
Abstract
This study investigates the impact of self-handicapping on psychiatric symptoms among students, focusing on the moderating role of authenticity. A total of 260 Pakistani students from various schools and colleges participated in the study through purposive sampling. Data were collected using the Self-Handicapping Questionnaire, the Four-Dimensional Symptoms Questionnaire, and the Authenticity Scale. Results indicate that self-handicapping significantly predicts psychiatric symptoms such as depression, anxiety, and distress. Furthermore, authenticity was found to moderate these relationships, suggesting that higher levels of authenticity can buffer the negative effects of selfhandicapping on mental health. The findings emphasize the importance of addressing self-defeating behaviours and promoting authenticity as part of mental health interventions in educational settings. These insights are valuable for educators and mental health professionals aiming to improve student well-being.
Introduction
Mental health challenges, including depression, anxiety, and stress, have become increasingly common among students in recent years. These psychiatric symptoms not only interfere with academic achievement but also undermine overall well-being (American College Health Association, 2021). Among the many factors contributing to poor mental health, self-handicapping has received significant attention. Self-handicapping refers to the tendency to create obstacles or excuses to protect one’s self-esteem in the face of potential failure (Urdan & Midgley, 2001). Although this behavior may offer temporary relief, it often leads to long-term negative consequences such as poor performance, heightened stress, and worsening psychiatric symptoms. Jones and Berglas (1978) first conceptualized self-handicapping as a self-esteem defense strategy, and subsequent research has consistently linked it to anxiety, depression, and academic underachievement (Martin et al., 2001; Zuckerman & Tsai, 2005). Among students, common self-handicapping behaviors such as procrastination and avoidance not only intensify stress but also fuel a cycle of poor coping and declining mental health (Schwinger et al., 2014).
In contrast, authenticity—defined as living in alignment with one’s true self—appears to serve as a protective factor against psychological distress (Harter, 2002; Kernis & Goldman, 2006). Authentic individuals are more likely to confront challenges directly, employ adaptive coping strategies, and maintain emotional well-being (Wood et al., 2008). Evidence suggests that authenticity reduces the tendency to engage in self-defeating behaviors like self-handicapping, thereby fostering resilience. Several studies provide empirical support for authenticity as a buffer against mental health difficulties. For example, research has shown that authenticity is positively associated with life satisfaction, self-esteem, and adaptive coping, while negatively related to anxiety, depression, and stress (Wood et al., 2008). In educational settings, authentic students are more likely to demonstrate persistence, intrinsic motivation, and effective self-regulation. Conversely, when students experience a disconnect between their actions and true self, they may be more vulnerable to engaging in self-defeating behaviors such as self-handicapping. Despite these insights, the specific role of authenticity in moderating the relationship between self-handicapping and psychiatric symptoms remains underexplored. Most existing studies have examined self-handicapping, authenticity, and psychiatric symptoms separately rather than integrating them into a unified framework. This fragmentation has limited our understanding of how these constructs interact to influence student mental health. Moreover, much of the available literature comes from Western contexts, with relatively little empirical evidence from South Asian populations. Considering the unique cultural, academic, and social stressors experienced by students in this region, it is important to investigate these relationships in a non-Western context to enhance both theoretical understanding and practical interventions.
The present study addresses this gap by examining the predictive role of self-handicapping on psychiatric symptoms—specifically depression, anxiety, and stress—while exploring the moderating role of authenticity. It is hypothesized that students with higher levels of self-handicapping will report greater psychiatric symptoms, consistent with prior evidence of its maladaptive consequences. At the same time, authenticity is expected to buffer this relationship by weakening the association between self-handicapping and psychiatric symptoms. By integrating these variables into a single framework, this research aims to make several contributions. First, it highlights self-handicapping as a risk factor for poor mental health among students. Second, it identifies authenticity as a potential protective mechanism, offering insights into psychological strengths that can be cultivated in educational contexts. Finally, the findings may inform targeted interventions for teachers, counselors, and mental health practitioners, who can design strategies to reduce self-handicapping behaviors and foster authenticity. In doing so, this study contributes to ongoing efforts to promote resilience, academic success, and mental well-being among students.
