
Abstract
This study investigated the impact of working for public versus private ambulance services in Turkey and elaborated on predictors of mental, physical, and emotional well-being in emergency medical technicians (EMT-Bs). In this observational cross-sectional study, an 81-question self-report survey was used to gather data about employee demographics, socioeconomic status, educational background, working conditions, and occupational health and workplace safety (OHS), followed by the 12-item General Health Questionnaire (GHQ-12), the Work-Related Strain Inventory (WRSI), and the Maslach Burnout Inventory (MBI) with three subscales: Emotional Exhaustion (MBI-EE), Depersonalization (MBI-DP), and Diminished Personal Accomplishment (MBI-PA). In 2011, 1,038 EMT-Bs worked for publicly operated and 483 EMT-Bs worked for privately owned ambulance services in Istanbul, Turkey, of which 606 (58.4%) and 236 (48.9%) participated in the study (overall participation rate = 55.4%), respectively. On all scales, differences between total mean scores in both sectors were statistically insignificant (p > .05). In the public sector, work locations, false accusations, occupational injuries and diseases, work-related permanent disabilities, and organizational support were found to significantly influence self-reported perceptions of well-being (p < .05). In the private sector, commute time to and from work (p < .05), false accusations (p < .05), vocational training and education (p < .05), informed career choices (p < .05), and work-related permanent disabilities (p < .05) were found to significantly influence self-reported perceptions of well-being. EMT-Bs were asked about aspects of their working lives that need improvement; priority expectations in the public and private sectors were higher earnings (17.5%; 16.7%) and better social opportunities (17.4%; 16.8%). Working conditions, vocational training, and OHS emerged as topics that merit priority attention.
Keywords
The recent decade represents an especially dynamic era in terms of health policy for Turkish public services. The Ministry of Health (MoH) launched a health care reform initiative in 2003; the Health Transformation Program (HTP) aimed to restructure MoH’s role from “provider of services” to “policy-maker and regulator” (World Bank Group [WB], 2013). Opponents from professional organizations, the media, and the general public contend that this change in fact is the “privatization” of public health services; the government now promotes market-based strategies in parallel with global priorities, posing substantial risks to the public (Turkish Medical Association, 2011). Market-oriented health care reforms promoted by the WB have long been criticized by researchers, experts, and social defenders throughout the world (Homedes & Ugalde, 2005; Lister, 2005). Ambulance services are currently operated by both public and private providers in Turkey. With general oversight of system operations, the MoH is responsible for the stewardship, governance, and regulation of both public and private services. Should pre-hospital emergency care (PHEC) be public, private, or a mix in terms of funding and delivery? Studies that have assessed system benefits have failed to present convincing evidence to support either service provider model over the others (Dolphin, 1978; Homedes & Ugalde, 2005).
Emergency medical technician-basic (EMT-B) and paramedic (EMT-P) represent the two levels of certification recognized by the MoH. EMT-Bs are graduates of high school vocational programs; EMT-Ps earn associate degrees. In 2011, a total of 1,521 EMT-Bs and 258 EMT-Ps worked for ambulance services in Istanbul. Of this total, 1,038 EMT-Bs and 231 EMT-Ps worked for public services; 483 EMT-Bs and 27 EMT-Ps worked for private companies. Six administrative city regions have been defined by health planning applications. Of the total number of 250 ambulance stations, 159 were publicly and 91 were privately operated.
Approximately two decades after EMTs first practiced in the United States in the early 1970s, an inaugural EMT training program was launched in Turkey in 1993. Progressive public health policy has since evolved, and the field has expanded dramatically. Presently, working conditions for EMT-Bs in Turkey resemble practice in countries of the western hemisphere. As in most parts of the world, EMTs in Turkey work full time, including nights, weekends, and holidays, typically 24 hours on duty and 48 hours off duty working an average of 10 shifts a month. EMTs work for ambulance services in urban and rural settings; career opportunities are also available in hospitals. Studies have reported internationally that exposure to violence is a major issue in PHEC and that underreporting exacerbates the problem (Yilmaz, Dal, Yaylacı & Uyanık, 2015). The rate of growth in EMT employment is expected to exceed other careers; Emergency Medical Services (EMS) professionals appear driven and enthusiastic to bring EMS to the forefront of Turkish health care (Rinnert, Miller, & Ersel, 2008).
