
Abstract
Background:
Healthcare workers (HCWs) in lower- and middle-income countries (LMICs) face unique, intersectional threats to their mental health at work. Despite the existence of recommendations for multi-tiered interventions to promote and protect occupational mental health for HCWs, there remain significant challenges to implementation worldwide.
Methods:
FHI 360, a global development organization, developed a novel technical assistance framework to accompany partners, including government and healthcare leaders to design, implement, improve, or evaluate any mental health and psychosocial support intervention. The EpiC Project, implemented by FHI 360, has utilized this framework in four countries (Vietnam, Philippines, Paraguay and Sri Lanka) specifically to guide the development of locally adapted occupational mental health interventions for HCWs.
Findings:
Each country applied this framework in various project cycle phases and in their unique local contexts; all countries reported positive developments in the advancement of their chosen interventions.
Conclusions/Application to Practice:
With the application of an adaptable, evidence-based technical assistance framework to guide collaborative consultation for project design, implementation, improvement, and/or evaluation, locally led teams pivoted from a solely “mental health” approach to more comprehensive, evidence-based interventions that framed mental health for HCWs as an occupational health priority. This allowed for teams advising interventions in LMICs to consider unique workplace, structural and policy-level factors rather than focusing solely on individual mental health strategies.
Background
The World Health Organization (WHO) and the International Labor Organization (ILO) released a global report and policy brief in September 2022 with evidence-based recommendations and calls to action to address mental health at work. WHO and the ILO acknowledge that everyone has the right to work, and that both work and workplaces have the potential to enhance or undermine mental health for all people (World Health Organization [WHO], 2022). Occupational health and safety (OHS) for healthcare workers (HCWs) in lower- and middle-income countries (LMICs) is a uniquely challenging issue that goes far beyond workers’ rights. Unmitigated burnout and psychological distress can lead to medical errors and compromised patient safety (Dewa et al., 2017) as well as increased absenteeism, turnover, attrition, and migration (Buchan et al., 2022). Inadequate OHS for HCWs affects the capacity of health systems, the quality and safety of patient care, and the economic stability of resource-constrained environments. This professional practice update describes how innovative, high-quality technical assistance can inform evidence-based, sustainable, and locally led interventions to effectively address the complex challenges of occupational mental health for HCWs in LMICs. Individual or workplace/team-based programs implemented without commitment to higher level structural and policy changes pose both programmatic and ethical concerns.
Concerns for widespread burnout, moral injury, and rising rates of mental health conditions like depression, anxiety, and insomnia among HCWs are rising in step with the growing recognition of pandemic-related mental health conditions (Santomauro et al., 2021). Several studies have reported a high prevalence of these conditions among HCWs in LMICs (Dagget et al., 2016), who often face disproportionately high workloads, long hours, unstable or insufficient remuneration, and limited healthcare resources. These factors directly correlate to increased rates of stress and burnout as well as occupational hazards (WHO, 2019). There is ample evidence from the COVID-19 pandemic, as well as prior outbreaks of infectious diseases, demonstrating the impact of occupational threats to psychological well-being (Kisely et al., 2020), and several studies have described that work-related threats to physical health and safety may exacerbate psychological distress (Billings et al., 2021). While evidence-based interventions that have been employed, such as mental health awareness programs, peer support, and access to counseling services, demonstrate an impact on mental health scores, their evaluation has been limited, and the interventions themselves have not been well described (Robins-Browne et al., 2022; Wykes et al., 2021). Furthermore, the majority of research investigating interventions to protect the mental health of frontline health workers occurred in high-income countries, potentially diluting the additional complex social, economic, and environmental factors affecting psychological health among HCWs in LMICs.
Yet, documentation of the complex OHS dynamics facing HCWs in LMICs has not resulted in significant progress in evidence-based occupational mental health interventions (Ndejjo et al., 2015). While several calls to action in the postpandemic rhetoric have aimed to bring the health and well-being of the healthcare workforce closer to the top of agendas, the issue (and subsequent interventions) have largely remained framed around mental health diagnoses of individual HCWs rather than presented as a comprehensive (and admittedly complex) OHS mandate. Structural changes at the policy level, including improving working conditions, providing adequate rest periods, and addressing chronic staff shortages, are essential to address mental health concerns among healthcare workers in LMICs. Individual or workplace/team-based programs implemented without commitment to higher level structural and policy changes pose both programmatic and ethical concerns. Research and advocacy efforts are needed to highlight the importance of mental health for healthcare workers in LMICs and to drive policy changes and resource allocation (Søvold et al., 2021). There are clear recommendations from multiple international health agencies promoting multi-tiered strategies to protect and support mental health at work; the most effective interventions simultaneously target individual, interpersonal, organizational, and structural factors, including policy environments through the lens of World Bank, 2018; Center for Health Worker Innovation [CHWI], 2021; Hoover et al., 2023; WHO, 2022).