Method
Study Design
The study employed a cross-sectional survey design to examine the interrelationships among self-handicapping, psychiatric symptoms, and authenticity among adolescents and young adults.
Ethical Consideration
The study was conducted in accordance with the ethical standards of the American Psychological Association and the Declaration of Helsinki. Ethical approval was obtained from the University of Sargodha, Institutional Ethics Committee for Research [RefSU/PSY/990-S]. This study was approved by the Department of Psychology, University of Sargodha. Pakistan. Participants provided informed consent before data collection, and for participants, consent was additionally obtained from their parents/guardians. Confidentiality, anonymity, and the voluntary nature of participation were assured.
Sample
Data were collected over a period of four months (Nov 2024 to Feb 2025). A total of 260 students (N = 260) were recruited from multiple educational institutions, including schools, colleges, and universities, to obtain a representative sample across different educational levels. The final sample consisted of students aged 11–25 years from schools, colleges, and universities in both urban and semi-urban areas. The sample included 135 males and 125 females, representing a fairly balanced gender distribution.
Inclusion Criteria
• Students enrolled in secondary school, college, or university. • Age range between 11 and 25 years. • Ability to understand and complete the questionnaires in English. • Provision of informed consent (and parental/guardian consent for minors).
Exclusion Criteria
• Individuals with a prior diagnosed psychiatric disorder under treatment. • Students with significant cognitive or developmental impairments that could affect their ability to complete the survey.
Measures
The Self-Handicapping Questionnaire (adapted from Jones & Rhodewalt, 1982) was used to measure self-handicapping behaviors. The scale consisted of 10 self-report items designed to assess the extent to which individuals engage in self-handicapping strategies. Responses were recorded on a six-point Likert scale ranging from “Disagree Very Much” to “Agree Very Much.” The SHQ has demonstrated good internal consistency (α = .78–.86) and construct validity across student populations.
