
Abstract
Our study estimates the odds of older adults developing limitations in activities of daily living (ADL) and instrumental activities of daily living (IADL) after a fall and examines additional factors for developing ADL/IADL limitations. We used 2015-2020 Medicare Current Beneficiary Survey data and calculated crude and adjusted odds ratios of developing ADLs/IADLs with 95% confidence intervals (CI), adjusting for demographic and health variables. Older adults who fell had twice the odds of developing ADL (OR = 2.02; CI:1.70-2.39) or IADL (OR = 2.46; CI:2.11-2.87) limitations in the year following the fall compared with those who did not fall. Among those who fell, adjusted ORs for developing ADL or IADL limitations were significantly higher for adults aged 75+ compared with those 65-74, and for adults with 2 or more chronic conditions compared to those with less than 2 chronic conditions. Adjusted ORs were lower for adults who engaged in moderate or vigorous physical activity compared with those who did not. Although the likelihood of developing limitations after a fall may increase with age, engaging in physical activity or other preventive measures may be protective.
Keywords
“A comprehensive approach incorporating both individual-level and structural or environmental level strategies can be essential to achieving meaningful reductions in falls among older adults.”
Introduction
While many falls among older adults (ages 65 years and older) can be prevented, about one in four older adults report falling each year resulting in nearly 3.8 million emergency room visits and 1.2 million hospitalizations. 1 In the United States, the age adjusted fall death rate has increased over 30% over the past decade with about 41,000 deaths due to a fall-related injury reported in 2022.1,2 Additionally, non-fatal falls pose a substantial burden on health care systems with many injuries resulting in prolonged clinical needs and associated medical costs. 3 Serious injuries from falls such as hip fractures or traumatic brain injuries often lead to hospitalization. 4 A fall-related hospitalization also increases the likelihood of a long-term nursing home admission, leading to a temporary or permanent loss of independence. 5 A less severe fall or non-injurious fall may also lead to persistent pain, 6 fear of falling,7,8 increased risk of recurrent falls, 9 and decreased physical abilities often leading to functional limitations, that is, difficulties in performing activities of daily living (ADLs) and instrumental activities of daily living (IADLs).10-12
ADLs are activities related to personal care, including bathing or showering, dressing, getting in and out of bed, and eating. IADLs are activities related to independent living such as preparing meals, managing money, or shopping. 13 Difficulty in performing ADLs and IADLs result in dependence on other individuals for care and is a strong risk factor for decreased quality of life and future falls.14,15
The primary objective of this paper is to estimate the odds of developing ADL and IADL limitations in the year after a fall among older adults who did not have such prior limitations. The secondary objective is to identify the risk and protective factors for developing ADL and IADL limitations among older adults who have experienced a fall. We aim to understand the relationship between falls and ADLs and IADLs as a possible path to develop strategies and policies to reduce falls burden and maintain independence with advancing age.
Materials and Methods
Data
Data from the Medicare Current Beneficiary Survey (MCBS) were examined for this study. MCBS is a longitudinal, multistage, continuous survey of a nationally representative sample of Medicare beneficiaries, administered by the Centers for Medicare and Medicaid Services. 16 Each sampled beneficiary is selected as part of a panel and is interviewed up to 3 times per year (spring, summer, and fall rounds) for 4 consecutive years creating a continuous profile of selected beneficiaries’ health experiences. All the data elements used in this study were collected during the fall round (Oct-Dec) of each year from 2015-2020. These data elements include demographic and socioeconomic characteristics, residential location, history of falling, current limitations with ADLs and IADLs, physical activity level, and the presence of chronic conditions. The variables of interest in this study were abstracted from the following 4 MCBS survey files: demo (beneficiary demographics and socioeconomic characteristics), chrncond (chronic conditions), falls (falls), and nagidis (physical activity, muscle strength activity, activities of daily living and instrumental activities of daily living).
Our study examines 2015-2020 responses from Medicare beneficiaries aged 65 years and above who were community-dwelling and those who had no ADL/IADL limitations in the baseline year of the study. This restriction was to ensure that our outcome—development of a new ADL or IADL limitation—was not present at baseline. For the current study analysis, we examine the effect of falls in the baseline year on the development of ADL/IADL limitations in the following year. We combined the year pairs of 2015-2016, 2017-2018, and 2019-2020. The baseline year in this study is specified as 2015, 2017, and 2019, and the following year in this study is specified as 2016, 2018, and 2020. The final analytic sample for the study included 14,042 beneficiaries, population weighted to be representative of 61,227,941 continuously enrolled community-dwelling Medicare beneficiaries.
