
Abstract
The aim of the present study was to examine the factor structure of a Norwegian version of the Highly Sensitive Person Scale (HSPS) and to investigate how sensory processing sensitivity (SPS) is related to personality traits of neuroticism, extraversion, and openness and to subjective health complaints (SHC) in a sample of 167 undergraduate psychology students. The results showed that the variance in a shortened version of the HSPS was best described by three separate factors: ease of excitation (EOE), aesthetic sensitivity (AES), and low sensory threshold (LST). Furthermore, the result showed than an overall SPS factor (EOE, LST, and AES combined) was predicted positively by neuroticism and openness and negatively by extraversion. With respect to SHC, the results showed that EOE and LST were positively associated with psychological health complaints. However, the personality trait of neuroticism contributed more than the SPS factors as predictor of SHC. In conclusion, the present study supported a shortened version of the HSPS and its relation to personality factors and SHC.
Keywords
Introduction
Sensory processing sensitivity (SPS) is a personality trait that refers to the tendency to process stimuli and information more strongly and deeply than others (Aron & Aron, 1997; Aron, Aron, & Jagiellowicz, 2012). This includes sensory processing of aesthetic experiences, other people’s mood and feelings, loud noises, caffeine, and pain. Whereas SPS has often been considered as interchangeably with more established personality factors, such as neuroticism and introversion, Aron and Aron (1997) maintained that it is partially separable and distinct from these personality traits or combinations of them. However, previous research has also shown that SPS is a risk factor for anxiety and depression (Booth, Standage, & Fox, 2015; Liss, Timmel, Baxley, & Killingsworth, 2005) and more frequent symptoms of ill health (Benham, 2006) and agoraphobic avoidance (Hofman & Bitran, 2007), and health problems are also related to personality factors, in particular to neuroticism (Charles, Gatz, Kato, & Pedersen, 2008).
Hence, exploring the relationship between SPS, personality, and common health complaints is of importance for understanding the SPS construct, in particular by controlling for personality factors when investigating the relation between SPS and health. The aim of the current study is to investigate the factor structure of a Norwegian version of an inventory measuring SPS, thus further validating this construct, and to investigate the relationship between SPS, personality, and subjective health complaints (SHC).
Sensory Processing Sensitivity
Approximately one fifth of the population is hypothesized to be highly sensitive to various types of information and stimuli (Aron, 1996a). Highly sensitive individuals tend to notice more subtle stimuli in their environment and are more easily aroused by this, in addition they also respond to lower threshold of stimuli. These individual differences are hypothesized to have a genetic basis and to be present at birth (Aron et al., 2012).
The Highly Sensitive Person Scale (HSPS) was developed and validated in a series of studies seeking to explore the personality construct of SPS (Aron & Aron, 1997). The scale contains 27 items intending to measure various aspects of SPS. This inventory was originally considered to reflect a one-dimensional SPS construct (Aron & Aron, 1997). However, Smolewska, McCabe, and Woody (2006) found that the HSPS was accounted for by three separate factors, labeled as aesthetic sensitivity (AES: the awareness of aesthetics in ones surroundings), low sensory threshold (LST: unpleasant sensory arousal), and ease of excitation (EOE: the feeling of being overwhelmed by both external and internal demands). Smolewska et al. (2006) remarked that “the positive intercorrelations among these factors (…) are consistent with a general, higher-order construct of SPS” (p. 1276), and their own findings suggested a modest intercorrelation between the factors with EOE correlating .32 with both AES and LST, and the latter two correlating .23. In fact, Evans and Rothbart (2008) suggested a two-factor solution, in which EOE and LST items were collapsed into one single factor and LST as a separate factor. But they remarked that their “reason for preferring the two-factor solution is primarily conceptual, rather than statistical” (p. 115), and that both a two-factor and a three-factor solution produced better model fit than a one-factor solution.
Whereas it has been claimed that the results of factor analyses of the HSPS have been inconclusive (Aron et al., 2012), the three-factor structure suggested by Smolewska et al. (2006) has been supported in subsequent research (Aron & Aron, 2010; Booth et al., 2015). However, previous research has also shown weak factor loadings for some of the items (Smolewska et al., 2006), and a shorter version of the scale (12 items) has been proposed, but it does not appear to have been validated (Aron & Aron, 2013).
