
Abstract
The Centre for Disease Control recommends vaccination of children against SARS-CoV-2 to reduce the severity of COVID-19 disease and reduce the likelihood of associated complications. Vaccination of children requires the consent of parents or guardians, and levels of consent may ebb and flow over the course of the pandemic. This exploratory study examines predictors of parental intentions to vaccinate their children and the speed with which they would have them vaccinated during the fifth wave of the pandemic when vaccines were just being approved for use in children using a convenience sample of 641 parents reporting on 962 children. Multi-level regression analyses demonstrated regional differences in likelihood, with those in the Northeast reporting higher likelihood than those in the West. Parents with a conservative belief system were less likely to want to have their children vaccinated. Parents were more likely to have their child vaccinated if the child had COVID-19-related health risks, their child had a more complete vaccination history, and COVID-19 was perceived to be a greater threat to oneself and one’s family. Faster intended vaccination speed was associated with regional urbanicity, liberal belief systems, more complete vaccination histories, and parental COVID-19 vaccination history. Higher levels of parental anxiety and lower levels of perceived vaccine danger were associated with increased speed. The severity of the COVID-19 pandemic within one’s county was marginally related to speed, but not likelihood. These results underscore the importance of regular assessment of parental intentions across the pandemic, for practitioners to probe parental anxiety levels when discussing vaccination, to explicitly address risk/benefit analyses when communicating with parents, and to target previously routine unvaccinated parents and those in more rural areas to increase vaccine uptake. Comparisons are made with Galanis et al.’s (2022) recent meta-analysis on the topic.
Keywords
Introduction
Over the last two years, COVID-19 vaccines have been rolled out in an age-staggered manner as evidence for their effectiveness in younger populations emerged. In early Fall 2021, vaccines were approved for use in anyone aged 12 and up. In late Fall 2021, vaccines were approved for ages 5–11, and in Summer 2022, vaccines were approved for 6-month to 5-year-old children (Centers for Disease Control, CDC, 2022, June 18). The CDC recommends COVID-19 vaccines for everyone ages 6 months and older. Uptake in children has been low, and a full 6 months after this latest approval, for children aged 6 months–4 years, coverage with at least one dose was 10.1% and 5.1% for series completion (Murthy et al., 2022). Based on data published by the CDC in April 2023, only 8.2% of children younger than 2-year, 10.6% of 2–4-year-olds, and 39.9% of 5–11-year-olds have had at least one dose of COVID-19 vaccine, with lower rates for completing the primary multi-dose series (CDC, accessed 2023, April 4). COVID-19 vaccination of children is important to decrease the severity of disease, including for those who are at high-risk (Swann et al., 2020; Wong et al., 2021) and decrease the risks of Multisystem Inflammatory Syndrome (CDC, accessed 2022, April 15); while data on the ability of child vaccination to reduce transmissibility (i.e., to help curb the spread of SARS-CoV-2) is mixed (Wong et al., 2021).
A recent review determined that parental vaccine hesitancy is one of the most important barriers to the receipt of vaccinations in the United States (Olusanya et al., 2021). As parents and guardians (hereafter referred to as parents) are the primary healthcare decision makers for their children, it is important to understand what might predict the decision to vaccinate, continue to vaccinate (i.e., complete the vaccine series), or not to vaccinate their children, and the speed with which those vaccinations may happen. Vaccine uptake is not uniform. Rates of regularly scheduled immunizations and seasonal influenza vaccination are not equivalent, and intentions to vaccinate against H1N1 were higher than intentions to vaccinate against seasonal influenza (Gust et al., 2008; Makarovs & Achterberg, 2017). Parental attitudes differ across vaccines (e.g. the high degree of concern over the varicella vaccine in Gust et al., 2008). We cannot entirely look to existing vaccine literature to predict vaccination intentions during pandemics, including COVID-19.
Lackner and Wang (2021) explored the intentions to vaccinate Canadian children during the early stages of the COVID-19 pandemic when vaccines were not yet approved for use. Older parental age, living in the Prairies (relative to Central Canada), more complete child vaccination history, and a greater tendency to prioritize the risks of the disease relative to the risks of side effects (i.e. lower omission bias) were associated with higher likelihoods of intention to vaccinate participants’ children. Faster speed of intended vaccination was associated with a similar constellation of variables with the additional association of a child in the family having a COVID-19 related health risk being associated with slower intended speed. We wanted to know if similar variables would relate to US parents’ intentions to begin or continue vaccinating their children now that vaccines are approved for use in younger age ranges. Differences in demographics, political beliefs, race and attitudes necessitate separate investigations of intentions to vaccinate (Gravelle et al., 2022; Pennycook et al., 2022). As articulated by Salmon and Dudley (2020), in the context of COVID-19 vaccines: “Vaccine perceptions and disease outbreaks are often localised issues and as such it is vital to have serial, cross-sectional surveys that can identify issues within communities, countries, and regions” (pp. 870). Notably, perceptions of vaccination likelihood are likely to ebb and flow over the course of a pandemic, perhaps owing to changing pandemic severity and scientific developments (e.g., clinical trial data).
In addition to older parental age (Chen et al., 2015; Lackner & Wang, 2021), there are various demographic factors associated with vaccination intentions and vaccination receipt for children. Parents or guardians with higher socioeconomic status (SES) or residing in more privileged neighborhoods are more inclined to vaccinate their children for routine vaccination (e.g., MMR) and seasonal influenza compared to their counterparts (Chen et al., 2015; Friederichs et al., 2006; Green et al., 2015; Jung & Viswanath, 2013). Further, increased family size is negatively associated with the likelihood of immunizing children against pertussis (Li & Taylor, 1993) and achieving complete routine vaccination (DTP, polio, and MMR) by the age of 19 months (Trauth et al., 2002), although it is worth noting that Casiday et al. (2006) found a family size effect in the opposite direction. Also, parents from non-minority backgrounds are more likely to have their children vaccinated against pertussis, polio, MMR, seasonal influenza, and/or H1N1 compared to those from minority backgrounds (Casiday et al., 2006; Cheung et al., 2015). Additionally, vaccination rates vary across different regions within a country. For example, individuals in the Western USA are more prone to refuse or delay routine vaccinations for their children compared to those in other census areas (Gust et al., 2008). Moreover, political affiliation may affect parental decisions to vaccinate their children considering conservative individuals are less likely to endorse routine vaccination than liberal individuals (Baumgaertner et al., 2018), and the same is true for adult COVID-19 vaccination (Ruiz & Bell, 2021). We could find little literature on whether parent’s political beliefs influenced their intentions to have their child vaccinated (Szilagyi et al., 2021).
Thus, we investigated the demographic predictors of the likelihood and speed of children receiving a SARS-CoV-2 vaccination to determine whether the previously observed relationships related to child vaccination still hold in the novel public-health context of COVID-19 or if they are overshadowed by psychological and experiential factors that may be specific to COVID-19.
A recent systematic review and meta-analysis by Galanis et al. (2022) 1 summarized the existing literature on parental intentions to vaccinate against COVID-19 across some 44 studies including over 300 000 parents with data collection times ranging from March 2020 to October 2021. Patterns of explanatory variables were far from universal (Galanis et al., 2022). For instance, 20 of the studies measured income levels, and seven found it to positively predict intentions, two found it to negatively predict intentions, and 11 found no significant relationship. Further work is required to untangle these associations.