Measures
Dependent Variable (s)
We assess 2 outcomes in this study: Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs). ADLs and IADLs are defined according to criteria in the International Classification of Functioning, Disability and Health (ICF). 13 ADLs identified in this study include (1) bathing or showering, (2) dressing, (3) getting in and out of bed or a chair, (4) walking, (5) using the toilet, and (6) eating. If a beneficiary has difficulty performing any of these activities by himself/herself and without special equipment or does not perform the activity at all because of health problems, they are deemed to have a limitation in that activity. IADLs identified in this study include (1) preparing meals, (2) managing money, (3) shopping for groceries or personal items, (4) performing light housework, (5) performing heavy housework, and (6) using a telephone. Likewise, if a beneficiary has any difficulty performing any of these activities by himself/herself or does not perform the activity at all because of health problems, they are deemed to have a limitation in that instrumental activity. MCBS data pertaining to ADLs and IADLs are qualitative questions asked of each beneficiary with response options coded either as 1 = yes, there is difficulty performing the activity, or 0 = no, there is no difficulty performing the activity. We dichotomized beneficiaries into a diminished ADL vs non-diminished ADL group if any affirmative response was indicated for 1 or more of the 6 indicators of ADLs identified above. Likewise, we also dichotomized beneficiaries into a diminished IADL vs non-diminished IADL group if any affirmative response was indicated for 1 or more of the 6 indicators of IADLs identified above. Both ADL and IADL limitations are assessed in the following year (2016, 2018, 2020) after the year in which the fall was reported (2015, 2017, 2019) (hereinafter referred to as the baseline year). ADL and IADL limitations are assessed in the following year among older adults who did not have such limitations during the baseline year.
Independent Variable
The key independent variable in this study is a reported fall. Beneficiaries were asked if they experienced any fall in the baseline year and responses were coded as binary variables with 1 = yes, a fall occurred, and 0 = no, no fall occurred.
Covariates
To account for the influence of potential confounding, covariates were selected given existing literature of the associations between ADLs, IADLs, and various individual-level factors.17-23 They include demographics, socioeconomic characteristics, presence of chronic conditions, and level of physical activity. Socioeconomic characteristics and chronic conditions are categorized as risk factor covariates, whereas levels of physical activity are categorized as protective factor covariates. All covariates were measured in the baseline year.
Demographics
We include the following demographic variables in the study: racial identity and ethnic background, sex, age, and urban/rural geographical designation of residence. For racial identity and ethnic background, we grouped race and ethnicity due to small sample sizes and created a binary variable for race/ethnicity coded as 1 = non-Hispanic white and 0 = all others. For age, we stratified age into 3 categories 65-74 years, 75-84 years, and 85 years and older, given prior research that shows that among older adults the rate of falls among those 85 years and older is 4 times the rate for falls among older adults aged 65-74. 24 Sex is identified as 1 = male and 0 = female. Finally, urban/rural geographical designation included a measure of rural-urban commuting provided in the MCBS. Our study includes rurality as a binary variable coded as 1 = rural, 0 = urban.
Socioeconomic Characteristics
We include the following socioeconomic variables in the study: education and poverty level. Education was assessed using the highest level of education achieved. We created an indicator for education by grouping responses into a binary variable coded as 1 = less than a college degree and 0 = college degree or higher. For poverty level we used the MCBS income to poverty ratio Medicare threshold, which indicates the following income to poverty ratio classification: (1) less than 100% of the federal poverty level (fpl), (2) 100%-120% of the fpl, (3) 120% −135% of the fpl, (4) 135%-200% of the fpl, or (5) greater than 200% of the fpl. We created an indicator for poverty by grouping responses into a binary variable coded as 1 = income to poverty ratio of less than 120% and 0 = income to poverty ratio of greater than or equal to 120%, as Medicare establishes a threshold for specified low-income beneficiaries at an income to poverty ratio of less than 120%. 25
Chronic Conditions
Numerous chronic conditions have been identified to be associated with a higher prevalence of falling.26-28 We include the following chronic conditions in the study: Alzheimer’s, dementia, Parkinson’s disease, depression, mental disorder, atherosclerosis, hypertension, heart attack, congestive heart failure, other heart condition, stroke, diabetes, cancer, arthritis, rheumatoid arthritis, osteoarthritis, osteoporosis, partial paralysis, or loss of limb. Chronic conditions were reported based on the respondent ever being diagnosed with a condition (self-reported), with responses coded as 1 = yes, I have ever had this condition or 0 = no, I have not ever had this condition. We aggregated reported chronic conditions and classified 2 variables for the analysis: presence of at least 1 chronic condition and presence of multiple chronic conditions. Multiple chronic conditions were defined as having 2 or more affirmed responses for any of the above chronic conditions identified.