FHI 360 is a global development organization that supports health, education, and livelihood programs in partnership with governments and partners in over 60 countries worldwide. With a growing interest in high-quality mental health and psychosocial support (MHPSS) for the general population, as well as the amplification of impact when MHPSS approaches are integrated into routine health services, education, and livelihood programs, FHI 360 has recognized the importance of planning for the psychological safety and well-being of those rendering care services across multiple LMIC country programs (including, but not limited to, clinical and social service delivery). Therefore, with the release of a novel technical assistance tool aiming to improve the quality and efficacy of MHPSS programming in LMIC settings agnostic of target population, FHI 360 frames mental health of all providers of care services—including HCWs—as an OHS issue that must be addressed in any global development program. FHI 360 also recognizes that the mental health of care providers is pivotal to the provision of high-quality care and achievement of sustainable, high-impact results. As such, FHI 360 has sought and received funding to improve occupational mental health for care providers through a variety of technical assistance packages tailored to meet the context, government and donor priorities, and available funding. Since 2022, the activities in each country presented in this professional practice update have evolved from interventions that primarily focus on individual factors to interventions that simultaneously advocate for individual supports, workplace factors, and structural and policy factors. With the application of an adaptable, evidence-based model to guide collaborative consultation for technical assistance, teams pivoted from solely “mental health” approaches to more comprehensive, evidence-based interventions that framed mental health for HCWs as an OHS issue.
Methods
The Meeting Targets and Maintaining Epidemic Control (EpiC) project is an 8-year (2019–2027) global initiative, funded by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and the U.S. Agency for International Development (USAID), that provides strategic technical assistance and direct service delivery to achieve control of the HIV epidemic among key and priority populations, respond to the COVID-19 pandemic, and strengthen global health security Since December 2021, EpiC project teams in Paraguay, the Philippines, Sri Lanka, and Vietnam have worked to design, implement, and scale up programs to promote improved models of occupational mental health for HCWs. In response to requests from national governments, funding allocations by international donors, and a groundswell of urgency to address mental health challenges among health workforces globally in the context