
Abstract
Adult-onset asthma, notably prevalent among healthcare professionals, especially nurses, is often attributed to occupational factors such as exposure to cleaning agents. Studies consistently underscore the substantial role of such exposure in work-related asthma among hospital staff. We aimed to (a) identify and characterize current practices in cleaning and aerosolized medication administration; (b) assess changes in practices since a similar 2003 study of Texas healthcare workers; and (c) identify factors contributing to diverse exposures within healthcare job categories. We conducted focus groups with 38 participants in 6 healthcare settings, analyzing current practices, changes since 2003, and factors contributing to exposure diversity. We used a three-step approach for data analysis, including sociodemographic characterization, a scissor-and-sort technique for exposure description, and qualitative content analysis. Participants were primarily healthcare providers (76%) and housekeepers/cleaners (11%) who reported exposure to aerosolized medications, cleaning products, adhesives, and solvents. Participants reported transitioning from cleaning practices to new formulas with reduced odors and shifting from spray cleansers to wipes. Personal protective equipment (PPE) used during cleaning tasks varied, with training differing among job categories. Aerosolized medication administration varied among facilities, with reported medication types and protocol changes over time. The results emphasized the significance of maintaining uniform protection, disseminating knowledge, and consistently adhering to PPE protocols in the healthcare environment. Addressing the identified gaps in comprehension and potential sources of exposure variability requires additional focus on occupational health and safety initiatives.
Keywords
Background
Work-related asthma (WRA) is the most frequently reported occupational respiratory disease in the United States (U.S.; Burge & Hoyle, 2012). The Centers for Disease Control and Prevention (CDC) reports that the overall prevalence of asthma among adults has increased from 6.9% in 2001 to 8.0% in 2021, indicating a slight upward trend in asthma cases over the past two decades (Centers for Disease Control and Prevention, 2024). The condition, which is both serious and costly, includes new cases of asthma due to workplace exposures (i.e., occupational asthma) as well as pre-existing asthma triggered or worsened by exposure to workplace agents (i.e., work-exacerbated asthma; Malo & Vandenplas, 2011). It has a poor prognosis, with up to two-thirds of workers continuing to exhibit symptoms despite cessation of exposure (Burge & Hoyle, 2012). Furthermore, asthmatics are more likely than individuals without asthma to have functional work limitations, lost work time, symptomatic days, and increased medical costs (Burge & Hoyle, 2012; Malo & Vandenplas, 2011; Ojeda & Sanz de Burgoa, 2013). Up to $2.2 billion in annual costs were associated with WRA in the United States in 2002, an estimate that is most likely outdated (Leigh et al., 2002).
Occupational factors are the most commonly identified cause of adult-onset asthma (Burge & Hoyle, 2012) and healthcare workers (HCWs) are an at-risk group for WRA, especially nurses (Delclos et al., 2007; McHugh et al., 2010; Patel et al., 2023). Most studies of hospital workers, including nurses, have found that exposure to cleaning and disinfecting agents is a risk factor for WRA (Arif & Delclos, 2012; Mirabelli et al., 2007). However, changes in healthcare practices over time—including but not restricted to cleaning practices—may have modified the specific risk factors associated with WRA. Increasing or decreasing exposures to potential asthmagens due to shifting healthcare tasks, agents, and work settings have not been well characterized.
The objectives of this focus group study were threefold: (a) to identify and characterize current practices in cleaning and aerosolized medication administration; (b) to assess changes in practices related to WRA risk factors in healthcare settings since conducting a previous study of Texas HCWs in 2003; and (c) to identify factors that could result in varying exposures to these risk factors within job categories of HCWs. In addition, this focus group study was preparatory to a larger statewide study of Texas HCWs and was used to refine the study instruments (Mirabelli et al., 2007).
Methods
Institutional review and approval were provided by the Committee for the Protection of Human Subjects at The University of Texas Health Science Center at Houston and the Institutional Review Boards of Baylor College of Medicine and The University of Texas M.D. Anderson Cancer Center.
Focus group interviews were conducted in six different healthcare settings, among participants employed at the respective facility, with one focus group interview session per facility (n = 6 focus groups). Study participants were recruited from three large Houston, TX-area hospitals (a general tertiary-level hospital, a pediatric hospital, and a cancer center), two nursing homes, and one outpatient clinic. Employees of those facilities were eligible for recruitment if they were 18 years or older and had been actively working as a physician, nurse, occupational therapist, respiratory therapist, safety specialist, administrator, or housekeeper/cleaner for at least 1 year. The leadership of each participating healthcare facility, who had consented to participate in and support the study, employed purposive sampling to identify study participants and recruited them via email and in person.
