
Abstract
Introduction
Physical activity and social engagement protect older adults against functional decline and improve their quality of life. Physical inactivity poses an increased risk for noncommunicable diseases. Globally, one in four adults is physically inactive. Enhancing the physical activity of older adults is crucial not only for increasing their life expectancy but also for improving their functional status and quality of life.
Objective
This study aimed to evaluate the physical activity, functional status, and quality of life of older adults attending the medical outpatient department of a tertiary care hospital in Chennai, Tamil Nadu, India.
Methods
The study adopted a descriptive cross-sectional research design. A total of 100 female and male patients above 65 years of age with comorbid conditions attending the medical outpatient department participated in the study. The sociodemographic and clinical characteristics of these patients were assessed. In addition, the Rapid Assessment of Physical Activity, Katz Index of Independence in Activities of Daily Living, Lawton Instrumental Activities of Daily Living Scale, and Older People Quality of Life Questionnaire were used to measure the physical activity, functional status, and quality of life of patients. The data were analyzed using descriptive and inferential statistics.
Results
Among the participants, only 17% were active, and 35% were underactive for regular light activities. Approximately 81% did not perform any activity to improve their muscle strength or flexibility. In 56% of the participants, disability was present. The majority mentioned that they experienced difficulties in preparing food and shopping. Regarding the quality of life of the participants, the mean ± standard deviation score was 77.38 ± 9.03. Significant results were found in the domains of independence, control over life, and freedom. The overall quality of life was not related to leisure and activities, financial circumstances, the Instrumental Activities of Daily Living Scale score, the Rapid Assessment of Physical Activity 2 score, and the Rapid Assessment of Physical Activity 1 score. The quality of life was weakly related to emotional and psychological well-being, control over life, home and neighborhood, freedom, independence, and social relationships.
Conclusion
Limited physical activity and poor functional status impact the quality of life of older adults. Therefore, educational and physical interventions should be implemented at the hospital and community levels to improve the physical activity, functional status, and quality of life of older adults.
Keywords
Introduction
The aging population is increasing in both developed and developing countries (Chang et al., 2019). The World Health Organization (WHO 2022) projected that by 2050, older adults will make up 80% of the population in low- and middle-income countries. In 2020, the number of people aged 60 years and above surpassed the number of children aged under 5 years. Additionally, the global proportion of the aging population doubled from 12% in 2015 to 22% in 2020 (WHO, 2022). It is estimated that the population aged 65 years and above in the United States of America will double from 40 million to 88 million by 2050 (Jarzebski et al., 2021). In India, people aged 60 years and above constitute 8.6% of the total population (WHO, 2023). As the aging population continues to live longer, it is important for them to enjoy a healthy life and a high health-related quality of life (HRQoL) during their extended years (Langhammer et al., 2018).
Healthy aging includes reaching a specific age, independently performing activities of daily living (ADLs), remaining free from chronic illnesses, experiencing a high quality of life (QoL), maintaining good well-being, engaging in physical activity, actively participating in social activities, having minimal or no disability, and experiencing only insignificant loss of intellectual or functional abilities (Zhang et al., 2024). Many factors, including genetics, exercise, a healthy diet, and a healthy lifestyle, influence healthy aging. Additionally, a positive attitude and mental well-being enhance the QoL in advancing years (Kassis et al., 2023). A recent systematic review has highlighted that health promotion/empowerment, lifelong person-centered interactions, and adaptation are crucial for healthy aging (Menassa et al., 2023). Moreover, it is essential to provide older adults with resources, build trusting relationships with healthcare providers, and identify and implement effective strategies and programs (Dev et al., 2020).
Literature Review
In older adults, physical activity improves their well-being, QoL, and mental health and delays the onset of dementia (Langhammer et al., 2018). The risk of noncommunicable diseases such as stroke, diabetes mellitus, cancer, and cardiovascular diseases can also be reduced with improved physical activity (Jakicic et al., 2019). Further, physical activity lowers body mass index (BMI) and improves overall health among older adults (Dhuli et al., 2022). However, a lack of physical activity increases the risk of many chronic illnesses. Factors such as age, marital status, sex, educational level, income, and the presence of health problems affect the physical activity levels of older people (An et al., 2020). Despite the well-documented effects of physical activity, the levels among older adults remain low (Boulton et al., 2018).