In addition to demographics, we also explored the health, psychological distance from COVID-19, and other psychological factors that may influence intentions to vaccinate against SARS-CoV-2, both those specific to COVID-19 (e.g., knowing someone with the disease) and those not specific (e.g., levels of trait anxiety). Firstly, we examined prior experiences with vaccination, such as the completeness of vaccination history and encounters with vaccine adverse events (VAEs), as potential predictors for both the speed and likelihood of children receiving vaccinations. People who regularly received influenza vaccines were more inclined to get vaccinated against H1N1 during the 2009 epidemic (Galarce et al., 2011). Mothers who declined influenza vaccination during pregnancy were less likely to have their children fully routine vaccinated (Fuchs, 2016). Parental vaccine history was linked to MMR vaccine uptake (Flynn & Ogden, 2004). Therefore, those with complete vaccination histories may be more likely to have their children receive the SARS-CoV-2 vaccine, a prediction largely supported by Galanis et al. (2022). Further, children’s vaccination history is influenced by parental attitudes toward vaccines and their experiences with or concerns about VAEs. Early vaccination experiences can have lasting effects on subsequent vaccinations. Parents with personal experiences or knowledge of VAEs tend to have lower confidence in vaccine safety, health benefits, and effectiveness, leading to higher levels of vaccine hesitancy (Cheung et al., 2015; Nowak & Cacciatore, 2017). Exposure to scenarios involving VAEs decreases intentions to get vaccinated against hypothetical diseases (Haase et al., 2020). Therefore, we asked parents about their and their children’s experiences with VAEs, if any. Additionally, we assessed general attitudes toward vaccinations, including perceptions of danger, feelings of powerlessness, and trust in authorities regarding vaccines, all of which influence vaccination intentions and appear to influence vaccination intentions per the meta-analysis in Galanis et al. (2022) and Lackner and Wang (2021). We also inquired about whether participants and their children had a primary care physician. Having a strong, trusting relationship with a primary healthcare provider is associated with increased vaccine confidence (Nowak & Cacciatore, 2017). Doctor’s recommendations for vaccination were linked to higher H1N1 vaccine uptake (Ramsey & Marczinski, 2011), and we aimed to determine if a similar pattern held for SARS-CoV-2 vaccination intentions. The studies included in Galanis et al. did not appear to assess this important variable.
Additionally, we collected information on parent and child COVID-19 vaccination history to account for these important covariates. We collected information on COVID-19 status because parents of households with high rates of COVID-19 may wish to vaccinate their children to prevent further illness, or may believe that they do not have to vaccinate their children for reasons of natural immunity (e.g., Ebrahimi et al., 2021).
Experiential factors like vaccine history, VAEs, and access to care are closely intertwined with individuals' psychology which may also shape opinions about vaccination. The closer a disease “hits home” (reduced psychological distance), the more likely individuals are to act to protect themselves and their families. For instance, individuals with a family history of certain diseases are more likely to get vaccinated against them (Guthmann et al., 2013; Hsu et al., 2009). People who believe they have a low risk of infection are more likely to change their attitudes if someone in their social circle contracts the illness (Taha et al., 2013). In other words, the closer the perceived threat, the greater the inclination to vaccinate.
Social distance is one aspect of the broader concept of psychological distance, which influences how individuals view and respond to disease threats as a function of the perceived closeness of the threat to oneself. Therefore, we investigated how many people the responding parent knows who have been diagnosed with COVID-19, their closeness in relationship, and their health outcomes. The threat of COVID-19 may appear greater to those who know many people diagnosed with the disease or who have experienced severe outcomes, reducing psychological distance from COVID-19. A study in Malaysia supported this hypothesis, showing that knowing someone with COVID-19 was associated with a greater intention to vaccinate against SARS-CoV-2 (Wong et al., 2020), although we do not know if this relationship holds for decisions about vaccinating one’s children in the American context. Similarly, perceived risk of acquiring the disease influences vaccination decisions, including decisions about receiving the SARS-CoV-2 vaccine for oneself (Wong et al., 2020) and one’s children (Galanis et al., 2022), and likely affects how psychologically distant one feels from COVID-19.
Further, the tendency to favor inactive choices (such as not getting vaccinated) over active ones (vaccination) – a phenomenon known as omission bias – might arise from a heightened perception of the risks associated with vaccination (like side effects) compared to the perceived risks of not getting vaccinated (the danger of contracting the disease; Hamilton-West, 2006) and may lead to reduced vaccine uptake. Lackner and Wang (2021) found preliminary evidence that the strength of the omission bias predicted both likelihood and speed of getting one’s child vaccinated against COVID-19.
Our investigation also delved into how the pandemic impacted the psychological well-being of parents. We hypothesized that those most adversely affected by the pandemic would be more inclined to vaccinate their children when contrasted with their less affected counterparts. Additionally, we explored the potential correlation between levels of state (temporary) and trait (enduring) anxiety and the inclination to vaccinate. Mothers with high trait anxiety are less likely to have their children fully vaccinated compared to those with lower anxiety levels (Ozkaya et al., 2010). Healthcare workers who considered the H1N1 vaccine unsafe exhibited higher levels of state anxiety in contrast to those who deemed it safe (Savas & Tanriverdi, 2010). In contrast, mothers with mild anxiety symptoms are more inclined to receive the influenza vaccine during pregnancy compared to women without such symptoms (Mohammed et al., 2020). These inconsistent findings could be attributed to the distinction between making healthcare decisions for oneself versus one’s children, variations in measuring state and trait anxiety, and the specific characteristics of the vaccine and disease in question.
In the pandemic context, it is noteworthy that levels of state anxiety may be elevated, as parents report increased stressors related to relationships, health, safety, work, and finances (Brown et al., 2020). This heightened stress may promote both heightened and diminished intentions to vaccinate (Huang & Zhao, 2020; Rodriguez et al., 2020; Spinelli et al., 2020). Taken together, these lines of inquiry underscore the importance of examining the connections between state and trait anxiety and intentions to vaccinate children. Lackner and Wang (2021) found no association between state and trait anxiety and child vaccination intentions, but avoidant thought patterns were associated with increased speed. Urrunaga-Pastor et al. (2021) found that increased levels of anxiety and depression were associated with higher intentions to vaccinate children and adolescents against COVID-19 in a large Latin American and Caribbean sample while other researchers (e.g., Evans et al., 2021) found no association between vaccination intentions and mental health.
Thus, our objectives were exploratory in nature - to describe some of the variables related to intent to vaccinate (both speed and likelihood) children for SARS-CoV-2 during the time when vaccines were being approved for use in children in the USA. Thus, the hypothesized predictors (or more accurately in statistical terms, the explanatory variables, which strive to explain variance in parents’ intention to vaccinate children and do not focus on predictions) included: demographic variables (income, education, age, political affiliation, census region), parental mental health (anxiety and impact of COVID-19), psychological distance from COVID-19 (e.g., regional rates of COVID-19, knowing those with COVID-19 and their outcomes, COVID-19 risk perceptions), attitudes toward immunizations, health variables (previous experience with VAEs, access to primary care physicians, COVID-19 risk factors, and COVID-19 vaccination history), and omission bias.
