or more.
Power calculations were computed using G*Power (Faul et al., 2009) based on an existing study using SIM with a sample of individuals with mental-health issues (Cruwys et al., 2016). Here, quality of life and number of identities were found to have correlation coefficients of 0.24 to 0.39. To be conservative, the calculation was based on the correlation of 0.24 and power of .95. The required sample size was 179 participants (one-tailed test). In anticipation of attrition (e.g., if participants did not complete the mapping exercise or the survey or chose to stop participation), we opted to increase the number of participants by 10% (i.e., 196 participants, which was rounded up to 200).
A cross-sectional correlational design was used. Ethical approval was received from the HRA via Queen’s Square Research Ethics Committee (18/LO/0799). Patient and public engagement was an important part of our study development and design. Individuals with lived experience of psychosis and carers of individuals experiencing psychosis from the Service Users and Carers Groups Advising on Research (SUGAR; City, University of London) reviewed and commented on all of the study materials. The choice of SIM over other measures of social identity was informed by the feedback from SUGAR. The SUGAR group recommended participants be given as much flexibility and self-direction as possible. SUGAR’s feedback also led to the instructions and examples provided with the SIM questions being modified (e.g., the examples of groups were changed to be more fitting for participants in the United Kingdom; see supplementary materials).
Materials and measures
SIM
Groups and social identity features were measured using SIM (Bentley et al., 2020; Cruwys et al., 2016). Social identity maps are visual representations of participants’ social worlds, simultaneously capturing the key features of their various group memberships according to social identity and self-categorization theories. Social identity maps acknowledge the complexity of individuals, recognizing that they can belong to multiple groups and vary in their sense of identification and connection with these groups, and allow researchers to simultaneously measure different social identity features (Beckwith et al., 2019; Bentley et al., 2020; Cruwys et al., 2016; Firmin et al., 2015). To complete their maps, participants were asked to “think about all the groups and categories that [they] belong to.” A list of examples was read out to each participant: “You can belong to a group or category because: You have similar opinions about something (e.g. political party, sports team, world views). You were born in, or live in the same country . . . ” (see online supplement for complete wording: https://osf.io/ctdhy/).
The names written on a subset of 20% of the groups reported on social identity maps were categorized by two of the authors independently (M. Conneely and D. Giacco). Once an agreement on categories was made, M. Conneely categorized the remaining groups using the agreed categories. This allowed the types of groups, roles, and relationships to be summarized and how common each category was to be identified (see Table 1).
Categories of Groups Listed on Social Identity Maps With Examples
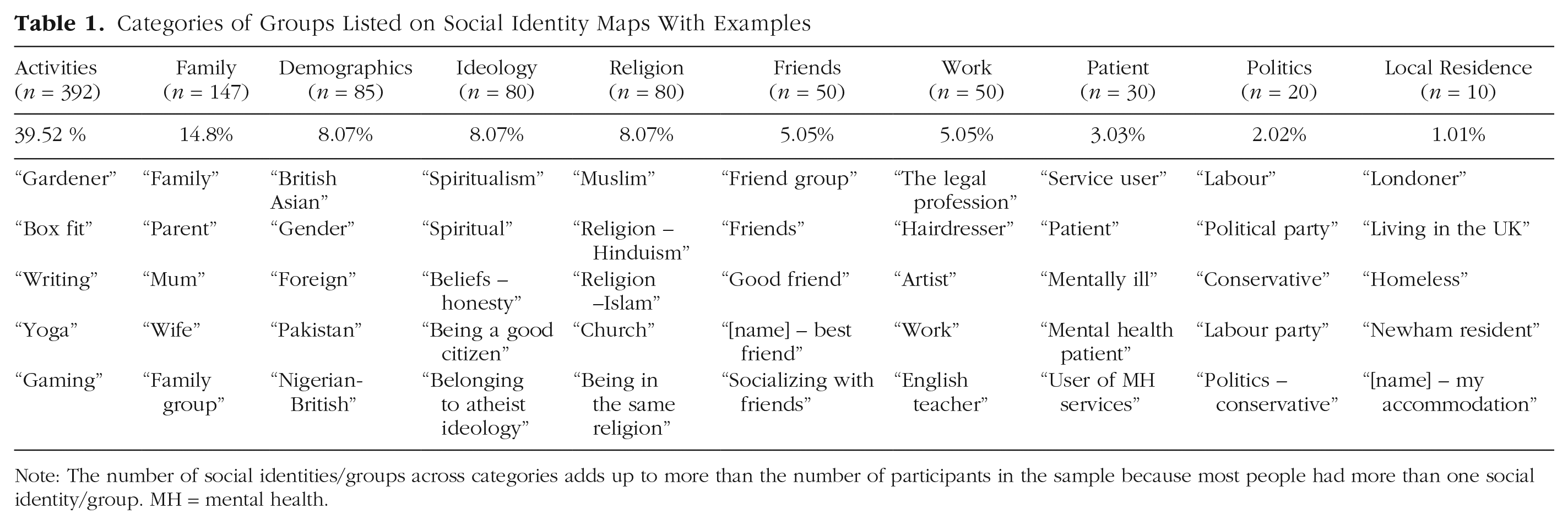
Note: The number of social identities/groups across categories adds up to more than the number of participants in the sample because most people had more than one social identity/group. MH = mental health.
