
Abstract
This study investigated whether factors related to bodily contact between health care workers and patients were associated with patient-initiated violence. This cross-sectional study surveyed 496 Danish health care workers measuring patient-initiated violence, use of assistive devices, body mass index, physical exertion, frequency of patient transfers, psychosocial work environment, gender, age, and seniority. Associations were modeled using logistic regression analyses using patient-initiated violence as the outcome. Twenty-five percent of the respondents had experienced physical or verbal violence during the past year. Infrequent use of assistive devices, high physical strain, and severe obesity all significantly increased the risk of physical violence (risk ratio [RR] = 1.18, RR = 1.18, and RR = 1.16, respectively), whereas only the lack of assistive device use significantly increased the risk of verbal violence (RR = 1.13 and RR = 1.08). Consistent use of assistive devices appears to reduce the risk of patient-initiated violence. Managers should require the use of assistive devices when designing work processes for patient transfers.
Keywords
It is well known that workplace violence in health care facilities increases workers’ risk of physical injury and death (Hsiao & Stout, 2010; Maguire & Smith, 2013), post-traumatic stress disorder (PTSD; Jacobowitz, 2013; Richter & Berger, 2006), depression (Bishop & Phillips, 2006; Gerberich et al., 2004), burnout (Estryn-Behar, Van Der Heijden, Fry, & Hasselhorn, 2010), less productivity (Gates, Gillespie, & Succop, 2011), less job satisfaction (Estryn-Behar et al., 2008), staff turnover (Alameddine, Mourad, & Dimassi, 2015; Heponiemi et al., 2014), and long-term sickness absence (Niedhammer, Chastang, Sultan-Taïeb, Vermeylen, & Parent-Thirion, 2013; Slany et al., 2014). Although workplace violence has long been recognized as an occupational hazard for individuals, organizations, and society, the problem continues (European Agency for Safety and Health at Work, 2010; Eurofund, 2015). A better understanding of workplace violence is needed to more efficiently target preventive initiatives. The reported prevalence of occupational violence is generally higher in health care studies than in general industry studies. In 22 European countries, the prevalence of workplace violence ranged from 6% to 22% across all worker populations (Eurofund, 2015). In the health care sector, studies on workplace violence report prevalences ranging from 18% to 87% (Cheung, Lee, & Yip, 2017; Hanson, Perrin, Moss, Laharnar, & Glass, 2015; Hylén, Kjellin, Pelto-Piri, & Warg, 2017; Pompeii et al., 2013; Sun et al., 2017) The actual prevalence of workplace violence is uncertain, partly due to differences in definitions and policies regarding recognition and documentation (Lanctôt & Guay, 2014). However, it is known that health care is a high-risk occupation for violence, which is typically perpetrated by patients and families (i.e., Type II workplace violence; Hahn et al., 2013). Working with patients who are mentally or emotionally unstable (Hahn et al., 2013; Pompeii et al., 2013) or under the influence of alcohol or drugs (Gillespie, Gates, Miller, & Howard, 2010; Speroni, Fitch, Dawson, Dugan, & Atherton, 2014) increases the risk of violence. Younger health care workers and workers with low seniority are at increased risk of violence (Fafliora et al., 2016; Hylén et al., 2017). Studies have indicated that being male increases workers’ risk of physical violence, whereas being female increases workers’ risk of verbal violence (Edward et al., 2015). Work environment factors (e.g., high quantitative demands, poor leadership, and lack of peer support) are all associated with a higher prevalence of violence (Agervold & Andersen, 2006; Roche, Diers, Duffield, & Catling-Paull, 2010; Sharipova, Hogh, & Borg, 2010). Working evening or night shifts has also repeatedly been found to increase the risk of violence (Diderichsen et al., 2016; Pinar et al., 2015; Ridenour et al., 2015).
One reason for the prevalence of occupational violence in health care may be the high frequency of face-to-face interaction compared with other industries. Studies have shown that frequency of contact with patients is positively associated with risk of violence (Çelik, Oktay, & Çebi, 2017; Koritsas, Boyle, & Coles, 2009). Likewise, tasks with close bodily contact (e.g., moving, dressing, or bathing patients) have been associated with acts of violence (Arnetz et al., 2015; Lanza, 2009; Rosenthal, Edwards, Rosenthal, & Ackennan, 2009; Xing et al., 2015). Understanding circumstances regarding physical contact between patients and caregivers might clarify effective preventive strategies to address occupational violence.