Each focus group interview session was comprised of four to eight participants. All sessions were conducted in English and attended by two members of the research team (one facilitator and one note-taker), all but one of the sessions were also attended by a researcher who was a native Spanish speaker. This presence helped to build rapport with participants who might have had varying levels of English proficiency, ensuring that language did not become a barrier to participation. As participants arrived, they were provided with information on the general nature of the session, the goals of the research, and measures being taken to protect confidentiality. Following an opportunity to ask questions, written informed consent was obtained from each participant. Respondents were then asked to complete a brief, eight-question sociodemographic survey. The discussions usually lasted 60–90 minutes and explored three primary topic areas: (a) the administration of aerosolized medications; (b) room cleaning practices and products; and (c) equipment cleaning practices and products. Additional information was captured on participants’ use of latex gloves, adhesives, and solvents. Details were collected on whether current practices represented changes to or the continuation of past practices. The research team prepared focus group interview guiding questions in advance, with structured content probe questions centered on each topic as an independent research domain. Additional content probe questions were used, when necessary, to clarify or expand specific points raised during the conversations. At the end of each session, participants were asked to provide further comments on any topic addressed during the session. Focus group interview audio recordings were transcribed verbatim into text and loaded into NVivo (version 11) qualitative analysis software (QSR International, Burlington, MA); demographic data were entered into Stata/SE (version 14.1) statistical software (StataCorp LP, College Station, TX).
A three-step approach was used to analyze the data. First, the study sample was described by its sociodemographic and occupational characteristics according to participant job category (e.g., healthcare provider, housekeeper/cleaner, facility administrator, and occupational/environmental safety manager) with frequencies and percentages or means and standard deviations. Due to small cell sizes, Fisher’s exact tests and Kruskal-Wallis equality-of-populations rank tests were used to compare the prevalence of categorical covariates and means of continuous covariates, respectively.
Next, a “scissor-and-sort” technique was employed to describe the tasks and products to which workers were exposed, as well as the frequency of current exposure and changes to that frequency over time (Stewart & Shamdasani, 2014). The technique involved (A) physically cutting out relevant passages from the transcribed focus group interview data and sorting them into three primary categories, based on the three major categories that emerged from the content probe questions: (a) aerosolized medication practices (i.e., medication types, administration protocols); (b) cleaning practices (i.e., room cleaning, equipment cleaning); and (c) other exposures (i.e., inclusive of, but not limited to, latex gloves, adhesives, and solvents, and excluding issues related to cleaning or medication administration); (B) within these categories, sub-categories were created to further organize the data by specific tasks and products, allowing for a detailed analysis of exposure frequencies and changes over time.
Finally, a qualitative content analysis was conducted using both deductive and inductive categories to identify the manifest and latent content meaning of the focus group text, respectively (Graneheim & Lundman, 2004). Initially, the content analysis employed
Results
A total of 38 individuals participated in the 6 focus group interview sessions. Most participants were healthcare providers (physicians, nurses, occupational therapists, respiratory therapists) (76%), with housekeepers/cleaners comprising the next most populous group (11%). Participants were predominantly female (82%). Approximately one-third of respondents were white, non-Hispanic (35%), another third were Black, non-Hispanic (32%), and more than 20% were white, Hispanic (22%). Less than half of the participants (45.9%) had a bachelor’s degree. On average, respondents reported working in healthcare for 18.0 years (SD: 11.3 years), with facility administrators reporting the longest tenure (M: 25.0 years; SD: 0.0 years) and housekeepers/cleaners reporting the shortest tenure (M: 12.5 years; SD: 7.9 years). However, no statistically significant differences were detected between job categories by sex, age, education level, race/ethnicity, workplace, or years in healthcare, which may be partially attributable to the small sample size analyzed (Table 1).