Next, participants were given an A3-size (297 mm × 420 mm) piece of paper and Post-it notes in three different sizes (small: 38 mm × 51 mm; medium: 76 mm × 76 mm; large: 76 mm × 127 mm). Participants were asked to choose a Post-it for each group that reflected an aspect of themselves and to write the name of the group on the Post-it. They were told that the size of the Post-it chosen should reflect the group’s importance to them, with large Post-its reflecting “highly important” groups, medium Post-its reflecting “important” groups, and small Post-its reflecting “less important” groups. Participants were then asked to put numbers in the corners of each Post-it to rate how many days out of a typical month they would have social contact with the group. Creating a social identity map resulted in the following variables for analysis. See Figure 1 for an example of a social identity map.
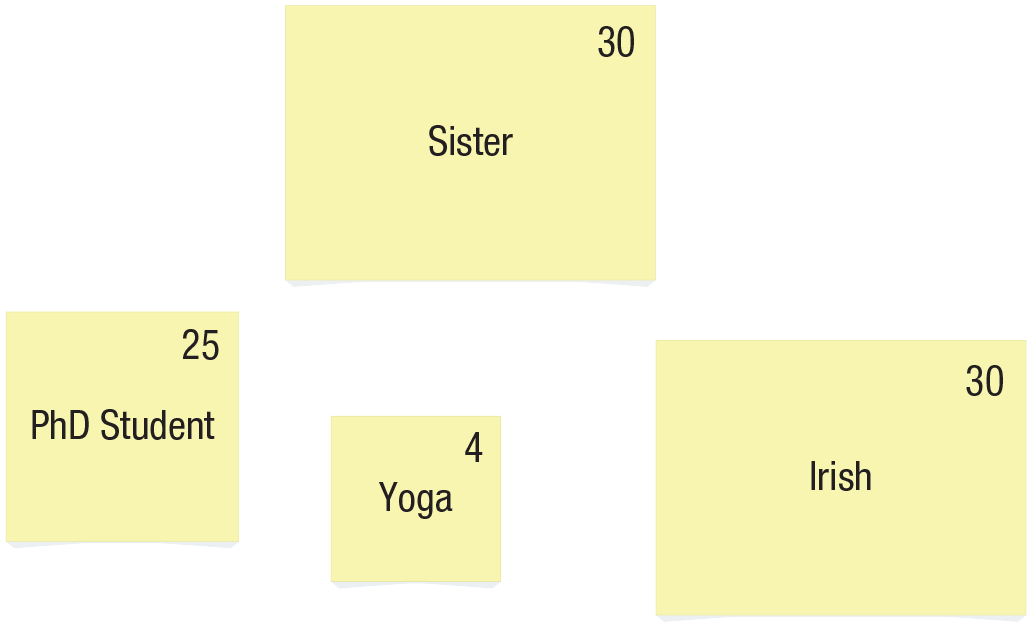
Example social identity map.
Number of groups
The total number of groups was calculated by summing all of the Post-its on the map. The number of groups was also subdivided into the number of highly important groups (i.e., the sum of large Post-its only), the number of important groups (i.e., the sum of medium Post-its only), and the number of less important groups (i.e., the sum of small Post-its only).
Number of positive groups
The number of groups that were rated as at least 6 out of 10 or more in ratings of positivity were summed. This process was used in existing SIM research (Bentley et al., 2020).
Social contact
On each Post-it, participants rated how often in a typical month they would have social contact with the group listed. This was rated from 0 to 30 days, and higher scores indicate more interaction over a given month. For example, having social contact in a typical month with the group on the map once a week would be rated as 4. The social-contact scores across the map were summed and divided by the total number of groups in the person’s map. This resulted in a measure of social contact across all the groups on the map.
Three additional measures were collected using SIM but not analyzed for the current article because they did not relate to this article’s aims: (a) a second rating of each group’s importance to their sense of self (0–10), (b) evaluations of the perceived compatibility between the groups on the map, and (c) an indication of how long participants had been a part of the group (in years).
Quality of life
The Manchester Short Assessment of Quality of Life (MANSA; Priebe et al., 1999; Cronbach’s α = .81, M = 4.35 SD = 1.02). comprises 12 items rated on a 7-point Likert-type scale (1 = couldn’t be worse, 7 = couldn’t be better). The MANSA assesses subjective quality of life by asking participants to indicate how satisfied they are with their life as a whole and with specific areas of their life, including their job, financial situation, friendships, leisure activities, accommodation, safety, physical health, and mental health. It also comprises four dichotomous yes/no questions (e.g., “Have you seen a friend in the last week?”). These questions are used to create the Objective Social Situation (SIX) scale (see details below). Quality of life was computed by averaging across the 12 nondichotomous items. The MANSA is widely used in psychosis research.
Self-esteem
The Rosenberg Self-Esteem scale (Rosenberg, 1965; Cronbach’s α = .84, M = 3.36, SD = 0.73). measures self-esteem using 10 statements rated on a 5-point Likert-type scale (1 = not very true of me, 5 = very true of me). Statements include “At times I think I am no good at all” (reverse-coded) and “I feel that I am a person with worth.” Self-esteem was computed by averaging scores on the 10 statements (reverse-coding the negatively worded statements).
Time since diagnosis
Time since diagnosis was calculated by taking the time between when participants became unwell and the date of participation. This was measured in weeks. Each participant was asked when they first became unwell. If participants did not remember, then their medical notes were used.