Working in close proximity to patients is a basic requirement of health care. Use of mechanical or other assistive devices to prevent work-related musculoskeletal disorders (e.g., back injuries) is common and can be expected to become more widespread in the future (Edlich, Winters, Hudson, Britt, & Long, 2004; Schoenfisch, Lipscomb, Pompeii, Myers, & Dement, 2013). Use of assistive devices may also be relevant to the occurrence of occupational violence because physical contact between patients and health care workers may initiate violent episodes (McGuire, Moody, Hanson, & Tigar, 1996; Ouellet & Rush, 1996). Patients experience less pain and feel safer when assistive devices are used during transfers and repositioning (Kjellberg, Lagerström, & Hagberg, 2004; McGuire et al., 1996), and health care workers experience less fatigue, irritability, and pain (Silverwood & Haddock, 2006). These study findings suggest a reduction in potential negative effects for both patients and caregivers that could prevent violent behavior.
Even though the use of assistive devices is increasing in general hospitals, research in this field has focused primarily on preventing occupational back injuries and musculoskeletal pain (Aslam, Davis, Feldman, & Martin, 2015). Only one study has specifically addressed assistive devices and risk of violent behavior. In an intervention study, Risør, Casper, Andersen, and Sørensen (2017) found that training health care workers to use assistive devices decreased violent behavior (odds ratio [OR] = 0.4) compared with a control group. However, the study did not clarify what part of the intervention, training, or use of assistive devices reduced patient-initiated violence. The effect may be the result of better quality care rather than the use of assistive devices (Risør et al., 2017).
The primary purpose of the present study was to investigate whether consistent use of assistive devices reduced exposure to violence. Second, because studies indicated that bodily contact and proximity to patients might be a primary factor in eliciting violent responses, the researchers also investigated whether other factors regarding physical contact between patients and caregivers affected the risk of violence, namely, (a) caregiver body mass index (BMI), (b) caregiver physical exertion, and (c) frequency of patient transfers.
Method
This cross-sectional study included employees from two general hospitals in the greater Copenhagen area of Denmark. A questionnaire was emailed to 2,907 employees in 2015. Email addresses were not identified for employees who did versus did not transfer patient, but it was emphasized in the cover letter that the study focused on the work environment of employees who transferred patients. According to research protocol approved by the hospitals, one single email was sent to each employee without subsequent reminders. A total of 817 (28%) employees completed the questionnaire. Only the 496 employees (61%) who transferred patients were included in the study analysis. Respondents were employed in 12 departments, including anesthesiology, oncology, orthopedic surgery, neurology, internal medicine, and logistics, representing the following professions: nurses, physicians, and other health professions (e.g., social workers, clinical assistants, and physiotherapists).
Variables
Table 1 displays the variables used in this study. Outcome variables were physical and verbal violence measured as separate outcomes. The definition of workplace violence generally includes both physical and verbal aggression. The United States Department of Labor, Occupational Safety and Health Administration (OSHA; n.d.) defines workplace violence as “any act or threat of physical violence, harassment, intimidation or other threatening or disruptive behavior that occurs at the worksite.” Similarly, the European Commission defines work-related violence as “both physical and psychological violence: incidents where staff are abused, threatened or assaulted in circumstances related to their work, including commuting to and from work, involving an explicit or implicit challenge to their safety, well-being and health”(European Agency for Safety and Health at Work, 2010, p. 16). Based on these definitions, two items regarding threats and violence were included in the survey, both from the Joint Programme on Workplace Violence in the Health Sector Questionnaire. The items were modified to focus on violence during patient transfers and included exemplifying text to counter underreporting of everyday acts of violence due to normalization of these occurrences in the work culture.