As people age, their physical activity and functional capacity decline due to loss of muscle mass, decreased range of motion, and diminished aerobic activity (Elam et al., 2021). Functional status refers to an individual's ability to perform ADLs across various aspects of life, including physical, intellectual, psychological, and spiritual functions (Idaiani & Indrawati, 2021). Activities of daily livings and instrumental ADL (IADLs) are measures used to assess the functional status of individuals (Edemekong et al., 2019). The QoL of individuals depends on their functional status. Factors such as age, the presence of comorbid conditions, depression, cognitive status, activity level, and social support influence functional status. In older adults, physical activity is strongly linked to functional status (Dombrowsky, 2017). When individuals need assistance with at least one ADL, it indicates a decline in functional status. This decline can lead to anxiety, a reduced sense of belonging, financial burden, and depression among older adults and their caregivers (Kwon et al., 2019).
Quality of life is an important indicator of subjective well-being, successful aging, happiness, and life satisfaction (Prati, 2022). Adequate social support, health-related knowledge, health-promoting behavior, and self-efficacy are determinants of a higher QoL among older adults (Feng et al., 2020). Currently, while the life expectancy among older adults has increased, comorbid conditions such as diabetes mellitus, hypertension, and heart failure have also become more prevalent. Therefore, HRQoL is considered an essential patient-reported outcome (Saqlain et al., 2021). With the growing older population, it is crucial to ensure that their physical activity, functional status, and QoL are maintained. Providing quality healthcare services and adequately addressing the needs of older people is essential to preserving their physical and mental health and their degree of independence (Ghenţa et al., 2022).
In the aging population, physical function is considered a significant predictor of QoL (Medhi et al., 2019). Earlier evidence shows that poor functional status leads to reduced HRQoL in older adults with chronic illnesses (Pei-Shan et al., 2020). According to Aung et al. (2022), the ability to perform ADLs is the most common determinant of HRQoL among adults. Moreover, the extent of independence in performing simple and complex activities determines the QoL of older people (Ćwirlej-Sozańska et al., 2020). Thus, maintaining physical activity and functional status is important for enabling older adults to perform self-care. A recent longitudinal survey conducted in India indicated that 27.39% of older adults had multimorbidities, and most of them did not engage in any moderate and vigorous physical activities. In another study, older adults who reported low levels of physical activity experienced more multimorbidities (Boro & Saikia, 2022).
To date, no studies have yet determined the relationship between physical activity, functional status, and QoL among older adults in Tamil Nadu, India. Furthermore, the authors observed that many older adults attending the outpatient department (OPD) of the data collection setting had limited physical activity, functional status, and QoL. Therefore, the authors decided to objectively measure these variables to obtain baseline data for designing interventions to improve the QoL of older people.
Methods
Approach
The study utilized a quantitative research approach.
Design
The study adopted a cross-sectional research design.
Setting
The study was conducted at the Medical Outpatient Department (OPD), `G' block, Sri Ramachandra Tertiary Care multi-specialty hospital, Chennai, Tamil Nadu, India. The hospital has 1,500 beds, 114 ICU beds, and 25 operating rooms, making it one of the largest private healthcare facilities in South Asia. Both male and female patients, along with their caregivers, visit the OPD for consultations. Older adult patients commonly visit the OPD to seek consultations for comorbid conditions, such as diabetes mellitus, hypertension, chronic obstructive pulmonary disease, tuberculosis, and osteoarthritis, as well as acute conditions, such as febrile illness, diarrhea, and fatigue.
Population
The study population included both male and female patients above 65 years of age attending the medical OPD of the target hospital.
Sample and Sample Size
The sample size was determined based on the physical activity variable outlined by Gomes et al. (2017). The calculation resulted in a sample size of 94, which was rounded up to 100 for an 80% confidence interval (CI).
Sampling Technique
Convenience sampling was used to select study participants.
Inclusion Criteria
The study included both male and female patients above 65 years of age with comorbid conditions such as diabetes mellitus, hypertension, and cardiovascular diseases attending the medical OPD.
Exclusion Criteria
The study excluded patients with known psychiatric illness and cognitive impairment, as they may not be able to provide appropriate responses.
