
Abstract
Natural language processing (NLP) is a subfield of machine learning that may facilitate the evaluation of therapist–client interactions and provide feedback to therapists on client outcomes on a large scale. However, there have been limited studies applying NLP models to client-outcome prediction that have (a) used transcripts of therapist–client interactions as direct predictors of client-symptom improvement, (b) accounted for contextual linguistic complexities, and (c) used best practices in classical training and test splits in model development. Using 2,630 session recordings from 795 clients and 56 therapists, we developed NLP models that directly predicted client symptoms of a given session based on session recordings of the previous session (Spearman’s ρ = .32, p < .001). Our results highlight the potential for NLP models to be implemented in outcome-monitoring systems to improve quality of care. We discuss implications for future research and applications.
Psychotherapy represents a class of mostly conversational treatments focused on behavior change or reduction of client distress. The primary goal of research on psychotherapy is to determine what sorts of conversations are most associated with the desired change. However, it has proven quite difficult to make consistent predictions about the outcome of psychotherapy from the content of the conversation (e.g., Webb et al., 2010). Client ratings of the therapeutic relationship consistently predict response to treatment but are distal to the session itself and place a burden on clients to repeatedly rate their experience. Our work focuses on evaluating machine-learning-based technology to make predictions about client-symptom change directly from the recording of a session.
Measurement-based psychotherapy relies on obtaining clinically meaningful information from clients, observers, or therapists based on process and outcome ratings. In measurement-based care (MBC), therapists use client ratings to guide discussion regarding treatment goals and approach (Fortney et al., 2017; Goldberg et al., 2018; Lewis et al., 2019; Scott & Lewis, 2015; Shimokawa et al., 2010). Likewise, psychotherapy research has relied on client, therapist, and observer ratings of clinical processes to predict client outcomes. For example, researchers have used therapist and client self-report measures to assess factors such as therapeutic alliance (Flückiger et al., 2018) and multicultural competency (Tao et al., 2015). Likewise, researchers have used behavioral coding to examine therapist adherence to specific interventions (Webb et al., 2010) and emotional expression (Elliott et al., 2011). Although traditional MBC generally has increased feedback on therapeutic processes and quality of care, methodological issues continue to limit therapists receiving feedback on client outcomes based on clinical interactions. Clients are often asked to retrospectively rate their experiences in sessions; consequently, client ratings may be more indicative of their general experiences in therapy rather than specific interactions with therapists. Therapist self-report measures similarly do not provide information on how specific therapist–client interactions drive client outcomes and are often less correlated with outcomes than client self-report ratings (e.g., Elliott et al., 2011; Tao et al., 2015). Observer ratings of sessions can provide valuable insight into how therapist–client interactions inform client-symptom improvement, but behavioral coding is often costly and time intensive (e.g., Moyers et al., 2003). Implementing routine outcome monitoring in large health-care systems also results in increased time burdens for clients to complete measures and therapists to collect data. Given current limitations in assessment of therapeutic processes, alternative methods of predicting client-symptom improvement directly from therapist–client interactions are needed to scale up research on how therapist behaviors decrease client distress and facilitate provision of feedback to therapists in a manner that minimizes client and therapist burden.
Natural language processing (NLP) is a powerful alternative to traditional methodologies that rely on self-report measures and behavioral coding to assess client outcomes and therapeutic processes. NLP is a subfield of machine learning (ML) that integrates linguistics and computer science to automatically make statistical predictions based on patterns in large bodies of text (Hirschberg & Manning, 2015; Jurafsky & Martin, 2014). NLP techniques derive these predictions by converting text into smaller units (e.g., phrases, sometimes called “n-grams”), assigning quantitative metrics to units of text, and examining how patterns in these quantitative metrics are associated with specific outcomes of interest (e.g., topics, interventions, emotion, changes in symptoms). NLP classification models are particularly useful because they analyze large bodies of text in relatively short time periods; efforts to manually analyze the same bodies of text using traditional coding methods would be slower and require extensive human resources. NLP technologies have been used in wide-ranging applications, from detecting urgency in spoken utterances (Landesberger et al., 2020) to examining themes in poetry (Kao & Jurafsky, 2012).
NLP classification has been leveraged to describe and predict therapeutic processes directly from the words spoken by therapists and clients rather than rely on client, therapist, or observer ratings of clinical processes. For example, topic models have been used to automatically assess motivational-interviewing fidelity (Atkins et al., 2014) and classify types of psychotherapy treatment used by providers (Imel, Steyvers, & Atkins, 2015). In addition, NLP models have been used to predict the sentiment of therapist and client statements (Syzdek, 2020; Tanana et al., 2016, 2021). Furthermore, NLP has shown promise in predicting therapeutic processes such as therapist empathy (Xiao et al., 2012, 2015) and therapeutic alliance (Goldberg et al., 2020).