Overview of Variables Listed by Variable Type, Construct Measured, Questionnaire Source, and Level of Measurement
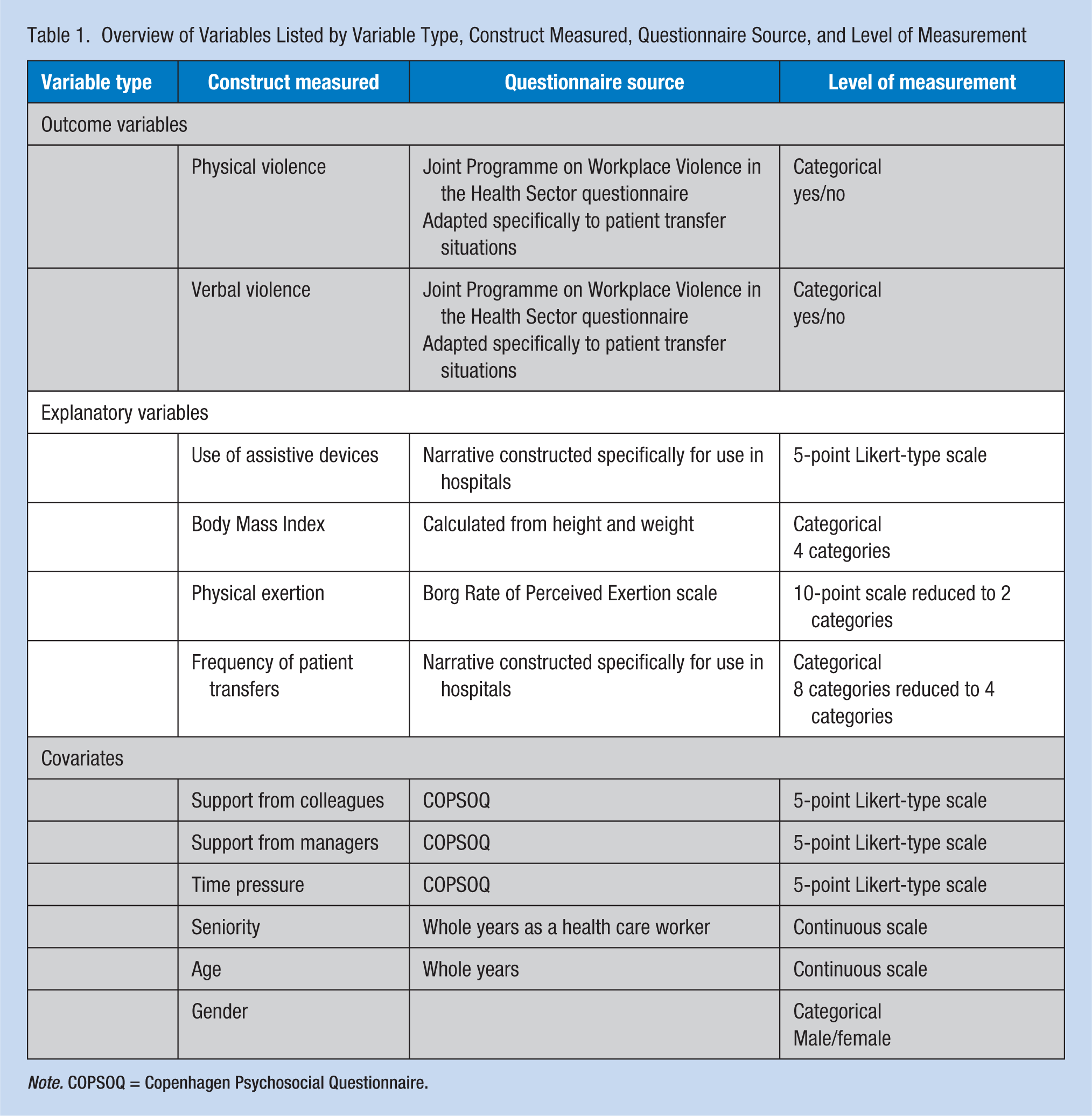
Note. COPSOQ = Copenhagen Psychosocial Questionnaire.
The single item on violence read, “Have you within the last 12 months been exposed to physical violence from patients during patient transfers (e.g., hitting, biting, pushing, pinching or pulling of hair)?” The single item about verbal violence read, “Have you within the last 12 months been exposed to verbal violence from a patient during patient transfers (e.g., threats or verbal abuse)?” For both items, responses were categorical answers of yes/no.