Symptoms
The Positive and Negative Symptoms Scale (PANSS; Kay et al., 1987; Cronbach’s α = 0.90, M = 58.34 SD = 19.21). measures positive, negative, and general symptoms of schizophrenia. It is based on a standardized clinical interview in which a researcher rates the presence and degree of 30 items, each capturing a symptom. The items comprise seven positive symptoms (delusions, hallucinations, conceptual disorganization, excitement, grandiosity, suspiciousness, and hostility), seven negative symptoms (blunted affect, emotional withdrawal, poor rapport, difficulty in abstract thinking, lack of spontaneity, stereotyped thinking, and social withdrawal), and 16 general psychopathology symptoms (somatic concern, anxiety, guilt feelings, tension, mannerisms and posturing, depression, motor retardation, uncooperativeness, unusual thought content, disorientation, poor attention, lack of judgment and insight, disturbance of volition, poor impulse control, preoccupation, and active social avoidance). The severity of each item is rated on a scale from 1 (absent) to 7 (extreme). The ratings are summed to create the variable for symptoms with a possible score ranging from 30 to 210.
SIX
The SIX (Priebe et al., 2008) comprises four items that assess objective features of a person’s social situation. It consists of four items designed to evaluate various aspects of a person’s social circumstances. Participants respond to questions about their employment status, living arrangements, social interactions, and whether they have met a friend recently. Each response is assigned a score of 0, 1, or 2, depending on the level of social support or stability indicated. For example, for employment, no employment receives a score of 0, and regular, nonsheltered employment receives a score of 2. Likewise, living alone is scored as 0, and living with a partner or family is scored as 1. The total score can range from 0 to 6; higher scores indicate a more favorable objective social situation.
Procedure
Participants were recruited during their outpatient appointments with psychiatrists or multidisciplinary teams or while they were staying in inpatient wards. M. Conneely or a research assistant employed by ELFT met with each potential participant to determine if they met the eligibility criteria. Individuals who did not meet the criteria were not invited to participate. Eligible participants were provided with the participant information sheet, and if they wished to take part, they gave informed consent (the participant information sheet and consent form are available online at https://osf.io/ctdhy/). A researcher then arranged to meet with the individual in a suitable location, either at an outpatient or inpatient ELFT clinic or in the individual’s home. Participants were given adequate time to complete the measures, typically ranging from 40 min to 70 min. After completion, participants were thanked for their time and given £10.
Because this study was the first application of SIM in a sample of individuals with psychosis, the first month of data collection was treated as a pilot phase to troubleshoot any potential issues that might be encountered (Janghorban et al., 2014). Additional details about this phase are available in the online supplement (https://osf.io/ctdhy/). Twelve participants were recruited during this time. Because nothing was changed as a result of the piloting phase, these 12 participants were included as part of the main sample, which is standard with internal piloting phases (Arain et al., 2010).
Data analyses
Qualitative content analysis was conducted using N-Vivo to describe the types of social connections listed on maps. Statistical analyses were performed using IBM SPSS (Version 25). Descriptive statistics, including frequencies, means, and standard deviations, were used to assess the selections and ratings associated with participants’ social identity maps. Pearson’s bivariate correlations and independent samples t tests were employed to explore associations between participant characteristics (e.g., time since diagnosis, symptoms, and objective social situation) and variables, such as the number of social groups, social contact, self-esteem, and quality of life. Hierarchical regression analysis was used to examine whether the number and quality indicators of social groups or social contact were better predictors of quality of life while controlling for objective social situation and symptoms. These control variables were chosen because previous research indicates that social contact is associated with quality of life and to attempt to isolate and investigate whether the meaning attributed to each social connection is associated with quality of life above and beyond the amount of social contact. Without controlling for objective social situation, one might assume any correlation identified between quality of life and features of social identity maps could be a product of people having a greater number of social contacts, which is known to be associated with better outcomes. Given the potential influence of participants’ symptoms on a given day, this variable was also controlled for in all analyses to reduce the risk of spurious correlations between SIM variables and quality of life. In addition, a mediation analysis was conducted to explore whether any associations between social identity features and quality of life could be explained by self-esteem (Model 4; Hayes & Rockwood, 2017).
Results
The content of social identity maps for individuals experiencing psychosis
Participants reported approximately five groups on their maps (range = 0–18). The names listed on the Post-its fit into 10 response categories: activities (39.56%), family (14.8%), demographics (e.g., ethnicity, gender, nationality; 8.6%), ideology (8.07%), religion (8.07%), friends (5.05%), work (5.05%), patient-related groups (3.03%), politics (2.02%), and local residence (1.01%; for examples of social identity map names within each category, see Table 1). Just under 5% of responses (i.e., 47/992 responses) could not be categorized because what was written was illegible or difficult to interpret (“self,” “Eclipse,” “not too many friends”). Of the five groups listed by each participant, approximately two to three groups were highly important, one to two groups were important, and zero to one groups were less important (for the exact means and standard deviations for the variables, see Table 2).