Personality
Previous research has shown correlations between SPS and personality factors, in particular introversion, neuroticism, and openness. Correlations between introversion and SPS have proven to be small to moderate in six quantitative studies by Aron and Aron (1997). However, although the personality trait of introversion bears much resemblance to SPS, qualitative research by Aron and Aron (1997) shows that not all highly sensitive display the profile of being socially introverted.
The different components of the HSPS relate differently to the personality construct of neuroticism, extraversion, and openness, however. Research by Smolewska et al. (2006) showed that LST and especially EOE were significantly associated with neuroticism. Furthermore, there was a moderate association between AES and openness. The only significant correlation with extraversion was a weak negative association with LST. Also, Sobocko and Zelenski (2015) found that an overall HSPS factor correlated positively with extraversion and neuroticism, the EOE factor correlated positively with openness and neuroticism, whereas the LST factor correlated positively only with neuroticism, and the AES factor correlated positively only with openness.
The reason why many highly sensitive individuals act in an introverted manner might be that social interactions generally are a major source of stimulation (Aron & Aron, 1997). Consequently, social withdrawal would be a natural strategy for reducing stimulation for highly sensitive people. Thus, highly sensitive individuals seeking to reduce an uncomfortable level of stimulation are considered introverts by others.
Furthermore, SPS and neuroticism seem to have much in common. A possible reason is that both highly sensitive and fearful individuals tend to respond to stimuli in a cautious manner (Smolewska et al., 2006). As highly sensitive individuals are more aware of their surroundings, and are more easily aroused, it would only seem natural to respond to stimuli in a cautious manner but without this implying that highly sensitive individuals are necessarily fearful and neurotic (Aron & Aron, 1997).
Taken together, there is ample evidence for relations between more established measures of personality and SPS. But subscales of SPS may be differentially related to different personality factors.
Health Complaints
Individual differences in neuroticism may explain why some people are more prone to experience health complaints and psychological distress. Neuroticism is described as individual differences in the tendency to experience distress and negative emotions (Costa & McRae, 1987). Accordingly, Muris, Roelofs, Rassin, Franken, and Mayer (2005) found a positive correlation between rumination, worry, and neuroticism, and previous research has also shown a positive association between somatic morbidity and neuroticism (Neeleman, Bijl, & Ormel, 2004).
Neuroticism is often correlated with physical symptoms and disease presence (Charles et al., 2008), and previous research has shown relations between negative emotionality and physical distress (Hampson, 2012). Although most of this research has focused on objectively measurable diseases, such as coronary heart disease and ulcer, there are also indications of relation between neuroticism and subjective somatic health complaints. For example, Bru, Mykletun, and Svebak (1993) found significant relations between neuroticism and neck, shoulder, and lower back pain.
SPS also seems to be associated with health complaints. According to Liss, Mailloux, and Erchull (2008), the SPS factors of EOE and LST were related to anxiety and depression, and symptoms of autism and alexithymia, which is the subclinical inability to identify and describe emotions in the self (Sifneos, 1973). However, this study showed a different pattern of relationships for AES, which was positively related to anxiety but not to depression. AES was also related to attention to detail, which may be a symptom of autism. On the other hand, individuals scoring high on AES were less likely to show other symptoms of autism such as communication deficits. Furthermore, AES was negatively related to externally oriented thinking.
A study by Evers, Rasche, and Schabracq (2008) on SPS and work stress showed that the components of EOE and LST were positively related to measures of work stress, work displeasure, and need for recovery. In addition, EOE and LST were also positively associated with negative affectivity. However, AES was not related to any measures of work stress, but this factor was positively correlated with self-efficacy, and sense of coherence in terms of a feeling of meaningfulness. Benham (2006) showed that high SPS, as assessed by the HSPS, was associated with greater perceived stress and more frequent symptoms of ill health, and that SPS was a more powerful predictor of health than was self-perceived stress. A possible explanation was that heightened sensitivity increases general physiological arousal, leading to a chronic stress to the body with subsequent health consequences (Benham, 2006). Another explanation is that highly sensitive people are more aware of somatic symptoms that others may not notice. Accordingly, persons scoring high on SPS are more affected by pain (Aron, 1996b), medications, caffeine, and to have a higher rate of somatic problems like migraine, headaches, chronic pain, and chronic fatigue (Jawer, 2005; Jonsson, Grim, & Kjellgren, 2014). However, the findings of Liss et al. (2008) and Evers et al. (2008) indicate that EOE and LST are more related to poor psychological health and distress, compared with AES, which seems to measure the more positive aspects of being a highly sensitive person.