The Four-Dimensional Symptoms Questionnaire (4DSQ; Terluin et al., 2006) was used to assess three dimensions of psychological symptoms: anxiety, distress, and depression. While the original scale also measures somatization, this study focused solely on anxiety, distress, and depression. The 4DSQ evaluates bodily distress, the severity of psychological suffering (distress), and specific symptoms of depressive and anxiety disorders. The scale has demonstrated good reliability, with an alpha coefficient of .77 in previous research. The Authenticity Scale developed by Wood et al. (2008) was employed to measure authenticity, which comprises three dimensions: self-alienation, authentic living, and accepting external influence. The scale consists of 12 items rated on a seven-point Likert scale ranging from 1 (“Does not describe me at all”) to 7 (“Describes me very well”). The scale has been widely used and validated in diverse populations.
Procedure
After securing institutional approvals, permission was obtained from school/college authorities. Surveys were administered in classroom or designated settings. Participants were briefed about the study’s purpose, confidentiality, and voluntary participation before completing the instruments. Collected data has been empirically analyzed through SPSS v24.
Results
Mean Standard Deviation, Range and Skewness of Study Variables (N = 260)
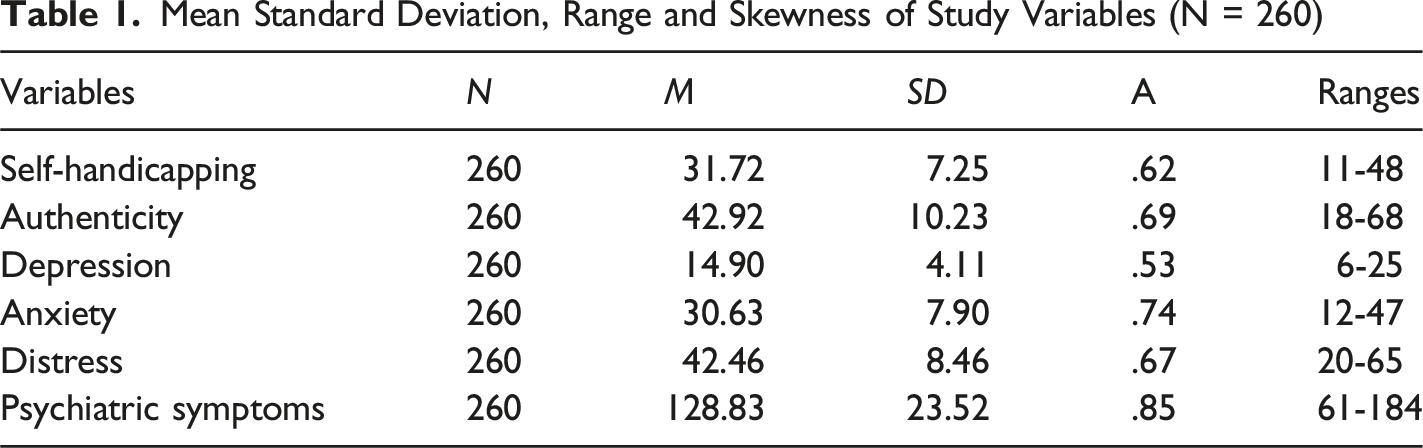
Findings of pearson correlation indicated that self-handicapping is positively correlated with distress, depression and anxiety. Distress positively correlates with depression and anxiety. All the variables are positively correlated with each other. And the values are significant which shows that self-handicapping can positively correlated with psychiatric symptoms, and authenticity. So, the theoretical relationship among self-handicapping, authenticity and psychiatric symptoms has supported by the empirical results. It is Indicated in this study that self-handicapping as predicting variables of psychiatric symptoms i.e. depression, anxiety, distress. Model found significant with (F (1, 258) = 5.19, p < .05), suggesting that self-handicapping predict depression account for 5% variance in the outcome variable (i.e. depression) (R 2 = .05). Further, it is observed that predictor variables predict out variables in positive direction. Self-handicapping predicts (β = .14, t = 2.27, p < .05). 