Physical Activity
We include 3 measures of physical activity in the study: vigorous physical activity, moderate physical activity, and muscle strength activity. CDC guidance recommends adults 65 years and older should get at least 75 minutes of vigorous activity (1 hour 15 minutes) per week, 150 minutes of moderate activity (2 hours 30 minutes) per week, or a combination of both each week. 29 It is also recommended to perform muscle-strengthening activities at least 2 days a week.30,31 Each activity level question asks beneficiaries to report the number of hours of activity performed each week. For descriptive analysis, we recoded the variable for vigorous activity as 0 = 0 hours reported per week, 1 = 1-2 hours reported per week, and 2 = greater than or equal to 3 hours reported per week. For moderate activity, we recoded the variable as 0 = 0 reported hours per week, 1 = 1-2 hours per week, and 2 = greater than or equal to 3 hours per week. For muscle strength activity, we recoded the variable as 0 = no muscle strength activity reported per week and 1 = 1 hour or more of muscle strength activity performed per week. For statistical analysis we created binary variables for each activity level. As only hours and not minutes of physical activity could be captured in MCBS, we rounded up to the next hour to create variables as comparable to the CDC guidelines as possible. Vigorous activity was coded as 1 = greater than or equal to 2 hours, 0 = less than 2 hours; moderate activity was coded as 1 = greater than or equal to 3 hours, 0 = less than 3 hours; and muscle-strengthening activity was coded as 1 = greater than or equal to 1 hour, 0 = less than 1 hour.
Statistical Analysis