Past application of NLP-based tools to identify therapeutic processes suggests that NLP models can be similarly used to automatically predict client-symptom improvement from in-session content. NLP-based tools that predict client outcomes have the potential to be implemented in large health-care systems to automatically monitor symptoms directly from session data rather than relying on self-report measures that increase burden on clients and therapists. Three recent studies have used computationally derived ratings of important therapeutic processes to predict treatment outcomes. Ewbank et al. (2020) applied a deep-learning model to classify therapist messages during an Internet-enabled text-based cognitive-behavioral therapy delivered via synchronous messaging (n = 17,572). They grouped therapist messages into categories (e.g., use of change methods, arranging next session) and found several features had small associations with treatment improvement, including use of change methods and therapeutic praise (ORs = 1.11 and 1.21, respectively). In a sample of 729 psychotherapy sessions, Shapira et al. (2021) found that lower frequency of negative emotion words (using a predefined dictionary) in a given session was associated with lower distress at the subsequent session. In addition, a decline in first-person singular words was associated with pretreatment to posttreatment improvement. Finally, Atzil-Slonim et al. (2021) applied topic models to transcripts of 873 sessions and used model-derived topics to examine how changes in topics of conversation between therapists and clients predicted symptom change; they found that increases in topics associated with higher client functioning were associated with greater symptom improvement.
Ewbank et al. (2020), Shapira et al. (2021), and Atzil-Slonim et al. (2021) demonstrated the promise of using session content to not only scale up the evaluation of session content but also derive important metrics to predict outcomes. Application of NLP models to identify therapist interventions and emotional valence allows for more detailed understanding on a large scale of how these components inform client change. At once, these studies could be further methodologically strengthened. First, past studies used NLP models to first label therapist–client interactions and then used separate analyses to correlate client outcomes with the labels rather than raw text. Directly predicting client outcomes from therapist–client interactions may capture more nuanced linguistic patterns that are important to client-symptom change but uncaptured through the particular human-conceived labels. Topic-modeling approaches, such as those used in Atzil-Slonim et al. (2021), are effective in identifying interpretable text patterns without relying on prior human-conceived schemes; however, topic models often do not take into account nuanced meaning and context in text that can affect the topics that are generated (Barde & Bainwad, 2017).
Second, previous studies developed NLP models that used dictionary-based and word2vec methods to identify labels of interest; recent models incorporate more contextual information that could improve measurement of client symptoms. NLP researchers have recently developed more advanced models such as Bidirectional Encoder Representations from Transformers (BERT; Devlin et al., 2019) that account for (a) more information from text corpora of interest and (b) language-specific complexities (e.g., shifts in word meaning based on context). Models such as BERT have been found to exceed performance of older models that use dictionary-based methods and word2vec (Dai et al., 2019; Konstantinov et al., 2021). Third, Ewbank et al.’s (2020) models were applied to text-based therapy, and similar models may benefit from being trained on spoken-language interactions. Although text-based therapy can be effective in reducing client distress (Aguilera et al., 2017; Marcelle et al., 2019), interventions provided via text may unfold differently compared with traditional spoken interventions. Furthermore, the vast majority of mental-health care remains delivered via spoken language, which presents a number of additional analytic complexities related to speech processing. Fourth, previous studies did not apply classical ML test-train splits to evaluate model accuracy in predicting outcome. ML researchers typically train and test models on distinct subsets of their data to ensure that final model-evaluation results are not due to models identifying outcomes based on unique features in the data (Jurafsky & Martin, 2014). Using the same sample for testing and training could result in models that are overfitted to the primary text corpora and perform poorly in other text corporas. Finally, Shapira et al. and Atzil-Slonim et al. used text generated by human transcribers; the application of models derived from human transcriptions (which take longer than a client simply filling out a symptom measure) could be strengthened with the use of automated transcriptions. Recent advances have improved automated transcription of recordings through automated speech recognition whereby NLP tools quickly segment and convert therapist and client speech into text. Although there may be some error in how NLP tools convert speech to text, application of NLP tools to transcribe session recordings allows for examination of therapist–client interactions on much larger scales. Reliance on human-generated transcripts is time-consuming and significantly limits the scalability of researching how session content informs client improvement. Thus, evaluations of NLP to predict treatment outcomes directly from recordings are warranted.