Demographic and Occupational Characteristics of Focus Group Participants by Job Category
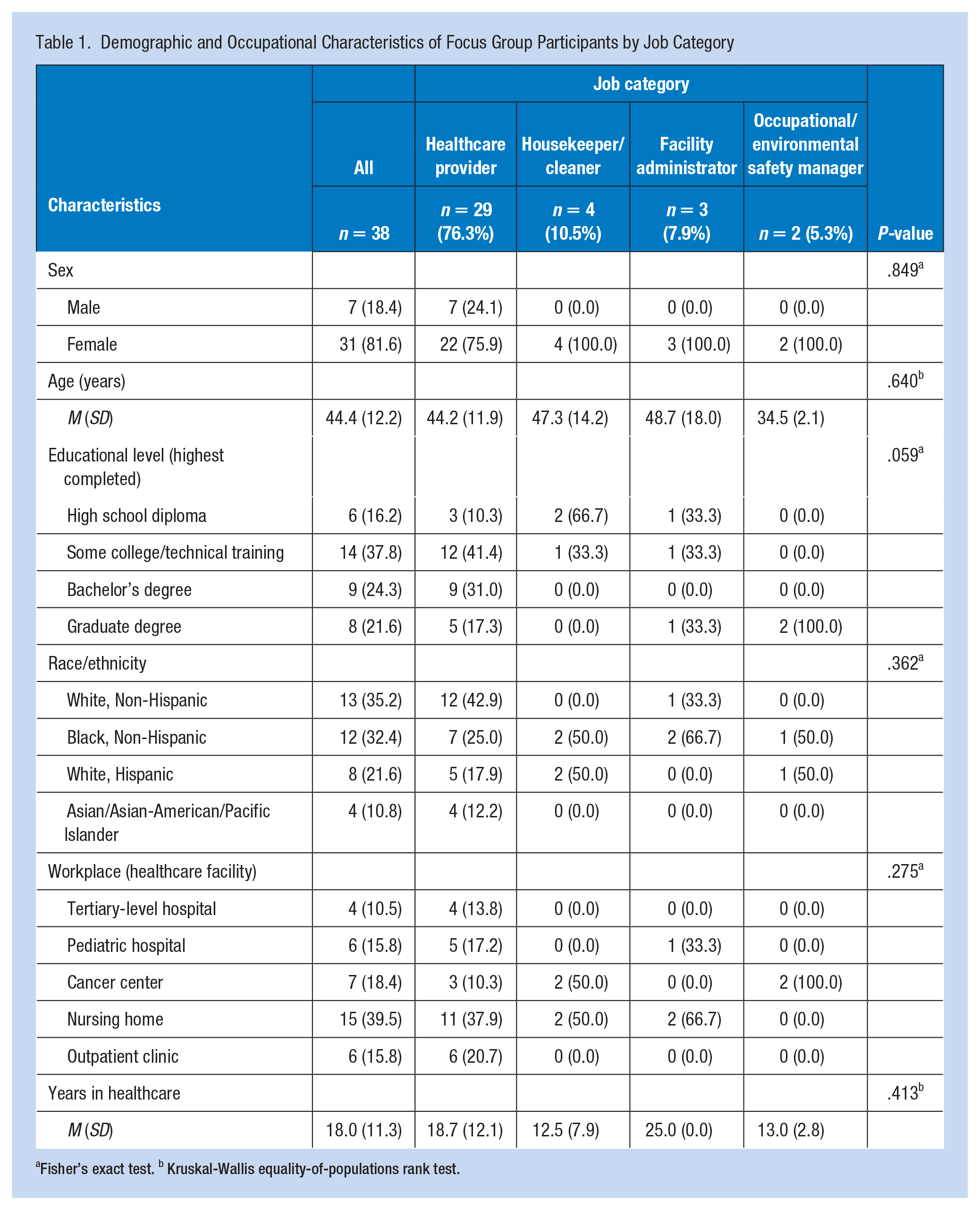
Fisher’s exact test. b Kruskal-Wallis equality-of-populations rank test.
Participants reported exposure to five broad categories of aerosolized medications (e.g., antibiotics, bronchodilators) and 10 general categories of cleaning products (e.g., glass cleaner, cleaning wipes). In addition, 12 broad categories of exposure to adhesives, solvents, or other products and procedures were identified (e.g., air fresheners, paint, spray adhesives). Respondents at three of the six facilities indicated they had access to latex gloves (with and without powder). When asked to specify medications or products that respondents or their co-workers found irritating (i.e., throat, eyes, skin) or offensively odored, they named 15 aerosolized medications, 5 cleaning products, and 5 adhesives/solvents.
Cleaning Products and Practices
Participants from each of the healthcare facilities reported transitioning to cleansers with new cleaning formulas from 7 years earlier to as recently as 2 years before the focus group interview session. The new formulas were unanimously described as an improvement in terms of having a lower odor. They often were considered superior to the previous products in other ways: What I’ve noticed for the new one that we have [is that] the smell is less compared to the previous one, and it dries faster also. So, I think they’re just trying to remove the old one and give us the better one (Nurse, nine years in healthcare).