Descriptive statistics were computed to provide baseline percentages of falls and baseline percentages of ADLs/IADLs for the study population. Using multivariable logistic regression, we calculated crude and adjusted odds ratios (OR) of the association of falls and diminished ADLs/IADLs, and calculated crude and adjusted ORs of the association of diminished ADLs/IADLs and demographic and physical activity characteristics among older adults who fell. All analyses accounted for survey design using the recommended longitudinal weights. Replicate weights were used with the balance repeated replication (BRR) method to account for correlations in the pooled data. 32 Complex survey procedures were conducted in SAS (version 9.4; SAS Institute); 95% confidence intervals (CI) were estimated and P-values <0.05 were used for denoting statistical significance. This study did not meet the criteria of human subjects research and was exempt from IRB approval.
Results
Percentage of Older Adults Reporting a Fall Without Limitations in Activities of Daily Living (ADL) or Instrumental Activities of Daily Living (IADL)in the Baseline Year, Medicare Current Beneficiary Survey, 2015-2020.
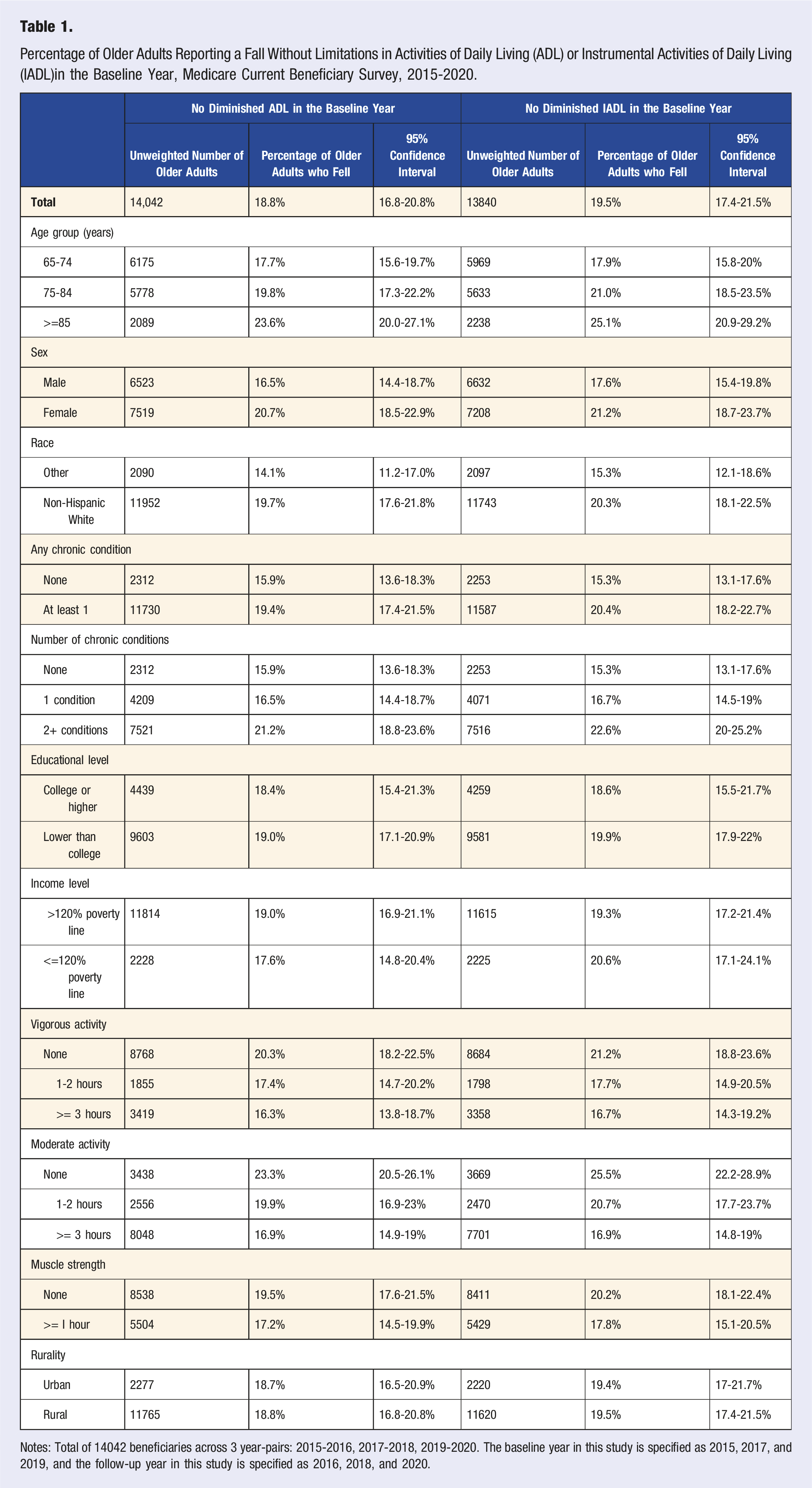
Notes: Total of 14042 beneficiaries across 3 year-pairs: 2015-2016, 2017-2018, 2019-2020. The baseline year in this study is specified as 2015, 2017, and 2019, and the follow-up year in this study is specified as 2016, 2018, and 2020.
Odds of Developing Diminished Activities of Daily Living (ADL) and Diminished Instrumental Activities of Daily Living (IADL) Resulting From a Fall Occurring in the Baseline Year, Medicare Current Beneficiary Survey, 2015-2020.
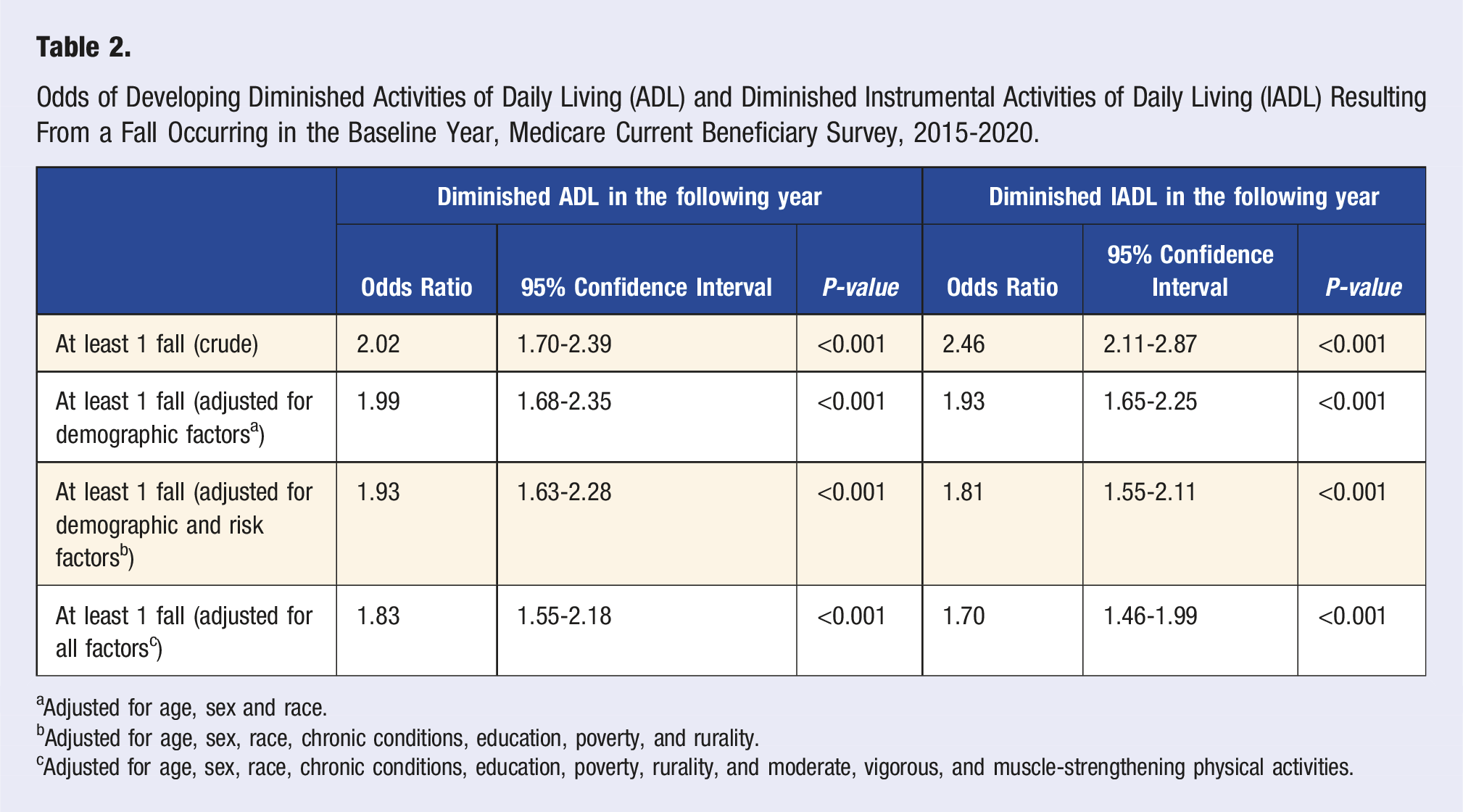
aAdjusted for age, sex and race.
