
Abstract
Background: The evidence for the health benefits of physical activity is growing; however, the prevalence of unhealthy lifestyles continues to contribute to the increase in chronic non-communicable diseases. We know that occupational-time physical activity does not provide the same benefits as leisure-time physical activity, which has been shown to reduce mortality and pain. We also know that multiple factors influence pain; however, there are no studies that specifically analyze the impact of type of working time and occupational-time physical activity on the impairment of daily activities due to pain. We aimed to study the influence of both personal and occupational factors on the impairment of daily activities due to pain, assessing whether leisure-time physical activity acts as a protective factor. Methods: A cross-sectional, population-based design was used based on the 2017 National Health Survey in Spain (ENSE). Sociodemographic, leisure-time physical activity, and work-related variables were collected. The outcome variable was the impairment of daily activities due to pain. Ordinal logistic regression was applied, and the analysis was complemented with simple correspondence analysis. Results: A total of 1,441 workers between 18 and 65 years of age were studied. Significant differences were found between sexes for all variables except age and leisure-time physical activity. Logistic regression revealed significant associations between sex, primary and secondary education levels, no leisure-time physical activity, and overweight with impairment of daily activities due to pain. Simple correspondence analysis showed that the categories doing leisure-time physical activity several times a week as well as several times a month are closer to the categories of little or no pain. Conclusion: Female gender, low educational level, overweight, and lack of leisure-time physical activity were associated with increases in impairment of daily activities due to pain. Occupational-time physical activity and work shift were not related to impairment of daily activities due to pain. Implications for Occupational Health Practice: Occupational Health Nursing interventions through education and counseling on the importance of leisure-time physical activity promotion programs potentially can reduce the impairment of daily activities due to pain in working populations.
Background
Ever since Morris et al. published their famous article in 1953 on the increased risk of cardiovascular disease in London bus drivers due to sitting all day in front of constantly wandering ticket inspectors (Morris et al., 1953), the evidence for the beneficial effects of physical activity on health has been growing. Unfortunately, the prevalence of sedentary lifestyles and physical inactivity continues to increase worldwide, becoming the leading cause of premature death and contributing to the rise of chronic non-communicable diseases (Túnez Rodríguez et al., 2017).
Leisure-time physical activity (LTPA) is not the same as occupational-time physical activity (OTPA). Workers who perform moderate to strenuous efforts in their jobs and who do not engage in leisure-time physical activity have a higher risk of all-cause mortality compared to those who do not perform such efforts but do exercise in their leisure time (Bonekamp et al., 2023; Harari et al., 2015; Holtermann et al., 2012).
However, in addition to reducing overall mortality, physical activity benefits the workers who engage in it by reducing pain (Kirsch Micheletti et al., 2019). In Spain, chronic pain affects 17-18% of the population, with an intensity considered moderate to severe in 12% of cases. The age of patients treated in Spanish pain units is between 48 and 57 years, being productive members of the workforce. However, 89% of these patients are considered to have limited capacity for work (Caramés-Álvarez & Navarro-Ribero, 2016), and experience an annual average of 14 days of temporary work disability (Torralba et al., 2014).
The way in which exercise decreases pain may be due to the so-called exercise-induced hypoalgesia effect (EIH), the mechanisms of action of which are still being studied (Kami et al., 2022; Risa et al., 2021), but for which there is increasing evidence. Naugle et al. (2012), in a meta-analytic review, concluded that EIH varied from small to large effect sizes depending on pain characteristics and was most effective in chronic regional pain and at low-to-moderate intensity levels. Later, Booth et al. (2017), in a biopsychosocial approach to exercise for chronic musculoskeletal pain, also highlighted its benefit. Alzahrani et al. (2019) also pointed out the usefulness of aerobic exercise on non-specific low back pain in a systematic review and meta-analysis carried out in 2019 with more than 95,000 participants, something already pointed out by White et al. (2016) in a synthesis of systematic reviews on workers carried out in 2016.