Other participants were less certain about the reasons for switching formulas: “I don’t know exactly—if it’s because it’s cheaper, or because it’s better or more effective” (Nurse’s assistant, four years in healthcare).
With the introduction of these new formulas, participants reported less variation among cleaning agents than in previous years. This was due, in part, to having fewer cleaning agents made available by the organization. Whereas the majority of respondents indicated they were provided with a single cleaning agent per cleaning task, a few stated they could select among more than one option: “So we have choices. We can use [a liquid cleaner] or the wipes<!--index: wipes–>. There’s like three choices” (Physical therapy technician, 28 years in healthcare). It was noted that access to the cleaning agents varied within organizations, with some units having greater flexibility in requesting alternative cleansers than other units. In addition, all participants reported that they were not allowed to deviate from the cleansers provided by their organizations, such as by supplying their own products, nor were they able to request that additional cleansers be stocked by their employers: “In the past, some of the housekeepers would bring their own products from home that they liked better, and now that’s not allowed” (Facility administrator, 50 years in healthcare).
Participants employed by two of the six organizations reported changing cleaning agent formulas when they migrated to centralized distribution and dilution systems for their cleaning products. These systems were housed at one or more locations within a facility and dispensed pre-mixed chemicals to healthcare or housekeeping workers. Participants using these systems reported that the individual cleaning products were either color- or number-coded; one of the two systems also provided the cleanser’s brand name. Respondents indicated that chemical safety data sheets were available at specific locations in the facility, such as nursing stations or where the cleansers were stored. The two facilities reporting centrally dispensed and pre-diluted cleansing agents characterized them as “green” and “non-toxic.” However, that did not preclude the products from being respiratory or skin irritants: “It’s a non-toxic product, but it’s irritating to some folks” (Facility administrator, 20 years in healthcare). One of the facilities’ participants indicated that the shift to the new cleanser system had resulted from employee complaints about the previous cleaning agents: But some people maybe have different reactions, or they may not have any. It was maybe three years ago we were using something else. An employee was complaining about something [that] got on her skin by her using it. That’s why we got the “Go Green” [products] (Building attendant, 25 years in healthcare).
Responses from participants using centrally dispensed/diluted cleaning systems suggested that they typically did not know what specific products they were using, with participants identifying products solely by number, such as “something called 67” and “5 is [to] disinfect, 24 is for cleaning.” In addition, it was reported that some organizations’ centralized systems used the same color or number for different cleansers in different areas of the facility: “[In the nursing unit], Windex is the blue one. Disinfectant is the orange, and the floor cleaner is brownish colored. [In our department], we have a different kind for grease. It’s a blue one” (Housekeeper, 3 years in healthcare).
Some participants employed by in-patient facilities differentiated between cleaning agents that could be used around patients versus those that could not.
However, it was acknowledged that patients may still be exposed to strongly scented cleansers: I would say for us in ICU, once they clean the room, it’s really a strong smell. I don’t stay in there. I crank down the temperature really low to get rid of the smell before I get the new patient in (Nurse, 9 years in healthcare).
It could be unclear whether the odors irritated the patients. Although none of the participants reported patient complaints or physical symptoms of irritation, it was acknowledged that the most vulnerable patients might not exhibit such symptoms, such as “if they’re knocked out [and] intubated” healthcare providers “can’t really tell” if an odor was bothersome to the patient.
Participants reported a decrease in the use of spray cleansers over time, which had been replaced, in general, with hand-held paper or cloth towelettes, or “wipes.” The decline in spraying cleaning agents onto surfaces was reportedly to eliminate the risk of slips or falls among patients or staff: “The biggest reason not to do sprays is that it gets onto the floor and makes the floor slippery . . . [I]f you put all that spray down, then the staff or a resident or nurse could fall” (Nurse, 17 years in healthcare). All participant groups indicated that their most common cleaning chemical applicator was via wipes, characterized as “the standard pretty much throughout” the organizations for cleaning and disinfecting. All healthcare providers and cleaners in our study reported job-related use of cleaning wipes several times per day, with less frequent use by the participating occupational and environmental safety managers: “It started eight years ago. I’ve been using wipes ever since constantly” (Nurse’s assistant, 20 years in healthcare). Cleaning staff reported the most frequent use of wipes. Several participants reported the presence of more than one kind of wipe within their organization. Respondents widely acknowledged that they were aware that they should not have skin contact with the wipes; fewer mentioned that they were aware that there should be no contact with the surface that was wiped until it was dry. In addition, new forms of cleaning, such as ultrasonic cleaners for instrument cleaning, were noted as reducing participants’ exposure to certain cleaning products and protocols.