Methods
Procedure and Participants
We recruited 864 participants using Amazon’s Mechanical Turk system (MTurk). An announcement was posted on the MTurk Web site. Participants, over the age of 18, registered on Amazon’s site to become ‘workers’ who can participate in simple tasks whenever it is convenient. ‘Workers’ were asked to confirm that they met the eligibility criteria of being a parent of at least one child under the age of 18, lived in the USA, and wished to participate in our study. Anyone meeting inclusion criteria was free to participate, and we did not restrict the number of participants as a function of geographic region, or other demographic characteristics (i.e., convenience sampling). Participants then clicked on a hyperlink which redirected them to an online survey platform. After completing the questionnaires, participants were thanked for their participation and provided a unique 6-digit code which they entered into the MTurk Web site to receive their compensation.
All participants received US$1.25 for participating in the study -- a higher level of compensation than other MTurk tasks. The median hourly wage for MTurk tasks $1.38 (Horton & Chilton, 2010); therefore, for the current study compensation of $1.25 for 40 minutes equates to a $1.66 hourly wage. Both clinical and non-clinical MTurk samples yield reliable and valid data (Arditte et al., 2016; Buhrmester et al., 2011; Paolacci et al., 2010).
Descriptive Statistics of Final Sample.
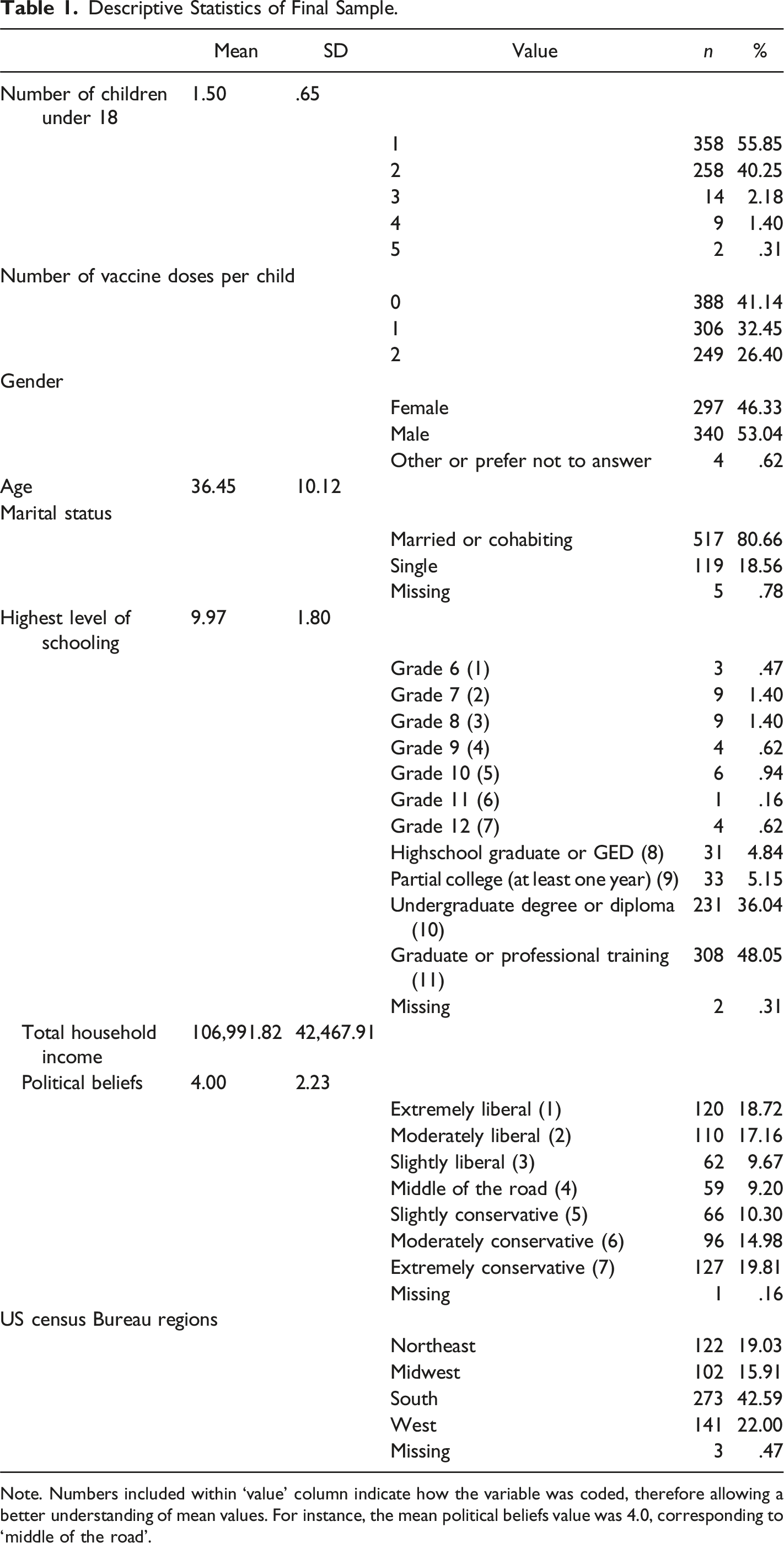
Note. Numbers included within ‘value’ column indicate how the variable was coded, therefore allowing a better understanding of mean values. For instance, the mean political beliefs value was 4.0, corresponding to ‘middle of the road’.
Survey Timing
Data were collected between September 8, and October 2, 2021 when vaccines were approved for use and available to anyone ages 12 and up. In November 2021, 1 month after data collection was complete, vaccines were approved for ages 5–11 (CDC, 2021, November 2).
Measures
Independent Variables
Family Variables
We asked how many children aged <18 years are currently under parental care, how many adults aged ≥18 years live in the home, children’s ages, and their relationship to the child (e.g., biological mother/father, stepmother/father).
Demographics
Parents reported their age, sex, ZIP code, work status, occupation, total family income, marital status, and highest education level. Income was non-normally distributed and was log transformed. Region of residence was categorized according to the US Census Bureau regions of Northeast, Midwest, South, and West using ZIP code information, and the rural proportion of the county was extracted from this ZIP code information (US Census Bureu, 2021). If participants indicated that they were married, they reported their spouse/partner’s work status, occupation, and highest education level. If two parents lived in the home, averaged educational levels were calculated.
Participants rated their political beliefs from extremely liberal to extremely conservative, corresponding to scores of 1 and 7, respectively, similar to Szilagyi et al. (2021).
Access to a Primary Care Physician
The responding parent reported, for each child and their spouse/partner (if applicable), if they have a family doctor or pediatrician. From this, we calculated the proportion of family members with a doctor.
Pre-Existing Risk Factors for COVID-19
The responding parent selected from a list of 17 cardiac, respiratory, weight-related, and immune system conditions (e.g., congestive heart failure, chronic lung disease, obesity) that they had been diagnosed with, if applicable. They completed this same checklist for each child. We summed the number of COVID-19-related health risks the responding parent and each child possessed. Parental health risks were treated as a continuous variable (range = 0–8), while child health risks were dichotomized to 0 versus 1 or more given the relatively fewer reported in this group.