Several of the aforementioned health problems related to SPS and neuroticism may be characterized as SHC. Investigating the relationship between SPS and SHC is important as SPS may explain why some people are more inclined to experience health-related issues. In a clinical setting, understanding how individual differences in sensitivity affect mental health may provide an additional tool for therapists in understanding their clients. However, because personality factors, particularly neuroticism, also account for health complaints, it is also important to control for the effects of these more established measures of personality.
Problems and Hypotheses
The objectives of the present study are to investigate the factor structure of the HSPS and to investigate the relation between SPS, personality, and SHC. Because SPS has been linked with several of the personality factors within the big-five model, it would seem appropriate to investigate the relative importance of these established personality factors as predictors of SPS factors. Finally, it is an aim to investigate the relative contribution of SPS and personality as predictors of SHC. Hypothesis 1: The HSPS will be accounted for by a three-factor structure. Hypothesis 2: The SPS factors of LST and EOE will be positively related to neuroticism. AES will be positively related to openness. Hypothesis 3: The SPS factors of EOE and LST will be positively related to subjective health complaints. Hypothesis 4: There will be a positive relation between neuroticism and subjective health complaints.
Method
Participants
A total of 167 undergraduate psychology students participated in this study (28 male and 139 female, M age = 21.2 years). A survey was administered to students attending a lecture. Participation was voluntarily, and 82.6% of the attendants responded. The survey was completed by the students before the lecture started and in the break between lectures.
Measures
Highly Sensitive Person Scale
To assess SPS, a translated version of the HSPS was utilized (Aron & Aron 1997). This inventory was translated by means of a standard translation—back translation procedure. The items in this scale reflect various aspects of sensitivity, both in terms of external and internal stimuli, such as sensitivity to arts, life changes, other people’s mood, pain, and loud noises. The students were instructed to state their relative agreement to items describing various aspects of thoughts feelings, and behavior that a person may have. This scale consists of 27 items, each rated from 1 (Strongly disagree) to 7 (Strongly agree).
NEO-FFI
Personality was assessed by means of the NEO-FFI (five factor inventory), which is a shorter 60-item version of the NEO PI-R (personality inventory-revised) and is designed to measure neuroticism, extraversion, openness, agreeableness, and conscientiousness (Costa & McRae, 1992). In this survey, the items assessing agreeableness and conscientiousness were removed because previous research has shown that these items are not associated with the components of HSPS (Smolewska et al., 2006). Hence, 36 items from NEO-FFI measuring the factors of neuroticism, extroversion, and openness were utilized in the present survey, with extroversion representing the opposite of introversion, as described in the Introduction section. The students were instructed to indicate their relative agreement to items describing various aspects of thoughts feelings and behavior reflecting individual differences in personality on a scale ranging from 1 (Strongly disagree) to 5 (Strongly agree). A factor analysis reproduced the expected three factors of neuroticism, extroversion, and openness.
Subjective health complaints
To measure SHC, items from the Health Behaviour in School-aged Children symptom checklist (Currie, 1998) were utilized, including headache, abdominal pain, backache, depressed mood, irritable, nervousness, sleeping difficulties, fatigue, neck pain, and being afraid. The students were instructed to report how often they had experienced these problems during the course of the past 6 months on a 5-point scale with responses 1 (About every day), 2 (More than once a week), 3 (About every week), 4 (About every month), and 5 (Seldom or never). A factor analysis showed a two-factor solution for these items reflecting psychological and somatic health complaints, respectively. Due to weak factor loadings, the items “abdominal pain,” “sleeping difficulties,” and “dizziness” were subsequently removed. Eight items were then subjected to a principal components analysis (varimax rotation) which showed that the factors of psychological and somatic health complaints accounted for 57.17% of the variance. The remaining items for somatic health complaints were “headache,” “backache,” and “pain in neck and shoulder,” and the items for psychological health complaints were “feeling low,” “irritability,” “nervousness,” “tired and exhausted,” and “scared.”