Participants reported widespread use of personal protective equipment (PPE) when cleaning, with gloves identified as the most frequently donned PPE for cleaning. Although using gloves was common, it varied depending on the cleaning task. When individuals were disinfecting surfaces with wipes, glove use was inconsistent: “Most of the time, we do [wear gloves]—just when you’re thinking . . .‘Hurry up and disinfect,’ we might not” (Nurse, 20 years in healthcare). Hand washing was widely believed to counteract any adverse effects of skin contact with the cleansing products: “I don’t use gloves all the time. I just wash my hands” (Nurse, 40 years in healthcare). Participants noted that if they were cleaning up a visible spill, they wore gloves “all the time.” Other items of PPE identified as worn when cleaning included masks, goggles, and gowns. Participants stated that the use of these forms of protection varied similarly to that of gloves: “I probably should use a mask when I spray that stuff because it is kind of strong, but I don’t. I just get it over with and do it” (Nurse, 21 years in healthcare). Respondents stated that “some people complain it’s hard to breathe with the mask” and “sometimes [PPE] is hot” as reasons that they or their peers would choose not to wear PPE when performing cleaning tasks. It was noted that some of the PPE use reported by participants did not correspond to the issues identified with the cleaning agents, such as only wearing gloves when working with cleaners that irritated skin (e.g., not also wearing a gown) or airways (e.g., no use of a mask). Within organizations, the shift to institution-wide use of gloves when cleaning was often tied back to a specific infectious event, such as an outbreak in the facility.
Training on the specific cleaning products and their applications varied by facility and job title. In general, housekeeping staff members reported the most focused training on cleansers and cleaning practices (up to 5 days). In contrast, nurses reported the longest training period that included some instruction on cleaning (up to 2 weeks) and the most frequent continuing training on cleaning practices (monthly to quarterly). Other HCWs reported training in using cleansers at orientation and on the job, as needed. Although cleaning staff and nurses generally reported receiving some formal instruction when new cleaning products were introduced at their facilities, other participants did not: “One product disappears, and a new one shows up” (Nursing assistant, 14 years in healthcare).
Aerosolized Medications
Respondents at four of the six participating healthcare facilities reported administering aerosolized medications; participants from the outpatient clinic and the tertiary-level hospital stated that they did not provide aerosolized medications as part of patient care. Participants responsible for the administration of aerosolized medications reported lengthy initial training periods (up to 12 weeks of one-on-one training) and routine ongoing training (up to monthly), as well as instruction on an as-needed basis (e.g., for new medications).
Participants reported the greatest variation over time in aerosolized medications due to changes in medications and protocols. In addition, the current administration of aerosolized medications varied greatly among the organizations reporting their use, particularly in the frequency of administration and type of medication. Although aerosolized medications were administered daily at each facility reporting their use, several participants noted the seasonal administration of certain medications (e.g., ribavirin is more likely in the winter months). One facility’s participants indicated that during their peak period, they saw an increase from administering medications “twice a shift” to “up to six times a day on multiple [patients].” Another facility’s participants noted that, during peak periods, not only did the frequency of aerosolized medication administration increase substantially, but the medications being given shifted from those considered less irritating to those considered more irritating (e.g., certain bronchodilators) or with more potential deleterious effects (e.g., irradiated medications). As a result, the administration of medications characterized as “put the ‘Do not go inside’ sign out and don’t come in without [PPE]” increased from “maybe once a week” to “every day” on “ten patients” where “one treatment goes for three hours on, five hours off . . . for the course of seven days or ten days.”
Participants indicated that their organizations provided specific PPE protocols to limit workers’ exposure to aerosolized medication. Still, they also stated that policy adherence and availability of the requisite PPE varied within their organizations. When asked to describe their experiences and practices related to PPE usage, the responding respiratory therapists reported the greatest familiarity with the medications and associated PPE and the greatest adherence to the PPE policies. However, the respiratory therapists mentioned that not all their nursing or housekeeping co-workers knew the guidelines for using specific forms of PPE with particular medications. They also indicated that those who were aware of the policies occasionally violated them: “We have a sign that says, ‘Do not enter.’ But nurses do go in. They have to go in, but sometimes they’re not covered like we are” (Respiratory therapist, 7 years in healthcare). Facility maintenance and cleaning staff participants stated that they occasionally entered treatment rooms without the correct PPE because it was not available: Sometimes the housekeepers have to go in there, and then we have to wear a special mask . . . But sometimes they don’t have the size you need . . . If they don’t have your size, you have to wear what they have” (Housekeeper, 4 years in healthcare).