of the pandemic, technical experts at FHI 360 aimed to develop an evidence-based, adaptable framework for technical assistance in this area entitled The 8Cs Model of Collaborative Consultation for Mental Health and Psychosocial Support Programs (Kohrt et al., 2023). This section will describe the methods and approaches each country team applied to work closely with local governments and health authorities to respond to requests for technical assistance related to occupational mental health for HCWs that emerged in the context of the COVID-19 pandemic.
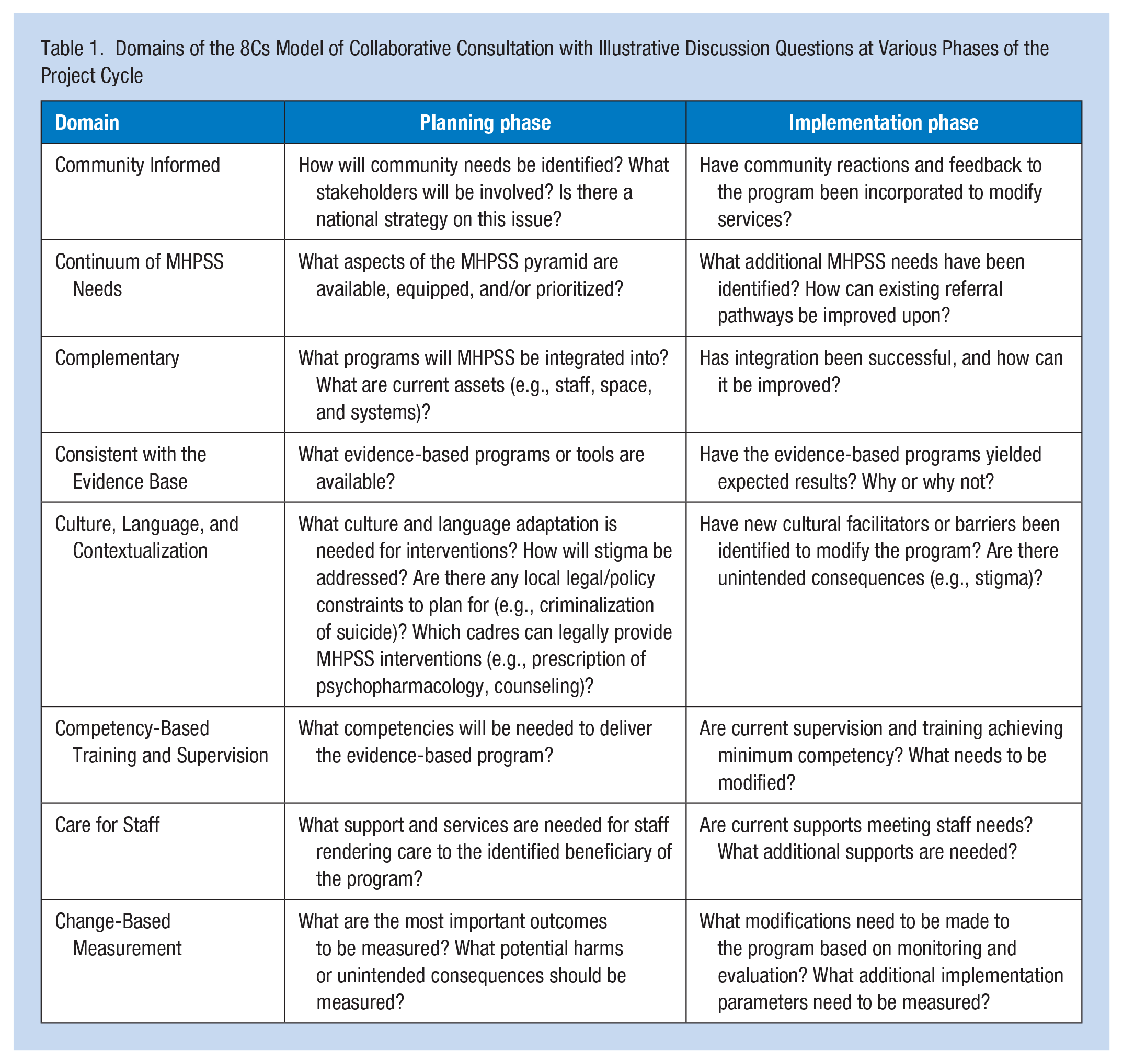
Using this novel technical assistance framework, several country teams within the global EpiC portfolio have designed high-quality technical assistance packages to support the integration of MHPSS services into health programs. As of October 2023, the 8Cs Model has been piloted in nine countries to inform MHPSS programming, primarily for HIV and COVID-19 response programs supported by FHI 360. The 8Cs Model includes eight domains that should be considered when planning integrated MHPSS interventions (Table 1). The 8Cs Model is unique in that it is designed to be applied irrespective of geographic area, target beneficiary population, phase of project cycle, and level of funding. The seventh domain is “Care for Staff,” which offers clear, evidence-based guidance and recommendations to plan for individual, workplace, and policy factors that protect the OHS of those rendering the service.
Domains of the 8Cs Model of Collaborative Consultation with Illustrative Discussion Questions at Various Phases of the Project Cycle
While country programs that have applied the 8Cs Model have, by default, considered components of staff care and well-being, Paraguay, the Philippines, Sri Lanka, and Vietnam used the 8Cs Model to design, improve, and/or evaluate programs to address occupational mental health and psychological well-being among HCWs. This process was implemented differently in each setting, in the context of local project phases and needs, and was often applied cyclically, with multiple consultations accruing throughout the project life cycle to inform, improve, or redirect specific components of these projects.
Philippines
Since 2021, the EpiC project has support 82 public hospitals across the Philippines in their COVID-19 response. One of its key programmatic areas is promoting mental health resilience and preventing burnout among HCWs using evidence-based, practical approaches that are adapted to the local context. In a rapid survey conducted by EpiC in January 2022, of the 27 hospitals that completed the survey, 80% introduced interventions to address mental health, wellness, and burnout among HCWs, and 90% of the respondents agreed that HCW burnout affects patient care, but only 60% screened HCWs for signs of poor mental health.