2nd model is found significant with (F (1, 258) = 3.88, p < .05), suggesting that self-handicapping predict anxiety for 4% variance in the outcome variable (i.e. anxiety) (R 2 = .04). Further, it is observed that predictor variables predict out variables in positive direction. Self-handicapping predicts (β = .12, t = 1.97, p < .05) anxiety. 3rd model is found significant with (F (1, 258) = 12.19, p < .001), suggesting that self-handicapping predict stress for 6% variance in the outcome variable (i.e. stress) (R 2 = .06). Further, it is observed that predictor variables predict out variables in positive direction. Self-handicapping predicts (β = .21, t = 3.49, p < .001) stress.
The findings also demonstrate the authenticity as moderator in relationship of self-handicapping and anxiety (see Figure 1). First model explain the prediction of self-handicapping. It is observed that first model is significant for self-handicapping (ΔR
2
= .01, F (1, 258) = 3.98, p < .05). Self-handicapping is found to be a predictor of anxiety (β = .13, t = 2.10, p < .05) and it has been found contributing for 1% variance in the outcome variable (R
2
= 1). In second model self-handicapping and authenticity entered in the prediction values list. Findings indicate that significant with (ΔR
2
= .02, F (2,257) = 3.49, p < .05). Self-handicapping is found to be a non-significant predictor (β = .06, t = .88, p > .05) and authenticity is also shows as non-significant predictor for anxiety (β = .09, t = .75, p > .05). When both values are entered in the predictor list, 4% variance in the dependent variable (R
2
= .04). The third model presents an interaction of self-handicapping and authenticity predicting anxiety. Overall model is found significant with (ΔR
2
= .03 F (3,256) = 3.57, p < .05) and product of self-handicapping and authenticity predict the dependent variable with (β = .87, t = 2.50, p < .05). Therefore, these variables cause 6% variance in dependent variable the total variance is strong enough to cause a significant impact on outcome variable (R
2
= 0.06). Authenticity as Moderator of the Relationship Between Self-Handicapping and Anxiety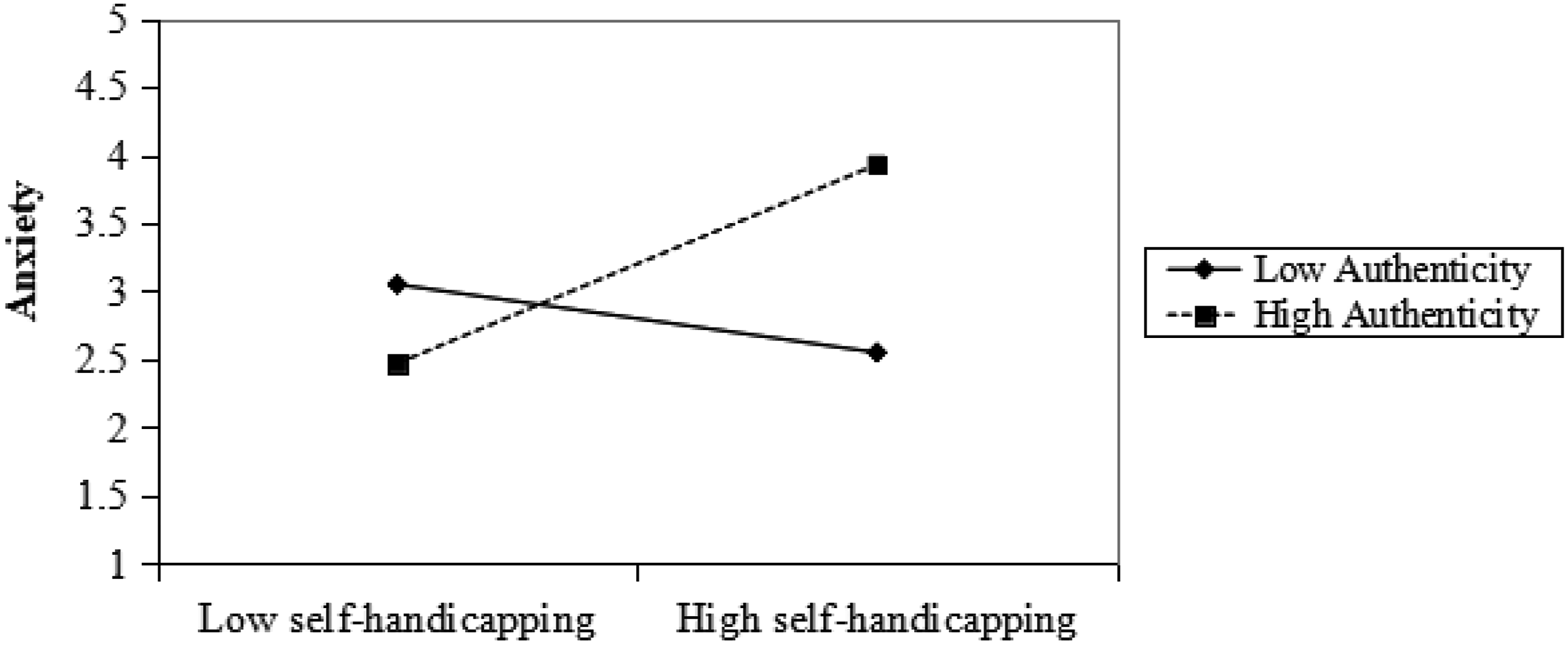
The moderated role of authenticity between depression and self-handicapping has been calculated which demonstrates the authenticity as moderator in relationship of self-handicapping and depression. First model explain the prediction of self-handicapping. It is observed that first model is significant for self-handicapping (ΔR