Explanatory variables
Four explanatory variables were used in the analysis. Use of assistive devices was measured with a single item: “Do you neglect to use assistive devices during patient transfer (Think about the situations where you ought to use assistive devices). “Respondents were offered a 5-point Likert-type scale from never to very often. BMI (measured as kg/m2) was categorized as “normal” (BMI < 25), “overweight” (25 < BMI > 29.9), “obese” (30 < BMI > 34.9), and “severely obese” (BMI > 35). “Physical exertion during transfer” was measured with a single scale based on the Borg Rate of Perceived Exertion scale (RPE; Andersen, Clausen, Persson, & Holtermann, 2013). Respondents were asked, “How would you rate your physical exertion in general during patient transfer?” with answers from the BORG CR10 scale, 0 (not at all strenuous) to 10 (very very strenuous, almost maximal). On this scale, 3 equals “moderate,” and the responses were collapsed into two categories: 0 to 3 “low/moderate degree of exertion” and 4 to 10 “high degree of physical exertion.” “Frequency of patient transfers” was assessed with a single item:
Patient transfer includes helping a patient move from one location to another or changing position (e.g., from bed to wheelchair, from chair to bedside commode, adjusting to sitting in bed or changing position in a wheel chair, turning, or lifting arms or legs. Patient transfer can also include help with dressing or personal hygiene. Do you perform patient transfers in your work?
The eight response categories ranged from “less than one patient daily” to “more than 10 patients daily.” For the subsequent analyses, the eight response categories were reduced to four categories: “less than one patient transfer a day,” “one to four patient transfers a day,” “five to eight patient transfers a day,” and “nine or more patient transfers a day.”
Covariates
Several covariates were included as possible confounders based on existing literature. Single items from the Copenhagen Psychosocial Questionnaire (COPSOQ) were included as proxy measures of “support from colleagues,” “support from managers,” and “time pressure” (Pejtersen, Kristensen, Borg, & Bjorner, 2010). All three items used a 5-point Likert-type scale ranging from never/almost never to always. “Seniority” was assessed as work years in the current profession measured in whole years, “age” was also measured in whole years, and both seniority and age were continuous variables. “Gender” was measured as male or female.
Statistical Analyses
The risk of workplace violence was estimated using Poisson regression with log link function. Risk ratios (RR) and 95% confidence intervals (CIs) were calculated for physical and verbal violence as outcome variables. Relative risk was used because of the high prevalence of both physical and verbal violence reported by the study sample. Explanatory mutually adjusted factors were “use of assistive devices,” “BMI,” “perceived physical exertion during patient transfer,” and “frequency of patient transfer.” The analyses were additionally adjusted for possible confounders: “support from manager,” “support from colleagues,” “time pressure,” “seniority,” “age,” and “gender.” Because the employees were situated in different departments, observations were not statistically independent (Twisk, 2006). PROC GENMOD of SAS version 9.2 was used for all logistic regression analyses, and the “repeated subject” option was used to adjust for random effects at the department level.
Study Approval
According to Danish law, survey-based studies do not require approval by a Scientific Ethics Committee. All respondents provided informed consent as part of their participation in the electronic questionnaire. The National Research Centre for the Working Environment has an institutional agreement with the Danish Data Protection Agency about procedures for handling confidential data (Journal number 2015-41-4232).
Results
Table 2 presents the descriptive statistics for the main variables. Eighty-five percent of the study population was women, the mean age was 44 years (SD = 11.2), and mean experience (seniority) was 7.4 years (SD = 7.8). The largest group of respondents was nurses (60.7%). Of the 411 respondents who answered the questions on violence, 25.5% had been exposed to physical violence and 25.1% to verbal violence during the past 12 months. The majority of respondents reported transferring patients one to four times per day (42.9%); 30.9% reported five or more patient transfers a day. Nearly 14% of the entire study population often or very often neglected to use assistive devices when transferring patients. Finally, only 2.2% of the study population was severely obese.
Descriptive Characteristics of the Study Population (N = 496)
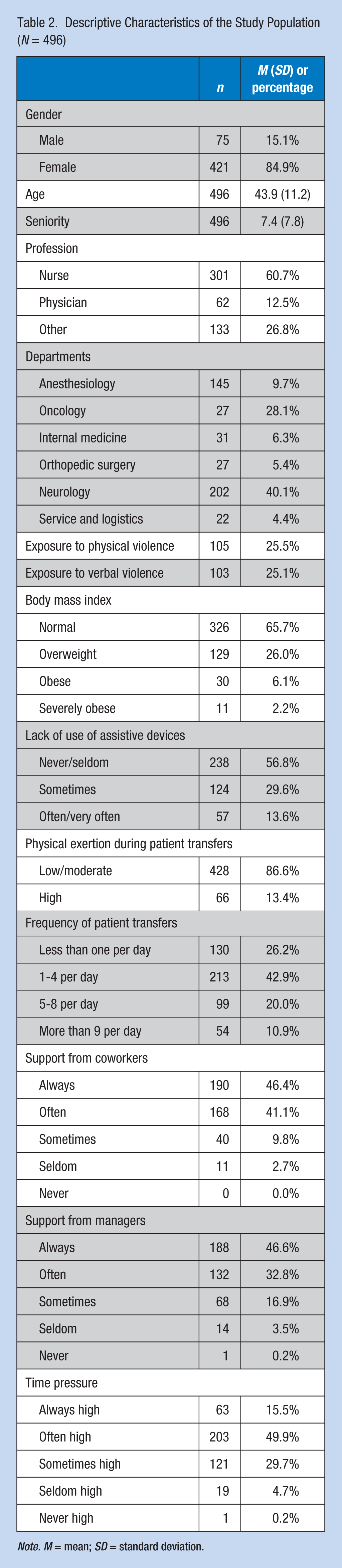
Note. M = mean; SD = standard deviation.