Description and Interpretation of the Data Collection Tool
Part 1: Sociodemographic Variables
The sociodemographic variables evaluated included age, sex, marital status, educational level, employment status, family income, and family type.
Part 2: Clinical Variables
The clinical variables recorded included height, weight, and BMI.
Part 3: Rapid Assessment of Physical Activity
The Rapid Assessment of Physical Activity (RAPA) is a self-administered tool used to assess physical activity levels. It has two components and nine items. Seven items are included in RAPA 1 and two items in RAPA 2, with responses provided in a yes/no format. RAPA 1 measures overall physical activity, while RAPA 2 assesses strength and flexibility. The RAPA evaluates physical activity levels ranging from sedentary to vigorous activity and examines engagement in strength and flexibility training. For RAPA 1, the total possible score is 7. Individuals who score below 6 are considered to have suboptimal physical activity. For RAPA 2, strength and flexibility are scored separately, with scores assigned as 1 for strength training, 2 for flexibility training, and 3 for both. The r-value is 0.968 (Aktan et al., 2021).
Part 4: Functional Status
Part 4 of the data collection tool was divided into Parts A and B.
Part A: Katz Index of Independence in ADLs
The Katz Index of Independence in Activities of Daily Living is a semi-Guttman scale. The items of the scale are arranged in terms of difficulty in performing various functions. These functions include dressing, bathing, transferring, feeding, continence, and toileting. The adequacy of the performance of these six functions is measured by this scale. A high score of 6 indicates high independence, while a low score of 0 indicates high dependence.
Part B: Lawton IADL Scale
The Lawton IADL Scale assesses the ability of individuals to live independently in their own homes. Specifically, it evaluates their ability to shop, prepare food, use the telephone, take medications, do laundry, perform housekeeping tasks, manage finances, and use transportation. Each domain is scored, with a score of 0 indicating low functional ability and high dependence and a score of 8 showing high functional ability and independence.
Part 5: Older People Quality of Life Questionnaire
The Older People Quality of Life Questionnaire (OPQoL) consists of 35 items designed to evaluate QoL. Respondents indicate their level of agreement with each item using the following options: “strongly agree,” “agree,” “neither agree nor disagree,” “disagree,” and “strongly disagree.” Each option is scored from 1 to 5. The scale assesses various aspects of QoL, including health, independence, home and neighborhood, social relationships and participation, control over life and freedom, psychological and emotional well-being, financial circumstances, religion, and leisure activities. The total possible score ranges from 35 to 175. A score of 35 represents the worst possible QoL, while a score of 175 reflects the best possible QoL. Thus, a higher score indicates a better QoL.
Reliability of the Data Collection Tool
The Cronbach's alpha coefficient of the Lawton IADL Scale was 0.843. The test–retest reliability and interrater reliability of the Katz Index of Independence in ADLs were excellent (ICC = 0.999, 95% CI = 0.999–1.000). The internal consistency of the OPQoL was 0.78. For the RAPA, the sensitivity, specificity, and predictive value were 81%, 69%, and 77%, respectively.
Pilot Study
A pilot study was conducted with 10 patients at the medical OPD of the target hospital for 1 week. The study was deemed feasible, and no modifications were made during this pilot phase.
Ethical Considerations
The institutional ethics committee of Sri Ramachandra University granted ethical approval. Permission for data collection was obtained from the medical superintendent, nursing superintendent, and head of the general medicine department. The study purpose was explained to participants, who then signed a written informed consent form after having their queries answered. No participants were forced to participate in the study. Participants were informed that they could withdraw from the study at any time. All collected data were coded and stored in a password-protected file, with access limited only to the authors of the study.
Data Collection
The data were collected from March 7, 2022, to August 30, 2022, through patient interviews. The OPD register was checked, and patients who fulfilled the inclusion criteria and agreed to participate in the study were selected as study participants.
Data Analysis
The collected data were analyzed using descriptive and inferential statistics.
Results
The sociodemographic data of the participants are presented in Table 1. The mean ± standard deviation (SD) age of the participants was 71.30 ± 6.1 years. Among the participants, more than half were women; 81% were married; 61% completed primary school education; the majority were unemployed and had a low family income; and 38% belonged to a nuclear family.
Demographic and Clinical Characteristics of Older Adults (N = 100).