Istanbul, located in the heartland of Turkey’s economic, cultural, and historical identity, is a large and densely populated transcontinental city in Eurasia. In 2013, population per station was 37,002 residents compared with 74,139 per station in Istanbul; population per public emergency care ambulance in Turkey was 22,838 compared with 52,253 in Istanbul (Basara, Guler, Yentur, Birge, & Pulgat, 2014). From an international perspective, Turkey is geographically situated as a bridge between cultures, ideas, ethnicities, and religions. The applicability of the Turkish model to other developing countries has attracted the attention of policy-makers from around the world, especially from the African region. Primary care, EMS, and information systems are examples of recent successful transformations in services (Perekli, 2012; Rinnert et al., 2008). According to WHO, a salient feature of the HTP was the PHEC system expansion including establishment of a European-model emergency “112” system (Rinnert et al., 2008). Ambulance planes and helicopters were introduced to improve access and efficiency in urgent care. The World Health Organization reports the increase from 350,000 EMS calls per year in 2002 to 2,680,000 calls in 2011, several years after the implementation of the HTP, a positive health system performance indicator (WHO Regional Office for Europe, 2012). Apparently, the impact of these changing dynamics on EMS personnel’s work life and welfare raises health policy questions.
Occupational health and safety (OHS) continue to be issues in ambulance services. Increasing evidence suggests that ambulance workers experience more health problems than the general working population and other groups of health care workers (Sterud, Ekeberg, & Hem, 2006). Frontline ambulance personnel are highly vulnerable to critical incident stress, which manifests as a wide range of physical and mental health problems (Gallagher, & McGilloway, 2007; Neely & Spitzer, 1997). Work-related stressors such as the work environment, job conditions, cognitive demands, and lack of support from colleagues and supervisors pose significant risks to mental health (Aasa, Brulin, Angquist, & Barnekow-Bergkvist, 2005; Revicki & Gershon, 1996; van der Ploeg & Kleber, 2003). Excess prevalence of psychological distress and burnout have been reported among ambulance workers (Alexander, 2001; Bennett, 2004; van der Ploeg & Kleber, 2003). Infectious risks from needlestick injuries and other exposures to blood and body fluids (Rischitelli, Harris, Mccauley, Gershon, & Guidotti, 2001); work-related musculoskeletal disorders with frequent complaints of neck, shoulder, low back, and knee pain (Hogya & Ellis, 1990; Maguire, Hunting, Guidotti, & Smith, 2005; Okada, Ishii, Nakata, & Nakayama, 2005); injuries from assaults; and physical and verbal acts of violence are sources of threat to EMTs’ general well-being (Duchateau, Bajolet-Laplante, Chollet, Ricard-Hibon, & Marty, 2002; Mechem, Dickinson, Shofer, & Jaslow, 2002). Ambulance personnel have more physical health problems, such as hypertension, than the general population (Boreham, Gamble, Wallace, Cran, & Stevens, 1994). Register-based studies indicate that EMTs are at higher risk of permanent impairment and early retirement for health reasons than other health services staff, the main causes of disability being musculoskeletal, circulatory, and mental disorders (Rodgers, 1998a, 1998b). Reports also indicate relatively high numbers of occupational fatalities; mortality is most commonly associated with transportation accidents (Balarajan, 1989; Maguire, Hunting, Smith, & Levick, 2002). Job benefits (i.e., higher earnings, social amenities, better work environments, professional respectability, opportunities for career development, social conveniences such as day care, housing assistance, lodging, hobby and recreation centers, private day activities, events organizations, counseling services, professional support, and advocacy groups) may potentially contribute to the development of optimistic attitudes and psychosocial well-being.