Table 3 presents RRs for physical and verbal violence as outcomes of each explanatory variable. Neglecting to use assistive devices “often/very often” increased the risk of both physical and verbal violence. Neglecting to use assistive devices “sometimes” increased the risk of verbal violence. More physical exertion during patient transfers and severe obesity increased the risk of physical but not verbal violence. Finally, a clear dose–response association was found between frequency of daily patient transfers and increased risk of both physical and verbal violence.
Risk Ratios (95% CI) of Physical and Verbal Violence Related to Use of Assistive Devices During Patient Transfers
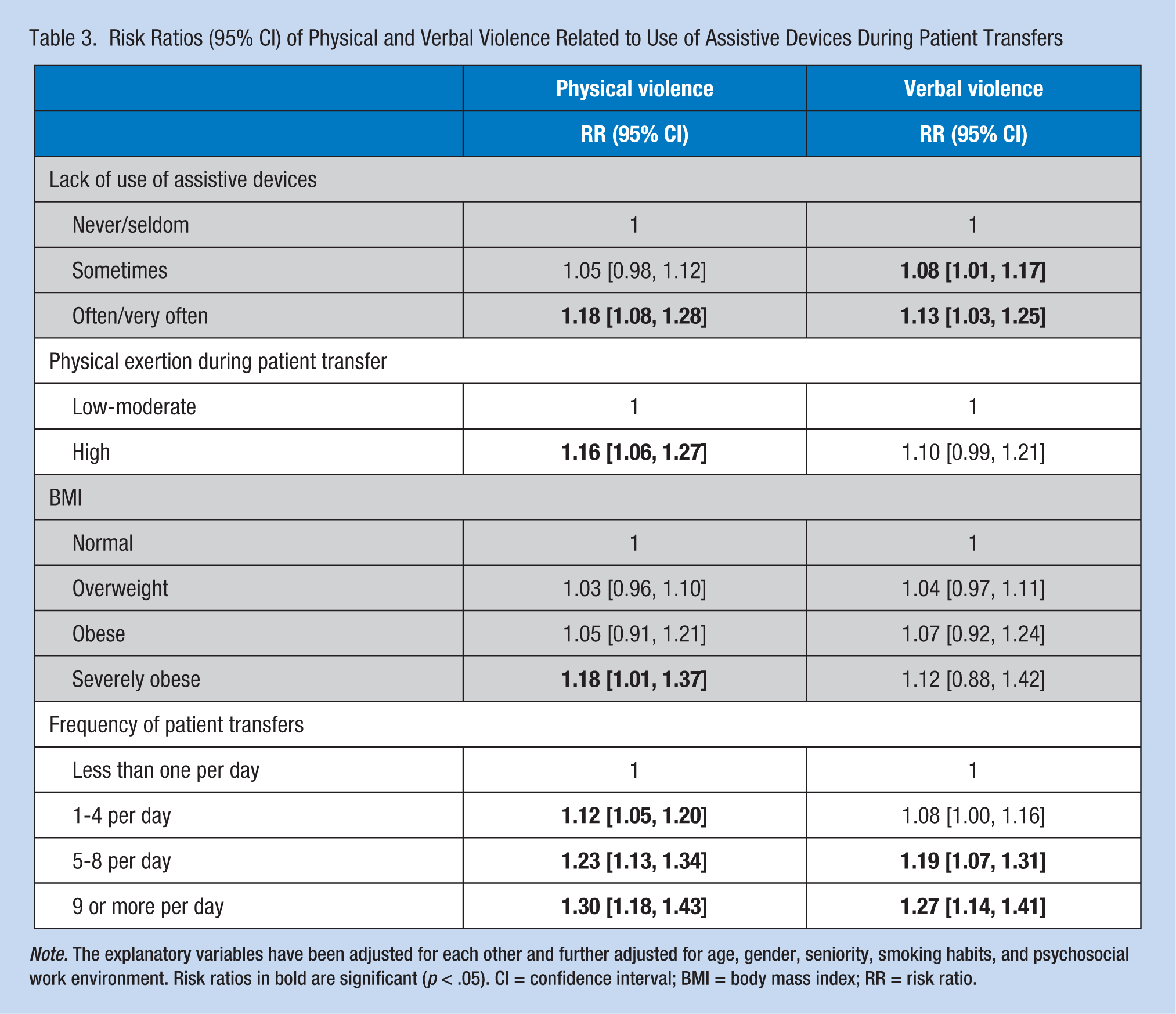
Note. The explanatory variables have been adjusted for each other and further adjusted for age, gender, seniority, smoking habits, and psychosocial work environment. Risk ratios in bold are significant (p < .05). CI = confidence interval; BMI = body mass index; RR = risk ratio.