Purpose of the Study
The use of NLP methods to predict treatment outcomes directly from clinical encounters has numerous practical applications, including supporting quality-assurance efforts, providing feedback to providers, and enriching research efforts seeking to link elements of clinical interactions to treatment effects. Indeed, NLP-based predictions of treatment outcome directly from session recordings could help augment the otherwise limited objective feedback that is routinely available to clinicians providing psychotherapy (Tracey et al., 2014) while minimizing time burden on clients. However, to date, there are limited studies that have used transcripts of therapist–client interactions as direct predictors of client-symptom improvement. Furthermore, previous applications of NLP models to prediction of client outcomes were limited by (a) reliance on models that do not take into account contextual linguistic features, (b) applications to text-based psychotherapy, and (c) lack of differentiation between training- and test-data samples. To address limitations in past NLP research in predicting client symptoms, we developed and evaluated NLP models that automatically predicted client-symptom ratings of a given session based on transcripts of their previous therapy session using 2,630 transcripts of therapy sessions from 795 clients and 56 therapists. Based on best practices in NLP research, we used separate training, validation, and test samples of transcripts of therapy sessions (Jurafsky & Martin, 2014).
Transparency and Openness
Preregistration
The current study was not preregistered.
Data, materials, code, and online resources
We are unable to provide access to our data and analysis script because our data set comprised transcripts of therapy sessions. Clients in our sample did not consent to having their data made available to the public. Our analysis script was tailored to our data set.
Reporting
This study involved an analysis of existing data rather than new data collection.
Ethical approval
This study was approved by the University of Utah’s Institutional Review Board (Protocol No. 00083132) and was carried out in accordance with the provisions of the World Medical Association Declaration of Helsinki.
Method
Overview of text corpora
Our data consisted of 2,630 recordings from individual counseling sessions at a large university counseling center. Recordings were collected as part of a National Institutes of Health-funded grant (2 R01 AA018673). Transcripts were generated from recordings using a combination of Kaldi (Povey et al., 2011), a speech recognition tool kit, and another set of models specifically tuned to the language used in psychotherapy, which we refer to as the "speech pipeline" (for details on the speech recognition, diarization, role assignment, and voice-activity detection systems, see Flemotomos et al., 2022). Sessions in which both therapists and clients consented to have their sessions recorded were processed with the speech pipeline. We analyzed only sessions in which client-symptom ratings were available for the next session. Processing steps involved voice-activity detection (e.g., identifying whether someone is talking), diarization (e.g., identifying whether the speaker was the client or therapist), and transcription of audio to text (e.g., automated speech recognition).
To create our sample of training and test transcripts, we randomly assigned clients into training, validation, and test sets so that roughly 80% of the transcripts were in the training set, 10% were in the validation set, and 10% were in the test set. Percentage allocation of transcripts to training, validation, and test sets were based on standard NLP practices to balance (a) maximizing the amount of data that models are trained on to learn various patterns in text and (b) allowing for varied validation and test sets to adequately assess model performance (for more information, see Jurafsky & Martin, 2014). Clients could be part of only one set. For example, a client who was assigned to the training set could not be in the validation or test set. We were unable to randomize transcripts at the therapist level because of the relatively smaller number of therapists in our sample. Consequently, therapists could have concurrently been included in the training, validation, and test sets. Overall, 2,044 transcripts were assigned to the training set, 314 transcripts were assigned to the validation set, and 272 transcripts were assigned to the test set.
Participants
Client demographics
Our sample consisted of 1,002 clients. Regarding racial-ethnic identity, 74.2% identified as White, 8.4% identified as Latinx, 8.3% identified as Asian American, 5.6% identified as multiracial, 1.6% identified as African American/Black, and 2.0% self-identified their racial-ethnic identity. Regarding gender, 55.2% identified as cisgender women, 40.8% identified as cisgender men, and 3.4% self-identified their gender identity (e.g., transgender man, transgender woman, gender queer). Regarding sexual orientation, 70.9% identified as heterosexual/straight, 12.2% identified as bisexual, 5.7% indicated they were questioning their sexual orientation, 5.2% identified as gay, 3.3% self-identified their sexual orientation (e.g., pansexual, demisexual), and 2.6% identified as lesbian. Regarding religious and spiritual identity, 27.4% identified as members of the Church of Jesus Christ of Latter Day Saints, 14.8% self-identified their religious and spiritual identity, 13.8% identified as atheist, 12.1% identified as Catholic, 11.5% identified as agnostic, 5.8% identified as spiritual but not religious, 3.3% preferred not to disclose their religious and spiritual identity, 3.2% identified as Protestant, 2.3% identified as Buddhist, 1.9% identified as Jewish, 1.9% identified as Lutheran, 1.7% identified as Hindu, and 1.3% identified as secular. The average age of clients was 23.3 years (SD = 4.7), and client ages ranged from 18 to 54.