More recently, both Belavy et al. (2021) and García-Correa (2021) in systematic reviews and meta-analyses corroborated the effect of the EIH on chronic pain. The same was done by Frutiger and Borotkanics (2021) and with the same design, but focusing on neck pain affecting white-collar workers.
Pain is influenced by multiple personal factors such as negative family environments, moods, educational level, and even gender (Gil-García & Cáceres Matos, 2020; Kami et al., 2022). It is also influenced by occupational factors such as shift work, work stress, or type of work (Chang & Peng, 2021; Lee et al., 2020).
The aim of this study was to examine the association between personal (LTPA, demographics, and body mass index [BMI]) and occupational factors (type of working time and occupational-time physical activity) and to examine if LTPA could act as a protective factor.
Methods
Study Design: Population and Sample
A cross-sectional, population-based design was used based on the 2017 National Health Survey in Spain (ENSE), carried out by the Spanish Ministry of Health, Consumer Affairs, and Social Welfare with the collaboration of the Spanish National Institute of Statistics (Ministry of Health, Consumption and Social Welfare, 2017). The ENSE 2017 was conducted by computer-assisted personal interview and complemented by telephone interview. It includes health information on the population residing in Spain in 23,860 households with a sample of 29,800 individuals (Figure 1).
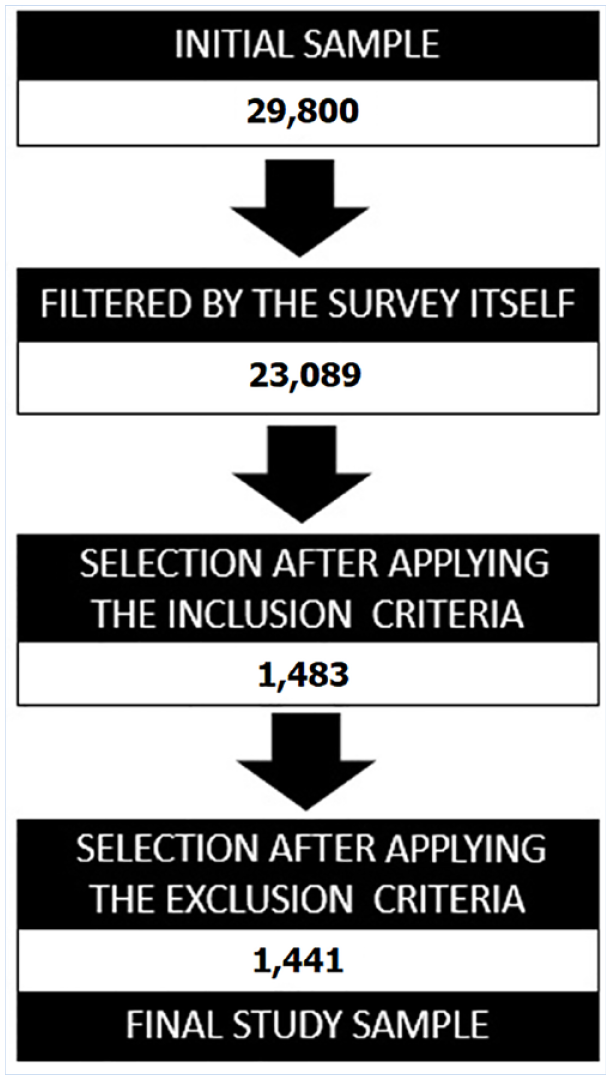
Flowchart of Participants.
The data collection period covered the period from October 2016 to October 2017. A stratified three-stage sampling method was used for the ENSE whereby the sample was distributed evenly and proportionally to the population of each autonomous community within Spain. Similarly, census tracts were selected within each stratum with probability proportional to their size.
Within each census tract, households were drawn using a systematic sampling method after sorting them by size, resulting in self-weighting samples in each stratum. The Kish random procedure, which assigns equal probability to all household members, was used for selecting respondents.