Means, Standard Deviations, and Correlations Between Participant Characteristics (Time Since Diagnosis, Symptoms, and Social Situation), Number of Groups (Highly Important, Important, and Less Important), Social Contact, Number of Positive Groups Time Since Diagnosis, Self-Esteem, and Quality of Life
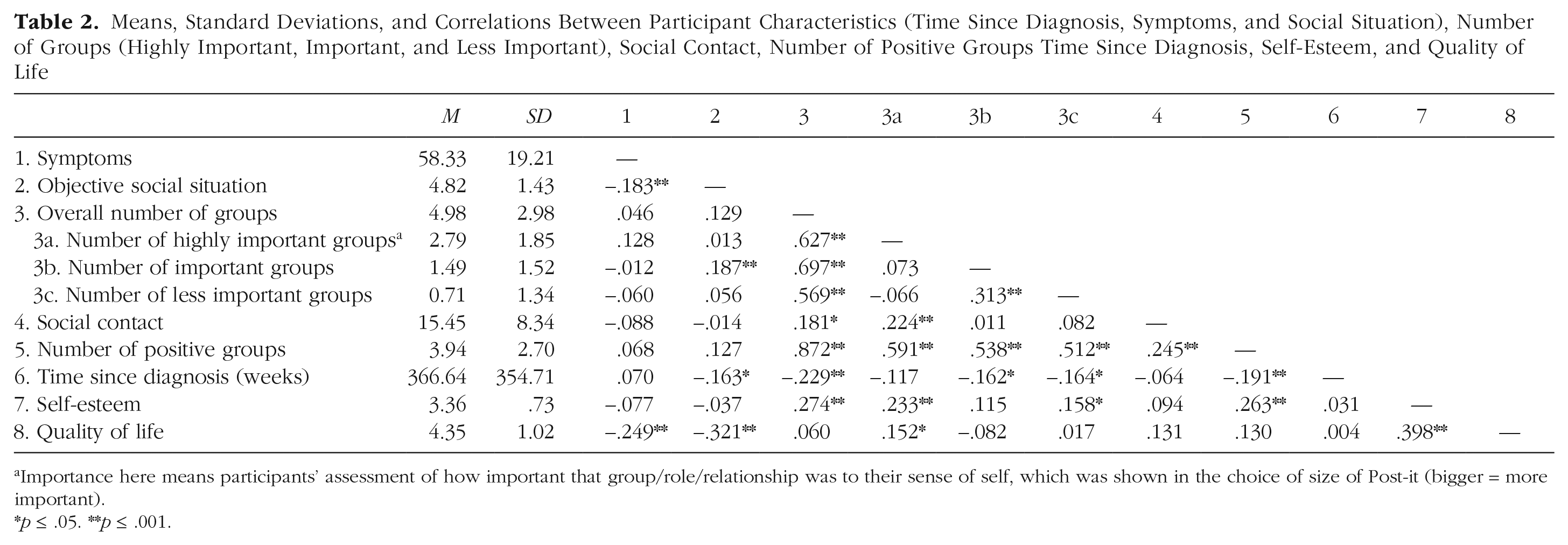
Importance here means participants’ assessment of how important that group/role/relationship was to their sense of self, which was shown in the choice of size of Post-it (bigger = more important).
p ≤ .05. **p ≤ .001.
Relationships between participant characteristics, social identity maps, self-esteem, and quality of life
Pearson’s correlation was used to examine the relationships between participant characteristics, the number of groups, social contact, self-esteem, and quality of life (see Table 2). As might be expected, time since diagnosis was negatively associated with objective social situations: As the weeks since diagnosis increased, objective social situation scores decreased (i.e., participants were more likely to be unemployed, in less independent living situations, and more isolated). Symptoms were also negatively associated with objective social situation: As symptoms increased, objective social situation scores decreased. Both symptoms and social situation, but not time since diagnosis, were negatively associated with quality of life. When considering the aspects of the social identity maps, the overall number of groups was positively associated with time since diagnosis, social contact, and self-esteem but not quality of life or social situation. Note that only the number of highly important groups was positively associated with quality of life. The number of highly important groups was also positively associated with social contact and self-esteem but unrelated to participant characteristics. Both the number of important groups and the number of less important groups were negatively associated with time since diagnosis: As the weeks since diagnosis increased, the number of important groups participants listed and number of less important groups decreased. The number of less important groups was positively related to self-esteem. The number of important groups was unrelated to self-esteem and quality of life.
Predicting quality of life
Hierarchical regression was conducted to examine whether any of the social identity features were associated with quality of life controlling for symptoms and objective social situation. Step 1 included symptoms and objective social situation as control variables. Step 2 included the number of highly important groups as the predictor. The overall model was significant, F(1, 193) = 43.16, p < .001, R2 = .148. After accounting for symptoms and social situation, the number of highly important groups explained an additional 5% of the variance in quality of life, ΔF(3, 194) = 8.99, p = .011, ΔR2 = .048. For a table with standardized and unstandardized betas, see the supplementary material (https://osf.io/ctdhy/).
Next, using PROCESS (Model 4; Hayes & Rockwood, 2017), we conducted a mediation analysis to examine whether self-esteem might help us to explain the relationship between the number of highly important groups and quality of life. There was a significant relationship between the number of highly important groups and self-esteem (a path: b = 0.099, p < .001) and a significant relationship between self-esteem and quality of life (b path: b = 0.527, p < .001). Critically, the relationship between the number of highly important groups and quality became nonsignificant with the inclusion of self-esteem in the model (see Fig. 2). The overall model predicting quality of life was significant, F(4, 195) = 21.18, p < .001, R2 = .30, indicating 30.3% of the variance in quality of life was accounted for by number of highly important groups.