At the critical juncture of national health care reform controversies, this study attempted to identify key health policy issues at the crossroads of EMS, reconstruction of the national health system, public interest versus privatization debates, mental health issues, and OHS regulations. This study is a thorough investigation of the impact of working for public versus private ambulance services and an elaboration on the predictors of mental, physical, and emotional well-being among EMT-Bs in Istanbul.
Method
This cross-sectional study used an 81-question, four-section self-report survey. In the “Organizational Culture/Climate, Global Occupational Health, Mental Health” section, study-specific questions assessed participant demographics (e.g., age; gender; duration of employment; marital status; appointment type; socioeconomic status such as income, need for additional financial support, number of household members, number of income-earning household members, and home ownership; educational background including graduation, current enrollment, vocational training and pre-licensure education, informed career choice, continuing education, and in-service training; working conditions including last and current place of employment, location of choice, work schedule, average monthly shifts, number of cases per shift, commute time, patient transportation problems, quality of guidance from the ambulance station or command control center, false accusations, and priority expectations; and occupational health and safety including perceived safety at work, history of occupational injuries and diseases, work-related permanent disabilities, organizational support, and disciplinary measures) followed by the 12-item General Health Questionnaire (GHQ-12), the Work-Related Strain Inventory (WRSI), and the Maslach Burnout Inventory (MBI; three subscales including Emotional Exhaustion [MBI-EE], Depersonalization [MBI-DP], and Diminished Personal Accomplishment [MBI-PA]). Study reports have shown the Turkish versions of the GHQ-12, WRSI, and MBI are valid and reliable instruments for health professionals (Aslan, Alparslan, Aslan, Kesepara, & Unal, 1998; Aslan, Gurkan, Girginer, & Unal, 1996; Ergin, 1992; Kilic, 1996; Kilic et al., 1997). The Cronbach’s alpha coefficient for the GHQ-12 was .78, and for sensitivity and specificity was .74 and .84, respectively (Kilic, 1996; Kilic et al., 1997). The reliability of the Turkish version of the WRSI completed by health professionals was Cronbach’s alpha coefficient = .75 (Aslan et al., 1998; Aslan et al., 1996). The reliability of the Turkish version of MBI completed by health professionals was Cronbach’s alpha coefficient = .79; for subscales MBI-EE, MBI-DP, and MBI-PA, the coefficients were .89, .72, and .76, respectively (Ergin, 1992).
The Research Monitoring Committee officially approved the study on December 6, 2010, before data collection was initiated. All participants were informed of the objectives of the investigation and that participation was voluntary. For the limited population of 1,521 EMT-Bs in Istanbul (N), power analysis was conducted using Raosoft web survey software. For a confidence interval of 95%, a sample size of 307 EMT-Bs (n) was needed; for a confidence interval of 99%, a sample size of 463 EMT-Bs (n) was needed to achieve adequate power.
A pilot study was conducted with 17 participants from public and five participants from private ambulance services for a total of 22 EMT-Bs. Comprehensive in-depth interviews were conducted with EMS authorities, directors of ambulance services, and chiefs in charge of these operations. The prominent features of work life were emphasized by the officials and researchers gained insights into several issues. EMTs emphasized the problems faced in coordinating emergency response with other federal officers on the scene, identified obstacles to practice, and elaborated on topics including false accusations. EMS authorities drew attention to the inconveniences caused by non-emergency and prank calls to 112. EMTs indicated that assaults caused anxiety among EMS personnel threatening their practice, and expressed the importance of public health communication to prevent violence. The questionnaire design was tested and improved for efficiency. Following the pilot study, a minor typographical error was corrected and three survey questions were rephrased for clarification and elaboration purposes.
An official letter was disseminated to facilitate data collection. To reach the entire population of 1,521 EMT-Bs, surveys were distributed by official mail to all 159 public and 91 private ambulance stations. Prior to distribution, researchers informed 60 public and 91 private station officials about study procedures. Forms were distributed and collected by station officials and operators in charge of each station. Surveys were administered during a 3-month period, between February 8 and May 7, 2011.