Discussion
Only one study has investigated how the use of assistive devices might affect the risk of occupational violence. The present study shows that infrequent use of assistive devices increased the risk of both verbal and physical violence in the health care workplace. This finding is consistent with Risør and colleagues’ (2017) finding that training and use of assistive devices significantly reduced the risk of patient aggression (OR = 0.4). The current study focused on the use of assistive devices rather than worker training and found that the use of assistive devices alone was a key factor. However, more research on the associations between use of assistive devices and occupational violence is needed to draw conclusions regarding assistive devices as a protective factor.
The study also found that severe obesity and physical exertion during patient transfers increased the risk of physical, but not verbal, violence. No other studies have investigated these explanatory factors in relation to occupational violence, so confirmation of these findings is needed.
Finally, a dose–response relationship between frequency of patient transfers and risk of occupational violence was supported, confirming previous findings. Findorff, McGovern, Wall, Gerberich, and Alexander (2004) found that the risk of occupational violence increased in a dose–response pattern (OR = 6.7 for moderate frequency of patient contact and OR = 8.6 for high frequency of patient contact compared with low frequency of patient contact). Shi and colleagues (2017) found a dose–response pattern between risk of occupational violence and hours spent with patients in tertiary hospitals (2-4 hours: OR = 1.8; 4-6 hours: OR = 2.7; and 6-8 hours: OR = 3.07 compared with workers who spent less than 2 hours a week with patients). This finding was not supported for workers at communal hospitals for whom only 6 to 8 hours of patient contact per shift significantly increased the risk of occupational violence compared with less than 2 hours of patient contact per shift (OR = 1.7; Shi et al., 2017).
Despite the lack of studies regarding the relationship between occupational violence and “use of assistive devices,” “obesity,” and “physical exertion during patient transfer,” all three risk factors contribute to the type and proximity of physical contact between caregiver and patient. Assistive devices and mechanical lifting typically reduces physical contact (Risør et al., 2017), just as severe obesity increases bodily contact when caregivers reach over or around patients during turning, lifting, and repositioning tasks. Similarly, employees who report higher levels of exertion during patient transfer can be expected to decrease proximity to patients to either establish a better hold or use their own body weight to move patients. In light of these practical implications, study results are generally consistent with multiple studies that have demonstrated contact and proximity to patients increase the risk of occupational violence. Whittington, Shuttleworth, and Hill (1996) found that in a population of 396 health care professionals at a general hospital, a main precursor for workplace violence was initiating physical contact with patients (e.g., moving, dressing, or providing personal hygiene; Whittington et al., 1996). In a survey study of 840 health care workers, Xing and colleagues (2015) found the risk of violence almost doubled when dressing, bathing, or moving patients, all work tasks that increase bodily contact between patients and caregivers (Xing et al., 2015). Finally, Arnetz and colleagues (2015) studied 214 documented incidents of Type II violence and found that working in close proximity to patients was a situational factor leading to violence. Both patient transfer and care that causes patients pain (e.g., repositioning patients) triggered violent behavior (Arnetz et al., 2015).