A few of the nurses participating in the focus group interviews noted that they would try to avoid breathing when working with aerosolized medications that did not require the use of masks: “When the [inhaler] is dispensing, I won’t breathe, but it’s not strong” (Nurse, 20 years in healthcare).
Participants indicated they experienced effects from certain aerosolized medications, even when wearing the prescribed PPE. Healthcare workers named five specific medication categories with which they experienced irritation of the airways or skin or flushing despite PPE use (bronchodilators, antimicrobials, hypertonic saline, mucolytic agents, and racemic epinephrine). All five of these medication categories were reported in use at the children’s hospital, with four reported at the cancer center and one reported at both nursing homes. Additional effects were reported with the administration of an anesthetic gas used in the care of some intubated patients at the children’s hospital.
The respiratory therapists in the focus group interviews reported shifting work assignments to accommodate co-workers’ pregnancies or facial hair. Although respondents from two of the three facilities reporting aerosolized medication administration stated that they sought to reduce or eliminate the exposure of pregnant women to certain medications, they were clear that doing so was “not a hospital policy” but, instead, “just a unit-based nice [thing] to do” and that they did so even though administering the medication was “not contraindicated for a pregnant worker.” They characterized this practice as reflecting that their work groups were “really accommodating—if we can pass [a patient] on to another [respiratory therapist]—that’s how our group is. It’s not a big issue.” This restructuring of work assignments occurred on the floor within small peer groups, where respiratory therapists traded patients among themselves. One respiratory therapist with a beard stated that he did not currently have any patients whose medications required him to wear a fit-tested respirator, as those patients were being cared for by a clean-shaven male colleague. However, he did state that “if I absolutely have to, I’ll go” into a room wearing his respirator, he preferred to “find somebody who has shaved” to send in instead.
Other Agents and Procedures
The use of latex gloves was reported by participants employed by three of the six healthcare facilities: the cancer center, the outpatient clinic, and the tertiary-level hospital. The cancer center participants reported that “in our vending department, they do have some latex gloves, [including] powdered,” but that their use was limited, such as in “one particular pharmacy.” In contrast, participants from the outpatient clinic and the tertiary-level hospital reported widespread use of latex gloves. Those participants reported that both latex and non-latex gloves were available and that they were given a choice as to what to wear. Respondents agreed they “always use” latex gloves, with an exception made “only if the patient is allergic to them.” They stated that a single day’s use of latex gloves would be “too many to count,” as they were used for cleaning, patient care, and medical procedures. Regarding powdered latex gloves, participants at the cancer center and the tertiary-level hospital reported using powder-free latex gloves. However, participants in the outpatient clinic reported that they still had powder-free and powdered latex gloves at their facility.
The daily use of adhesive tapes or liquids was mentioned by participants from the children’s hospital and the nursing homes, and the frequent use of solvent wipes was mentioned by nursing home staff. Participants representing the remaining facilities noted the occasional use of adhesives and solvents.
Additional exposures to strong odors or agents that caused dizziness were facility-specific. Medical procedures that produced strong odors were reported by participants from the outpatient clinic and the cancer center; exposures not directly related to medical procedures, such as fumes from paint, floor stripping, and cosmetology salons, were reported by respondents from the nursing homes.
Discussion
The findings of this focus group study provide crucial insights into the current practices and potential risk factors associated with WRA among HCWs through a comprehensive qualitative analysis conducted in Texas. The study, conducted across six healthcare facilities in the Houston, TX area, included diverse healthcare professionals (i.e., physicians, nurses, occupational therapists, respiratory therapists, safety specialists, administrators, and housekeepers/cleaners). The participants’ sociodemographic and occupational characteristics revealed a mix of job roles, with healthcare providers comprising the majority. The demographic distribution highlighted the high prevalence of females in healthcare occupations.
Exposure to various aerosolized medications, cleaning products, adhesives, solvents, and latex gloves was reported by the participants. Cleaning practices and aerosolized medication administration emerged as key focus areas in the discussions, with participants providing insights into changes in practices since a previous study conducted by our group in 2003. The study aimed to identify and characterize these practices, assess changes over time, and identify factors contributing to varying exposures within job categories.