bAdjusted for age, sex, race, chronic conditions, education, poverty, and rurality.
cAdjusted for age, sex, race, chronic conditions, education, poverty, rurality, and moderate, vigorous, and muscle-strengthening physical activities.
Crude Odds of Developing Diminished Activities of Daily Living (ADL) and Diminished Instrumental Activities of Daily Living (IADL) Among Older Adults Who Fell by Demographic, Risk Factor, and Protective Factor Covariates, Medicare Current Beneficiary Survey, 2015-2020.
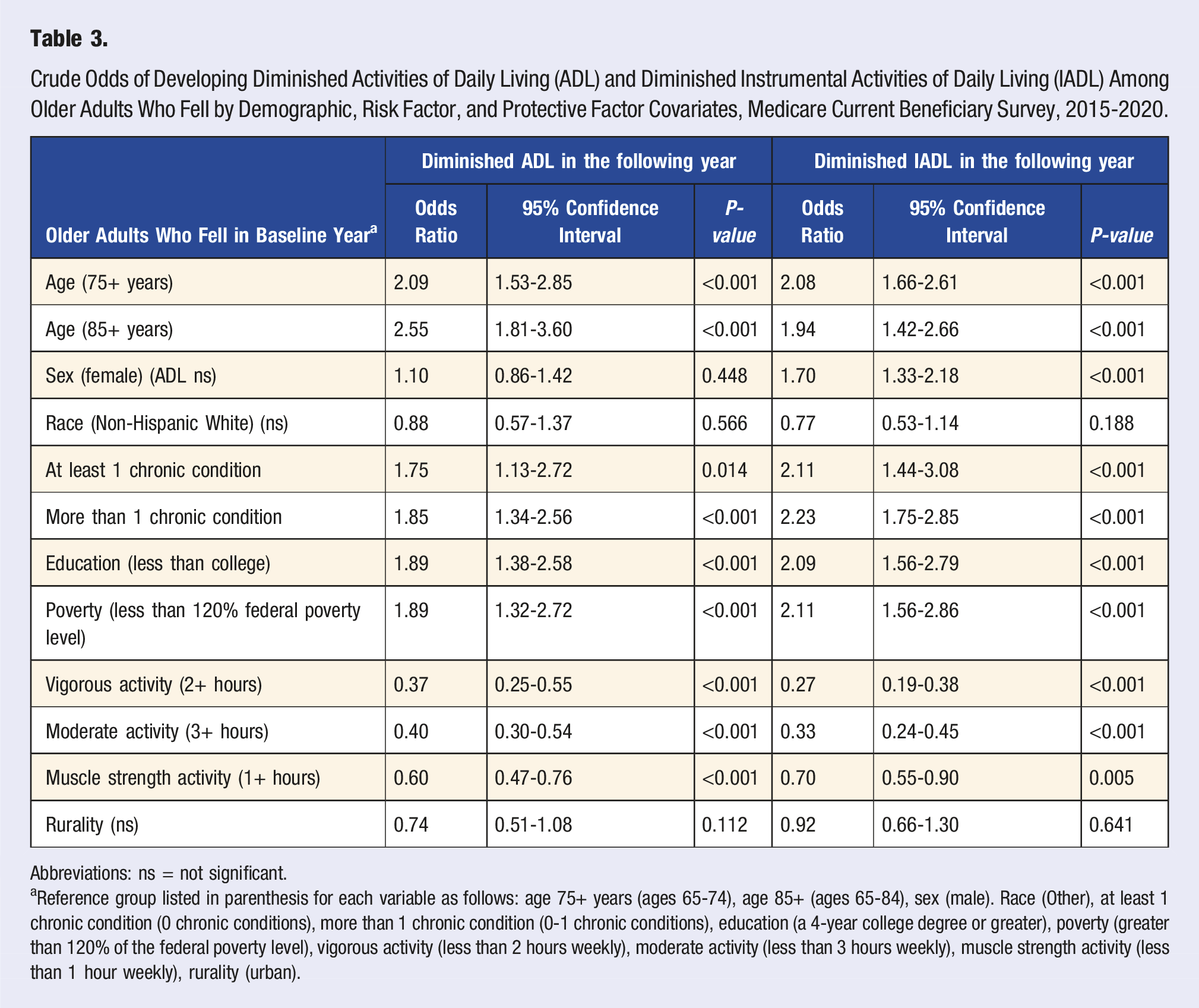
Abbreviations: ns = not significant.