For the current analysis, a subsample of subjects was selected. The eligibility criteria were (a) being between 18 and 65 years old; (b) employed full-time (employed as a civil servant, for an indefinite period, or as an employer with or without dependants); (c) having at least one chronic or long-term health problem; (d) having had no traffic, domestic, or leisure-time accidents; (e) had not been admitted to the hospital in the last 12 months; and (f) having some degree of pain (from very mild to extreme) in the last four weeks.
Respondents answering ‘no response/don’t know’ to any of the variables analyzed and values not belonging to any of the categories included in the scales were excluded. The analysis of missing data was not significant (missing completely at random [MCAR] χ2 = 2.848, degree of freedom [df] = 1, Sig .= .09), with a loss of only 2.96%.
Variables and Measurements
The independent variables were demographics, including age measured in years, sex (male or female), educational level (cannot read or write, incomplete primary education, complete primary education, lower secondary education, high school studies, intermediate vocational education, higher vocational education and university studies), and BMI (underweight, normal weight, overweight and obesity). The work-related variables were type of working time (split shift, morning, afternoon, night, and shift work) and OTPA (sitting most of the working day, standing most of the working day, walking with some weight, and performing physically demanding tasks).
LTPA was categorized as none, occasional, several times a month, or several times a week, using the short version of the International Physical Activity Questionnaire (IPAQ). The short version has been shown to have a reliability of .65 (r = .76; 95% confidence interval [CI] = [0.73, 0.77]) and the validity coefficients suggest that the long and short versions have an acceptable reliability (r = .67; 95% CI = [0.64, 0.70]) (Pérez-Soto & García-Cantó, 2012). Finally, the outcome variable was impairment of daily activities due to pain (IDAP) (nothing, a little, moderate, quite a lot, a lot).
Ethical and Legal Considerations
The use of ENSE data does not require approval by an ethics committee. Files for public use are not considered confidential according to Regulation (EU) 2016/679.
Statistical Analysis
Statistical analyses were performed using IBM’s SPSS Statistics software (version 26.0).
To increase statistical power, the categories of the education level were merged into (a) primary education, (b) secondary education, (c) vocational education, and (d) university. The categories of the variable BMI were merged into (a) under weight or normal weight, (b) overweigh, and (c) obesity, and the categories of the variable type of working time were merged into (a) split shift, (b) morning or afternoon, and (c) night or shift work. The last two categories of the outcome variable IDAP, quite a lot and a lot, were also merged.
Quantitative variables were expressed as arithmetic means and standard deviations, and qualitative variables as absolute frequencies and percentages. A Mann–Whitney U for the comparison of medians and chi-square tests were used to analyze contingency tables. A cumulative odds ordinal logistic regression with proportional odds determined the factors related to IDAP. The statistical significance threshold was set at <5%. Confidence intervals were calculated with 95% certainty.
The analysis between IDAP and LTPA was complemented by a simple correspondence analysis.
Results
Description of the Study Sample
The overall sample size was 1,441 workers, between 18 and 65 years old; 655 were male (45.4%) and 786 were female (54.6%). In terms of education, secondary education was predominant (35.7%), followed by university studies (33%). The most common working time and activity level was split shift and mainly sitting for most of the working day, but closely followed by standing. Most did not exercise or exercised only occasionally. The most common BMI categories were underweight or normal followed by overweight. 65.7% reported IDAP between a little and quite a lot or a lot.
The comparison between men and women revealed significant differences for each variable analyzed, with the exception of age and LTPA. Significant differences were found in the levels of studies. More women completed university studies (38.4%, p < .001). Primary (11.8%, p = .02), secondary (38.8%, p = .03) and vocational education predominated in men. Morning or afternoon working hours were more common in women (46.1%, p < .001), and split working hours (49.3%, p < .001) and night or shift work in men. Men worked predominantly in jobs requiring walking with some weight (20%, p = .001) or performing physically demanding tasks. They were also more frequently in the heaviest weight categories: overweight (49%, p < .001) and obese (20.9%, p = .002). In the dependent variable, the categories of having none or little pain in daily activities were higher in men. Women were more likely to have moderate and quite a lot or a lot of impairment due to pain (Table 1).