The present study cannot discern the causal mechanism between use of assistive devices and risk of occupational violence. However, Winstanley’s (2005) “cognitive model of patient’s aggression toward healthcare personnel” conceptualized the association. Hospitalization is generally stressful to patients, who are sick and in pain, in an unknown setting with little privacy and control. In this context of increased vulnerability, patients can be expected to have varying degrees of heightened arousal that may impair cognitive information processing due to attentional narrowing and a tendency to dichotomize information (Winstanley, 2005). In this state, patients may attribute negative perceptions to their surroundings, viewing caregivers as potential threats (Winstanley, 2005). In Winstanley’s model, patient transfers with close bodily contact may enhance patient stress, which increases the risk of occupational violence; close physical contact is known to heighten arousal and defensive responses (Åhs, Dunsmoor, Zielinski, & LaBar, 2014; Kennedy, Gläscher, Tyszka, & Adolphs, 2009). Neglecting to use assistive devices can result in more bodily contact and thus increase the risk of occupational violence. The conclusion that proximity and level of physical contact might augment the level of stress and risk for violence could also explain why severe obesity and high exertion during transfers increase the risk for occupational violence because both variables increase bodily contact between patient and caregiver.
Limitations
This study’s design was cross-sectional, and associations between use of assistive devices and violence cannot be interpreted as causation. It could be argued that aggressive patient behavior explains inconsistent use of assistive devices or that employees who refrain from using assistive devices have work habits that elicit violent responses. Indeed, longitudinal studies are needed to better assess possible causal pathways. Another consideration is information bias because data were solely collected through self-report; some of the data required extended recall periods. Although surveys are more amenable to large samples, subjective factors (e.g., mood, personal convictions, or workplace culture regarding violence) may result in over- or underestimation of reported violence. Also, the risk of overestimation of associations may result from participants’ general response style. The use of validated survey items may lessen the risk of information bias, but future studies combining multiple data sources would increase the validity of the associations found in this study. Selection bias might also affect study findings; employees exposed to violence may have been more motivated to answer the questionnaire compared with other employees, increasing violence estimates. Future studies should use randomized samples or other sampling strategies to compensate for this type of bias. Confounding factors are another limitation. Although the study incorporated multiple competing risk factors, the list of possible confounding variables is not comprehensive. For example, time of work shift and patient characteristics could both be confounders affecting the use of assistive devices as well as increasing the risk of violence. However, the interpretation and validity of the results are strengthened by the fact, that there is a general pattern where factors of close proximity increases risk of violence.
Conclusion
This study indicates that the use of assistive devices is central to lessening the risk of violence during patient transfer tasks when multiple known risk factors are controlled. Also, the study indicates that other factors pertaining to close bodily contact (i.e., severe obesity and high physical exertion) during patient transfers may trigger occupational violence. Future studies should investigate the potential for prevention of violence at work.
However, study results emphasized that assistive devices should be used to prevent patient-initiated violence. Furthermore, the results indicated that staff training should focus on patient transfer techniques that can be adapted to individual caregivers’ strength and body size to prevent occupational violence.
In practice, it is recommended that management encourages use of assistive devices and examines why and in what situations staff refrain from using these devices to change their behavior and secure beneficial effects that reduce work-related musculoskeletal disorders as well as patient-initiated violence.
Applying Research to Practice
Patient-initiated violence is a major risk for health care workers, and the risk of violence increases during work tasks that require bodily contact between patients and caregivers. Occupational health nurses and managers should increase their focus on the use of assistive devices during patient transfers because assistive devices appear to be a protective factor for patient-initiated violence. Transfer techniques should be adjusted to both the physical strength and body size of health care personnel because both factors are associated with patient-initiated violence.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Jesper Pihl-Thingvad is a licensed clinical psychologist and PhD student at department of Occupational and Environmental Medicine, Odense University Hospital. His main areas in both research and clinical work are occupational violence and work-related psychotraumatology.
Lars P. A. Brandt, MD and PhD, is head of department as well as head of the research unit at Department of Occupational and Environmental Medicine, Odense University Hospital. His areas of expertise within the occupational medicine are musculoskeletal problems, pain disorders, and stress.
Lars L. Andersen is professor at the National Research Centre for the Working Environment in Copenhagen, Denmark. His current research on work environment covers (a) epidemiological studies to investigate risk factors for sickness absence and disability pension, (b) randomized controlled trials with physical exercise programs and participatory ergonomics to prevent and reduce back or neck pain and to improve work ability and well-being, and (c) laboratory studies with physiological measurement to study responses to office work as well as heavy and fatiguing work.