aReference group listed in parenthesis for each variable as follows: age 75+ years (ages 65-74), age 85+ (ages 65-84), sex (male). Race (Other), at least 1 chronic condition (0 chronic conditions), more than 1 chronic condition (0-1 chronic conditions), education (a 4-year college degree or greater), poverty (greater than 120% of the federal poverty level), vigorous activity (less than 2 hours weekly), moderate activity (less than 3 hours weekly), muscle strength activity (less than 1 hour weekly), rurality (urban).
Adjusted Odds of Developing Diminished Activities of Daily Living and Diminished Instrumental Activities of Daily Living Among Fallers by Demographic, Risk Factor, and Protective Factor Covariates, Medicare Current Beneficiary Survey, 2015-2020.
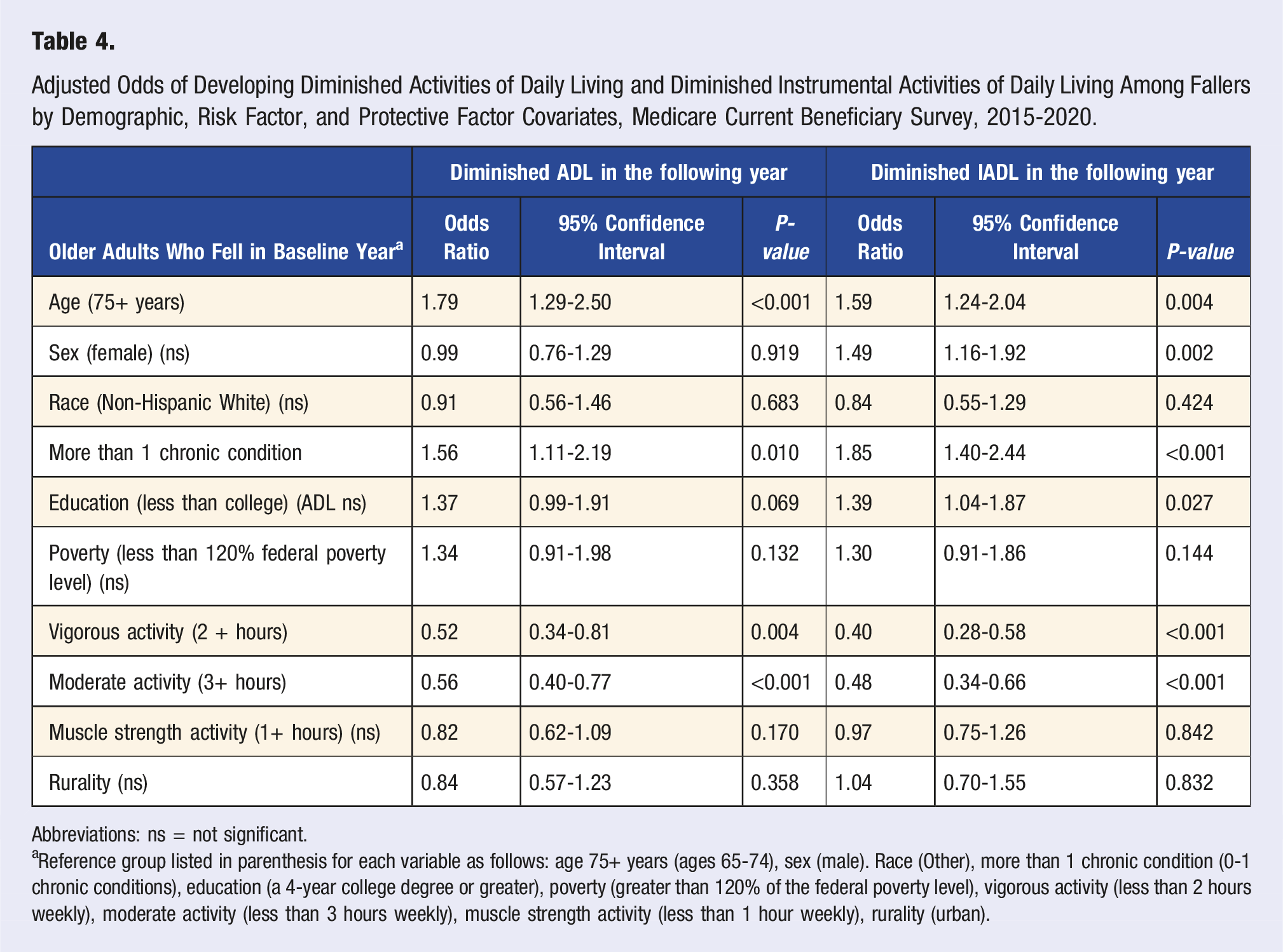
Abbreviations: ns = not significant.