EpiC collaborated with key stakeholders, such as government bodies and professional societies, to synergize efforts and complement activities providing a more holistic and integrated approach to mental health programming specific to the health workforce. EpiC facilitated three communities of practice (COP) webinar events focused on HCWs’ mental health with over 1,200 participants and with topics ranging from compassion fatigue to existing MHPSS interventions for HCWs. The project integrated stress management sessions into hospital visits and trainings on clinical case management, orienting over 500 hospital staff, and developed a mental health training course about “caring for carers,” which aims to equip HCWs with the knowledge, skills, and behaviors to foster healthier mental health practices while they continue to ensure the public’s health and well-being during the COVID‑19 pandemic. During the pilot training, EpiC trained over 90 HCWs from more than 40 hospitals across the country who have developed mental health action plans for their facilities’ own staff and clients. EpiC identified two provincial hospitals in the southern Philippines to receive a technical assistance package to establish a wellness room dedicated to their hospital employees. To maximize and sustain this safe space, EpiC helped these hospitals create their own mental health resilience teams that will manage their hospital wellness program for both medical and non-medical staff.
Sri Lanka
From early in the pandemic, the Sri Lankan Ministry of Health was committed to implementing programs to build resilience and address burnout among multiple cadres of HCWs as part of a comprehensive COVID-19 response plan supported by EpiC. The already limited workforce, with 2.12 nurses per 1,000 population and 0.92 doctors per 1,000 population (Medical Statistics Unit, Ministry of Health, Nutrition and Indigenous Medicine, 2017) faced frustration with the inability to provide optimal services to patients, with the added burden of stock-outs of medication, supplies, and PPE; and concurrent social, economic, and political unrest that severely strained already exhausted resources amid an active pandemic. COVID-19-related stigma against HCWs and their families was rampant, and many HCWs reported rejections from their neighboring communities added to their psychological distress.
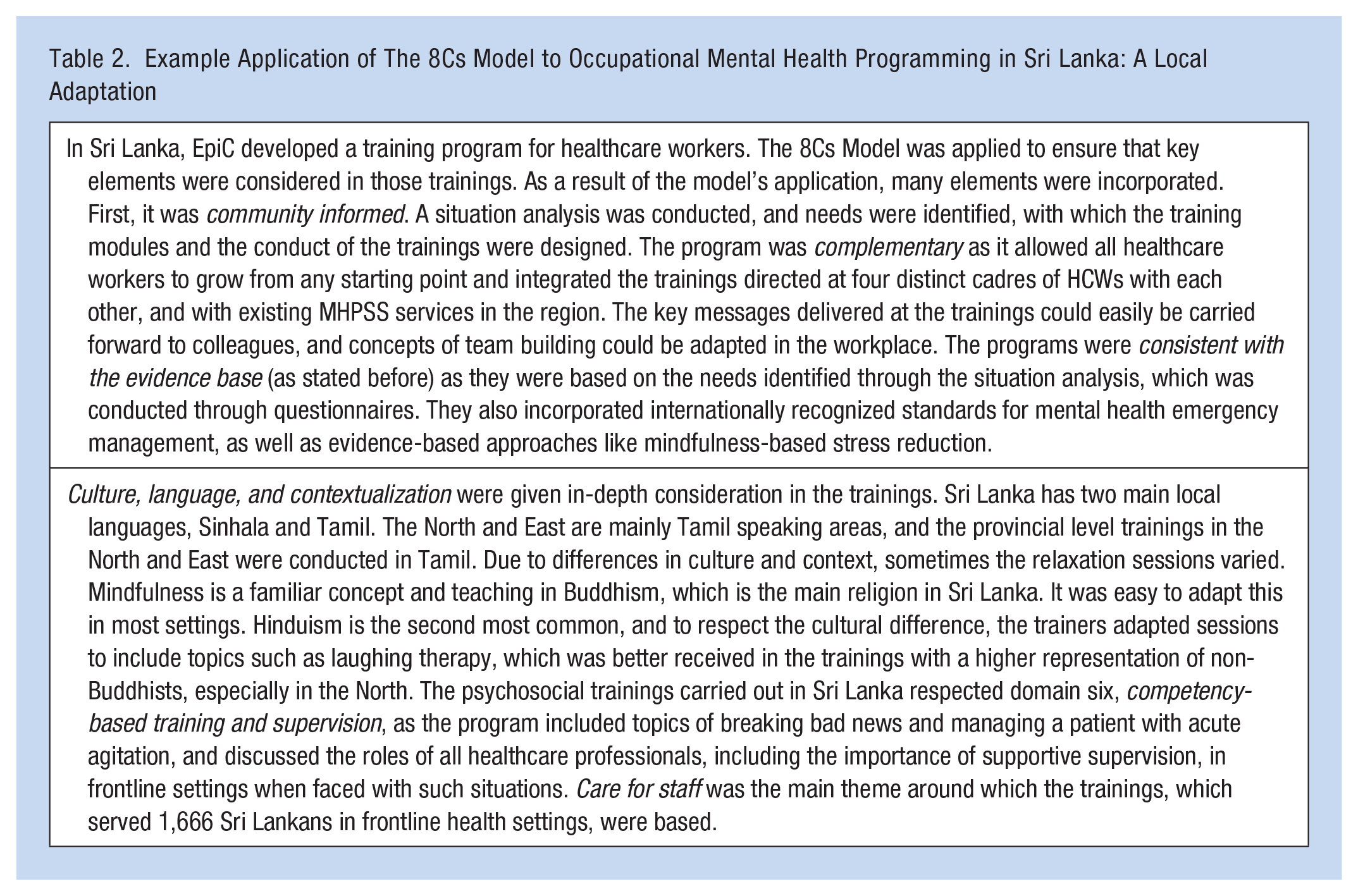
EpiC partnered with the Sri Lanka College of Psychiatrists to conduct a rapid needs analysis among frontline HCWs that directly informed the design of a comprehensive MHPSS training package. The approach was unique in that it was designed to apply a cascade training model to increase capacity for multiple cadres of frontline workers (clinicians, mental health professionals, ambulance drivers, and staff of a newly established national mental health hotline) to render improved MHPSS care to patients and clients in the community while simultaneously integrating principles of staff well-being, self-care, and peer support throughout the modules. The training programs conducted in Sri Lanka covered many domains discussed in the 8Cs Model (Table 2). While the 8Cs Model was developed after most of the training manuals were finalized, it served as an important tool in the development and continuity of training programs and as a checklist to ensure that most aspects were considered in the intervention.