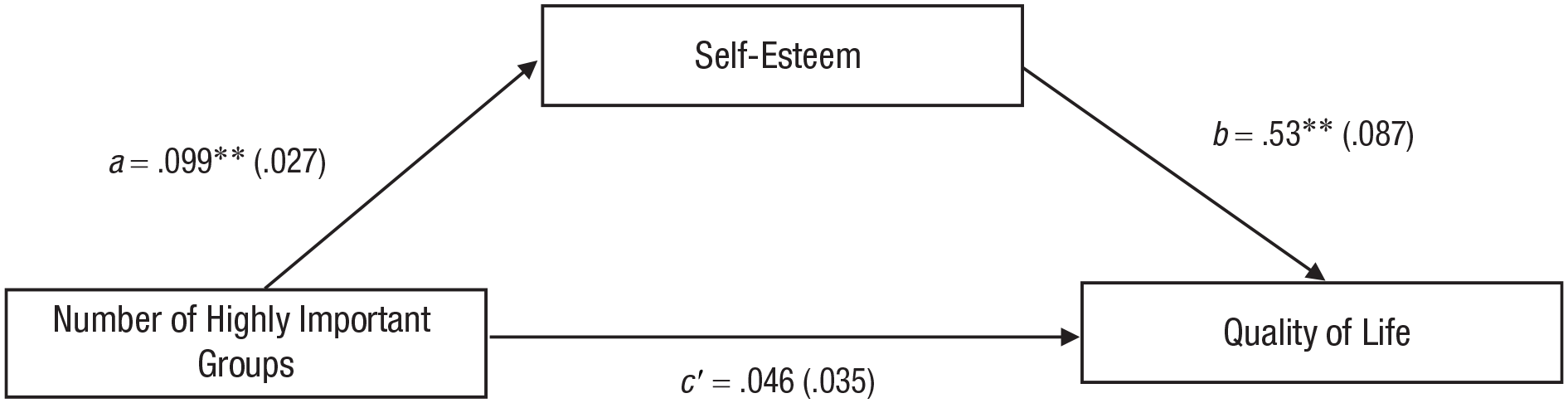
Conceptual model for mediation to explain the relationship between number of highly important groups with self-esteem as the mediator (standard errors in parentheses). *p ≤ .05. **p ≤ .001.
Discussion
The aim of this study was to provide the first examination of the nature of social connections and social identity features and their associations with self-esteem and quality of life among people diagnosed with a psychotic disorder. We used SIM. The SIM tool refers to our varied social connections as “groups” and measures quantitative number of connections and people’s personal appraisal of the connections’, or groups’, significance. Participants are asked to give names to the groups they belong to and indicate how positive the group is and how important it is to their sense of self and how frequently they have social interactions with people in the group. We found that participants reported an average of five groups, of which, two to three were deemed highly important. The most common categories groups fit into were activities, that is, things individuals did, such as gardening or yoga. This category represented 39% of all connections listed. We observed a positive association between the number of highly important groups and quality of life after controlling for symptoms and objective social situation. This suggests that having more social contact alone does not explain the higher quality of life: There may be something separate that makes a difference to quality of life that comes from belonging. No associations were found between other features of social identity maps and quality of life, such as number of positive groups or overall number of groups. Finally, we found that the relationship between the number of highly important groups and quality of life was mediated by self-esteem, suggesting that having highly important group memberships may help individuals to feel more satisfied with their lives because they also help them to feel good about themselves. Our findings broadly align with and extend what would be expected from the SIAH. The findings also align with recent SIAH-informed investigations of subclinical paranoia in the community. Our results emphasize how important it is that future studies take into account the qualitative assessment of personal meaning connected to social interactions. Not all social connections will benefit quality of life in the same way, and a feature of social connections that deserves more study based on our findings is the degree to which people see social connections as important to and strengthening an aspect of their sense of self. Solely increasing the number of social connections people have might not improve quality of life: It may be that social connections that people consider personally meaningful and that furnish people’s sense of self will have a greater impact on quality of life. This is critical information that should be considered in interventions that aim to improve quality of life. This work also highlights areas that require further investigation in working toward a “social cure,” in which one harnesses the benefits in social connections to support quality of life in people with psychosis (summarized in Table 3).
Key Challenges and Priorities for Social Identity Research in Psychosis
Research by McConnell (2011) on self-aspects, or the multiple context-dependent elements that define an individual, suggests that on average, individuals list approximately five self-aspects when asked to describe themselves. Likewise, the present research found that individuals with a psychotic disorder listed about five groups on their social identity maps. The overall number of groups listed by students was slightly higher in previous SIM research (e.g., n = 6.52; Cruwys et al., 2016, Study 1), although the number of highly important groups was similar (n = 2.74 in Cruwys et al., 2016 and n = 2.74 in the present study). That individuals with a psychotic disorder have a similar number of important groups is an important novel finding from our research given that the literature and focus of many interventions are currently primarily trying to increase the overall number of social connections. However, it may be that strengthening existing connections may mean increases in social contacts that do not translate into improvements in people’s quality of life. The finding that people with psychosis list a similar number of groups on social identity maps to other populations is interesting given the substantial evidence suggesting people with psychosis are more likely to be isolated and, on average, have fewer social connections. Researchers should perhaps consider whether existing measures rely too heavily on objective measures of social contact without considering what the measured connections mean to people: These quality indicators may matter more in affecting quality of life than the sheer quantity of connections, which is discussed in more detail below.
There is some evidence for interventions aiming to increasing social contacts being effective (D. Fowler et al., 2018). Social-recovery therapy, a combination of assertive outreach and case management, had the aim of encouraging socially withdrawn individuals back into social environments. The trial showed a significant increase in time spent in structured activities compared with treatment as usual in people with a first episode of psychosis. However, although there was an increase in time doing structured social activities, the effect on symptoms at 15-month follow-up was less clear, in part due to missing data. Researchers should aim to understand whether increase in time doing social activity will have the expected improvement quality of life. The suggestion from the present study’s findings is that it may be that only increasing activity with groups that people see as important to their sense of self would lead to improved quality of life. This study’s findings and the expectation from the SIAH would suggest the latter to be the case, that is, that not all social connections are equal. Furthermore, group-based social connections allow for social identification-building in a way that not all social connections might. This study supports the notion that interventions that seek to build, restore, and sustain social identity-enhancing group-based connections may have a greater effect on mental health than other approaches. Haslam and colleagues (Haslam et al., 2022; Häusser et al., 2020) argued that social identity research may open the door to understanding, preventing, and curing the loneliness epidemic that people, including people with psychosis, are facing. This may be because group-based social connections have a distinct capacity to provide people with a sense of shared meaning, purpose, support, and self-efficacy (Haslam et al., 2022).