Characteristic of the Study Sample and Gender Differences
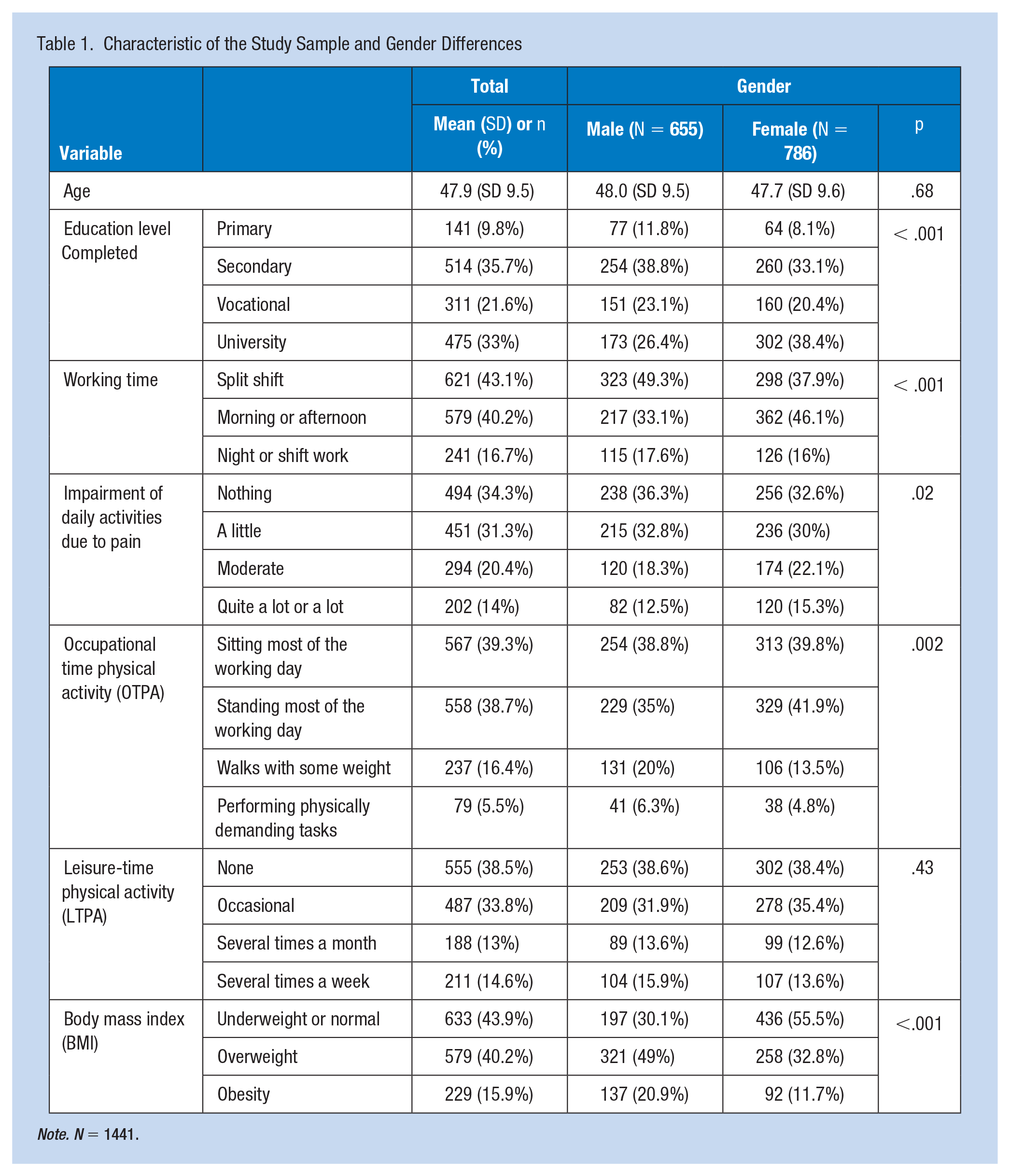
Note. N = 1441.