Example Application of The 8Cs Model to Occupational Mental Health Programming in Sri Lanka: A Local Adaptation
Vietnam
USAID/Vietnam and the EpiC project recognized that any program designed to improve COVID-19 clinical care had to consider the needs of HCWs as the backbone for providing quality health services to patients and families in Vietnam. In early 2021, Vietnamese HCWs were feeling the pressure, pain, and fatigue of a prolonged stressful work environment due to COVID-19. Even before infections spiked in May 2021, the national COVID-19 response strategy mandated that many Vietnamese HCWs work extra shifts to cover quarantine facilities while remaining isolated from their families and communities for extended periods of time as an infection prevention and control measure. In the face of intense workplace pressure coupled with fear of infection, many HCWs left the bedside. Those who remained struggled to manage their growing workload due to staff shortages. Postpandemic reviews showed that although COVID-19 drew attention to this issue, the mental health impacts of stress, burnout and vicarious trauma had been an unspoken issue among the healthcare workforce for some time. There was little professional or occupational MHPSS support available for HCWs, high levels of stigma, and insufficient awareness of the importance of mental healthcare. In the wake of the COVID-19 pandemic, it was evident that MHPSS services for HCWs needed to be integrated into long-term OHS strategies.
Subsequently, EpiC Vietnam developed an integrated mental health support package to complement clinical case management and infection prevention and control trainings during the COVID-19 response. In recognition of the need to expand and improve institutional occupational MHPSS health support, the Ho Chi Minh City (HCMC) Department of Health requested that FHI 360 identify additional financial resources to help them implement a strategy to address the long-term occupational mental health needs of the healthcare workforce.
Paraguay
The EpiC project has supported the Government of Paraguay in its response to the COVID-19 pandemic since the early stages of the public health emergency, mostly focusing on strengthening the oxygen ecosystem and providing clinical trainings on topics related to COVID-19 for the primary healthcare workforce. A series of virtual and in-person clinical training events were conducted between April 2022 and April 2023, reaching over 150 physicians, nurses, and healthcare leaders from three regions in Paraguay. Each participant completed a basic training evaluation, which provided 10 options for future training sessions on topics such as medical oxygen therapy, COVID-19 vaccine information, long COVID, and mental health. The mental health and well-being of HCWs was the top request for each session evaluation; mental health and well-being for the general patient population was the second most common request in all session evaluations. While the literature on mental health among HCWs in Paraguay is limited, initial evidence suggests relatively high rates of burnout, posttraumatic stress disorder (PTSD), depression, and anxiety symptoms among this population (Villalba-Arias et al., 2020; Villalba-Arias, et al., 2023; Torales et al., 2022).