aReference group listed in parenthesis for each variable as follows: age 75+ years (ages 65-74), sex (male). Race (Other), more than 1 chronic condition (0-1 chronic conditions), education (a 4-year college degree or greater), poverty (greater than 120% of the federal poverty level), vigorous activity (less than 2 hours weekly), moderate activity (less than 3 hours weekly), muscle strength activity (less than 1 hour weekly), rurality (urban).
Discussion
Our results show that among older adults with no prior ADL or IADL limitations, those who fell had higher odds of developing an ADL or IADL limitation in the next year than those who did not fall. This relationship persisted even after adjusting for demographic, risk, and protective factors. These findings support evidence in previous reports examining the effect of falls on developing functional limitations.10,12 Choi et al 10 found an increased odds of developing an ADL limitation after a fall in a study examining functionally independent adults aged 65-74 years. This effect increased with the number of falls and when the fall resulted in an injury requiring medical attention. Other studies reported clinically significant functional decline or high disability scores after a fall irrespective of the functional status before the fall.33,34
Among older adults who fell, those in the older age-groups (vs those in the younger age-groups) and older adults with 2 or more chronic conditions (vs those with 0-1 chronic conditions) had higher odds of developing functional limitations in the next year. The association between age and functional limitations persisted even after adjusting for comorbidities and other covariates and the association between comorbidities and functional limitations persisted after adjusting for age and other covariates. Age and comorbidities are common risk factors for falls and functional limitations. While age-related physical and physiological changes place an older adult at risk for falls 35 and developing functional limitations, 36 comorbidities in the presence of these changes increase the risk for both outcomes.35-37 With age, the number of comorbidities in an older adult increase 38 and so do the associated risks for falling 26 and developing functional limitations.36,39
Both ADL and IADL functioning is important to older adults as the autonomy provided by being able to care for oneself plays an important role in social engagement, physical and mental health and overall quality of life as one ages. 36 Therefore, developing performance limitations in such activities can impact multiple areas of an older adult’s life. One common consequence of having ADL or IADL limitations is increased falls risk. 40 Older adults with functional limitations may fall because of several reasons. First, gait, strength and balance, and cognitive limitations directly increase the risk of falling. 24 Second, developing these limitations may cause or worsen symptoms of anxiety or depression, increase social isolation and reduce physical activity level in an older adult;36,37 all of which, in turn, increase falls risk.41-43 Additionally, functional limitations may act as mediators between other known falls risk factors such as comorbidities, 44 and unsafe home environment (e.g., broken steps, lack of grab bars in toilets). 45 Older adults with a history of falls are at higher odds of falling again when compared with those without a history of falls. 14 Thus, the development of functional limitations after a fall may partly explain this phenomenon.
Falling and developing functional limitations, however, are not a natural part of aging; they can be prevented, or their progression slowed down. One common protective factor for both falls and developing functional limitations is physical activity.43,46 Regular, structured lower limb muscle-strengthening exercises and exercises improving balance are an effective fall-prevention strategy.46-49 Moderate intensity physical activity can prevent the onset or progression of ADLs, and physically active older adults have a lower risk of developing cognitive limitations. 47 The older adult physical activity guideline recommends multicomponent physical activity which includes aerobic, balance training, and muscle-strengthening activities.30,31 Our study found that older adults who regularly performed moderate (≥3 hours/week) or vigorous (≥2 hours/week) physical activity or muscle-strengthening activities (≥1 hour/week), had a protective effect from developing functional limitations after a fall. The recommended dose for adults with disabilities and chronic conditions (i.e., for those who are able to perform such activities) is similar to those of older adults.30,48 Further, bolstering physical activity with other fall-prevention strategies such as home modification (e.g., installing grab bars, repairing broken steps) could be beneficial as functional limitations were reported to mediate the relationship between home or environmental hazards and falls. 45 The CDC’s STEADI initiative (Stopping Elderly Accidents, Deaths and Injuries) https://www.cdc.gov/steadi/index.html) aims to help health care providers integrate fall prevention into clinical practice and educate older adults about how to reduce their risk of falls. A main component of STEADI is addressing gait, strength, and balance limitations with targeted exercises or physical therapy to reduce functional decline. The STEADI initiative represents a comprehensive approach to addressing older adult falls as a significant public health issue. By promoting early identification of fall risk factors and implementing evidence-based interventions, STEADI aims to reduce falls, fall injuries, and related complications.