Data were analyzed using SPSS Version 17.0. Means, standard deviations, frequencies, and percentages were calculated. For categorical variables, Chi-square and Fisher’s exact tests were used to compare frequencies between groups. To compare continuous variables, Student’s t test was used to examine mean differences between two groups, and one-way ANOVA was used to examine mean differences between more than two groups with normal distributions. In cases of statistically significant results between several groups, post hoc subgroup analyses were calculated (e.g., Tukey’s honest significant difference and the least significant difference tests). In conjunction with ANOVA, the Mann–Whitney U and the Kruskal–Wallis ANOVA non-parametric methodology was used when groups consisted of unequal sizes or variances were not sufficiently homogeneous. The level of significance was set at .05.
Results
Responses were received from 606 of 1,038 EMT-Bs (58.38%) working for public services and 236 of 483 EMT-Bs (48.86%) working for private services. Overall, 842 EMT-Bs participated in the study (55.36%), excluding ineligible responses from 40 participants. Exclusion criteria included invalid certificates, employment under 6 months, and essential data missing from survey forms (e.g., highest level of education: invalid certification indicated that two respondents were not EMT-Bs). Each survey was examined for completeness prior to entering responses. Responses were excluded from the data set if respondents answered less than one section of the survey or marked the same answer choice for virtually all questions. For reversely worded questions, “same answer replies” did not provide logically consistent responses and were excluded. Forms with excessive missing data were omitted from the study, inferring that participants had not given sufficient attention to the survey.