In March 2023, EpiC presented these results to counterparts in the Mental Health Division of the Paraguayan Ministry of Health (MOH) to discuss ongoing activities in this area. MOH officials shared that mental health for HCWs is a concern, but there was little confidence and virtually no national mental health budget to address this issue. The MOH requested EpiC’s support to conduct a rapid assessment of the experiences of primary HCWs with work-related stress and burnout. With 88% of respondents reporting that their mental health had been negatively affected by work-related stress in the prior six months, and 93% reporting that they would use or participate in MHPSS resources from their employer, the Paraguayan MOH committed to advancing workplace well-being as a national priority. With TA and support from EpiC, key stakeholders from central government, professional associations, academia, and facility-based leadership will engage in a series of educational and strategic road mapping workshops to envision a national approach and facility-based pilot interventions based on TA provided through the lens of the 8Cs Model. These workshops are scheduled to occur between October and November of 2023, with ongoing support planned through early 2024.
Each country worked with governments and key stakeholders in different ways. In some cases, project staff encouraged ministries to address the mental health needs of HCWs, and in others, governments reached out to project staff for support. Each country had a different set of needs and limitations. Using approaches designed to be adaptable to local contexts, each team was able to tailor evidence-based, sustainable, and locally led interventions to their own needs.
Results
These country-specific experiences demonstrated locally led approaches to providing high-quality technical assistance, fostering strong governmental partnerships, and applying comprehensive, evidence-based approaches to mental health for HCWs as an OHS priority. While qualitative, quantitative, and programmatic data are still being collected and analyzed, there were several key trends emerging from the cross-cultural comparative analysis of these programs. They are summarized as follows:
Improved Confidence and Competence of Government Partners Is Both Feasible and Essential
Work-related mental health issues—and the effects of poor mental health on work—are recognized concerns among healthcare leaders and national governments. In all four countries, government bodies either requested or accepted direct technical assistance from FHI 360/EpiC in this area. They all reported low confidence in the ability to create forward momentum in this area, particularly as all four countries historically maintained very low national budgets for MHPSS services. When high-quality technical assistance was presented in the context of strong, trusting partnerships between FHI 360, national governments, and local experts—and particularly with the reframing of MH for HCWs as a multi-tiered OHS issue rather than solely an MHPSS issue—progress was made toward envisioning a feasible approach to occupational mental health.
Adaptation of Multitiered Interventions Is Beneficial and Encouraged