Results
Factor Structure of the HSPS
Principal Component Analysis of SPS-Items With Varimax Rotation.
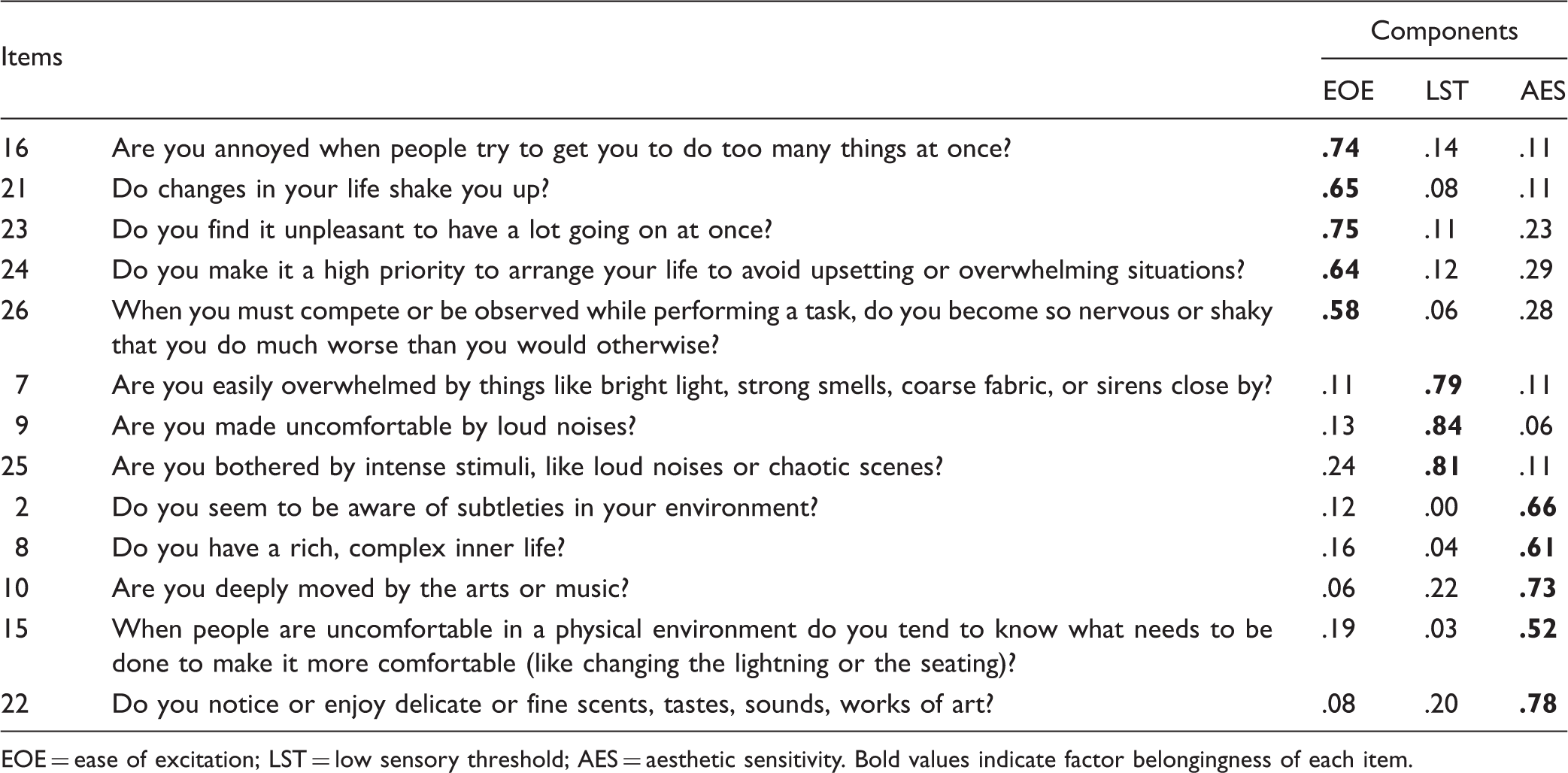
EOE = ease of excitation; LST = low sensory threshold; AES = aesthetic sensitivity. Bold values indicate factor belongingness of each item.