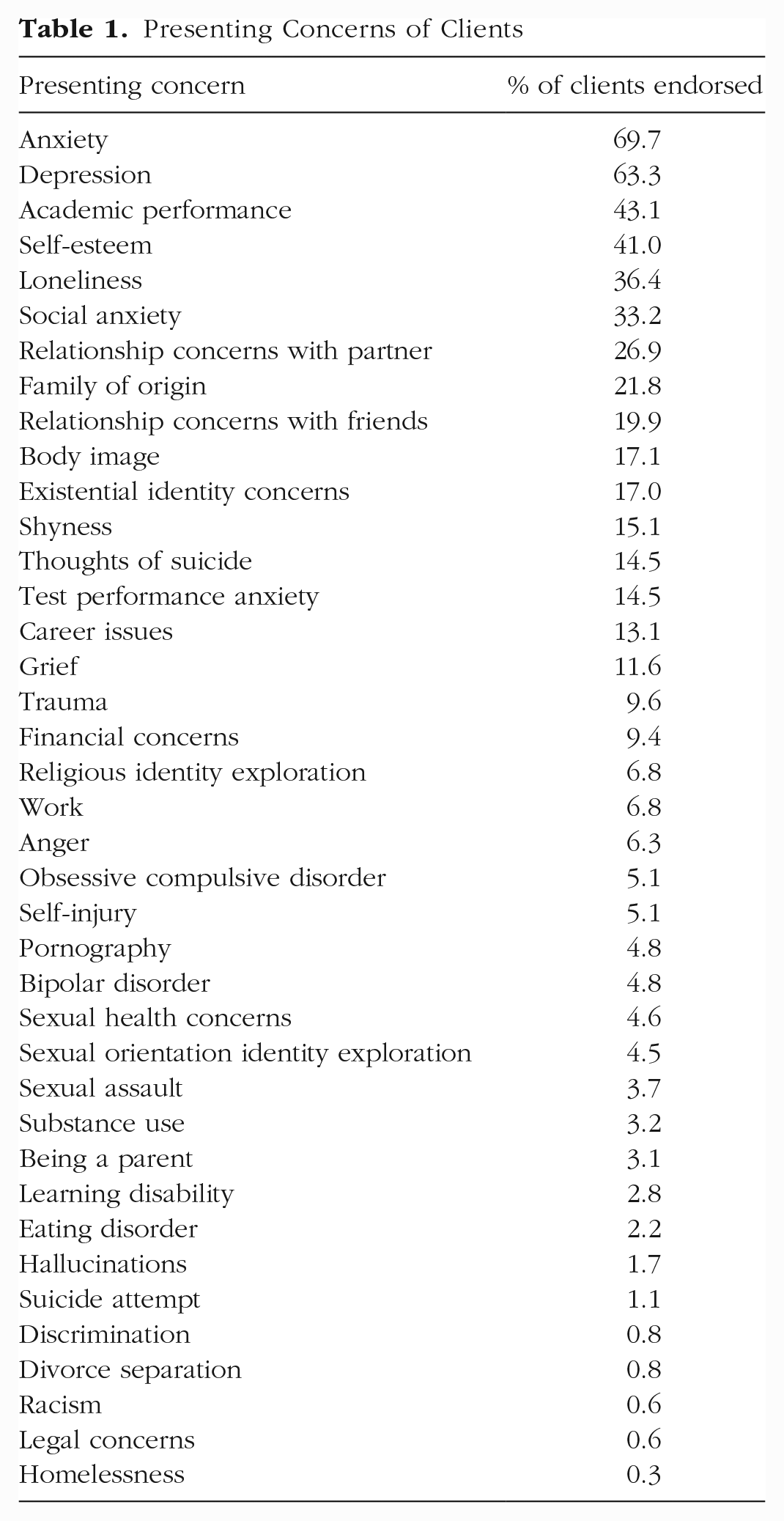
Table 1 presents the percentage breakdown of all presenting concerns endorsed by clients in our sample. The top 10 client-presenting concerns were anxiety (69.7%), depression (63.3%), academic performance (43.1%), self-esteem (41.0%), loneliness (36.4%), social anxiety (33.2%), relationship concerns with partner (26.9%), family of origin (21.8%), relationship concerns with friends (19.9%), and body image (17.1%).
Presenting Concerns of Clients
Therapist demographics
Our sample consisted of 56 therapists. Regarding racial-ethnic identity, 62.8% identified as White, 11.9% identified as Asian, 4.8% identified as Black, 4.8% self-identified their racial-ethnic identity, and 2.4% identified as multiracial. Regarding gender identity, 63.4% identified as female, 31.7% identified as male, and 4.9% identified as gender-queer. Regarding sexual orientation, 64.2% identified as heterosexual/straight, 14.2% self-identified their sexual orientation, 9.5% identified as bisexual, 7.1% identified as lesbian or gay, 4.6% indicated they were questioning their sexual orientation, and 2.4% did not disclose their sexual orientation. The average age of therapists was 32.2 years. Therapists consisted of psychologists, social workers, psychology and social-work interns, and psychology and social-work practicum students. Therapists in our sample used a variety of psychological interventions stemming from cognitive-behavioral-therapy, interpersonal, psychodynamic, and feminist-multicultural frameworks.