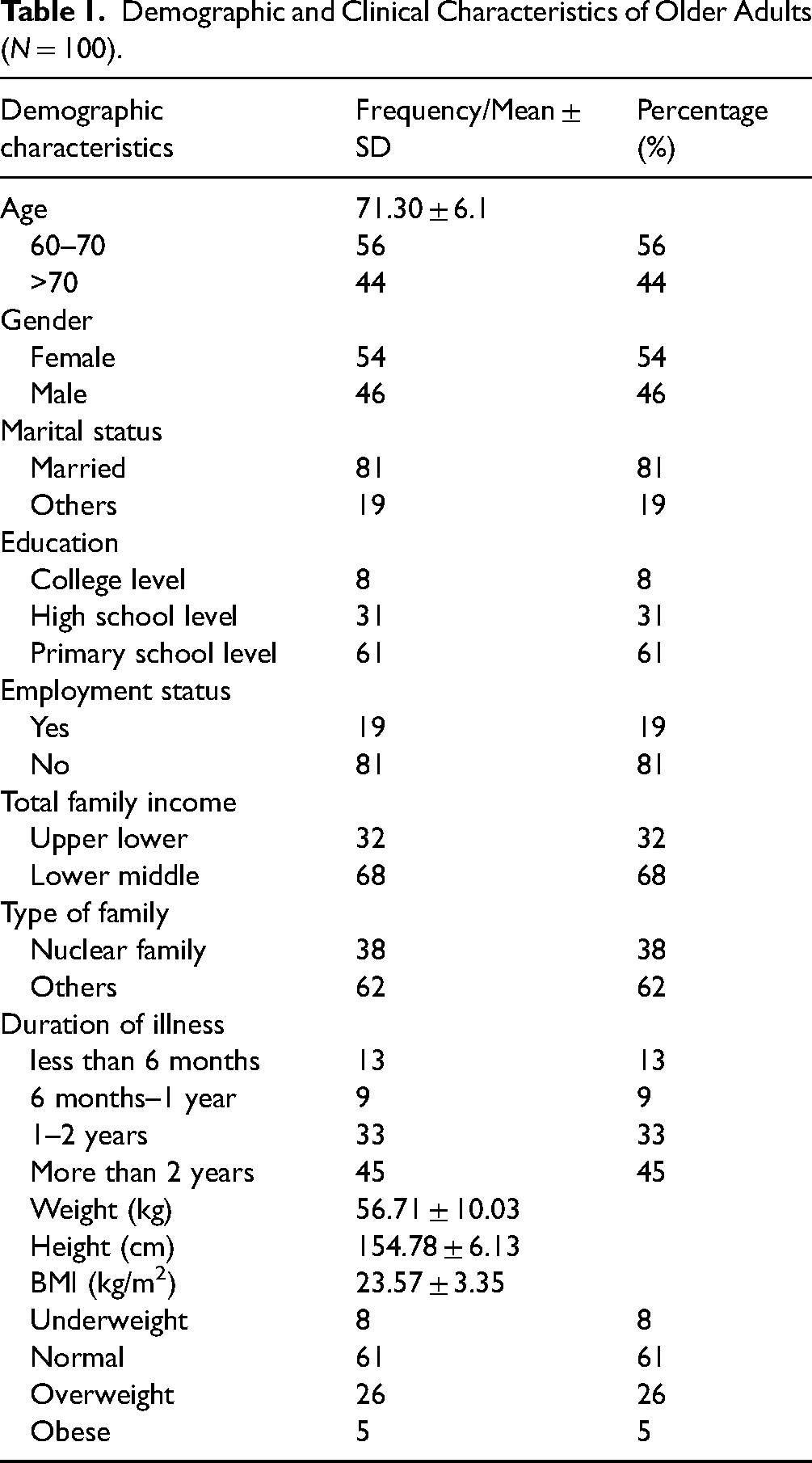
Approximately 45% of the participants had comorbid conditions lasting for more than 2 years. The mean ± SD BMI was 23.57 ± 3.35 kg/m2. The mean ± SD weight was 56.71 ± 10.03 kg, while the mean ± SD height was 154.78 ± 6.13 cm. Among the participants, 61% had normal weight.