The items in the short version of the HSPS (Aron & Aron, 2013) which were not included in this version are Item 14 (“Do you get rattled when you have a lot to do in a short amount of time?”) and Item 18 (“Do you make a point to avoid violent movies and TV shows?”). In the final analysis, “ease of excitation” (EOE) consisted of five items (Items 16, 21, 23, 24, and 26), “low sensory threshold” (LST) consisted of three items (Items 7, 9, and 25), and “aesthetic sensitivity” (AES) consisted of five items (Items 2, 8, 10, 15, and 22). Eigenvalues for Factor 1 (EOE) was 3.67 (28.24% of total variance), Factor 2 (AES) 2.14 (16.48% of total variance), and Factor 3 was 1.37 (10.53% of total variance). Main factor loadings were satisfactory, and cross loading values were low.
Correlations and Descriptive Statistics
Descriptive Statistics for SPS-Factors, NEO-Factors, Somatic Health Complaints, and Psychological Health Complaints.

SPStot. = total score of sensory processing sensitivity; EOE = ease of excitation; AES = aesthetic sensitivity; LST = low sensory threshold; SHCsom = SHC somatic; SHCpsyc = SHC psychological. N = 167.
Correlations of SPStotal, EOE, AES, LST, Neuroticism, Extraversion, Openness, Somatic Health Complaints, and Psychological Health Complaints.

SPStot. = total score of sensory processing sensitivity; EOE = ease of excitation; AES = aesthetic sensitivity; LST = low sensory threshold; SHCsom = SHC somatic; SHCpsyc = SHC psychological; N = Neuroticism; E = Extraversion; O = Openness. N = 167.
p < .05. **p < .01.
This overall SPS factor was positively correlated with psychological health complaints, neuroticism, and openness and negatively correlated with extroversion. Regarding the subscales of SPS, EOE had a moderate correlation with psychological health complaints, and that LST had a low but significant correlation with psychological health complaints. There were no significant correlations between AES and SHC, however. None of the SPS variables were correlated to somatic health complaints.
As for the association between the SPS factors and the NEO factors, neuroticism was positively correlated with both EOE and LST. In addition, extraversion was negatively related to EOE and LST. Openness was the only personality variable with a significant correlation with AES. With regard to the correlation between NEO factors and SHC, extraversion was negatively correlated with psychological health complaints, and neuroticism was positively correlated with both psychological and somatic health complaints. There was no significant correlation between openness and SHC.
Regressions
Regression Analyses of NEO Factors as Predictors of SPS Factors.

Note. SPStot. = total score of sensory processing sensitivity; EOE = ease of excitation; AES = aesthetic sensitivity; LST = low sensory threshold; N = Neuroticism; E = Extraversion; O = Openness. EOE, AES, and LST as dependent variables. NEO as independent variables. N = 167.
p < .05. **p < .01.
Hierarchical Regression Analysis of SPS and NEO as Predictors of SHC.

EOE = ease of excitation; AES = aesthetic sensitivity; LST = low sensory threshold; SHC: subjective health complaints; SPS: sensory processing sensitivity; N = Neuroticism; E = Extraversion; O = Openness. N = 167.
*p < .01.
NEO-FFI factors were added in the first step and the SPS factors in the second step. The result showed that NEO-FFI scores explained 37% of the variance in psychological health complaints, with a significant contribution from neuroticism. However, adding the SPS factors did not increase prediction of SHC, and neither of the SPS factors remained as predictors of psychological health complaints. In sum, the results suggest that neuroticism is a stronger predictor of psychological health complaints compared with the factors of SPS.
Discussion
The purpose of this study was to examine the factor structure of a Norwegian version of the HSPS, thus further validating the SPS construct, and to investigate the relations between sensory SPS, personality, and SHC.
Analysis of the factor structure of the full 27-item version of the HSPS showed that several of the items had weak and inconsistent factor loadings, and it was difficult to reproduce a three-factor structure. Similar weak factor loadings were observed by Smolewska et al. (2006), for Items 2 (“Do you seem to be aware of the subtleties in your environment”), 3 (“Do other people’s mood affect you”), and 4 (“Do you tend to be more sensitive to pain”) in the original scale. However, while Item 8 (“Do you have a rich, complex inner life?”) had a satisfactory factor loading (.61) in the present study, this item showed a factor loading of .25 in research by Aron and Aron (1997). The final shortened version in the present study produced the expected three-factor solution proposed by previous research (Aron & Aron, 2010; Booth et al., 2015; Smolewska et al., 2006), thus providing support for the first hypothesis.