Generally, the literature on psychotic disorders points to illness being accompanied by a loss of social connections and increase in the likelihood of isolation and loneliness. In turn, this loss of connections, isolation, and loneliness is associated with worse outcomes and is itself distressing (e.g., Badcock et al., 2021; Chau et al., 2019; Gayer-Anderson & Morgan, 2013; Nevarez-Flores et al., 2022; Palumbo et al., 2015). The participants in this sample had slightly fewer groups but the same number of highly important groups compared with general-population samples (Cruwys et al., 2016). This points to two notable points. First, the number of important connections is not necessarily in exact alignment with number of overall connections, and if the goal is to improve quality of life, it is the way of increasing number of groups that are considered important that should be focused on by researchers and practitioners. Currently, practitioners have no standardized means of distinguishing connections or groups from one another. This means efforts to increase connections, perhaps through social prescriptions, may not take personal significance or degree of internalization into someone’s sense of self into account. SIM may be a useful tool for practitioners to gain a better understanding of what the different social connections mean to their patients.
Second, it may be that the way that social connections are being defined and measured in the psychosis literature may end up missing out on some of the key ways that individuals think about themselves and interact with others after illness. Qualitative accounts have described that many people lose friends or relationships, and associated social identities, when they become unwell. A systematic review synthesizing ways identity change has been understood in the psychosis literature found that loss of roles and relationships was an important way that researchers conceptualize identity change (Conneely et al., 2021). The finding that the number of social connections and social identities is not lower suggests that in addition to changes in people’s sense of self via loss of meaningful roles and relationships, people with psychosis may gain connections, or ways of seeing themselves, after illness. This phenomenon has been observed in other groups who experience a profound change (e.g., Jones et al., 2011). This process of redefinition and potential gain of social identities deserves attention and careful study, reflecting on and questioning assumptions that have become accepted in research circles, for example, about loss of roles and the role of “illness identity” (Conneely et al., 2020; McCay & Seeman, 1998).
Self-esteem mediated the relationship between the number of highly important groups and quality of life. This was a novel finding that is supported by literature in nonclinical samples. Self-esteem has been associated with belonging to positively valued groups and identifying with those groups (Jetten et al., 2015). In the context of people who have not got psychosis but experience (subclinical) paranoia, self-esteem mediated the relationship between paranoia and low mood (McIntyre et al., 2018). Furthermore, social connectedness, measured as social support, was shown to be related to paranoia through self-esteem in people with psychotic-like experiences (Monsonet et al., 2023). It appears that to the extent that individuals feel connected to other people, they feel good about themselves and, in turn, less wary about their social worlds. Taking the findings of the present study together with research on subclinical paranoia and psychotic-like experiences would suggest that targeting social connections may be a fruitful way of improving the self-esteem and satisfaction with life for people with psychosis. More evidence pointing to this can be found in Lim et al.’s (2020) study of a digital intervention, +Connect, targeting loneliness in young people with psychosis, which showed, using a pre-post design, that the intervention reduced loneliness. Feeling connected to others may be a way of targeting the distress associated with psychosis and specifically help remedy paranoia (Lim et al., 2020). Researchers should explore the potential of interventions that take into account personal appraisal of connections, such as the Community Navigator intervention (Lloyd-Evans et al., 2020; Stefanidou et al., 2023) or Groups4Health, in reducing paranoia and other symptoms of psychosis. The Groups4Health intervention has been adapted to different contexts, including to support people in the pandemic (Bentley et al., 2022), people about to retire (La Rue et al., 2024), and people with substance-misuse problems (Beckwith et al., 2019). This study’s successful use of SIM in psychosis suggests Groups4Health could potentially be useful for people with psychosis (Steffens et al., 2021). The findings of this study suggest that interventions that deliberately aim to increase the number of group-based social connections that are considered highly important to people’s sense of self may be a promising way of increasing quality of life.
The negative correlation between time since diagnosis and number of groups is interesting because it suggests that the longer individuals have been contending with their condition, the fewer their connections. People who have experienced psychotic disorders have described the onset of the illness as having a profound impact on their sense of identity through changes in life circumstances and a questioning of what is real (Bayley, 1996; Harewood, 2021; Longden, 2010; Woods, 2011). Psychosis typically develops in adolescence or young adulthood, thereby coinciding with a stage of life when people are working out who they are and typically starting new ventures, studying, working, and establishing relationships (McGlashan, 1988; Rössler et al., 2005). The loss of roles and relationships can reduce how rooted people feel in their social world, and this lack of a sense of belonging is seen as an important source of poor quality of life (Conneely et al., 2021). Research has shown that the longer people have been unwell with psychosis, the smaller their social networks are, and a phenomenon sometimes termed “engulfment in the patient role” can be observed, in which people’s social connections become restricted to family members and health care professionals (Buhagiar et al., 2021; Konsztowicz & Lepage, 2019; McCay, 1995; McCay & Seeman, 1998). Rosenberg (1993) described the “patient role” as one of the few remaining open to a person with a severe mental illness. The patient identity is described as negative but as a useful means to “organize the person’s experience” because it is “better than no identity at all” (Rosenberg, 1993). This attitude may be changing. As discussed above, it appears possible that people may also gain identities throughout their lives, and this is a process that deserves attention, rather than focusing on loss of identities because of external factors that cannot be controlled. The present study showed most connections fit into the category of activities (39%), which are all connections that were chosen identities and accessible at any point in a person’s life. Comparatively fewer people identified patient or illness-related groups (3%). Although time since diagnosis was negatively associated with overall number of groups, it was not negatively associated with number of highly important groups. General-population research has also shown a reduction in overall number of groups with increasing age that is not necessarily accompanied by a reduction in well-being (Bruine de Bruin et al., 2020). This selective narrowing of social networks and social identities may also take place in the context of psychosis, and the loss of social contacts and group memberships might not result in reduced quality of life if it is not also related to a reduction in the groups that are important for making sense of one’s sense of self.