Factors Associated With IDAP
An ordinal logistic regression was carried out. The variance inflation factor (VIF) remained below 10 for all variables and categories, ruling out multicollinearity. There were proportional odds, as assessed by a full likelihood ratio test comparing the fitted model to a model with varying location parameters, χ2(18) = 829.08, p = .721. The deviance goodness-of-fit test indicated that the model was a good fit to the observed data, χ2(264) = 289.488, p = .135. Only 67 cells (18.2%) were sparse with zero frequencies. The final model statistically significantly predicted the dependent variable over and above the intercept-only model, χ2(9) = 843.2106, p = < .001. Working time and OTPA variables did not reach significant values. Significant associations were found between the dependent variable and sex, primary and secondary education level, no LTPA, and overweight (Table 2).
Ordinal Logistic Regression Adjusted for Sex, Education Level, LTPA, and BMI

Note. R2 Cox&Snell: .035; R2 Nagelkerke: .038. Ref: Reference Category.
The simple correspondence analysis between the variables IDAP and LTPA reached a cumulative proportion of inertia in the first dimension of 92.9%, reaching 99.4 for both dimensions (p = .008). Figure 2 shows how not doing LTPA is closer, in both dimensions, to the category having quite a lot or a lot of pain. The categories doing LTPA several times a week or a month are closer to the categories a little or no pain (Figure 2).
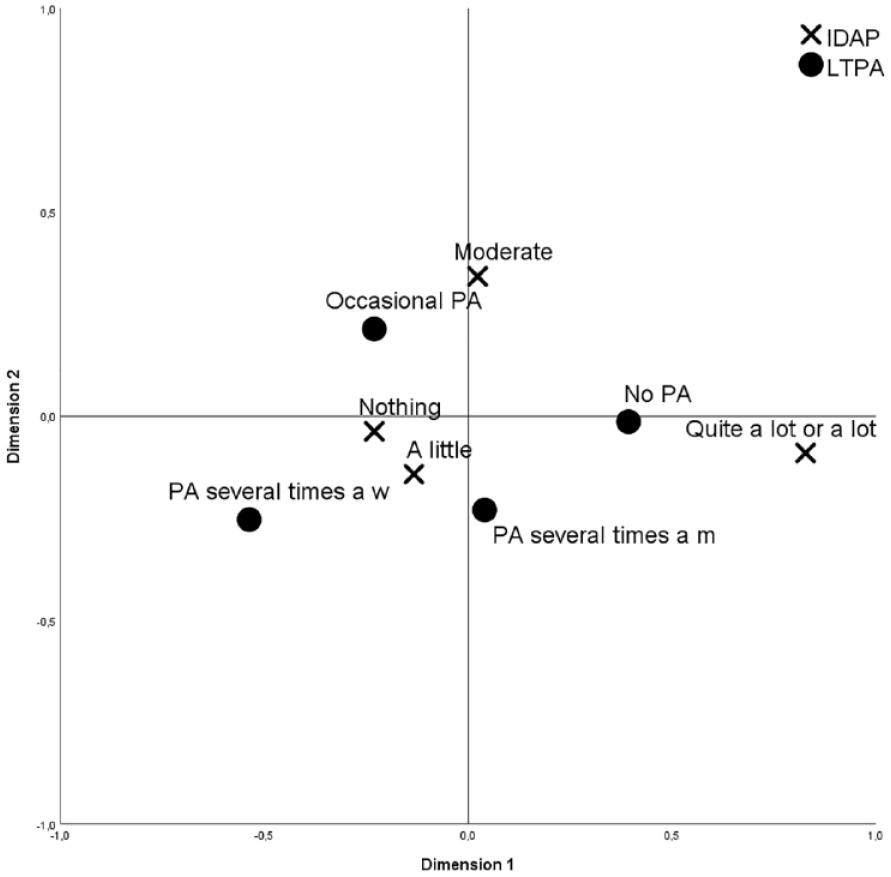
Simple Correspondence Analysis Between IDAP and LTPA.