Similar to our findings, Booth et al. (2015) also supported a reduction from the original 27-item scale to 21 items. However, the present study indicates that that the HSPS works best as a short version, similarly to the short 12-item version of this scale proposed by Aron and Aron (2013). In fact, 10 of these 12 items were retained in the present study. Whereas Aron and Aron (2013) discuss the applicability of the three-factor solution for HSPS, it is not clear whether they considered this factor structure to be applicable to their own suggestion of a short 12-item version, and there appears to be no subsequent validation study of this short version of the scale. However, whereas the present findings support a three-factor structure for SPS, a higher order total SPS factor may also be sustained, as the subscales were correlated, and theoretical assumptions may also justify a one-factor solution for SPS (Aron & Aron, 1997).
As regards the relation between personality and SPS, the correlation analysis showed that both EOE and LST were significantly correlated with neuroticism, and that AES was positively correlated with openness, in accordance with Hypothesis 2. As for the association between EOE and neuroticism, this is quite sensible, as neuroticism is related with proneness to worrying, high strung, and tense behavior (Friedman & Schustack, 1999). In addition, EOE and LST were negatively correlated with extroversion, but the correlations were small (LST) to moderate (EOE) in accordance with previous research on the relation between introversion (i.e., extroversion reversed) and SPS (Aron & Aron, 1997; Smolweska et al, 2006; Sobocko & Zelenski, 2015).
The total SPS score was significantly related to all of the personality factors in both the correlation and the regression analysis. Hence, SPS may, to a certain extent, be accounted for by a mixture of neuroticism, extraversion, and openness. This is in accordance with the conclusion that SPS is related to aspects captured by previous measures of personality (Aron et al., 2012).
SHC were positively correlated with EOE and LST, but AES was not. Hence, Hypothesis 3 was supported. However, EOE was only related to psychological but not somatic health complaints. This finding also supports the necessity of keeping AES as a separate factor (Evans & Rothbart, 2008) because it is differentially related to SHC than EPE and LST. Neuroticism was also the only significant predictor of somatic health complaints, in addition to being a predictor of psychological health complaints. Hence, there was support for Hypothesis 4.
The association between SPS and psychological health complaints seems to suggest some potential for clinical application of the HSPS, although the scale was not originally developed for this purpose (Aron & Aron, 1997). However, the relation between SPS and psychological health complaints disappeared when controlling for the effect of neuroticism, probably due to substantial statistical overlap between SPS and neuroticism. This effect of neuroticism has also been observed in an experimental study, in which individuals scoring high on SPS did not report being more distracted by either moderate or high intensity audio stimulation when controlling for the effect of neuroticism (Gearhart, 2014).
Although SPS and neuroticism may have similarities, neuroticism seems to be better when it comes to understanding of psychological health complaints. Nevertheless, Aron (1996a) claims that highly sensitive individuals may benefit greatly from counseling about issues such as the normalcy of their reaction to stimuli as well as their need to consider their sensitivity in relation to work, health, and relationship. Thus, applying the HSPS in a clinical setting may provide both the therapist and the client with an additional tool in terms of understanding and adapting to the challenges of being highly sensitive.
As there was no significant relation between AES and SHC or between AES and neuroticism, it is reasonable to assume that AES comprises the more positive aspects of SPS. Thus, being for example aware of subtleties in the environment is not associated with health complaints. As the present results support, it would appear likely to assume that the AES factor share qualities with the openness factor of personality, including openness to aesthetic experiences such as music and art. For example, individuals with a high score on openness are often imaginative, witty and have a strong aesthetic sense (Friedman & Schustack, 1999).
Aron (1996a) discusses the many advantages of being a highly sensitive person. For instance, highly sensitive individuals are described as being more empathetic, imaginative, and creative. From the present analyses, it would seem that positive aspects of being highly sensitive are more associated with AES than to the components of EOE and LST. This is in accordance with previous research, which has shown that AES has a markedly different pattern of relationships with health issues compared with the factors of EOE and LST. For example, AES does not appear to be related to depression (Liss et al., 2008) or to any measures of work stress, and AES is, in fact, positively related to self-efficacy (Evers et al., 2008).