The differences between total mean scores and standard deviations on the GHQ-12, WRSI, and MBI from participants in the public and private sectors were not statistically significant (GHQ-12 p = .22; WRSI p = .19; MBI-EE p = .84; MBI-DP p = .62; MBI-PA p = .61). With respect to general health, work-related strain, and burnout, significant findings were found for three of the five categories assessed: educational background (i.e., vocational training and pre-licensure education, informed career choice), work conditions (i.e., current work location, commute time to and from work, false accusations), and OHS (i.e., history of job injuries or occupational diseases, work-related permanent disabilities, organizational support; p < .05, Tables 1 and 2).
Scale Comparisons in the Public Sector (M ± SD; p Value)
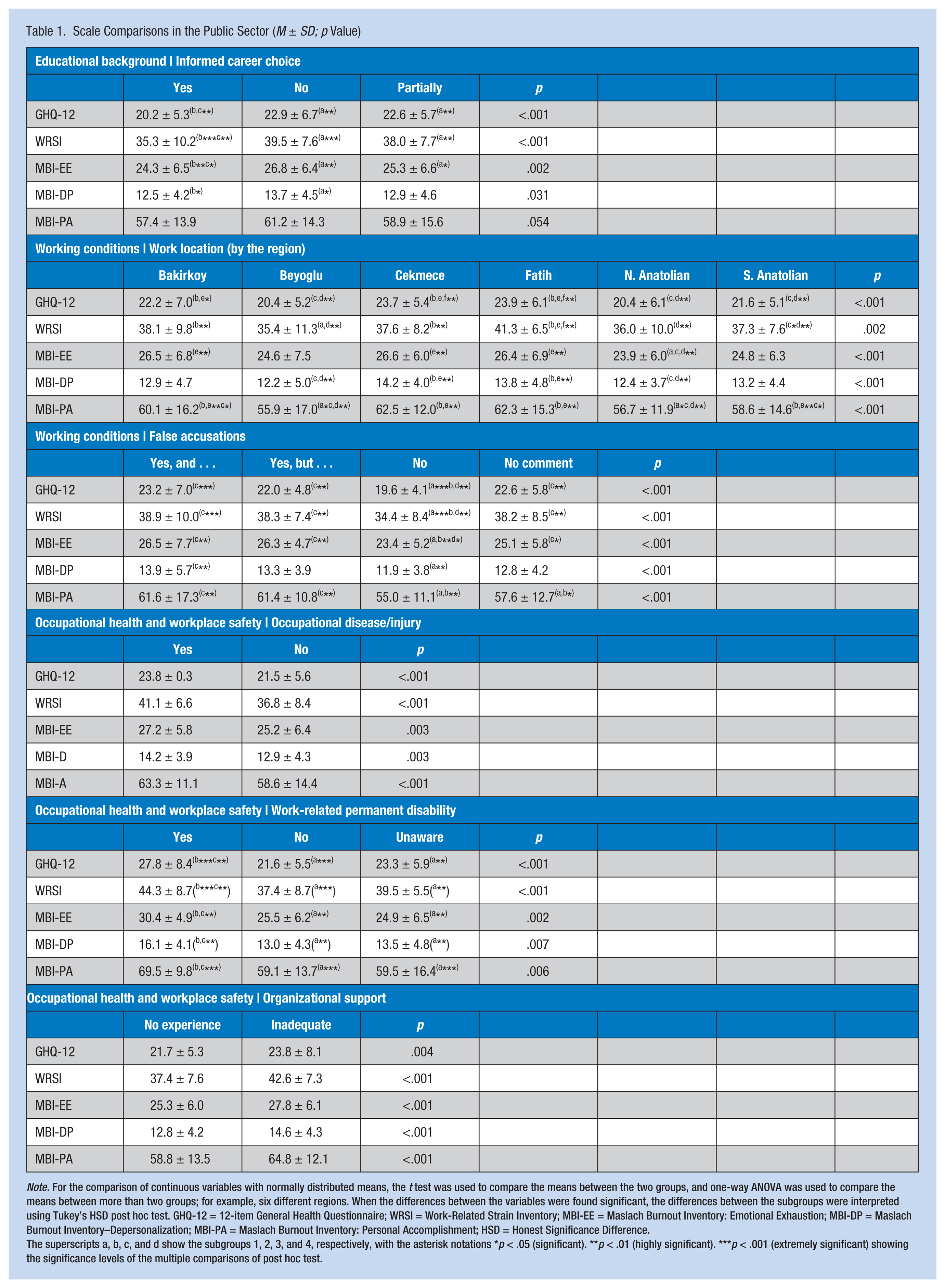
Note. For the comparison of continuous variables with normally distributed means, the t test was used to compare the means between the two groups, and one-way ANOVA was used to compare the means between more than two groups; for example, six different regions. When the differences between the variables were found significant, the differences between the subgroups were interpreted using Tukey’s HSD post hoc test. GHQ-12 = 12-item General Health Questionnaire; WRSI = Work-Related Strain Inventory; MBI-EE = Maslach Burnout Inventory: Emotional Exhaustion; MBI-DP = Maslach Burnout Inventory–Depersonalization; MBI-PA = Maslach Burnout Inventory: Personal Accomplishment; HSD = Honest Significance Difference.