Over the past two decades, and considering the recent COVID-19 pandemic, there have been significant changes in the nature and frequency of cleaning and disinfection products, with a greater emphasis on automation of practices and increased use of protective equipment (Bush, 2008; Carpenter & Hoppszallern, 2010; Delclos et al., 2007; Dumas et al., 2017; Kurth et al., 2017; Lytras et al., 2018; Oh & Uhm, 2016; Roberts et al., 2022; Tsai et al., 2015). A greater focus on controlling hospital-acquired infections has led to detailed cleaning and disinfection guidelines, with concurrent changes in environmental policies and regulations that may have unintended consequences on HCWs (Kurth et al., 2017; Oh & Uhm, 2016). However, a recent report found no change in the percentage of WRA cases associated with cleaning agents, underscoring the need to increase the knowledge of potential cleaning hazards (Rosenman et al., 2020). The scissor-and-sort technique was employed to categorize tasks and products, revealing three significant categories: aerosolized medication practices, cleaning practices, and other exposures. The qualitative content analysis, using deductive and inductive categories, showed detailed insight into the current state of cleaning and disinfection practices in the healthcare work environment.
Comparison With Existing Literature
The results pointed toward several noteworthy findings in cleaning practices. Participants highlighted a shift to new cleaning formulas in recent years, with improved characteristics such as lower odor and faster drying. The standardization of cleaning agents within organizations was observed, limiting variation among agents. Changes in cleaning agent formulas were noted in facilities adopting centralized distribution and dilution systems, providing pre-mixed chemicals with color or number coding.
Our study identified two primary sources of unaddressed variability in exposure: (a) individuals using cleaning products or administering aerosolized medications as part of their job tasks were generally well protected from the products. Still, individuals exposed to these agents while performing other tasks were only sometimes protected from them—for example, a nurse might be exposed to aerosolized medications while assisting a respiratory therapist, even though administering these medications is not part of their primary job responsibilities; and (b) the practice of healthcare providers trading patients, especially during high season, skewed the levels of exposure substantially toward certain providers and away from others. Further, there was no indication that PPE that did not require a close fit to the face was available, such as a powered air-purifying respirator.
The findings of this study align with earlier research indicating that HCWs are frequently exposed to various aerosolized medications, cleaning products, and other substances known to trigger asthma (Bush, 2008; Delclos et al., 2007; Rosenman et al., 2020). The shift toward new cleaning formulas with improved characteristics, such as lower odor and faster drying, reflects ongoing changes noted in the literature aimed at reducing occupational hazards (Kimberly-ClarkSterling, 2018; Malerich et al., 2008). However, despite these advancements, the persistence of unaddressed variability in exposure, particularly among individuals performing ancillary tasks, resonates with findings by Tsai et al. (2015) and Roberts et al. (2022), who observed similar challenges in consistent PPE use and hazard awareness among HCWs.
Our analysis highlighted that variability in exposure was influenced by a combination of factors, including the specific job roles, the level of training, the availability and use of PPE, and the frequency of engagement with hazardous substances. For example, respiratory therapists (RTs) were generally more knowledgeable and consistent in their use of PPE, reflecting their specialized training and frequent interaction with aerosolized medications. In contrast, other HCWs, such as nurses and housekeepers, displayed more variability in their knowledge and PPE use, which may be linked to differences in training opportunities and job responsibilities. These findings align with previous research that has shown disparities in occupational exposure and safety practices based on job roles and training (Roberts et al., 2022; Tsai et al., 2015).
The continued presence of WRA cases associated with cleaning agents, despite enhanced protective measures and cleaner formulas, underscores the complex nature of WRA and the need for more nuanced interventions (Rosenman et al., 2020). This is consistent with research indicating that while protective equipment and improved products reduce direct risks, they may not fully mitigate secondary exposure risks (Kurth et al., 2017; Oh & Uhm, 2016). A clear communication gap regarding the rationale behind usage restrictions may contribute to suboptimal adherence to safety protocols. Furthermore, the observed inconsistency may be attributed to a broader lack of awareness among HCWs about the potential risks of exposure to cleaning agents.