Measures
Client demographics questionnaire (Standardized Demographic Set)
The client demographics questionnaire (Standardized Demographic Set [SDS]) is administered to all clients before their intake session and includes information pertaining to client cultural identities (e.g., race/ethnicity, gender, sexuality, religion, nationality, and ability status). The SDS also gathers information regarding the client’s family, mental-health treatment, and substance use histories. The SDS is used by university counseling centers that are affiliated with the Center for Collegiate Mental Health and was developed from feedback from more than 100 counseling centers. The SDS is revised each year to be as comprehensive and inclusive as possible.
College Center Assessment of Psychological Symptoms-34
The College Center Assessment of Psychological Symptoms-34 (CCAPS-34; Locke et al., 2012) is the primary outcome measure in our study and is a 34-item self-report measure assessing symptoms across a broad range of symptoms among university students. The CCAPS-34 is a subset of the larger CCAPS-62 scale and is measured on a 5-point Likert scale ranging from 0 to 4. The CCAPS-34 consists of seven subscales—depression, generalized anxiety, social anxiety, academic distress, eating concerns, hostility, and alcohol use; the CCAPS-62 subscale contains an extra subscale assessing family stress. Cut scores indicating elevated distress are 1.70 for depression, 1.70 for generalized anxiety, 2.50 for social anxiety, 2.40 for academic distress, 1.80 for eating concerns, 1.43 for hostility, and 1.40 for substance use. In addition to the subdomains, the CCAPS-34 also generates a distress index that incorporates items across subscales to assess general distress of clients; we used the distress index as our primary outcome, and the cut score for the distress index is 2.15. Higher scores on the distress index indicate greater overall distress. Sample items in the CCAPS-34 include “My heart races for no good reason” and “I don’t enjoy being around people as much as I used to.” The CCAPS was normed on a sample of 448,904 university students across the United States and has strong evidence of convergent validity with other measures assessing specific distress domains and high test-retest reliability (0.78 to 0.91; Locke et al., 2011). Internal consistency of CCAPS subscales range from 0.78 to 0.91. In our sample, the CCAPS-34 is administered to clients before the start of every session.
Statistical Analyses
Preprocessing and feature extraction
We prepared transcripts for analyses (e.g., preprocessing) by exporting each of the psychotherapy sessions into text documents that could be read by NLP models; speaker labels for therapists were indicated by “T:,” and clients were indicated by “P:” (e.g., “T: How were you feeling today. C: I am feeling a little depressed. T: I am sorry to hear that.”). After preprocessing transcripts, we extracted text for analyses (e.g., feature extraction) using the default Robustly Optimized BERT Pretraining Approach (RoBERTa) byte-pair encoding, which breaks down a sentence into words and word pairs. This algorithm strikes a balance between word-based language models and character-based language models (Sennrich et al., 2015). The vocabulary for the byte-pair encoder was 50,000. All inputs are wrapped in the standard starting and ending tags for RoBERTa (“<s>” and “</s>”). We also standardized all raw symptom scores to help stabilize error propagation in the models. Given our interest in developing tools that could independently predict client symptoms from transcripts of therapy sessions in a context in which client ratings are not available, rather than examining the causal importance of therapist–client interactions in predicting client outcomes, we did not use client symptoms as predictors in our models. Furthermore, content of therapy sessions is intertwined with client symptoms (e.g., shifts in distress could be due to content that is discussed during sessions, and session content may also be informed by current symptoms). Consequently, including client symptoms as predictors in our models could unintentionally result in models that are statistically overcontrolled, removing true statistical signal that is related to symptom ratings.
Overview of models
We used RoBERTa (Liu et al., 2019) as our primary representation of the text. RoBERTa is a transformer neural network that can take sentences or paragraphs and output numeric vectors that can then be used for other prediction tasks. Neural networks are ML algorithms that are broadly modeled after human neuron connections and are composed of nodes (e.g., computational units) separated into an input, hidden, and output layer (Jurafsky & Martin, 2014). Nodes in the input layer transmit predictor information to nodes in the hidden layers, which detects and uses patterns in the text to make predictions that are ultimately transmitted to the output layer. RoBERTa is pretrained on a corpus of 160 GB of English text to predict words hidden from the model. The pretrained model was downloaded from the Huggingface repository (https://huggingface.co/). We used the base-English pretrained model, which has 355 million parameters (hidden nodes of 1,024; 16 attention heads that change weights assigned to features based on observed patterns; and 24 layers). The base model was used rather than the large model to limit the amount of computer memory used for each training example.
One of the major challenges with using transformer-based models for analyzing entire psychotherapy sessions is that computation complexity (and memory requirements) increases exponentially as the length of the inputs increase. Generally, there is a limit of 1,024 input words or word parts, whereas 50-min psychotherapy sessions typically range from 10,000 to 20,000 word parts. To solve this issue, we broke sessions down into chunks with maximum lengths of 1,024. We extracted the output above the classifier token (“<s>”) from each chunk. This left us with a variable-sized matrix of (Hidden Size × Number of Chunks). We initially experimented with two different methods for simplifying this variable-sized matrix into a standard-size vector: average-pooling and max-pooling. Average-pooling simplifies the matrix by calculating the average values of numeric outputs across layers, whereas max-pooling calculates the maximum value numeric outputs across layers. Initial piloting suggested that the max-pooling strategy provided the best performance. After max-pooling, we were left with a 1,024-length vector. We then added a continuous layer that reduced the vector into a single, continuous prediction.
All models were trained using the Adam optimizer (Kingma & Ba, 2014), and we used mean square error loss for the final outcome prediction. We used the validation set to tune the learning rate (e.g., parameter that controls model adjustments based on estimated errors) and tested the best model on the test set. We used pytorch and the Huggingface framework to train all models. Models were trained on an Nvidia Quadro 8000 with 48 GB of computer memory. We tuned the number of epochs (e.g., number of times the model reviews the training set and updates model parameters) using the validation set. We used Spearman’s ρ as our main measure of model performance because the outcome variable was not normally distributed and we were interested in how well our model ordered clients compared with their own symptom reporting. We also report R2 as a measure of absolute performance on the test set (this version of R2 can be negative because we did not fit any parameters to the test set).
In addition, we used an n-gram term frequency, inverse document frequency (TF-IDF) model with a regularized linear regression model (for more information on this model see Goldberg et al., 2020). This model is a simple statistical model that predicts a continuous outcome from counts of words and phrases (called n-grams). TF-IDF examines how the presence of specific words in the text corpora contributes to relevant outcomes of interests; words in TF-IDF models are given less weight if they frequently occur across documents in the text corpora. For example, words such as “the,” “it,” and “and” would be given less weight because they frequently occur across therapy sessions and consequently would not help models differentiate between different sessions. For these analyses, we used the open source sklearn tool kit in Python.
Results
Client-outcome scores at the start of treatment on the CCAPS-34 ranged from 0 to 3.45 (M = 1.75, SD = 0.70), and client-outcome scores at termination ranged from 0 to 3.9 (M = 1.29, SD = 0.75). Overall client-outcome scores ranged from 0 to 3.9 (M = 1.69, SD = 0.72). Regarding baseline severity of clients across CCAPS-34 subdomains, mean baseline scores were 1.60 for depression, 1.89 for generalized anxiety, 2.05 for social anxiety, 1.99 for academic distress, 0.79 for eating concerns, 0.66 for hostility, and 0.35 for substance use. Clients in our sample attended on average 8.06 sessions (SD = 3.68), with treatment length ranging from two to 24 sessions. Approximately 87.1% of clients terminated treatment below the clinically significant distress index cutoff score, and 49.3% of clients terminated treatment below the low distress index cutoff score. About 24% of clients achieved reliable change at termination. Cohen’s d values between the first and last observed CCAPS ratings were −0.53 for overall distress, −0.34 for depression, −0.33 for generalized anxiety, −0.22 for social anxiety, −0.23 for academic distress, −0.11 for eating concerns, −0.24 for hostility, and −0.12 for substance use.
Symptom prediction
The average number of words in each transcript was 6,997.30 (SD = 1,819.12) and ranged from 19 to 15,526. Across all transcripts, there were 43,234 unique word tokens. We examined learning rates ranging from 1e-5 to 1e-10 using the validation set with a linear decay of the learning rate over the course of training. In addition, we tested between 15,000 and 40,000 learning steps. The performance on the validation set varied widely depending on the learning rate and the number of learning steps (between ρ = .38 and −.04). The best model used a learning rate of 1e-8 and trained for nine epochs (both were tuned using the validation set, not the test set). On the test set, the final model had a Spearman’s ρ of .32 (p < .001) and an R2 value of 7%, meaning 7% of a client’s symptom rating in the subsequent session could be predicted by the raw linguistic content of the prior session.