COVID-19 Health Status
One item used, with permission, from unpublished data by Santistevan and colleagues (Santistevan et al., 2020), assessed the responding parents’ current COVID-19-related health status. Positive test results versus all other responses were entered as a categorical variable into the models. Parents reported whether each of their children had been diagnosed with COVID-19.
Responding Parent Vaccination History
We provided parents with a list of the recommended routine childhood vaccines and asked if they had received all those vaccines at the recommended ages, all according to a delayed schedule, were partially vaccinated, or not at all (scored from 1 to 4). We opted not to ask for this information on a vaccine-by-vaccine basis, as we anticipated significant memory difficulties at this single-vaccine level. We asked how frequently they get the flu shot (with options ranging from every year to never), and responses were scored from 1 to 4. Biological females were asked if they received the human papillomavirus (HPV) vaccine (scored 0 or 1). All participants aged >50 years were asked if they received the shingles vaccine (scored 0 or 1). Total vaccination completeness was converted to a score out of 8 to account for age and sex differences in the total number of recommended vaccines. Parents were asked how many doses of the COVID-19 vaccine they had received, and how many they were eligible for.
Children’s Vaccination History
Parents completed the above vaccine completeness measures for each of their children, excluding questions about HPV and shingles vaccines. Vaccine completeness was scored out of 8. Parents reported how many doses of the COVID-19 vaccine their child(ren) had received, and how many they were eligible for.
Adverse Immunization Reactions
We asked parents if they or each of their children had ever experienced an adverse reaction to immunization. This was coded dichotomously (yes/no).
Attitudes Toward Vaccines
We assessed participants’ attitudes toward vaccinations generally using measures from Jolley and Douglas (2014). Eight questions measured the perceived dangers of vaccines (e.g., ‘vaccines lead to allergies’). Three items measured feelings of powerlessness surrounding vaccination (e.g., ‘I feel that my actions will not stop the negative outcomes of immunizations’). Perceived dangers and powerlessness were measured on a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Two questions measured trust in authorities (e.g. ‘I trust corporations to tell the truth about vaccinations’) on a Likert scale ranging from 1 (strongly distrust) to 6 (strongly trust). Responses to subscales were summed. Jolley and Douglas reported good reliability of these four measures (all αs ≥ .82). However, due to issues with collinearity of the data, only the perceived danger subscale was used. An additional attention check question was inserted into this measure. Participants were asked to leave question 10 blank. A data validity check ensures that participants are paying attention while completing the questionnaires and that we can trust the validity of the results.
Omission Bias
The strength of the omission bias concerning the COVID-19 vaccine was measured using modified materials from Hamilton-West (Hamilton-West, 2006). All references to the MMR vaccine were replaced with the SARS-CoV-2 vaccine. To calculate omission bias, two variables were needed: (1) risks associated with not vaccinating (total COVID-19 risk perception mean × risks of COVID-19 if not vaccinated) and (2) risks associated with vaccinating (risk of COVID-19 if vaccinated × total COVID-19 risk perception, plus risk of COVID-19 vaccine side effects × severity of side effects). The risks associated with vaccinating were subtracted from the risks associated with not vaccinating, and negative scores indicate perceived greater risk associated with vaccinating, and a likely tendency to prefer inaction/non-vaccination (i.e. negative scores are associated with greater omission bias).
COVID-19 Risk Perceptions
Participants rated, on a scale from 1 (no risk) to 5 (very serious risk), how much risk COVID-19 poses to them personally, to their family, to their community, and to humankind (4 items). Personal and family ratings were summed (proximal risk), as were community and humankind ratings (distal risk). These items were used, with permission, from unpublished data (Santistevan & Bliss-Moreau, 2020).
Psychological Distance
To measure psychological distance, we asked participants how many people that they knew who had been diagnosed with COVID-19 and how close their relationship was to each person(s) (to a maximum of five people) ranging from 1 (distant acquaintances) to 100 (very close relationship). These values were averaged to form a relationship score. For each of these five people, participants were asked to rate their health outcome from 1 (deceased as a result of COVID-19) to 100 (recovered at home with little or no medical intervention). These values were averaged to create an outcome score.
ZIP code data were used to extract the severity of the COVID-19 pandemic in the participant’s county from two interactive websites which derive their data from the CDC. This was done in two ways – (1) the number of positive cases in the last week prior to completing the surveys (USA Facts, 2021a), and (2) the number of total COVID diagnoses per 100, 000 people in their county over the entire pandemic (USA Facts, 2021b). The CDC regularly updates the number of COVID-19 cases, deaths, and other trends by county. We asked for ZIP code rather than county to improve accuracy.
Impact of the COVID-19 Pandemic
The subjective impact of the COVID-19 pandemic was assessed using The Impact of Event Scale for COVID-19 (Vanaken, 2020). The scale is comprised of 15 items forming two subscales: the Intrusion subscale includes 7 items (e.g., ‘I thought about it when I didn’t mean to’), and the Avoidance subscale includes 8 items (e.g., ‘I avoided letting myself get upset when I thought about it or was reminded of it’). All responses were scored on a Likert scale ranging from 1 (not at all) to 4 (often). An additional manipulation or attention check was included as item 8. Participants were asked to choose ‘sometimes’ for this item.
Anxiety
We measured anxiety with the anxiety subscale of the Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995) The DASS-21 shows extremely good psychometric properties. The anxiety subscale includes 7 items measuring anxious experiences in the last week, including ‘I was worried about situations in which I might panic and make a fool of myself’, and are responded to from zero (did not apply to me at all) to 3 (applied to me very much, or most of the time).
Outcome Variables
SARS-CoV 2 Vaccination Intentions
Participants were asked to report on a scale from 1 to 100, how likely they would be to receive a vaccination and how likely they would be to have their child(ren) vaccinated against SARS-CoV-2 in the event that vaccine is approved for their child’s age range by the CDC. They were asked how quickly they would or did get themselves and each of their children vaccinated ranging from 1 (as soon as the vaccine is available in my area) to 5 (I would not get them vaccinated for SARS-CoV-2).
Data Analysis
Survey Sample Size Estimation
In questionnaire research, sample size is the number of completed responses a survey receives. When the population size N is very large (e.g., all US families with children as in our survey), the sample size is n =
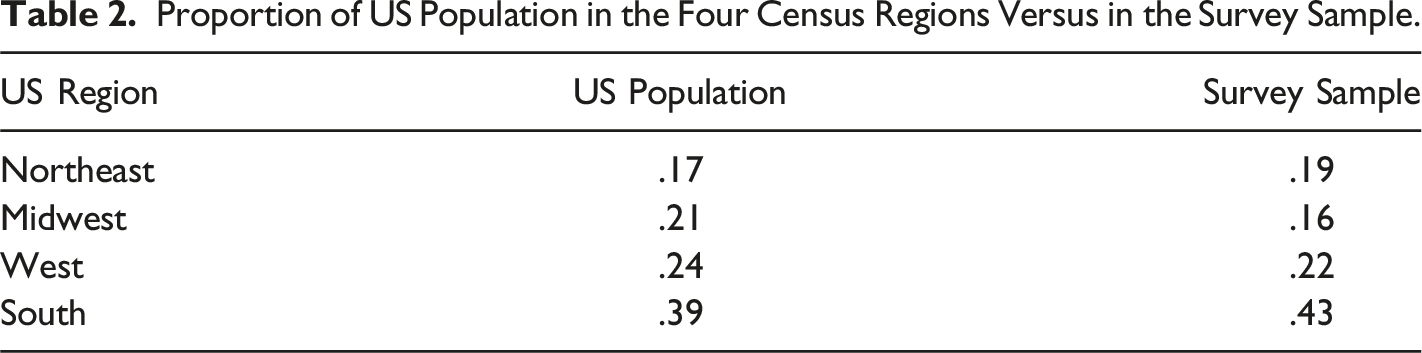
Proportion of US Population in the Four Census Regions Versus in the Survey Sample.