Conversely, LST and particularly EOE appear to represent the more negative aspects of SPS, as both are related to neuroticism, and EOE is in addition related to psychological health complaints. This is consistent with previous research, which has shown that both EOE and LST are related to anxiety and depression (Liss et al., 2008), and that EOE and LST are positively related to several measures on work stress (Evers et al., 2008). The EOE factor comprises descriptions of being overwhelmed by both internal and external stimuli, as well as to disruptions in concentration, and the LST factor describes a physiological predisposition to process stimuli at lower thresholds of stimulation. These aspects of SPS seem to be associated with various psychological health complaints in highly sensitive individuals. Hence, they may predispose an individual to be more attentive toward possible threats in the environment and to be more physiologically reactive (Liss et al., 2005). Consequently, highly sensitive individuals may seek solitude and stimuli reduction in order to prevent psychological distress caused by being exposed to overwhelming stimulus. However, social withdrawal and solitude may be less culturally accepted and more difficult to seek in a Western society which embraces virtues of being outgoing and gregarious (Cain, 2013), thus further strengthening the feeling of being overwhelmed by stimuli.
In explaining why some highly sensitive individuals are more prone to psychological health complaints, exploring early childhood experiences is also of importance. Research by Aron, Aron, and Davies (2005) showed that those scoring high on the HSPS in addition to reporting a troubled childhood scored particularly high on measures of negative affect. Accordingly, experimental studies with nonhuman primates (Suomi, 1997) have shown that reactive (“high sensitive”) infants raised by average mothers had the poorer outcomes compared with reactive infants raised by highly skilled mothers, while those with low reactivity (“low sensitive”) showed little effect from being raised by either average or highly skilled mothers. On the other hand, highly reactive infants raised by highly skilled mothers had the best outcomes in terms of high status within the social hierarchy of the group and more behavioral resilience to stress.
Hence, it would seem that highly sensitive children are more responsive to both negative and positive events and are also more dependent on the quality of care they receive compared with their less sensitive peers. Highly sensitive persons may not necessarily be predisposed to negative affect but still more sensitive to the quality of environmental support. The assumption that some individuals are more susceptible than others to both negative (risk-promoting) and positive (development-enhancing) environmental conditions has been discussed thoroughly by Ellis, Boyce, Belsky, Bakermans-Kranenburg, and Van IJzendoorn (2011).
However, as supported by previous research, the present findings show that a highly sensitive personality may be expressed along several dimensions. With respect to health issues, a higher score on AES is not necessarily detrimental to health, whereas a high score on EOE, as well as LST, may be more relevant. However, the present results suggest that these latter factors are more critical for psychological than for somatic health complaints.
Limitations and Conclusions
As the present study investigated correlations between SPS, personality, and SHC, no conclusions about causality between these constructs can be drawn. In addition, the present study did not use any behavioral, perceptual, or physiological measures to investigate the relationship between these constructs.
Furthermore, this study was conducted using a relatively homogenous sample in terms of undergraduate psychology students with a limited range of age and a majority of female students. It is uncertain whether the present findings might have been observed in a more diverse group. Future research should therefore examine a more heterogeneous group in order to support generalizability.
Despite of these limitations, this study has shown that SPS consists of three different components, similarly to previous research on the factor structure of the HSPS (Aron & Aron, 1997; Smolewska et al., 2006). However, some items in the 27-item version showed weak and inconsistent factor loadings, whereas the expected factor structure was reproduced when reducing the number of items. A test of the construct validity of the present Norwegian version of this inventory is valuable, also because it tested the HSPS in an alternative cultural context. However, this is also a limitation, and further studies of short versions of the inventory should be tested on alternative samples.
In addition, these components of SPS are differently associated with personality and SHC. These findings further strengthen the view of SPS as a multidimensional construct that is partially separable from similar personality constructs. Whereas a relationship between EOE or LST and SHC has been supported, this relationship disappeared when controlling for the effect of neuroticism, thus showing that neuroticism is a more important predictor of psychological health complaints. This is also in line with recent SPS research (e.g., Gearhart, 2014), in which it has now been common for researchers to control for neuroticism.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.