Regarding physical activity, only 17% of the participants were active, while 35% were underactive for regular light activities. All participants were able to perform suboptimal aerobic activity. Approximately 81% did not perform any activity to improve their muscle strength or flexibility (Table 2).
Distribution of Physical Activity of Older Adults According to Rapid Assessment of Physical Activity (RAPA 1 and RAPA 2).

The mean ± SD IADL score was 4.47 ± 1.93. No significant difference in the IADL score was found between the age groups (Table 3). In terms of specific IADLs, 91% and 74% of the participants experienced difficulties in preparing food and shopping, respectively. Some participants also reported difficulties in using transportation, using the telephone, taking own medications, performing housekeeping, doing laundry, and managing finances (Table 4).
Prevalence of IADL Level of Dependency among the Older Adults.

Item-Wise IADL Level of Dependency among Older Adults.

Significant results were found in the QoL domains of independence, control over life, and freedom, with a mean ± SD score of 8.65 ± 1.43 (Table 5).
Various Domains of Quality of Life of Older Adults.

As shown in Table 6, the overall QoL was not related to leisure and activities, financial circumstances, the IADL score, the RAPA 2 score, and the RAPA 1 score. The QoL was weakly related to emotional and psychological well-being, control over life, home and neighborhood, freedom, independence, and social relationships.
Correlation Between Physical Function and Domains of Quality of Life.

*Correlation is significant at the 0.05 level (two-tailed).
**Correlation is significant at the 0.01 level (two-tailed).
Discussion
Health-related QoL is influenced by various factors including physical activity, functional status, and living environment. Evidence shows that a positive HRQoL is strongly associated with physical activity and functional status among older people (Furtado et al., 2022). Older people exhibiting sedentary behaviors have an increased risk of developing diabetes mellitus and cardiovascular diseases (Sparling et al., 2015). For considerable health benefits, the WHO (2020) recommended 150–300 min of moderate-intensity aerobic physical activity throughout the week for individuals aged 65 years and above. Functional limitations and disabilities in older adults could be prevented by performing short-term exercise and regular aerobic activity (Stathi et al., 2022). Despite having numerous benefits, regular physical activity has not been effectively incorporated into healthcare practice (Izquierdo et al., 2021).
Regular physical activity enhances both physical and mental well-being, helping older people stay mobile and independent. Most older people do not meet the minimum physical activity levels needed to maintain health despite knowing the benefits of physical activity. Furthermore, sedentary lifestyles predominate older age, resulting in a premature onset of disease and frailty (McPhee et al., 2016). Notably, the prevalence of physical inactivity in adults aged 55 years and above is relatively low in 16 European countries. Likewise, in Sweden, the prevalence is shown to be 4.9%. On the contrary, the prevalence of physical inactivity in Portugal is higher at 29%. Various factors contribute to physical inactivity including memory loss, lack of social support, old age, limitations with physical activity, lack of sense of meaning in life, and depression (Gomes et al., 2017). Conversely, self-motivation, good perception of their own health, and self-motivation are linked to higher levels of physical activity in older adults (Notthoff et al., 2017).
The number of older adults engaging in muscle-strengthening exercise, aerobic conditioning, flexibility training, and balance training is substantially low. Additionally, many older adults are unaware of the suggested components of physical activity plans (Morey, 2019). Consistent with these findings, significantly few older adults in the current study were active, and most of them were underactive for regular light activities. Moreover, the majority of the older adults did not perform any activity to improve their muscle strength or flexibility. Despite these findings, it is suggested that functional status, physical activity, and QoL can be improved by attending senior social clubs (Stolarz et al., 2022). Physical recreation activities, such as yoga and tai-chi, as well as strength and resistance training are suggested (Taylor et al., 2021). Exercise interventions in older adults should be encouraged and performed under supervision to prevent functional and cognitive decline. Healthcare systems should systematically plan evidence-based exercise programs for older adults to promote healthy and dignified aging in both hospital and community settings (Izquierdo et al., 2021).