All psychoeducation and training activities, while locally adapted and delivered in various modalities, incorporated similar concepts, particularly concepts of self-care, self-compassion, and compassion for colleagues. After applying the 8Cs Model as part of the technical assistance efforts, all four countries’ training approaches emphasized the importance of comprehensive, complementary interventions that promote individual factors (i.e., for individual HCWs) in conjunction with workplace factors (i.e., for facility- or regional-level managers and leaders) and structural and policy factors (i.e., ministries of health, policymakers, professional associations, and other advocacy efforts around OHS).
All Country Teams Reported Positive Experiences Applying the 8Cs Model of Collaborative Consultation to Their Programs, Irrespective of Phase of Program Cycle
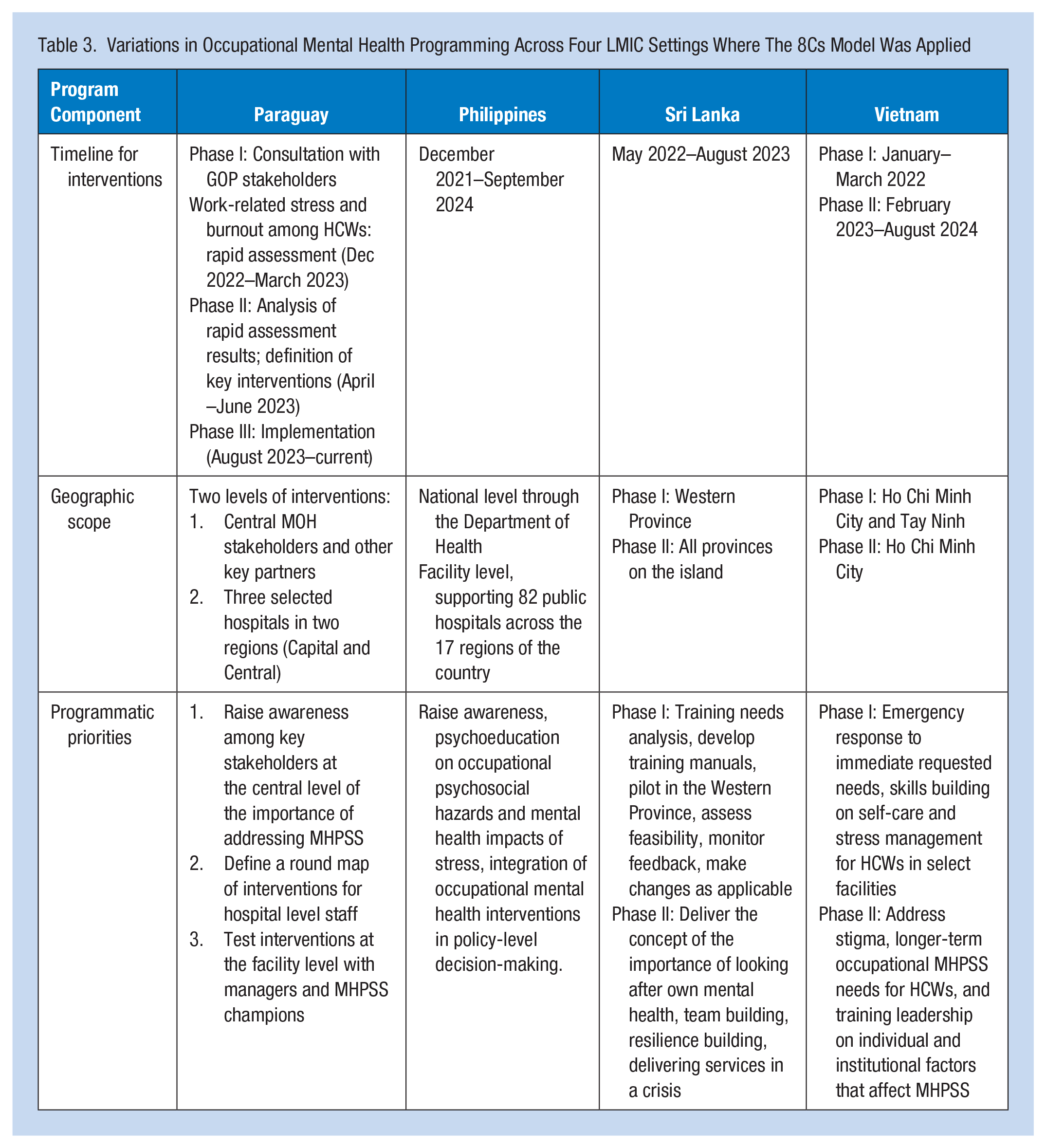
All four country teams reported ease of application of the 8Cs Model despite having highly variable program designs and being at relatively different phases of their program cycle (i.e., design, mid-implementation, or postimplementation review phases) (Table 3). The Philippines, uniquely, utilized the 8Cs Model of Collaborative Consultation directly with local health facility leaders to critically analyze, prioritize, and plan key components of their interventions. Local teams reported that the availability of this technical assistance approach promoted buy-in and support for several key policy changes and OHS advances intended to codify mental health for HCWs as an essential deliverable in the national OHS standards.
Variations in Occupational Mental Health Programming Across Four LMIC Settings Where The 8Cs Model Was Applied
Comprehensive Technical Assistance to Improve Occupational Mental Health Must Also Incorporate Operational Support
While high-quality technical approaches improved buy-in, confidence, and perception of feasibility among local partners, there remained significant barriers to rapid implementation of broad structural and policy changes. Comprehensive technical assistance for occupational mental health for HCWs requires dedicated support for budgeting, finance, and strategic human resources for health strategy and policy negotiation.
Government Commitment in Continued Support for HCWs Is Key for Sustainability
Programs have received positive feedback from the governments in all four countries. In Paraguay, the EpiC project has been invited to provide direct TA to the MOH to develop a roadmap for occupational mental health for HCWs. In the Philippines, the team is engaging with government for ongoing technical assistance and support to shore up an occupational mental health strategy, advocating for dedicated budget lines for mental health resources (i.e., staff psychologists in healthcare facilities), and developing sustainability plans for mental health resilience teams. In Sri Lanka, trainers from the Sri Lanka College of Psychiatrists and the MOH plan to reproduce and widely disseminate the trainings developed by the EpiC team. In Vietnam, EpiC will continue its mental health work in the current fiscal year in close partnership with national and district government leaders.