2
= .02, F (1,257) = 5.19, p < .05). Self-handicapping is found to be a predictor of depression (β = .12, t = 2.37, p < .05) and it has been found contributing for 4% variance in the outcome variable (R
2
= .04). In second model self-handicapping and authenticity entered in the prediction values list. Findings indicate that significant with (ΔR2 = .01, F (2,256) = 3.01, p < .05). self-handicapping is found to be a significant predictor (β = .08, t = 2.20, p < .05) and authenticity is shows as non-significant predictor for depression (β = .03, t = 1.70, p > .05). When both values are entered in the predictor list, 1% variance in the dependent variable (R2 = .01). The third model presents an interaction of self-handicapping and authenticity predicting depression. Overall model is found significant with (ΔR2 = .03, F (3, 255) = 3.13, p < .05) and product of self-handicapping and authenticity predict the dependent variable with (β = .49, t = 4.79, p < .05). Therefore, these variables cause 6% variance in dependent variable the total variance is strong enough to cause a significant impact on outcome variable (R
2
= .06). Figure 2 presents authenticity as moderator of the relationship between self-handicapping and depression. Authenticity as Moderator of the Relationship Between Self-Handicapping and Depression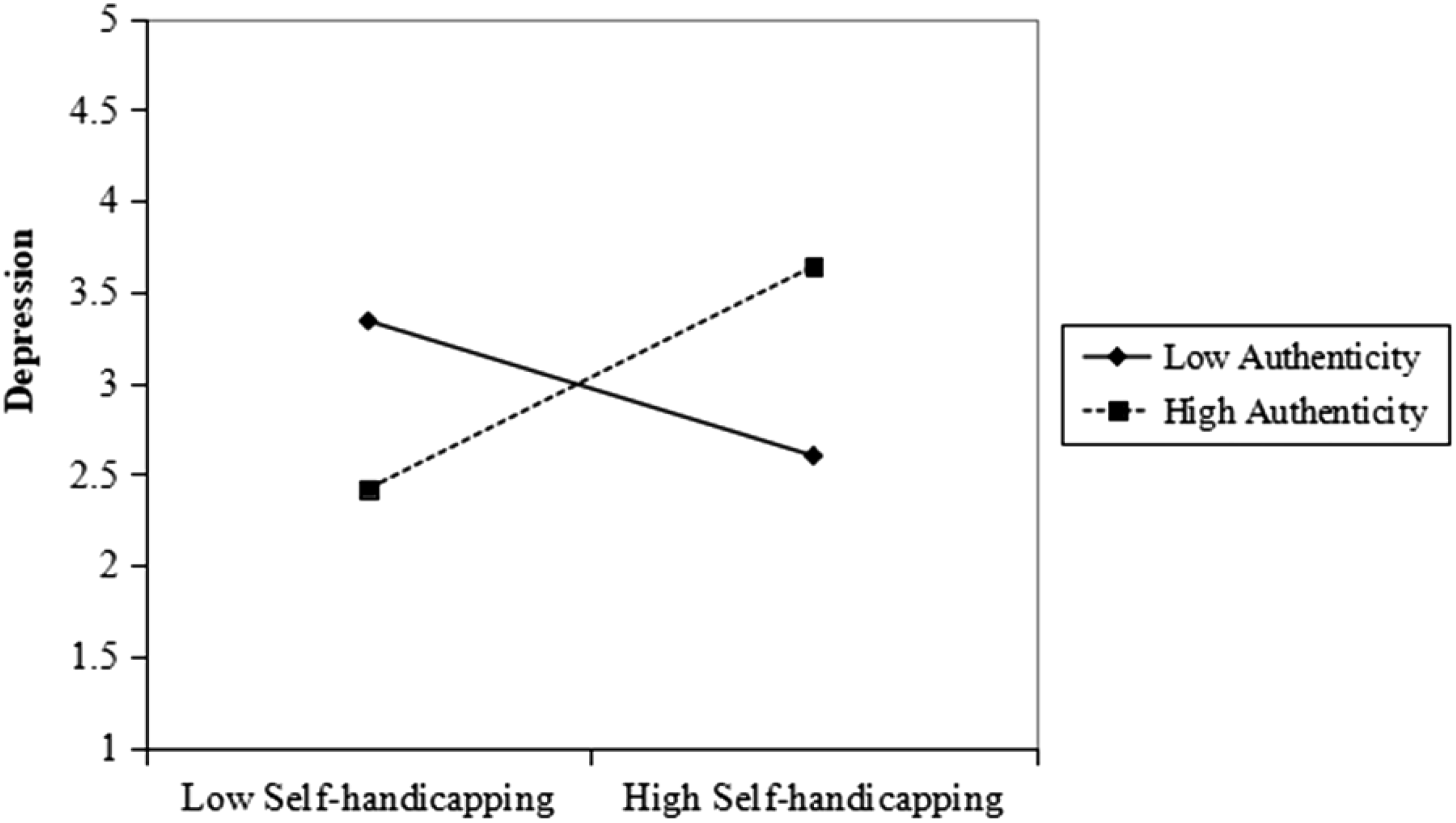
The moderated role of authenticity between distress and self-handicapping has been calculated and it demonstrates the authenticity as moderator in relationship of self-handicapping and distress. First model explain the prediction of self-handicapping. It is observed that first model is significant for self-handicapping (ΔR
2
= .04, F (1,254) = 12.19, p < .01). Self-handicapping is found to be a predictor of distress (β = .24, t = 3.49, p < .01) and it has been found contributing for 4% variance in the outcome variable (R2 = .04). In second model self-handicapping and authenticity entered in the prediction values list. Findings indicate that significant with (ΔR
2
= .08, F (2,253) = 12.62, p < .001). self-handicapping is found to be a non-significant predictor (β = .10, t = 1.36, p > .05) and authenticity is shows highly significant predictor for distress (β = .20, t = 3.53, p < .001). When both values are entered in the predictor list, 8% variance in the dependent variable (R
2