Measurement of social identification
Research conducted as part of a clinical-psychology doctoral thesis found that social identification was negatively associated with paranoia and schizotypy in a sample with psychotic experiences, some of whom had received a diagnosis of psychosis. H. Cooper (2022) found that the strength of this association depended on the type of social identity, with friend groups showing a stronger association than social identities such as ethnicity. Further research should explore this way of considering social identities and compare the findings with the constructs used in the SIM approach. The findings of this study generally align with H. Cooper’s findings insofar as the slightly different approaches can be compared. Across both studies, people described many groups that could be classed as “chosen”: friend groups and activity groups. Fewer groups in the current study were groups that might be considered unchosen, categorized as “patient” (3%) or “demographic” (9%), for example.
Some support for SIM’s ecological validity can be found in comparing it with different measures of social identification, which show similar numbers in participants with autism (Maitland et al., 2021) and with student samples (Cruwys et al., 2016) using slightly different approaches to capturing importance. This is also true in studies using different ways of measuring importance; Maitland and colleagues’ (2021) participants were asked to rate how much they identified with a group on a 7-point scale, and rating above 5 was used as the cutoff for a group to count as a social identity, that is, as a group that people identified with and felt a sense of belonging to. The range of social identities participants could have was between 0 and 4. Although different approaches to measurement were taken in Maitland’s et al.’s study and in the current study, the number of groups that were considered highly important to participants’ sense of self was similar (two to three). The similarities across groups using the same measures are a reassuring indicator that the tool was used and understood in a similar way. Further support for the measurement of social identity features using SIM can be found in research investigating SIM using a qualitative approach. Hogg and colleagues (2022) found participants with psychosis described the group memberships as significant contributors and essential for well-being, as did McNamara and colleagues in a study of patients from transition from child mental-health services to adult mental-health services (McNamara et al., 2017, 2021; McNamara & Parsons, 2016).
Limitations and future directions
An important limitation of the present research is the cross-sectional nature of the design. This means that although a direction of the associations identified between number of highly important groups, self-esteem, and quality of life is posited, it cannot be tested. This study is correlational, and causation cannot be inferred. The direction of association could be bidirectional or in the opposite direction to that tested in the mediation model: It is possible that having higher self-esteem is associated with seeing groups as highly important and even that better quality of life is then associated with higher self-esteem. The likelihood is that there is a bidirectional association, and virtuous and vicious cycles at play. The virtuous cycle might be that belonging to more groups improves both self-esteem and quality of life, which, in turn, makes it easier to interact with people and further increase and strengthen social connection. This should be tested because the cross-sectional design of our study could not test this. However, there is some support for the direction of associations proposed in Figure 2 from existing research. Jetten and colleagues (2015) followed a sample of students over a year and showed that increasing the number of groups participants were members of, and might therefore derive a sense of social identification from, was associated with improved self-esteem and through improving self-esteem, improved their well-being (Jetten et al., 2015).
Future research may wish to examine the types of social connections (e.g., activities, family, demographics) and how these may be related to different outcomes. A narrative synthesis found stronger evidence for direct associations between small-group social identities (e.g., friendships, family) and psychosis-related experiences and indirect associations for larger group social identities (e.g., ethnic identities; H. Cooper, 2022). Here, a particularly strong inverse relationship was found between friend-group identity and paranoia. In the current study, few of the groups were categorized as “friend” groups. It is possible that some of the activities groups listed would also have involved friends but were not named as such. Future work should examine whether certain types of social identities confer greater benefit than others on quality of life. It would be interesting to explore how identification with an illness identity, or “psychosis” identity, might be related to quality of life. Few of the groups listed were related to illness (3%), which contrasts strongly with the large space that this concept takes up in research about psychosis (Conneely et al., 2021). Much of the work in psychiatric or neurodiverse populations into identity focuses on identification with that group (e.g., autism identity, substance abuse/user identity; Cruwys et al., 2014; Jetten et al., 2015; Johnstone et al., 2015). Research should be led by how people are describing themselves and the groups they see as important to them instead of assuming which groups are likely to be important. This might increase the likelihood of interventions succeeding in harnessing the benefits of social connection.
Future research should investigate how belonging to a stigmatized group affects individuals with psychotic disorders given that previous studies have shown the detrimental effects of stigma on well-being (Puhl & Brownell, 2006). Individuals often attempt to mitigate the negative impact of low-status group membership by distancing themselves from the group (Deaux & Ethier, 1998; Swann, 1987; Ting-Toomey, 2015), and conflicts between identities may further reduce quality of life (Jones et al., 2011; Jones & Hynie, 2017). People with psychosis are placed in a highly stigmatized group (Sass, 2007; Taskin et al., 2003; Thornicroft et al., 2010; Thornicroft & Kassam, 2008), a new group that likely conflicts with other aspects of their identity (Woods, 2011, 2013, 2015). Future research should explore how compatibility between group identities influences quality of life and relationships with other social identity features. Psychological interventions targeting stigma and reframing the psychosis identity may alleviate negative associations with belonging to illness-related groups and may be fruitful to incorporate into social interventions targeting psychosis (Woods, 2011, 2013, 2015).