Discussion
We found that being female, having low levels of education, being overweight, and not doing LTPA were associated with IDAP. Gender differences in our population have been highlighted in previous studies. Women were more highly educated, although they tended to occupy lower-qualified positions (OSALAN-Instituto Vasco de Seguridad y Salud, 2021), with working hours that they tried to reconcile with family responsibilities (Boniol et al., 2019) and which, together with other factors, such as socioeconomic differences due to gender discrimination, would also explain why they were less physically active (De-Pedro-Jiménez et al., 2021). In this case, however, we only found significant differences in terms of occupational activity. They also report higher levels of pain (Bautista Sánchez & Jiménez Santiago, 2014; OSALAN-Instituto Vasco de Seguridad y Salud, 2021, 2021), mainly chronic, disabling, or limiting normal daily activities (Gil-García & Cáceres Matos, 2020).
Multivariate analysis, after adjusting for gender, education level, LTPA and BMI, confirms that IDAP is more associated with female gender, low education levels, non-exercise, and overweight.
Although no relationship was found between LTPA and IDAP to affirm that certain degrees of physical activity reduce IDAP, with our results we can affirm that it is the lack of LTPA that is associated with increased levels of IDAP. Moreover, this lack of physical activity is also associated with overweight and obesity (Petridou et al., 2018), which has an impact on IDAP. The highly significant value in the unifactorial relationship between the IDAP and LTPA variables allowed a simple correspondence analysis, which, reaching 99.4% of accumulated inertia, supports and consolidates the relationship between IDAP and lack of LTPA. It is easy to see in Figure 1 the relationship between those who do not exercise with a fairly high IDAP versus those who exercise several times a week and have little or no IDAP.
Associations between pain (mainly musculoskeletal) and physical inactivity have been highlighted, as well as the fact that some pain conditions may depend on the type of physical work demands (Dzakpasu et al., 2021). Similarly, other authors have pointed out that the benefit of LTPA on workers may depend on the type of OTPA, the lower the OTPA, the better (Prince et al., 2021). In our case, we found no relationship between OTPA and IDAP, possibly due to the selection criteria applied, the average age of the sample, and the fact that we did not control the type of work carried out. Alternatively, this lack of association may be because we did not study the relationship between OTPA and pain, with clear evidence of an association (Cillekens et al., 2020; Neuhaus et al., 2014; Thompson, 2017), but rather OTPA and its relationship with IDAP.
The limitations of the study were that the evaluation of the amount of exercise was based on questionnaires and on non-specific pain. Second, we did not assess variables that might have been interacting with IDAP, such as socioeconomic level (although indirectly through their relationship with the level of studies), the type of work carried out or the presence of previous pathologies, and other habits, such as the consumption of painkillers, that could be related to IDAP. Finally, the results can only be extrapolated to the Spanish working population. The considerable sample size used and the particular approach to pain related to limitations of daily activities were strengths of our study.
Applying Research to Occupational Health Practice
Neither OTPA nor type of working shift affected workers who reported some form of IDAP (moderate to very high). Female gender, low educational level, overweight, and lack of LTPA were associated with increases in IDAP. Further studies with an analytical design are needed to confirm the protective effect of physical activity against IDAP in workers. Yet, these findings suggest that, while no practice change is indicated, a continued emphasis on preventive health counseling around increased movement and exercise during personal time is warranted.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.