= .08). The third model presents an interaction of self-handicapping and authenticity predicting distress. Overall model is found significant with (ΔR
2
= .08, F (3,252) = 8.50, p < .001) and product of self-handicapping and authenticity predict the dependent variable with (β = .50, t = 2.49, p < .05). Therefore, these variables cause 8% variance in dependent variable the total variance is strong enough to cause a significant impact on outcome variable (R2 = .20). Figure 3 shows authenticity as moderator of the relationship between self-handicapping and distress. Authenticity as Moderator of the Relationship Between Self-Handicapping and Distress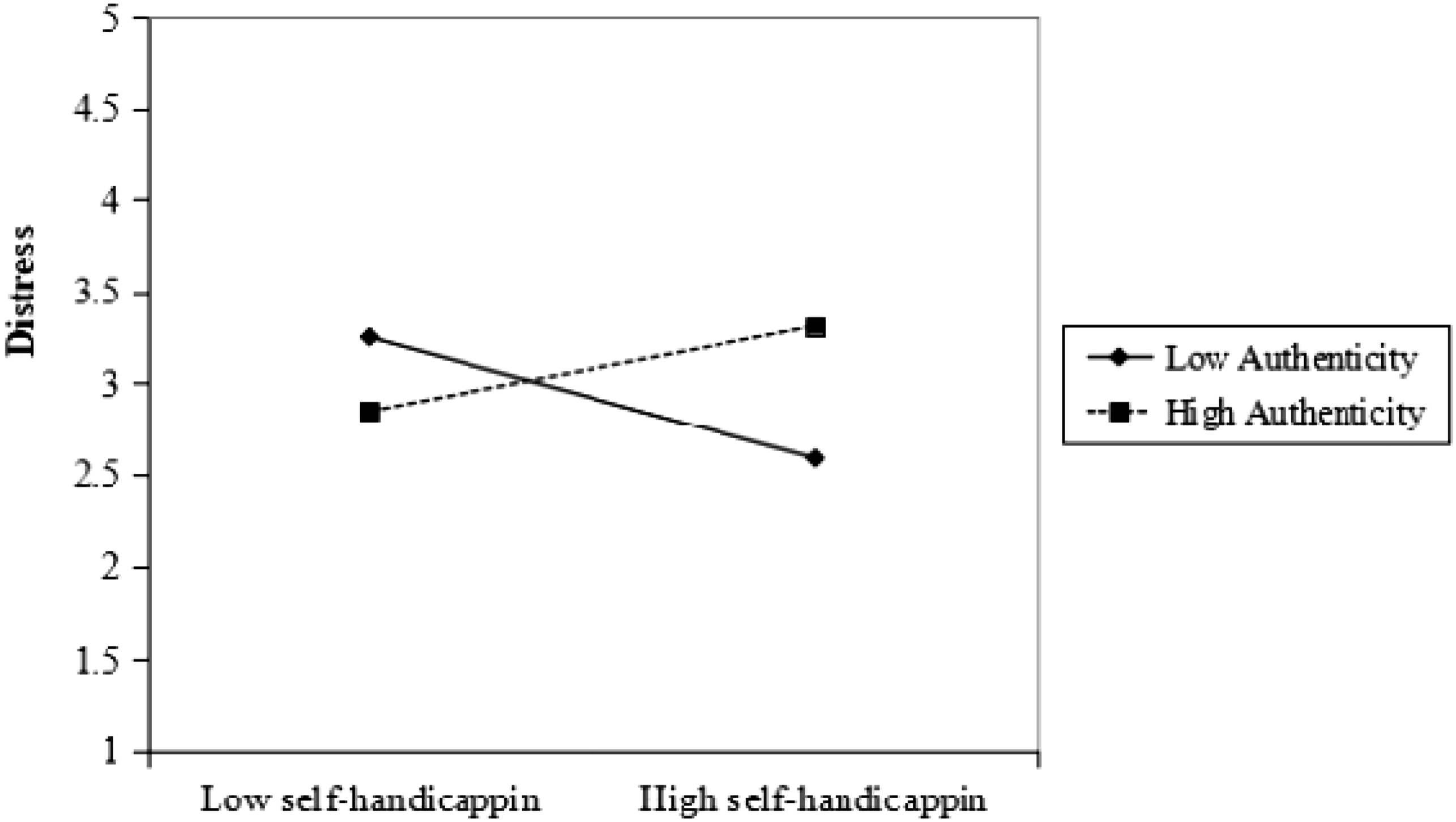
Discussion
The present study examined the predictive relationship between self-handicapping behaviors and psychiatric symptoms, including distress, depression, and anxiety, among students. The hypothesis proposed that “self-handicapping will positively predict psychiatric symptoms.” This hypothesis was tested using linear regression analysis. The results revealed that self-handicapping significantly predicted anxiety, depression, and distress at a highly significant level. These findings support previous literature, which suggests that self-handicapping behaviors are positively associated with psychiatric symptoms (Jones & Rhodewalt, 1982). The study confirms that self-handicapping is a significant predictor of mental health challenges among students. Self-handicapping refers to self-defeating behaviors that hinder an individual’s ability to perform at their best, leading to underachievement or non-performance of goals (Jones & Rhodewalt, 1982). The current findings align with previous research, which has shown that self-handicapping negatively impacts mental health, particularly in the form of increased anxiety, depression, and distress (Terluin et al., 2006). Adolescence, often considered a stressful period, can exacerbate these symptoms, as students transition from middle school to higher educational levels. Students who engage in self-handicapping behaviors often do so as a protective strategy, stemming from low self-esteem and heightened anxiety (Wood et al., 2008). The results of this study corroborate these assertions, indicating that self-handicapping behaviors are strongly linked to psychiatric symptoms.