This study underscores that solely focusing on a psychosis identity overlooks significant aspects of self-perception. Although positive appraisal of the group may improve quality of life and mental health, the highly stigmatized nature of psychosis diagnosis and internalized stigma negatively affect outcomes (Alexova et al., 2019; Roe et al., 2004; Wood et al., 2016, 2017, 2018). Clinical interventions should address self-stigma and identification with the illness group concurrently because reframing perceptions of psychosis may tap into positive psychological resources associated with group membership. These efforts should also be accompanied by attempts to reduce public stigma. Future research should examine the positivity or negativity of group identities in the social identity maps of individuals with psychosis.
Clinical implications
The present findings have implications for clinical practice, in particular, social prescribing and therapy. Social prescribing aims to improve health and quality of life through connecting individuals with community-based activities. In its simplest form it is a signposting usually to third-sector organizations or activities. It can also take a more involved support to enable community engagement. Social prescribing is currently used by primary care practitioners in the United Kingdom as part of the NHS long-term universal personalized care plan (NHSEngland, 2020). The results of this study suggest that social prescribers should consider, with the person who is receiving the prescription, whether the prescription is likely to lead to a new social connection or the strengthening of an existing social connection. An example of this can be found in the Community Navigator Programme, an intervention that aims to increase connections with local community, which considers the personal meaning and potential for social identification. The intervention is currently being tested in a large randomized controlled trial to reduce feelings of loneliness in people with treatment-resistant depression (Stefanidou et al., 2023).
In therapeutic conversations, clinicians could consider the significance of different social connections for people’s sense of identity (Conneely et al., 2024). Despite recognizing its importance, most clinicians feel ill-equipped to address identity-related issues with patients (Ben-David et al., 2021). Training, possibly drawing from interventions such as Groups4Health, could bolster clinicians’ confidence and elucidate the therapeutic value of social connections and identification with various groups (Cruwys et al., 2022). Encouraging clinicians to inquire about how patients perceive themselves within their social context and how different aspects of their lives contribute to their identity may prompt beneficial interventions, aligning with a recovery-oriented care approach (Law & Morrison, 2014). An increase in social contacts may not necessarily enhance one’s sense of belonging if acceptance within a group is lacking. Exploring how individuals with psychosis perceive themselves within their social environment remains a crucial yet underexplored aspect of achieving better well-being. Social identity maps offer a structured means to explore various aspects of identity, from group affiliations such as religious or recreational groups to personal activities, thereby facilitating meaningful conversations about what truly matters for someone’s recovery. The use of SIM could thus facilitate the enacting and implementation of a recovery-oriented approach in clinical practice for individuals with psychotic disorders (Bentley et al., 2020; Cruwys et al., 2016). Although symptoms persist for many people with psychosis, most services aim to foster recovery by promoting connectedness, hope, identity, meaning in life, and empowerment (Leamy et al., 2011). A strength of the SIAH and the use of SIM is that it is resource-oriented: Rather than looking at the lack of social contacts and social isolation, this approach considers what people do have and can do and the positive sequalae of internalization and belonging.
Key challenges for research
A key challenge for research going forward is to integrate ways of measuring both number of social connections and the quality or personal significance/meaning attached to those social connections. Qualitative research has described personal meanings of relationships and the impact psychotic symptoms had on people’s sense of self and social connections and the role social connections and belonging play in working toward recovery (McCarthy-Jones et al., 2013; Noiriel et al., 2020). Quantitative studies have shown an association between number of social connections and better quality of life in psychosis and the general population (Gayer-Anderson & Morgan, 2013; Holt-Lunstad et al., 2015; Palumbo et al., 2015). These bodies of research are separate, and as a result of their being explored using different methods, very little is known about how the combined number of high-quality/personally important social connections is related to quality of life. Using SIM appears a feasible option to combine quality and quantity. Future research using longitudinal designs should be carried out to better understand the direction of associations identified in this study, and identity-building interventions should be adapted and tested for people with a psychotic disorder. Research on social connectedness and loneliness should include social identity as a process variable. Key challenges and priorities for research examining social identity in psychosis are highlighted in Table 3.
Conclusion
This study is the first to use SIM among individuals with a psychotic disorder, showing a feasible means to quantify and explore meanings attached to social connections. The use of SIM generated novel insights, and the results generally support expectations from the SIAH. We found a cross-sectional association: The more highly important groups people listed on their social identity map, the better their subjective quality of life was, controlling for symptoms and objective social situation. In other words, it appears that it is not just the size of the social circle that matters but also the presence of deeply important connections. Social identity maps allow for the benefits that come from quantitative inquiry (e.g., standardized statistical tests, easy comparison, and the potential for meta-analysis) to be combined with the strengths of a qualitative approach: Social identity maps are “self-exploratory, self-created, and empowering” (Cruwys et al., 2016). The present findings suggest a need for the disciplines of psychiatry and psychology to consider how people see their social connections in relation to themselves: The internalization of social connections into people’s sense of who they are, through identification, may be an important part of how social connections affect health and well-being.
Footnotes
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions