
Abstract
In adults, pathologies of anxiety such as posttraumatic stress symptoms (PTSS) involve deficits in information processing that may reflect hypervigilance and deficient inhibitory control, specifically for negative information. However, little is known about inhibitory processing in children, particularly regarding the inhibition of emotional information. This study investigated whether children with PTSS or anxiety show impairments in executive control in an inhibition task. A total of 45 children (M age = 9.2 year, SD = 0.7, range: 8–11) completed an inhibition task involving emotional—happy, angry, and fearful—and neutral stimuli and clinical scales for PTSS and anxiety. The results indicated that the percentage of correct answers was modulated by PTSS status, particularly in the happiness task. PTSS and anxiety altered the inhibition of fearful information in children. These data suggest different types of inhibitory deficits depending on clinical symptoms, and implications are discussed.
Keywords
Introduction
Inhibition is the ability to deliberately block automatic or preponderant information when necessary (Eysenck, Derakshan, Santos, & Calvo, 2007). Cognitive models of inhibition distinguish between two components: performance effectiveness and processing efficiency. Performance effectiveness refers to the quality of performance as assessed by behavioral measures. Processing efficiency is defined as the relation between performance effectiveness and the use of resources or effort (Eysenck et al., 2007). Some studies have shown that clinical symptoms, such as posttraumatic stress symptoms (PTSS) or anxiety, may alter these two components.
PTSS corresponds to the presence of some symptoms of posttraumatic stress disorder (PTSD: intrusive memories, avoidance, negative alterations in cognition and mood, and hyperarousal; American Psychiatric Association, 2013) but under the clinical critical threshold and without psychiatric diagnosis (North & Oliver, 2012). From a cognitive point of view, people who have endured a traumatic event experience a first phase that is characterized by intense emotional distress, including anger, guilt, and fear (Horowitz, 1996). Consequently, denial and detachment behaviors may appear. In the subsequent phase, people try to integrate this traumatic experience into their cognitive schemes. Thus, they experience an oscillation between intrusive memories and avoidance. If the negative event is not fully integrated, risk factors for developing PTSD are increased. Among these risk factors, personal factors (i.e., schemes), strategic factors (i.e., coping) and event cognition have been identified (Joseph, Williams, & Yule, 1997).
Anxiety is defined as a subjective feeling of threat associated with appropriate physiological and behavioral modifications (Daleiden & Vasey, 1997). According to cognitive models, anxiety is defined as the tendency for people to perceive threatening and ambiguous stimuli as more dangerous than would individuals without anxiety and to develop inappropriate attentional and interpretative behaviors (Daleiden & Vasey, 1997).
Individuals with PTSS and anxiety have a hyperactive scheme of danger, which is characterized by a tendency to retrieve mainly negative or unpleasant stimuli rather than positive or neutral information during cognitive tasks (Mogg & Bradley, 1998). Nevertheless, the main difference between these two types of symptoms (PTSS vs. anxiety symptoms) is that in anxiety, the feeling of threat is non-specific and non-oriented, which induces apprehension, indecision, and arousal related to the potential occurrence of future threat (Sylvers, Lilienfeld, & LaPrairie, 2011). Commonly, individuals with PTSS present strategic and conscious behaviors during cognitive tasks, whereas anxious people have an unconscious bias. However, these different reactions to stress and apprehension lead to difficulties in information processing, particularly with regard to inhibition and attention.
Moreover, it has been reported that individuals with PTSS are characterized by altered inhibitory processing (Bomyea, Risbrough, & Lang, 2012; LaGarde, Doyon, & Brunet, 2010), with more mistakes and intrusions in Go-NoGo tasks (Falconer et al., 2008). These difficulties appear to correlate with reduced activation in brain areas associated with inhibitory control (i.e., the inferior frontal cortex and medial prefrontal cortex). For instance, severe PTSD has been reported to correlate with reduced recruitment of the inhibitory control network (Falconer et al., 2008). In addition, individuals with PTSS present a disengagement bias for negative or trauma-related information (DePrince, Weinzierl, & Combs, 2009; Masten et al., 2008; Pine, 2003; Pine et al., 2005). Individuals are slower to respond to negative stimuli (Mogg, Holmes, Garner, & Bradley, 2008), an attentional bias that may reflect a difficulty in disengaging attention from these stimuli.
In the case of anxiety, hypervigilance for negative or threat-related information has been reported (Britton et al., 2013; Hankin, Gibb, Abela, & Flory, 2010; Telzer et al., 2008). This hypervigilance bias is represented by an increase in threat sensitization within the environment. It has also been observed, in a laboratory setting, that participants with anxiety process negative information faster than neutral information (Koster, Crombez, Verschuere, & De Houwer, 2004). This bias can be considered “automatic” because it takes place in a preattentional stage and is activated automatically (Mogg & Bradley, 1998). Furthermore, these cognitive difficulties play a role in the development and maintenance of PTSD or anxiety symptoms (Aupperle, Melrose, Stein, & Paulus, 2012; Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg, & van IJzendoorn, 2007; Lindgren, Kaysen, Werntz, Gasser, & Teachman, 2013), especially during childhood (Baker, Den, Graham, & Richardson, 2013; Chu, Williams, Harris, Bryant, & Gatt, 2013).
Some studies have shown that PTSS and anxiety occur frequently in children and lead to significant clinical pain, but little is known about the effect of these symptoms on cognition (Aaron, Zaglul, & Emery, 1999; Carrion, Weems, Ray, & Reiss, 2002; Deblinger, Lippman, & Steer, 1996; King et al., 2000). Few studies have tested the effect of trauma in children (e.g., Gindt, Garcia, & Chanquoy, submitted); however, it is of particular interest to evaluate the short- and long-term modifications in this population. Indeed, exposure to traumatic events in childhood leads to clinical, cognitive, and personal changes (Banyard, Williams, & Siegel, 2001; Boney-McCoy & Finkelhor, 1995; Breslau, Chilcoat, Kessler, & Davis, 1999; Cisler et al., 2011). Some authors postulate that trauma in childhood leads to a lower intellectual quotient and impaired executive functioning (Beers & De Bellis, 2002; DePrince et al., 2009). These cognitive disabilities may be implicated in the development of pathologies in adulthood (Bomyea et al., 2012).
Concerning inhibition, the progression of this cognitive function is dependent on childhood development. Indeed, children as young as 4 years old are characterized by attentional biases toward positive stimuli (Lindstrom et al., 2009). At 6 years of age, some children present attentional biases toward threat-related information (Field & Lester, 2010). Children more rapidly detect information about common fears—for example, about spiders or snakes—compared with other types of information. Neural and cognitive development allows for inhibitory control beginning at approximately 8 years of age. At this age, attentional biases are often linked to clinical symptoms, such as PTSD or anxiety (DePrince et al., 2009; Field & Lester, 2010; Hunt, Keogh, & French, 2007; Masten et al., 2008; Telzer et al., 2008). Neuropsychological assessments, such as Stroop or Go/No-go tests, have revealed difficulties attending to neutral material for these two pathologies (Beers & De Bellis, 2002; DePrince et al., 2009; Hunt et al., 2007; Waters, Henry, Mogg, Bradley, & Pine, 2010; Watts & Weems, 2006). Commonly, PTSS lead to difficulties in performance effectiveness in children. For example, Wu et al. (2010) have shown that children with PTSS made more mistakes than a control group in a Go/No-go task, revealing inhibitory dysfunction. Conversely, individuals with anxiety often exert more effort than individuals without anxiety. Consequently, anxiety leads to altered processing efficiency but not altered performance effectiveness (Eysenck et al., 2007).
The aim of the present study was to explore whether PTSS and anxiety modulate inhibitory processing in children based on emotion. In line with previous studies, we expected that children with subclinical symptoms (PTSS and anxiety) would have more difficulty inhibiting fearful information, which would lead to a higher inhibition index (Eysenck et al., 2007; Masten et al., 2008; Pine et al., 2005). Moreover, according to PTSS symptoms, happy stimuli would lead to a greater percentage of errors (American Psychiatric Association, 2013).
Method
Participants
Children from two classrooms were invited to participate in this study. Parents and children gave consent to participate. Six participants were removed from statistical analyses because the clinical scales were only partially filled or the error rates exceeded 50%. In total, 45 fourth graders (25 boys and 20 girls) between the ages of 8 and 11 (M age = 9.2 year, SD = 0.7) volunteered to participate in this study. The participants were randomly assigned to each group. The age range of the participants was chosen according to neural and cognitive development. Indeed, by 8 years of age, inhibition difficulties have been linked to clinical symptoms (Field & Lester, 2010). The present sample of children did not have psychiatric diagnoses. Among our sample, 21 children had experienced a traumatic event, including road accidents (28.5%), diseases (24%), natural disasters (19%), parental divorces (14%), deaths (9.5%), and physical assaults (5%).
Materials
Inhibition task
Four types of stimuli were used in the inhibition task: neutral, angry, fearful, and happy faces. A total of 160 stimuli (40 per emotion) were selected from a French database of emotional faces (Meillon et al., 2010). All stimuli were previously validated with 120 children to be sure that the stimuli represented one of the different emotions.
Clinical scales
Children were screened for symptoms of PTSS and anxiety using the French CPTS-RI (Children Post-Traumatic Stress Reaction Index; Frederick, Pynoos, & Nader, 1992) and the State-Trait Anxiety Inventory for Children (STAIC; Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983).
The CPTS-RI consists of a collection of traumatic event information and a 20-item self-report scale with items for each PTSD symptom, according to the DSM-4-TR (American Psychiatric Association, 2000). Participants rated the degree to which they were bothered by each symptom on a 5-point scale ranging from 0 (Never) to 4 (More often). Possible scores range from 0 to 80.
The STAIC consists of 40 short sentences: 20 assessing the participant’s current state (STAIC-State; e.g., “I feel afraid”) and 20 assessing the participant’s usual state (STAIC-Trait; e.g., “I am happy”). These questions are rated on a 3-point scale ranging from 1 (Never) to 3 (Often). Possible scores for this clinical scale range from 20 to 60.
Apparatus
Stimuli for the inhibition task were presented on a 19″ monitor (800 × 600, 60 Hz) using Superlab software (Version 2; Cedrus Research, 1999) with a Dell XPS T500 computer. Response latencies (measured in ms) and accuracy were automatically recorded in Superlab.
Procedure
The participants were individually tested in a 1-hour session that consisted of the inhibition task followed by the administration of the STAIC and the CPTS-RI. This order was fixed to avoid the possible influence of clinical scales on participants’ mood during the task.
The inhibition task was an emotional Go/No-Go task with four blocks according to stimulus valence: neutral, fearful, angry, or happy faces (Figure 1). For each block, the participants were instructed to press a designated key (“k”) for a target stimulus that was established at the beginning of each block and to press a second key (“d”) for all other stimuli. Each block was composed of 20 target stimuli and 60 distractors (other faces with the same emotion tested in the block). The participants were instructed to respond as quickly as possible without sacrificing accuracy. Trials were randomized among participants.
Exemple of trial for the happy block.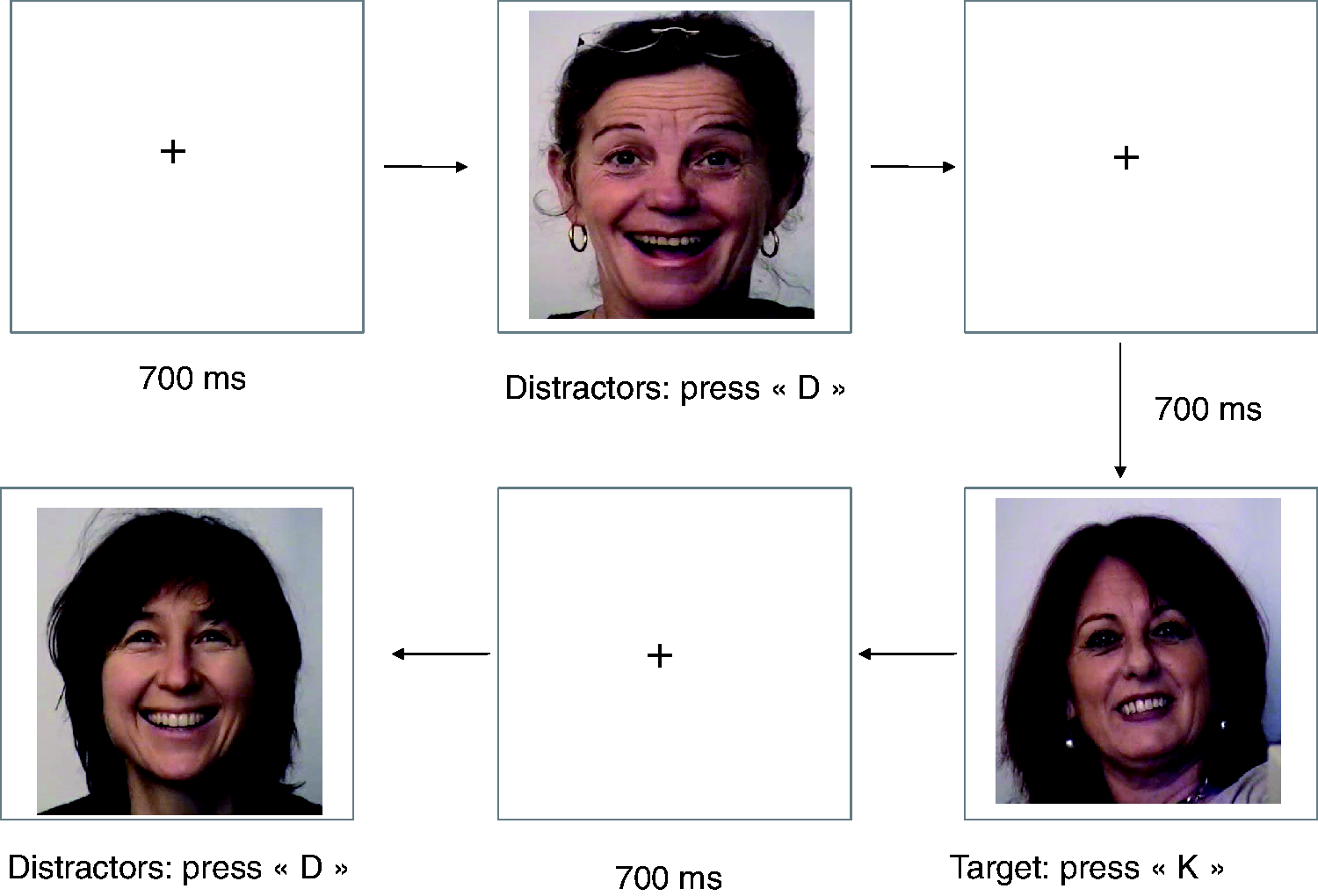
Each trial began with a black fixation cross in the center of a white screen for 700 ms. The fixation cross was immediately followed by an experimental trial with stimuli remaining on the screen until a response was registered. Stimuli appeared in the center of the monitor. The computer recorded the accuracy and response time for each response. For each participant, two measures were calculated according to these data: a general percentage of errors (including Go and No-Go trials) and an inhibition index, which is computed as the (No-Go)–(Go) response times on correct trials. A positive score on the inhibition index reflects difficulty inhibiting information, whereas a negative score corresponds to efficient inhibition.
Data Analysis
Several one-way analyses of variance (ANOVAs) were performed on the percentage of errors for age, sex ratio, and manual laterality. The same analyses were performed for the inhibition index. To evaluate the impact of PTSS and anxiety, multiple regressions were run on the percentage of errors and inhibition index. Finally, correlation analyses were performed between clinical score, percentages of errors and response times.
Results
Sample Characteristics
Sample Characteristics.

The Effect of PTSS and Anxiety Modulation on Cognition
A regression analysis was conducted to test the effect of PTSS and anxiety on the percentage of errors. No significant effect was found for neutral, F(1, 43) = 2.4, p = .11, angry, F(1, 43) = 1.1, p = .29, or fearful faces, F(1, 43) = 1.9, p = .18. However, CPTS-RI scores (B =−0.74, β = −0.31, p < .05) affected the percentage of errors for happy faces, F(1, 43) = 4.5, p < .05. Concerning the inhibition index, only fearful faces, F(2, 42) = 4.3, p < .05, were affected by anxiety (B =53.28, β = 0.46, p < .01) and PTSS (B = 13.47, β = 0.35, p < .05). Regressions for neutral, F(1, 43) = 2.7, p = .11, angry, F(1, 43) = 1.3, p = .25, and happy faces, F(1, 43) =1.4, p = .26, were not significant.
Correlations showed that the percentage of correct answers for fearful information correlated negatively with CPTS-RI scores, r = −.31, p < .05. Concerning the inhibition index, CPTS-RI scores correlated positively with fearful, r = .36, p < .05, and angry faces, r = .38, p < .05. Finally, there was a positive correlation between the inhibition index for neutral faces and STAIC scores, r = .31, p < .05.
Discussion
The present study sought to investigate inhibitory processing in response to faces conveying different emotions—anger, fear, and happiness—in children with varying levels of posttraumatic stress and anxiety symptoms. We found that the inhibition of fearful information was impacted by PTSS and anxiety. Moreover, PTSS altered accuracy for happy stimuli. We also observed that the frequency of PTSS in our sample was higher than the data from epidemiological studies.
According to results, inhibition of fearful information was altered by subclinical symptoms in these children. This result is consistent with previous studies (Falconer et al., 2008; Masten et al., 2008; Pine et al., 2005). Indeed, PTSD or anxiety leads to dysfunction in the fear network (Friedman, Keane, & Resick, 2010). From a behavioral point of view, children with PTSD have difficulty interacting with fearful or threat-related information. For example, these children are often slower to respond to negative stimuli. This may reflect an attentional bias toward threat-related information, which is a core feature of PTSD (Aupperle et al., 2012; American Psychiatric Association, 2000). This attentional capture may be related to intrusive memories. According to Cassiday, McNally, and Zeitlin (1992), fearful information may reactivate a partial traumatic memory. Similarly, when children with anxiety inhibit fearful information, the inhibition index is altered as well. For these children, fearful information increases cognitive cost. According to Eysenck et al.’s (2007) theory, to conserve performance effectiveness (accuracy), children with anxiety exert more attentional effort, leading to altered processing efficiency. Commonly, PTSD or anxiety is associated with overlapping fear structures. For example, in PTSD, emotional processing theory postulates that a large number of stimuli can activate the fear structure, leading to a perception of the world as entirely dangerous (Foa & Kozak, 1986). At the same time, according to this theory, people with PTSD develop a view of self-incompetence. These two negative cognitions (“The world is dangerous” and “I am incompetent”) increase PTSD symptoms and reinforce the erroneous cognitions. Interestingly, preexisting knowledge about the safety of the world and the competence of the self both influence the development of PTSD symptoms after a traumatic event (Friedman et al., 2010). Indeed, at 9 years of age, children elaborate their beliefs about the world and about themselves (Daud, Klinteberg, & Rydelius, 2008). A traumatic experience at this age may lead to erroneous schemes for these two beliefs in adulthood, leading to increased risk factors for developing PTSD (Baker et al., 2013; Banyard et al., 2001; Kendall-Tackett, 2000). Similarly, theory and experiments on anxiety indicate that these symptoms alter the fear network (Mennin, 2004). Anxiety symptoms lead individuals to adapt an attentional hyperarousal scheme for information being able to reactivate symptoms. This hyperarousal enhances detection of fearful information in the environment (Stapinski, Abbott, & Rapee, 2010). Consistent with studies on individuals with PTSD, studies have also shown that this hyperarousal spreads to other information (Hankin et al., 2010; Telzer et al., 2008). For example, ambiguous stimuli will be perceived as more negative by individuals with anxiety compared with controls (Daleiden & Vasey, 1997). Finally, this hyperarousal for negative information increases worry and is implicated in the maintenance of anxiety symptoms (Borkovec & Roemer, 1995; Puliafico & Kendall, 2006; Stapinski et al., 2010).
PTSS in children also led to a difficulty processing “happy” information. Impairments concerning happy information are less studied than those concerning negative information, but deficits in processing happy information have been reported in participants with PTSD (Moradi, Taghavi, Neshat-Doost, Yule, & Dalgleish, 2000; Paunovic, Lundh, & Öst, 2002). This impairment in processing positive stimuli may result from a deficit in resource allocation. Indeed, it has been suggested that these children process fearful stimuli more efficiently (Daleiden & Vasey, 1997). This facilitation leads to a reduction in performance when information is positive or neutral. As an example, dog-phobic children are terrified of all dogs because they have ceased to encode further information (i.e., neutral or positive; Daleiden & Vasey, 1997). Generally, after a trauma, children show memory impairments for positive stimuli compared with neutral or negative information (Masten et al., 2008; Moradi et al., 2000; Samuelson, Krueger, Burnett, & Wilson, 2010). Moreover, among PTSD symptoms, emotional numbing leads to reduced positive feelings, deficient reward functioning, and decreased interest centers (American Psychiatric Association, 2013; Nawijn et al., 2015). This symptom leads to a difficulty in recognizing and processing positive information. Wingenfeld et al. (2011) have shown that traumatic events in childhood increase emotional numbing, particularly anhedonia, and cognitive impairments in adulthood. Otherwise, anhedonia may be correlated with comorbidity. Effectively, Kashdan, Elhai, and Frueh (2006) found that patients with PTSD with high anhedonia are characterized by more depressive symptoms compared with patients with lower anhedonia. However, the interest for studying positive affect in PTSD is new. As a consequence, PTSD therapy is often focused on negative affect. A recent review proposed to modify actual PTSD therapy to include an emotional numbing aspect (Nawijn et al., 2015). According to these authors, it is very important to improve therapy efficiency to add a remediation of reward functioning. For example, psychotherapy outcomes in major depressive disorder can substantially improve by placing more emphasis on positive emotion experience, especially when patients report significant anhedonic symptoms. In patients with major depressive disorder, psychotherapy that is specifically aimed at increasing approach and the positive experience of rewarding stimuli results in a significant reduction in depressive symptoms (Nawijn et al., 2015).
The last result of this study is related to the percentage of children with trauma and its subclinical consequences. We found that almost 50% of children had a CPTS-RI score indicating probable PTSD. This percentage is higher than that from epidemiological studies. In urban areas, 60% of public school children had experienced at least one major traumatic event (Hoven, Duarte, & Mandell, 2003). The percentage of people who develop PTSD after traumatic events varies between 20% and 50% depending on the type of trauma (Berkowitz, Stover, & Marans, 2011; Huemer, Erhart, & Steiner, 2010). However, these percentages concern only full PTSD. Full PTSD corresponds to children with the four main symptoms and significant clinical distress (American Psychiatric Association, 2013). Some studies have shown that full and partial PTSD in children lead to the same distress and difficulties in functioning (Carrion et al., 2002; Daviss et al., 2000). In children, the percentage of subclinical symptoms is very important: 47.5% of traumatized children do not correspond to the full PTSD diagnostic criterion, but these children are characterized by serious clinical distress (Aaron et al., 1999; Carrion et al., 2002). Consequently, it seems very important to evaluate the intensity of children’s symptoms and the effect of everyday life rather than the mere presence of those symptoms. Moreover, even if children do not develop full PTSD, it seems that PTSS after a traumatic event can be a risk factor for developing mental disorders in adulthood (Baker et al., 2013; Banyard et al., 2001; Chu et al., 2013). Indeed, a traumatic event can change world beliefs and the development of personality (Kendall-Tackett, 2000; McTeague et al., 2010).
The results provide evidence for distinguishing patterns of attentional processing in anxiety and PTSS based on symptom levels and the emotional content of stimuli. However, the present study has several limitations. First, it would be important to take into account more information about the traumatic experiences. According to previous studies, the type (Ikin, Creamer, Sim, & McKenzie, 2010), number (McTeague et al., 2010), and date (Banyard et al., 2001) of traumatic events modify cognitive abilities and clinical symptoms. For example, the age of children during traumatic exposure modifies risk of PTSD development. Younger children (<6 years) have a higher risk than older children for developing PTSD after a trauma (Salmon & Bryant, 2002). Similarly, more control of comorbidity would be necessary. In this study, depression and hyperactivity were not controlled. We cannot exclude the possibility that these pathologies could have interfered with executive functioning, particularly for inhibition (Back, Sonne, Killeen, Dansky, & Brady, 2003; Freedman, Brandes, Peri, & Shalev, 1999; Zlotnick et al., 1999). Another factor is working memory. Commonly, PTSS affects the intellectual quotient for speed of processing and for working memory (Beers & De Bellis, 2002; Bücker et al., 2012; De Bellis, Hooper, Spratt, & Woolley, 2009; DePrince et al., 2009). These two components are strongly correlated. Usually, according to processing efficiency theory, attentional control may depend on the working memory system (Eysenck et al., 2007). Consequently, it would be interesting to pursue research by evaluating attention and working memory in children with PTSS. Moreover, it seems also of particular interest to consider family environment. In fact, family environment is thought to be a risk factor for developing or maintaining PTSD symptoms in childhood (Bluestone et al., 2011; Board & Dai, 2011; Morris, Gabert-Quillen, & Delahanty, 2012; Yehuda, Halligan, & Bierer, 2001). Parental stress or pathologies are known to increase the risk of developing PTSD in children (Bluestone et al., 2011; Yehuda et al., 2001).
The main goal of this research was to investigate inhibitory processing in children with subclinical symptoms of PTSS or anxiety. The results provide evidence for distinct patterns of attentional processing in children with PTSS based on anxiety and emotion. PTSS and anxiety influenced the inhibition of fearful faces, whereas only PTSS played a role in the response to happy faces. These results may be related to difficulties in emotional regulation and a higher risk of developing pathologies in adulthood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.