Psychiatric symptoms such as anxiety and depression are frequently triggered by stressors that individuals are unable to cope with effectively. Previous research has emphasized that these stressors can lead to prolonged feelings of sadness, worry, and frustration, which, in turn, contribute to depression (Terluin et al., 2006). The relationship between self-handicapping and anxiety has also been observed in prior studies (Jones & Rhodewalt, 1982). Students who engage in self-handicapping behaviors often experience heightened anxiety due to their belief that they cannot perform tasks well, leading to decreased performance (Wood et al., 2008). Additionally, the study found that self-handicapping is strongly linked to depressive symptoms. Depression is often a natural consequence for students who engage in self-handicapping behaviors, though it may diminish over time as they gain confidence and develop coping skills through education. However, the study also highlights that depression can persist in some individuals throughout their lives. Teachers and educators should be aware of the potential depressive symptoms among self-handicapping students and provide encouragement and support to reduce these symptoms, thereby improving students’ academic performance.
The relationship between self-handicapping and anxiety, as observed in previous research (Jones & Rhodewalt, 1982; Wood et al., 2008), is also supported by the findings of this study. Students who engage in self-handicapping behaviors often experience anxiety due to their perceived inability to perform well. This anxiety is exacerbated by social comparisons, as students may feel that their abilities fall short compared to others. Educators should be mindful of these factors and offer additional support and motivation to self-handicapping students to alleviate their anxiety and enhance their performance. Distress, which encompasses mental, emotional, and physical tension, was also found to be positively related to self-handicapping in this study. The interaction between individuals and their environment can lead to feelings of stress, which, when unresolved, contribute to distress (Terluin et al., 2006). Social comparisons, particularly among self-handicapping students, can further intensify distress. To address this, it is important to create an environment that fosters motivation and encourages self-handicapping students to engage in social activities that help them integrate into their peer groups and reduce feelings of distress.