All data were analyzed using the statistical package R (R Core Team, 2019). To model the likelihood of having their child(ren) vaccinated, considering that children in the same family are not independent, we applied a multi-level mixed-effects (MLM) model (Gelman & Hill, 2006), that tackles the nested relations between the children and family and between the family and geographic regions. The lme4 method (Bates et al., 2015) was used to run a MLM with random intercepts. Another way to model vaccination likelihood, while removing the effects of the natural dependencies among the observations within families, was to average vaccination likelihoods and average each child-level variable within a family and then model the average likelihood as a linear function of the averaged child-level explanatory variables and the parent-level explanatory variables, using an ordinary least square (OLS) regression, and the results of this analysis are included in Supplementary materials.
Multicollinearity among the independent variables in the linear and linear mixed-effects models was addressed using a variance inflation factor (VIF) analysis. VIF greater than 5 indicates significant multicollinearity and the responsible variable may need to be removed from the models. All variables in the final linear models had a VIF of <4 and therefore multicollinearity was not a significant problem. 2
To analyze the speed of vaccination, a categorical variable, a proportional odds logistic regression (polr) model for ordinal logistic regression (McCullagh, 1980) was applied. Vaccination speed was ranked from the fastest to the slowest: as soon as possible (ASAP), within weeks (Weeks), within months (Months), within a year or more (1 Year or more), and Never. Under a polr model, the event being modeled is the cumulative probability of the speed being less than or equal to a specific category. For vaccination speed, the possible cumulative groups of outcomes are: 1. ASAP 2. ASAP or Weeks 3. ASAP, Weeks, or Months 4. ASAP, Weeks, Months, or 1 Year or more 5. ASAP, Weeks, Months, 1 Year or more, or Never
Under the polr model, each of the above outcome groups has the same regression coefficients and a different intercept (the cut points between the speed categories). Regression coefficients, when exponentiated, represent the odds ratio for a one-unit change in the predictor being associated with an increase or decrease (depending on the sign of the coefficient) in the odds that the outcome variable is in one of the outcome groups (vs. not in that particular group). For instance, relative to the ‘Extremely/moderately liberal’ political beliefs as a reference group, the coefficient for ‘Moderately or Extremely conservative’ is, say, −.40. This means a change in political beliefs from the more liberal group to the more conservative group is expected to decrease the log odds of being in the ASAP speed versus all other speed categories by .4; so the odds for being in the ASAP speed group is reduced by 1-e−0.4 = .33 for the more conservative groups. Similarly, this political belief also decreases the odds for being in the ASAP or Weeks group versus all other speeds by .33. As with vaccination likelihood, vaccination speeds are not independent from each other in the same family. Therefore, we used averaged vaccination speed within families as the outcome variable and the explanatory variables pertaining to children within the same family were averaged.
Ideally, the above polr can combine with random effects modeling to account for the nested relations between children, family, and geographical regions. However, such a multi-level ordinal logistic regression model is not available in R or other statistical software packages. Instead, we built an ordinal regression with random intercepts to account for clustering effects of the US regions. Cumulative Link Mixed Models (CLMM) implemented in the ‘ordinal’ package was used. Furthermore, we had to reduce the number of vaccine speeds down to three categories, corresponding to ASAP, Weeks or Months, and over one year or never, from the original five levels in order to let CLMM run the model without having difficulties in numerical convergence.
Results
Vaccination Likelihood
Multi-Level Linear Model With Random Intercept for the Likelihood of Having Individual Children Vaccinated.
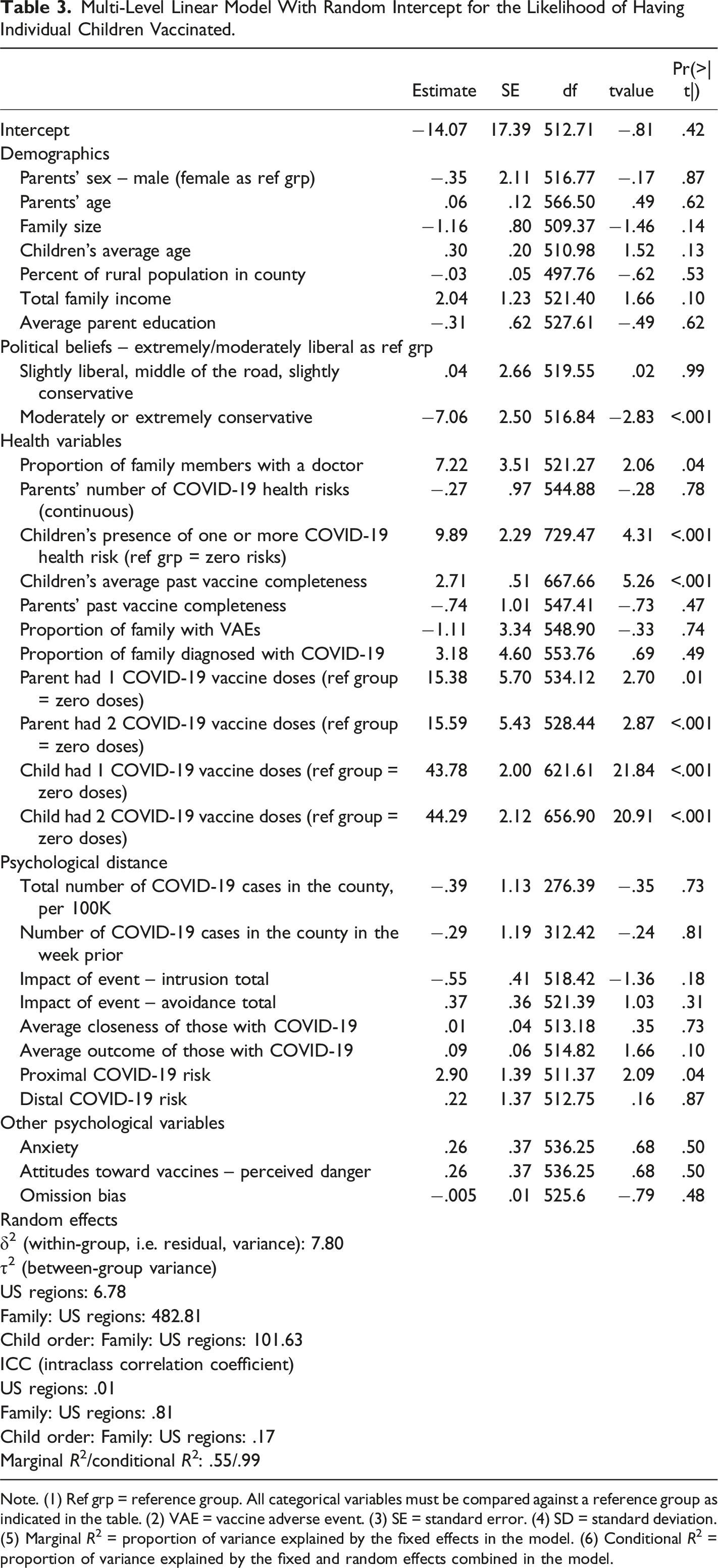
Note. (1) Ref grp = reference group. All categorical variables must be compared against a reference group as indicated in the table. (2) VAE = vaccine adverse event. (3) SE = standard error. (4) SD = standard deviation. (5) Marginal R2 = proportion of variance explained by the fixed effects in the model. (6) Conditional R2 = proportion of variance explained by the fixed and random effects combined in the model.
A second linear model for vaccination likelihood modeled average likelihood within a family as a function of averaged family-level independent variables to account for the clustering effect of children within families. Similar results were obtained, with the addition that higher total family income became a marginally significant correlate of increased average vaccination likelihood (p = .07). The within-family average vaccination likelihood model showed that those in the Northeast of the USA were more likely to vaccinate their children on average, than those in the West. Results of the non-nested model for average child vaccine likelihood can be found in the Supplementary materials (Table 1).
Vaccination Speed
Ordinal Regression Model Predicting Average Intended Speed of Vaccination Within a Family.
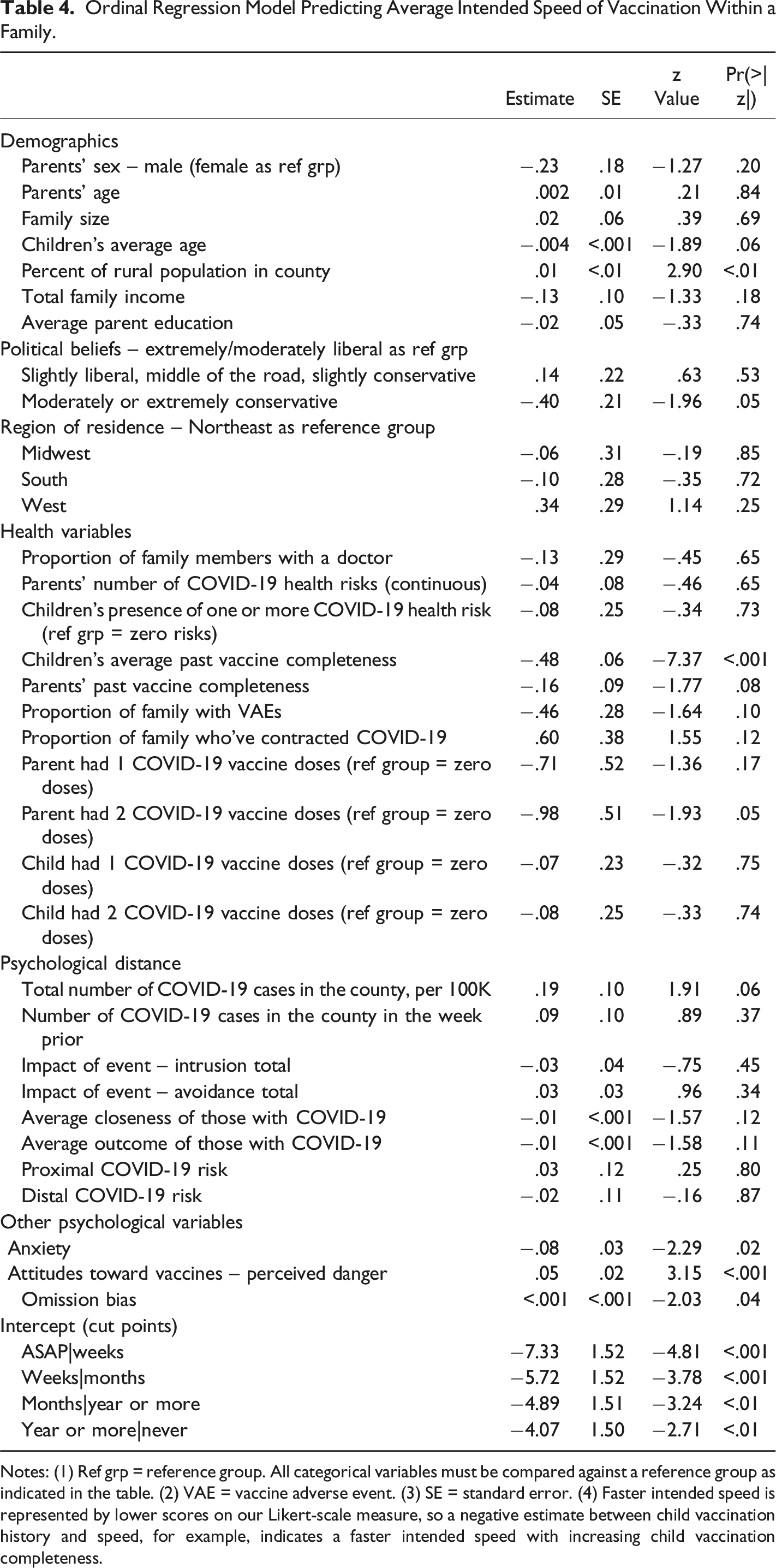
Notes: (1) Ref grp = reference group. All categorical variables must be compared against a reference group as indicated in the table. (2) VAE = vaccine adverse event. (3) SE = standard error. (4) Faster intended speed is represented by lower scores on our Likert-scale measure, so a negative estimate between child vaccination history and speed, for example, indicates a faster intended speed with increasing child vaccination completeness.
Ordinal Regression Model With Random Intercepts for Regions of USA Predicting Average Child Vaccination Speed.
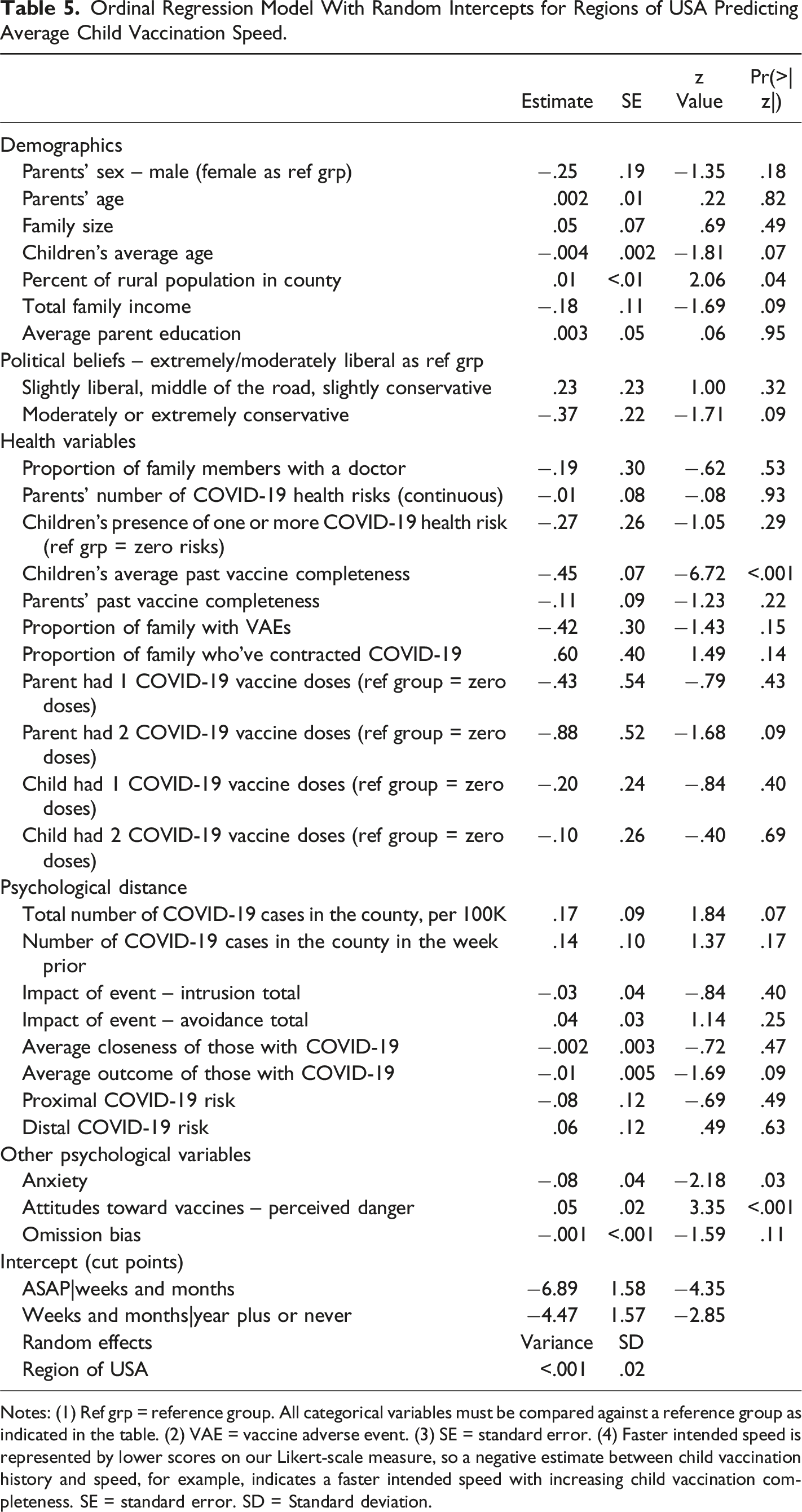
Notes: (1) Ref grp = reference group. All categorical variables must be compared against a reference group as indicated in the table. (2) VAE = vaccine adverse event. (3) SE = standard error. (4) Faster intended speed is represented by lower scores on our Likert-scale measure, so a negative estimate between child vaccination history and speed, for example, indicates a faster intended speed with increasing child vaccination completeness. SE = standard error. SD = Standard deviation.
Discussion
Since the early stages of the COVID-19 pandemic, researchers have been working to develop vaccines against SARS-CoV-2, but these vaccines are rendered ineffective if not accepted by the public, and this includes whether parents choose to vaccinate their child(ren) and how quickly they chose to do so. This cross-sectional study explored a series of explanatory variables for intending to vaccinate children just as the CDC was rolling out their immunization campaign for this age group. Following from Lackner and Wang (2021) we examined correlates of the likelihood and speed with which American parents intended to have their child(ren) vaccinated.
With respect to demographic variables, political beliefs were associated with both speed and likelihood, with those reporting moderately or extremely liberal belief systems being more likely to get their child(ren) vaccinated and get them vaccinated more quickly than those with relatively more conservative belief systems. This is consistent with existing literature on self-intention literature for routine vaccination (Baumgaertner et al., 2018), COVID-19 vaccination in adults (Ruiz & Bell, 2021), and parental COVID-19 vaccine intention in United States (Ruiz & Bell, 2022). Region of USA differentiated child vaccination likelihood, with parents in the Northeast of the USA being more likely to intend to vaccinate their child(ren) than those in the West. This dovetails well with COVID-19 vaccine uptake rates (rather than just intentions) as being higher in the Northeast relative to the Midwest (CDC, 2022) and child uptake of influenza vaccination (National Center for Health Statistics, 2019), perhaps related to differences in political beliefs (Baumgaertner et al., 2018). Socioeconomic variables such as average education and income were not associated with speed or likelihood, in agreement with Lackner and Wang (2021) and 8/29 (education) and 11/20 (income) studies included in Galanis et al.’s (2022) global meta-analysis of the correlates of child COVID-19 vaccination likelihood. As Humble et al. (2021) postulate, it may be that when associations with parental education are uncovered, they are reflections of other factors including perceptions of disease or vaccine risk, rather than pure associations with educational attainment. Children’s age was marginally associated with speed of intended vaccination, with parents of older children intending to have those children vaccinated faster than younger children. Little literature to date has examined the speed with which parents choose to vaccinate their child(ren), but McKinnon et al. (2021) reported higher COVID-19 vaccine intentions among parents of older children, yet of the 16 studies included in Galanis et al.’s meta-analysis (2022) which examined child age, only 4/16 found a positive association between increased child age and increased likelihood. Parent and child age are highly, but not perfectly, correlated and detailing how each independently contributes to vaccination speeds and intentions is worthwhile. Nonetheless, we found significant demographic explanatory variables (political beliefs, census region, and area rurality) of child vaccine speed and likelihood.
With respect to psychologically-relevant independent variables, parents’ anxiety during the week prior to the survey was associated with faster vaccination speed, but the impact of the COVID-19 pandemic on intrusive and avoidant thought patterns did not associate with either speed or likelihood. This pattern of mental health findings is somewhat different than in the Canadian sample responding to Lackner and Wang (2021) who found no associations with trait or state anxiety and vaccination speeds or likelihoods but did find marginally significant associations between avoidance and likelihood, and significant associations between avoidance and speed. The current association between anxiety and increased vaccination speed and the lack of association in Lackner and Wang (2021) can be contextualized by the work of Mohammed et al. (2020) who found that mothers with mild anxiety symptoms were more likely to receive the influenza and pertussis vaccine during pregnancy than their counterparts with no or high levels of anxiety symptoms. Anxiety levels have decreased over the course of the pandemic (Hajek et al., 2022), and so it could be that high levels of anxiety were captured in Lackner and Wang (2021) and therefore did not relate to vaccination speeds and likelihoods and now that anxiety levels are somewhat lower, anxiety is now correlated with intended vaccination speed. However, the two studies used different measures of anxiety (the State-Trait Anxiety Inventory vs. the DASS-21) and so direct comparisons in mean levels of anxiety are not possible. The lack of association between COVID-19-related intrusive and avoidant thought patterns and speed and likelihood of vaccination could be due to improved mental health at this later rather than earlier stage of the pandemic (Hajek et al., 2022) and/or sociopolitical differences between the two sample locations (Canada vs. USA).
The perceived danger of vaccines more generally correlated with vaccination speed, but not likelihood. Although not assessed presently, vaccine hesitant parents may have viewed vaccination of their children as unavoidable (e.g., as a necessary step toward easing lock-down measures, returning to school or daycare [Ruggiero et al., 2021]), but wanted to delay the receipt of vaccines for as long as possible, thus creating the association with speed, but not likelihood. Participants who preferred to accept the risks of not being vaccinated against SARS-CoV-2 (e.g., increased risk of getting COVID-19) relative to the risks of being vaccinated (e.g., side effects) score high on omission bias. Individuals high in omission bias intended to delay their child(ren)’s vaccination for longer. Again speed, but not likelihood, was associated with this variable, underscoring the importance of looking at these separately.