Discussion
This professional practice update shares four unique examples featuring the role of high-quality technical assistance in the global health and development sector to design, implement, and improve occupational mental health approaches for HCWs in LMIC settings. There were several constraints to design, implementation, and options for analysis given the programmatic and donor requirements and the aim of aligning with national government priorities. This work was also conducted amid an unprecedented global pandemic, and often amid concurrent local emergencies and civil unrest. These examples would be strengthened with more rigorous data collection and analysis, particularly related to costing of interventions and potential economic implications of investing in occupational mental health among HCWs in LMICs. To our knowledge, there are no existing monitoring and evaluation (M&E) frameworks that can be applied across cultural settings amid any combination of global or local crisis scenarios that can parse the nuances of rigorous evaluation for the multiple intersectional factors, including OHS factors, influencing mental health, well-being, performance, and outcomes among HCWs in LMICs. Developing such M&E frameworks while in the middle of emergency response programming is extremely challenging and leaves us with suboptimal data to analyze. More research and advocacy efforts, as well as a strong and comprehensive M&E framework, are needed to highlight the importance of mental health for HCWs in LMICs and to drive policy changes and resource allocation. More implementation science and more rigorous retrospective research is needed to measure impact and efficacy of interventions, evaluate fidelity when interventions are adapted to local settings in the face of paltry resources for culturally adapted MHPSS materials, and measure economic implications for occupational mental health programs.
The mental health and psychological safety of HCWs in LMICs is not only an ethical and compassionate necessity for individual well-being; it directly affects the quality of healthcare services rendered and therefore the functional capacity of a national health system. Promoting a universal culture of safety—for patients and staff alike—may even be bidirectionally conducive to both goals (Lu et al., 2022). Protecting and promoting occupational mental health in healthcare settings involves many of the same investments required for protecting physical health and safety. They include comprehensive strategies that focus on fostering supportive work environments, providing access to a diverse range of physical and mental health resources, and implementing robust policies and procedures that govern the conditions of labor. This also includes strategic investment in the health sector, particularly at the primary healthcare level, and adopting adequate and agile national finance strategies that treat the health sector—and the workforce that it depends on—as a quantifiable asset rather than a sunk cost. Mental health for HCWs may be an issue that requires less expertise in mental health or psychiatry and requires more commitment to structural changes in health policy, health financing and HRH management. These transitions to a more enabling policy environment should leverage existing OHS mechanisms to protect and promote HCW mental health.
The experiences and results from four distinctly different countries, cultures, programs, and approaches demonstrate that, with the availability of high-quality technical assistance to reframe MH for HCWs as an essential OHS priority in the workplace, enormous progress can be made. This represents an accompaniment model that acknowledges the many daunting challenges required to support HCWs sustainably and comprehensively in LMICs. These many challenges—originating both within and beyond the workplace—have profound impacts on the psychological well-being of the healthcare workforce.
Investments in the structural, organizational, and interpersonal integrity of the health system can have a compounding positive impact on multiple outcomes, including the comprehensive health and well-being of both HCWs and patients alike. Physical health and safety are inextricably linked to psychological health and safety. HCWs deserve and require robust protections for both while in the workplace. Expert advocacy matched with evidence-based, compassionate, and comprehensive technical assistance can accompany health systems to identify, at minimum, “one step forward” toward the goal of essential health, safety, well-being, and efficacy of the individuals that comprise the healthcare workforce.
Applications to Professional Practice
Healthcare workers in LMIC settings face numerous complex intersectional stressors in their occupations that place their physical and mental health at risk, particularly in the context of emergencies such as the COVID-19 pandemic. Reframing concerns for mental health of HCWs into a more comprehensive approach to mental health as an occupational health and safety issue presents opportunities to make significant progress in this health area while working within the constraints of LMIC settings. High-quality, evidence-based tools like The 8Cs Model for Collaborative Consultation can support occupational health nurse leaders to envision, develop, and implement comprehensive yet contextually appropriate strategies that incorporate financing, policy and structural changes with individual and workplace interventions to protect and promote occupational mental health for their teams.
Footnotes
Acknowledgements
The authors thank the invaluable contributions of their teams at FHI 360, the EpiC Project, and local healthcare partners.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was prepared without dedicated external funding, though the programmatic work described therein was funded in part by the United States Agency for International Development (USAID).
Human Subjects Review
This professional practice update reflects work that was not subject to human subjects review.