Older adults who regularly participate in social activities and maintain an active lifestyle have shown improvements in their QoL (Jin et al., 2023). Instrumental ADLs require engagement in social activities (Guo & Sapra, 2020). Evidence suggests that physical and cognitive functions are positively associated with functional status in IADLs (Clemmensen et al., 2020). Additionally, physical activity is associated with improved cognitive function; thus, active participation in physical activity is recommended to improve and maintain cognitive function (Jin et al., 2023). Regardless of knowing the benefits of physical and social activities on the QoL of older adults, most of the older adults in the present study experienced difficulties in preparing food and shopping. They also reported difficulties in using transportation, doing laundry, performing housekeeping, using the telephone, taking medications, and managing finances. In line with these findings, Burman et al. (2019) observed that older adults who received education lower than the primary level were women, were separated/widowed, belonged to a joint family, had a poor economic status, were depressed, and had multimorbidities had dependency for ADLs and IADLs. Therefore, intervention programs should be designed to improve the well-being, physical activity, functional status, and QoL of older people (Furtado et al., 2022).
The growing aging population poses unique challenges for older people, including various health problems, shifts in social structure, and limited access to healthcare facilities. These challenges can affect the QoL of older people (Rony et al., 2024). In this study, QoL was related to emotional and psychological well-being, home and neighborhood, autonomy, control over life, freedom, and social relationships. Similarly, another study indicated poor infrastructure, lack of healthcare facilities, and limited resources negatively affecting the HRQoL of older people (Saqlain et al., 2021). Additionally, Silva et al. (2019) identified a negative correlation of sedentary time with upper-limb flexibility and light physical activity. Krishnappa et al. (2021) found that older people from rural areas had a lower QoL irrespective of sex, educational level, and financial dependence. Klompstra et al. (2019) reported that a poorer ability to perform ADLs, higher symptom burden, and higher degree of depression was negatively associated with QoL. Therefore, it is essential to provide quality healthcare services to older people and adequately address their needs. When their needs are met, their degree of independence will increase, and their physical and mental health will improve (Ghenţa et al., 2022). Additionally, inequitable health resource distribution and inadequate support systems must be addressed to improve the QoL of older people (Krishnappa et al., 2021).
Considering the findings of the current study and other relevant studies, healthcare policies should be revised, and effective interventions should be implemented in clinical settings to address the needs of older adults, with a specific emphasis on equitable healthcare access, effective management of chronic comorbid conditions, and training of geriatric healthcare professionals (Rony et al., 2024). In outpatient settings, interprofessional teams including geriatricians, nurses, occupational therapists, social workers, speech therapists, physiotherapists, pharmacists, and dietitians could work together in interprofessional geriatric clinics to meet the healthcare needs of older adult patients.
Limitations
The study population was limited only to patients attending the OPD of a tertiary care hospital. Therefore, the study results are limited only to the study setting. Further studies with larger populations are needed to expand the generalizability of the findings. Another limitation is that the outcome measures were self-reported, which may be affected by recall and social desirability bias. Therefore, future studies are recommended to utilize objective measurements. As the study adopted a cross-sectional design, a true causal relationship could not be established. Future studies should assess the causal relationship between the study variables by using appropriate research designs. Lastly, the present study was conducted over a short period.
Nursing Implications
The study findings call for incorporating more physical activities into the lifestyles of sedentary or lightly active older adults to improve their HRQoL. Healthcare providers should provide personalized information tailored to the needs of older adults. Further, older adults should be supported in developing physical activity goals to improve their functional status and QoL. Healthcare providers should organize functional capacity screening programs and assist older adults in improving their ability to perform ADLs and preventing future complications. Older adults should also be assisted in identifying and managing chronic illnesses.
Recommendations
This study can be conducted with larger samples in different settings. A comparative study can be performed to compare physical activity, functional status, and QoL between home-based and hospital-admitted older adults.
Conclusion
Limited physical activity and poor functional status reduce the QoL of older adults. Therefore, educational and physical interventions should be implemented at the hospital and community levels to improve the physical activity, functional status, and QoL of older adults.
Footnotes
Acknowledgments
The authors acknowledge the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was granted by the Institutional ethics committee (IEC/N/17/MAR/58/30). Permission for data collection was obtained from the medical superintendent, nursing superintendent, and head of the department of General medicine. The study purpose was explained to the study participants. Participants signed in the written informed consent form after getting their queries clarified. None of the participants were forced to participate in the study. Participants were told that they can withdraw their participation at any point of time. All the collected data collection instruments were coded and stored in a password-protected file. Only the investigators of the study have access to the data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.