Participants reported a decrease in the use of spray cleansers, replaced by hand-held wipes to prevent slips or falls. The adoption of ultrasonic cleaners for instrument cleaning was also mentioned as reducing exposure to certain cleaning products. A wide use of PPE, especially gloves, during cleaning tasks was reported; however, glove use varied depending on the task. We have reported the change toward the null of a previously observed (i.e., our 2003 study) negative association of new-onset asthma with powdered latex glove use. This likely reflects the widespread substitution of latex by non-latex products and improvements in the manufacturing use of less allergenic lightly powdered or non-powdered latex gloves (Kimberly-ClarkSterling, 2018; Korniewicz et al., 2005; Malerich et al., 2008; Patiwael & Burdorf, 2013; Turner et al., 2012). Although latex glove use has dramatically decreased in clinical settings, there are still some settings where hypoallergenic, non-powdered (or lightly powdered) latex gloves may still be used. In our 2003 study, we found that many latex control programs had been implemented in the mid to late 1990s, such that we found a marked decrease in the risk of allergy associated with latex glove use after 2000. When we again examined this association, the magnitude of the association was similar to that in 2003, probably indicating that controls for latex allergy have remained effective in the subsequent period. Training on cleaning products varied across job categories, with housekeeping staff receiving more focused training.
In aerosolized medication practices, participants reported administering various medications, significantly varying administration frequency and types. Changes in medications and protocols over time were noted, with specific emphasis on seasonal variations. Personal protective equipment protocols were in place to limit exposure, but adherence varied. Respiratory therapists reported the highest familiarity with medications and associated PPE, while other HCWs acknowledged challenges in PPE availability and policy adherence.
Healthcare settings are committed to regularly cleaning and disinfecting their facilities to prevent the spreading of disease and infection. But during the COVID-19 pandemic, particularly in its early phases when the risk of getting the SARS-CoV-2 virus from a contaminated surface was thought to be high, the frequency of cleaning and disinfection of surfaces intensified to reduce virus exposure from surface contact. This overall increase in the extent, frequency, and intensity of use of disinfectants, particularly bleach-based ones, not only in healthcare facilities but also in households may have exacerbated the effect of cleaning on asthma. Later, it was determined that COVID-19 spread mainly through the air, but it is still being determined if cleaning practices and use of products have returned to pre-pandemic levels. At the same time, that effect may have been buffered by the widespread use of tight-fitting respirators such as the N95 masks to reduce exposure to virus aerosols. However, N95 masks do not protect from chemical odors, gases, or vapors. Although there is likely a bi-directional association between cleaning products and practices and asthma, more research is needed to establish which direction predominates.
Implications for Research
The gaps identified in this study point to the need for further research into the bi-directional relationship between cleaning practices and asthma among HCWs. Future studies should explore the long-term impacts of changes in cleaning protocols introduced during the COVID-19 pandemic and assess whether these changes have resulted in sustained improvements in occupational health. In addition, research should focus on identifying the most effective interventions for reducing secondary exposure risks and improving overall compliance with PPE protocols.
Implications for Occupational Health
From an occupational health perspective, this study underscores the need for ongoing monitoring and evaluation of workplace practices in healthcare settings to ensure that they meet current safety standards. Occupational health professionals should advocate for more rigorous enforcement of PPE use and better communication of potential risks associated with exposure to cleaning agents and aerosolized medications. Furthermore, there is a need to develop and implement targeted interventions that address the specific challenges faced by different job categories within healthcare, particularly those with higher exposure risks.
In conclusion, this focus group study provided valuable insights into the current practices and potential risk factors associated with WRA among HCWs. The findings underscored the importance of consistent protection, knowledge dissemination, and adherence to PPE protocols. The identified gaps in understanding and potential sources of variability in exposure warrant further attention in occupational health and safety efforts.
Footnotes
Disclaimer
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the National Institute for Occupational Safety and Health (NIOSH) or the Centers for Disease Control and Prevention (CDC).
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JP—Implementation of research methods, data collection, primary data analysis, manuscript writing; GLD—Study design and framework, implementation of research, direction, and planning, supervision, manuscript writing; DGRdP—Study design and framework, primary data analysis, implementation of research, direction, and planning, manuscript writing; AC, LWH, and IH—Study design and framework, exposure assessment, provision of subject expertise; LP and SC—Study design and framework, exposure assessment; RP—Exposure assessment, data collection, and data analysis; JR—Project administration, data collection, and analysis; LM, JPZ, and PKH—Study design and framework, provision of subject expertise.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by a grant from the National Institute for Occupational Safety and Health (NIOSH), part of the Centers for Disease Control and Prevention (CDC) (Grant RO1OH010648). JP, DGRdP, AC, LWH, IH, and GLD were partially funded by the Southwest Center for Occupational and Environmental Health (![]() ), the NIOSH Education and Research Center at The University of Texas Health Science Center at Houston School of Public Health, and awardee of Grant No. T42OH008421 from the CDC/NIOSH.
), the NIOSH Education and Research Center at The University of Texas Health Science Center at Houston School of Public Health, and awardee of Grant No. T42OH008421 from the CDC/NIOSH.