With respect to health-related independent variables, the proportion of family members with a family doctor was associated with increased likelihood, but not speed. Strong relationships with primary healthcare providers have been associated with confidence in vaccines generally (Nowak & Cacciatore, 2017) and doctor recommendations are associated with H1N1 vaccine uptake (Ramsey & Marczinski, 2011). Given that most vaccinations occurred at mass community vaccination clinics (FEMA, 2022), it may be that the speed of vaccination is somewhat independent from the relationship that one has with their physician. Further, the presence of children’s COVID-19 health risks was associated with increased likelihood, and inconsistently linked with speed. Ruggiero et al. (2021) similarly found that parents of children with chronic illnesses were more likely to vaccinate their children, but this was not a robust finding in Galanis et al. (2022). Additionally, children’s past vaccine completeness was associated with both likelihood and speed, in concert with Galanis et al. (2022), and previous literature on other vaccine types (H1N1 [Galarce et al., 2011; Kaboli et al., 2010; Maltezou et al., 2010; Ramsey & Marczinski, 2022], seasonal influenza [Fuchs, 2016], and MMR [Flynn & Ogden, 2004]).
Psychological distance has previously been associated with the probability of perceiving and reacting to disease threats (White et al., 2014), and some of our variables related to psychological distance were associated with vaccination speeds and likelihoods. Primarily, the severity of the COVID-19 outbreak was marginally associated with increased speed, and this result remained even when the nested relationships among region of the USA were accounted for. Perhaps high rates of COVID-19 transmission in one’s county motivates parents to vaccinate their children faster. The perceived threat of COVID-19 to oneself and one’s family was related to an increased likelihood of vaccination in agreement with 4/6 studies in Galanis et al. (2022). Not all psychological distance variables were similarly associated. Psychological distance is likely a multi-faceted phenomenon with several dissociable subcomponents (White et al., 2014).
Theoretical Implications
Several theoretical frameworks have been developed or applied to understand the determinants of COVID-19 vaccine hesitancy in adults. These include the health belief model (e.g., Limbu et al., 2022), the theory of planned behavior (e.g., Hayashi et al., 2022), the protection motivation theory (e.g., Eberhardt & Ling, 2021), and others. Importantly, the predictions of each of these models should be qualified by including mediating or moderating variables, and psychosocial variables such as the ones considered in the present investigation have been given less weight (Limbu et al., 2022). Some research has applied these frameworks to understand COVID-19 vaccination intentions for children (e.g., Ellithorpe et al., 2022; Wan et al., 2022), but to our knowledge none have applied it to understand COVID-19 vaccination speeds for children.
Practical Implications
The findings from this and other studies may contain key suggestions for practitioners. First, past research on anxiety and vaccinations point to the utility of health practitioners probing for parents’ general anxiety levels when discussing intentions to vaccinate their children. Second, speed, but not likelihood, was associated with perceived vaccine risks, thus demonstrating the importance of healthcare professionals and public messaging campaigns to explicitly address risk/benefit analyses when communicating with parents, to encourage slower, analytic decision-making, rather than a fast, intuitive one (Musiienko, 2021). Third, the proportion of family members with a family doctor was associated with intended speed. Together with previous literature (Nowak & Cacciatore, 2017; Ramsey & Marczinski, 2011), this underscores the importance of developing a sense of trust with medical and public-health professionals including staff at vaccination clinics and public-facing health authorities (e.g., CDC Director Robert Redfield). Fourth, past vaccine completeness was associated with both likelihood and speed. Thus, targeting messages to previously unvaccinated groups may be required to increase COVID-19 vaccine uptake in children. Fifth, the perceived threat of COVID-19 to oneself and one’s family was related to an increased likelihood of vaccination. Our results suggest that balanced and honest conversations about risks to parents and their families may increase vaccine uptake in children. Sixth, severity of the COVID-19 outbreak in one’s area was marginally related with increased speed. Therefore, areas with slower rates of transmission may need to be a focus of public-health professional’s messaging campaigns to increase vaccination uptake in children and promote herd immunity in these regions. It would be wise for federal-level programs including Healthy People 2030 (OASH, 2023) to continue their campaigns, but to add goals targeted at increasing COVID-19 vaccination uptake in children to their objectives.
Limitations and Future Directions
Our study is limited in its data capture during a narrow window of the COVID-19 pandemic. Due to the dynamic nature of the pandemic and shifting correlates of intent to vaccinate across time and location, it is wise to revisit parental intentions to vaccinate their children at regular intervals (Salmon & Dudley, 2020). Further, while our sample was sizeable, and well-powered enough for the majority of our analyses, we had to reduce the number of vaccination speeds down to 3 in our CLMM model to allow it to run. The reduced temporal precision of these analyses could be seen as a limitation.
As above, further work needs to be done to better understand the conditions with which child age and COVID-19 vaccination likelihood and speed are related. We uncovered a marginally significant association with speed, but others have found more robust associations with likelihood. Additionally, we found associations between increased anxiety and increased speed, while Mohammed et al. (2020) found associations in the opposite direction for maternal vaccines. This points to the utility of examining curvilinear relationships of anxiety to vaccination intentions. Last, we found that increased health risks were associated with increased likelihood of vaccination, but Galanis et al.’s (2022) meta-analysis shows mixed support for this finding. Further research on subtypes of chronic illness (e.g., immunocompromised conditions vs. not) may be warranted.
Conclusions
In sum, we found several explanatory variables of parental intentions to vaccinate their child(ren) in the fifth wave of the COVID-19 pandemic in the USA, some of which differed when likelihood versus speed were used as dependent variables. Further, our results both agreed with and disagreed with Galanis et al. (2022), and further work is needed to clarify the reasons for these differences.
Supplemental Material
Supplemental Material - Predictors of Intention to Vaccinate or Continue to Vaccinate Children Against SARS-CoV-2 During the Fifth Wave of the COVID-19 Pandemic in the USA
Supplemental Material for Predictors of Intention to Vaccinate or Continue to Vaccinate Children Against SARS-CoV-2 During the Fifth Wave of the COVID-19 Pandemic in the USA by Christine L. Lackner, and Charles H. Wang in Psychological Reports.
Footnotes
Acknowledgments
The authors thank Dominic Mantilla, Putnam Valley High School, for his help with entering the COVID-19 severity, ZIP code, and rurality data and Jerry Zupan, Putnam Valley High school, for mentoring Dominic. The authors also thank Jianwen Wang for her editorial suggestions.
Author Contributions
C.L.L. was responsible for acquiring funds, the study design, data collection, some data analysis, and drafting the manuscript. C.H.W. was responsible for the statistical modelling and reviewing drafts of the manuscript. Both authors have approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Mount Saint Vincent University under a Rapid Response COVID-19 Grant and the Mantilla Family.
Ethical Statement
Data Availability Statement
Data sets were generated or analyzed, but we do not have the permission from our ethics board to share the files.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.