As a comparison, we ran an n-gram model to assess the degree to which the pretrained RoBERTa model improved performance. We tested unigrams, bigrams, trigrams, and regularizers (c parameters; variables that adjust model estimates based on error) ranging from .01 to 100 on the validation set. The best model was a trigram model with a regularizer coefficient of .01. This model did not predict the outcome better than chance (Spearman’s ρ = .08, p = .18, R2 < .001). This indicates that the transfer learning used by the RoBERTa model had a meaningful impact on the prediction of outcomes in these sessions beyond simple word-frequency counts.
Discussion
Recent advances in technology have resulted in innovative methods for scaling up the evaluation of therapeutic processes (e.g., Goldberg et al., 2020) and client-symptom improvement. Previous studies used NLP-derived ratings of therapeutic processes (e.g., emotion words from a predefined dictionary in Shapira et al., 2021; interventions in Ewbank et al., 2020; topics of conversation in Atzil-Slonim et al., 2021) to predict client outcomes but relied on older dictionary-based models, did not use classical test-train splits, and did not directly predict client symptoms from session recordings. Consequently, the purpose of the current study was to build on past NLP psychotherapy research by developing models that predict symptom improvement of a given session based on the recording of the preceding session. Using 2,630 session recordings, we were able to develop and train a model that was able to significantly predict client symptoms at an effect size similar to other psychotherapy process variables (e.g., alliance; Flückiger et al., 2018) yet do not rely on asking clients to rate sessions or therapists to guess about how a client is doing. Our results are a promising start to developing NLP tools that could quickly predict client-outcome trajectories and provide therapists with important information to tailor and improve quality of care. Furthermore, our findings highlight how session recordings contain meaningful linguistic signals that have the potential to inform and provide contextual information for client and therapist session process ratings. Future studies would benefit from continuing to leverage session recordings to better understand which aspects of therapist–client interactions contribute to client change. For example, researchers could analyze how shifts in client, therapist, and both client and therapist language across sessions are associated with treatment trajectories. Likewise, researchers could also examine how therapist and client language in specific content areas (e.g., exploration of identities, suicidality, behavior change) may account for symptom change.
Note that our final model outperformed a comparison with an n-gram TF-IDF model as well as past NLP models that predict specific continuous variables from session transcripts. Our comparison n-gram model did not predict session outcomes better than chance, and effect sizes from previous studies applying NLP models to session outcomes were quite small. For example, Goldberg et al. (2020) was able to only modestly predict alliance from session recordings (ρ = .15). Likewise, effect sizes for Shapira et al. (2021) from multilevel models using NLP-extracted linguistic features from transcripts to predict outcomes were small (0.011 < f2 < 0.022; η2 = .08). Our model may have outperformed past models because of the application of RoBERTa. Instead of relying on the presence of specific words (as is done in traditional n-gram models; Jurafsky & Martin, 2014), RoBERTa examines how the relationship between phrases is associated with changes in outcomes of interest. Given the complexities associated with therapist–client interactions, RoBERTa may be better suited for predicting client symptoms than the previously employed simpler models. For example, a client expressing a desire to terminate therapy (e.g., “I think I should stop coming to therapy”) could be positive (e.g., treatment goals achieved) or negative (e.g., premature termination). The presence of these words alone is insufficient to indicate symptom improvement. Contextual information from the rest of the session is necessary to understand the outcome trajectory of the client. NLP models that account for more context have similarly outperformed older dictionary-based models in predicting sentiment in therapy contexts (Tanana et al., 2021). Future studies predicting therapeutic processes and outcomes directly from session recordings may greatly benefit from including RoBERTa models in model comparisons. Another reason our models may have performed better than Goldberg et al. (2020) is because symptom measures may assess client factors that may be more linguistically observable in session (e.g., statements regarding mood, physical symptoms) compared with a client’s feelings about the relationship. Raw text may not capture self-report client measures of therapeutic processes such as alliance as fully because these measures assess internal experiences of interactions; other cues such as vocal tone and body posture may be more strongly correlated with self-report measures of therapeutic processes (Imel et al., 2014; Ramseyer & Tschacher, 2011).