The role of authenticity in moderating the relationship between self-handicapping and psychiatric symptoms was also examined. Authenticity, as defined by Wood et al. (2008), refers to the extent to which individuals engage in activities that align with their true selves. Students who engage in self-handicapping behaviors are often highly sensitive to how their actions are perceived by others, leading them to adopt strategies to minimize the negative effects of self-handicapping. The study’s findings support the theoretical model, demonstrating that authenticity moderates the relationship between self-handicapping and psychiatric symptoms. This suggests that fostering authenticity in students may help mitigate the negative effects of self-handicapping behaviors on mental health. The study also highlights the gender differences in the impact of self-handicapping. Females, in particular, were found to experience higher levels of depression as a result of self-handicapping behaviors. Additionally, students at lower educational levels were more likely to experience negative effects from self-handicapping compared to those at higher educational levels. These findings underscore the importance of targeted interventions for self-handicapping students, especially females and those at lower educational levels. Educators, policymakers, and mental health professionals should focus on providing support, motivation, and confidence-building measures to help reduce the negative impact of self-handicapping behaviors.
In summary, the findings of this study emphasize the significant role of self-handicapping in predicting psychiatric symptoms, particularly anxiety, depression, and distress. The moderating role of authenticity further highlights the importance of fostering self-awareness and self-esteem in students. The study also underscores the need for targeted interventions to address the mental health challenges faced by self-handicapping students, particularly among females and those at lower educational levels. Future research should continue to explore the complex relationship between self-handicapping, psychiatric symptoms, and authenticity, as well as the potential for educational and psychological interventions to mitigate the negative effects of self-handicapping behaviors.
Conclusion, Limitations, and Recommendations
The present study highlights the significant role of self-handicapping in predicting psychiatric symptoms, including anxiety, depression, and distress, among students. The findings demonstrate that students who engage in self-handicapping behaviors are at a higher risk of experiencing adverse mental health outcomes. Importantly, authenticity was found to buffer these relationships, suggesting that fostering self-awareness, alignment with one’s true self, and adaptive coping strategies can mitigate the negative effects of self-handicapping. These results emphasize the value of promoting authenticity and personal growth within educational settings to enhance student well-being and resilience.
However, several limitations should be acknowledged. The study employed a cross-sectional design, which restricts the ability to infer causal relationships between self-handicapping and psychiatric symptoms. Additionally, data were collected through self-report questionnaires, which may be influenced by social desirability or subjective bias. The sample, drawn from students in Pakistan, may not fully represent the diversity of experiences in other cultural or educational contexts. Moreover, the study focused specifically on anxiety, depression, and distress, and did not encompass other psychological outcomes such as somatization or substance use, which may also be affected by self-handicapping behaviors.
Despite these limitations, the findings offer important implications for practice and future research. Educators and mental health professionals are encouraged to develop interventions aimed at reducing self-handicapping behaviors, such as programs that enhance self-esteem, stress management, and adaptive coping skills. Given the observed gender differences, with females showing higher vulnerability to depressive symptoms, interventions should consider gender-specific strategies. Promoting authenticity through self-reflection, emotional intelligence, and personal growth initiatives can serve as a protective factor, reducing the negative impact of self-handicapping on mental health. Future research could adopt longitudinal designs to establish causal pathways and examine the long-term effects of self-handicapping, as well as explore cultural variations to determine whether these findings generalize to different populations. By integrating these strategies, educational institutions can support students in achieving both academic success and psychological well-being, fostering a more resilient and mentally healthy student community.
Footnotes
Ethical Considerations
This study was approved by the Institutional Ethics Committee for Research [RefSU/PSY/990-S] Department of Psychology, University of Sargodha. Pakistan on the 2nd November 2024.
Consent to Participate
Participants were informed about the purpose and scope of the study and were assured that their participation was entirely voluntary and that their responses would remain confidential. Informed consent was obtained in writing prior to participation. Each participant received a survey packet containing three instruments along with an information sheet detailing the study procedures and their rights as participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.