While our findings reinforce the importance of the STEADI initiative, the increase in prevalence of fall-related morbidity and mortality among community-dwelling older adults 1 suggests that additional strategies beyond those targeted at the individual-level might be needed. 50 Strategies that modify the home to incorporate fall-prevention features such as non-slip flooring, adequate lighting, and walk in showers51,52 and polices that support expanding funding for home modification programs for the elderly 53 are examples of structural or environmental strategies for consideration. These strategies also address social determinants of health related to housing. A comprehensive approach incorporating both individual-level and structural or environmental level strategies can be essential to achieving meaningful reductions in falls among older adults.
The results of this study are subject to several limitations. First, MCBS data are self-reported and may be subject to recall bias, especially data on falls. Second, we did not assess for the number of ADL or IADL limitations in this analysis, so beneficiaries could have only 1 limitation or all 6 limitations and these potential differences were not accounted for in our models. Third, the questions about functional limitations do not assess for severity. Therefore, we could not determine if the risk or protective factors had a differential relationship to severity of functional limitations among older adults who fell. Fourth, physical activity is reported in minutes in MCBS and we rounded up to the nearest hour both for consistency with other variables in the dataset and to facilitate analysis. We recognize that this could have led to some respondents to exceed the guideline thresholds and acknowledge this as a potential source of misclassification bias. Fifth, as the fall-related question in MCBS inquires if a beneficiary fell anytime in the past 12 months, it was not possible to determine the date of the fall. Lacking the date of when the fall occurred limited our ability to assess the timing of falls relative to outcomes. While our analysis shows that associations can be examined, the temporal and causal relationship between falls and ADL or IADL limitations could not be determined without precise dates. Sixth, MCBS included only a binary indicator of whether a fall occurred (yes/no) in the main analysis sample; information on details related to the fall was available for a smaller subsample of those who reported a fall in the past 12 months; however, we did not perform sub analysis to determine severity of the fall. Follow-up fall data were not always complete or consistent so including the follow-up severity of the fall would greatly decrease the sample size. Therefore, our study objective was to examine overall associations between having experienced a fall (yes/no) and subsequent limitations in the broader sample, rather than to characterize fall severity or outcomes within the smaller subsample. Focusing on the binary fall variable allowed us to retain the full sample size and statistical power necessary for computing stable odds ratios. We acknowledge that follow-up data could provide valuable insights into severity and ADL or IADL limitations and is an area for future research. Last, our study dichotomized variables to facilitate interpretation and maintain statistical power; however, dichotomization may reduce sensitivity and oversimplify associations. By retaining some of the multi-category response values we might have been able to identify thresholds, improve statistical sensitivity, and more effectively control for confounding. Future research using the full range of available response categories may provide a deeper understanding of the relationships between falls and ADL/IADL limitations.
Conclusion
As the United States population ages, there is increasing awareness of the prevalence of older adult falls; however, falls among older adults are common but not inevitable. Falls pose a substantial burden on older adults and often result in functional decline, loss of independence, and increased risk of subsequent health challenges. Multifactorial strategies with special focus on gait, strength and balance exercises can serve as protective factors to reduce risk of falls or risk of developing limitations in ADLs/IADLs after a fall.
Supplemental Material
Supplemental Material - Risk of Diminished Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs) After an Older Adult Fall, Medicare Current Beneficiary Survey, 2015-2020
Supplemental Material for Risk of Diminished Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs) After an Older Adult Fall, Medicare Current Beneficiary Survey, 2015-2020 by Ketra Rice, Jufu Chen, Ramakrishna Kakara, and Yara K. Haddad in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
Conceptualization: KR, JC, RK, YH Investigation: KR, JC, RK, YH Data curation: KR, JC Formal analysis: KR, JC Methodology: KR, JC, RK Writing—original draft: KR, RK, YH Writing—review and editing: KR, JC, RK, YH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to required data use agreements to access data through the Centers for Medicare and Medicaid Services (CMS) Virtual Research Data Center (VRDC). Any SAS output tables generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.