Limitations and future directions
There were several limitations in the current study. First, our models were based on predominantly White, cisgender, heterosexual clients and therapists in a university setting; furthermore, we did not collect information on socioeconomic status. Although the sample was relatively large for a psychotherapy process evaluation, it was restricted to one treatment milieu, and thus our NLP models may have been based on clinical interactions that were unique to our sample, which limits generalizability. Future research should develop models based on session recordings from different clinical settings (e.g., community mental health, hospital) across intersecting client and therapist identities. Given documented bias in ML and NLP models (Mehrabi et al., 2021; Yapo & Weiss, 2018), researchers should be aware of how clinical settings and identities of clients and therapists in their sample affect language associated with symptom improvement. Researchers would benefit from testing models in different samples (i.e., external validation) and comparing model performance across samples. Second, our models did not include other client information, such as client demographics and past mental-health history, in prediction of symptom change. Consequently, information relevant to symptom improvement was excluded from our models. Future studies could incorporate more client information into models predicting treatment trajectories. Third, although our models were able to predict symptom scores from session recordings, our models did not identify what specific content in sessions affected predictions the most. Future studies can continue to examine and implement methods of better interpreting how language shifts in therapist–client interactions drive NLP-model predictions of client outcomes. Qualitative and behavioral coding methodologies (e.g., Gonçalves et al., 2011) could also be used to examine sessions that were associated with increased or decreased symptom improvement. Themes, interventions, and other labels from these studies could be used to further refine NLP models and facilitate automated identification of specific session content that predict client improvement. Fourth, contextual NLP models such as RoBERTa are powerful in predicting outcomes of interest based on the word patterns in the context of specific documents, but the word patterns–outcome relationship is not necessarily generalizable outside of the document context. In other words, it is not a specific phrase in any session that influences the prediction of outcomes, but the use of specific phrases in the context of the specific session that affects outcomes. Conversely, it is difficult to interpret how specific text features extracted from these models predict overall outcomes of interest (e.g., “Why does language predict symptoms?”) because the impact of these text features varies based on specific documents (Belinkov et al., 2020). The interpretability of contextual-based NLP models is an active area of research in NLP, and future studies could focus on innovative ways of applying these methodologies in psychotherapy contexts to better derive methods of interpreting model findings on client-symptom improvement.
Implications
Our study has several important implications for research and clinical practice. First, our initial model results indicate that context-based NLP models have great potential in identifying patterns of therapist–client interactions that contribute to client outcomes. Moreover, as NLP modeling approaches improve (e.g., shifting from unigram models to RoBERTa), their practical utility is only likely to increase. Psychotherapy researchers could implement NLP-based model predictions in studies seeking to clarify therapeutic processes at a massive scale (e.g., within the National Health Service), providing unprecedented opportunities for investigating linkages between psychotherapy processes and outcome. Large-scale examinations of mechanisms of change in therapy could also allow researchers to identify patterns in language associated with more effective therapists and, in turn, facilitate efforts to augment training of future therapists. Second, at clinic or health-systems levels, aggregate outcome predictions could be used to support quality-improvement efforts (e.g., evaluating the impact of a clinic- or system-wide training initiative). Agencies could use outcome predictions to identify groups of clients at risk for treatment failure or clinicians who consistently underperform to provide additional support or training (Imel, Sheng, et al., 2015). Automated feedback could be particularly helpful for clinicians who no longer receive supervision and whose outcomes may actually decline as they gain experience (Goldberg, Rousmaniere, et al., 2016). For example, Goldberg, Babins-Wagner, et al. (2016) found that client outcomes gradually improved at a mental-health agency over the course of 7 years after an outcome-monitoring system was implemented; furthermore, the effect size of improvement in client outcomes was almost 3 times as large as gradual decreases in outcomes over time observed in Goldberg, Rousmaniere, et al. (2016). Implementation of NLP-based outcome-monitoring systems could facilitate targeted feedback by quickly flagging session information that contextualizes client symptoms and encourage greater therapist reflection (Hirsch et al., 2018; Imel et al., 2019). This would be particularly valuable in community settings in which providers often have large caseloads and are unable to review all of their session information because of time constraints.
Given the potential of systemic quality improvement in large clinical health settings (Boswell et al., 2015), future research could focus on developing symptom-prediction-based feedback systems and evaluating feasibility and acceptability of these systems. Although current feedback systems provide estimated predictions of symptoms based on past symptom scores (Goldberg, Babins-Wagner, et al., 2016; Lambert, 2015) or summaries of specific interventions (Imel et al., 2019), to date, there are no feedback systems predicting symptom change directly from session content. Feasibility and acceptability studies could focus on examining ways to facilitate clinician openness to using feedback systems, particularly given the context of clinician resistance to receiving feedback and concerns of trusting model predictions (Creed et al., 2022; Hirsch et al., 2018; Imel et al., 2019). Likewise, evaluations of feedback systems could focus on understanding how clinicians integrate knowledge of their client’s predicted scores into interventions in subsequent sessions. Although much work remains to be done developing, testing, and implementing these systems in clinical settings, NLP models may hold great promise in improving the quality and efficiency of clinical care and ultimately the lives of clients.
Footnotes
Acknowledgements
M. J. Tanana, S. Narayanan, D. C. Atkins, and Z. E. Imel are each cofounders and minority share holders in Lyssn.io, a technology company focused on developing machine-learning tools to evaluate the quality of behavioral-health conversations.
Transparency
Action Editor: Pim Cuijpers
Editor: Jennifer L. Tackett
Author Contribution(s)