The superscripts a, b, c, and d show the subgroups 1, 2, 3, and 4, respectively, with the asterisk notations *p < .05 (significant). **p < .01 (highly significant). ***p < .001 (extremely significant) showing the significance levels of the multiple comparisons of post hoc test.
Scale Comparisons in the Private Sector (M ± SD; p Value)
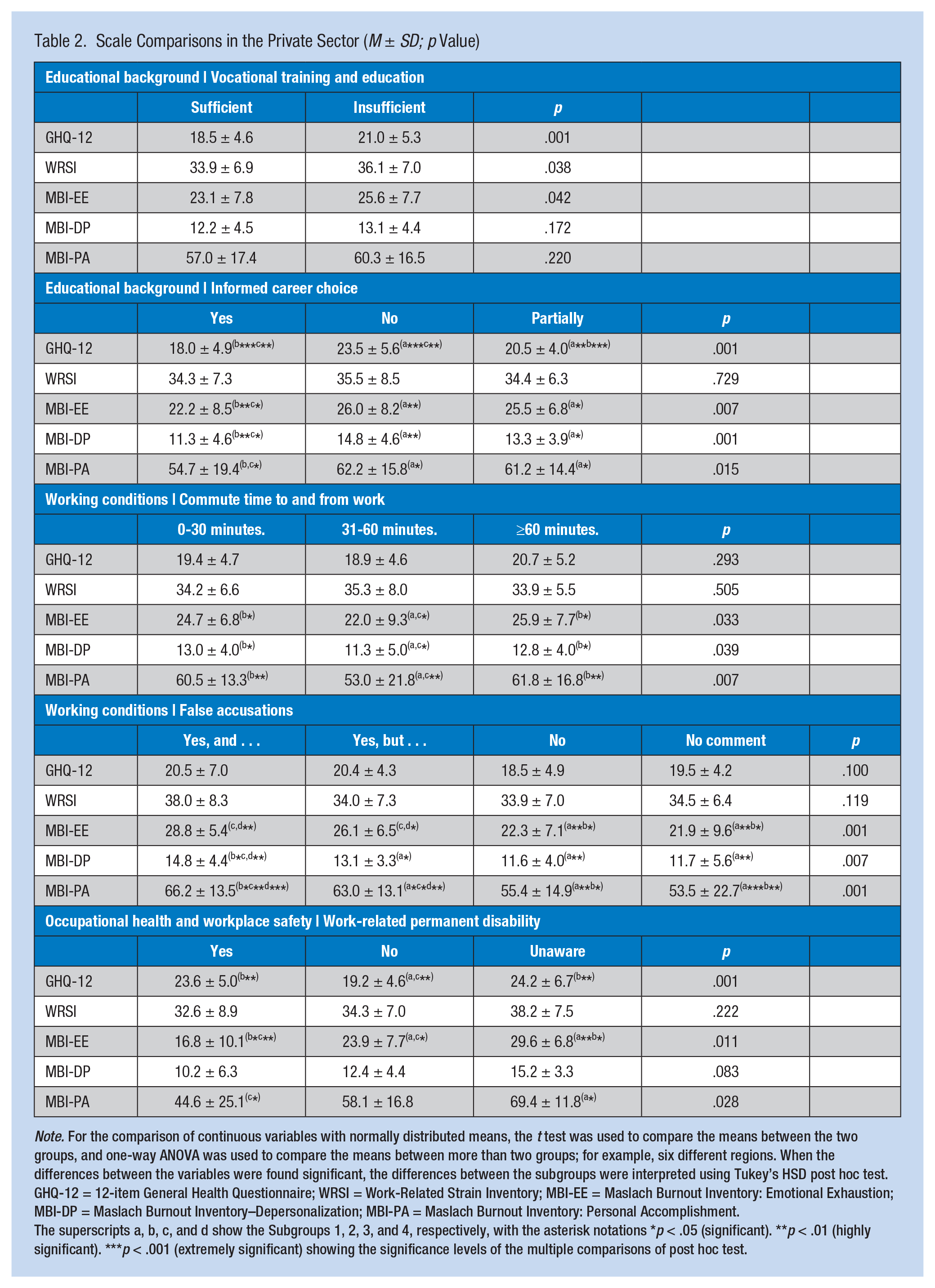
Note. For the comparison of continuous variables with normally distributed means, the t test was used to compare the means between the two groups, and one-way ANOVA was used to compare the means between more than two groups; for example, six different regions. When the differences between the variables were found significant, the differences between the subgroups were interpreted using Tukey’s HSD post hoc test. GHQ-12 = 12-item General Health Questionnaire; WRSI = Work-Related Strain Inventory; MBI-EE = Maslach Burnout Inventory: Emotional Exhaustion; MBI-DP = Maslach Burnout Inventory–Depersonalization; MBI-PA = Maslach Burnout Inventory: Personal Accomplishment.
The superscripts a, b, c, and d show the Subgroups 1, 2, 3, and 4, respectively, with the asterisk notations *p < .05 (significant). **p < .01 (highly significant). ***p < .001 (extremely significant) showing the significance levels of the multiple comparisons of post hoc test.
In the public sector, perceived issues regarding work locations, false accusations, occupational injuries or diseases, work-related permanent disabilities, and organizational support were found to significantly influence EMT-Bs’ well-being (p < .05 on all scales; Table 1). Work locations were categorized by the six regions of the city (i.e., Bakirkoy, Beyoglu, Cekmece, Fatih, Northern Anatolian, Southern Anatolian). Commute time to and from work ranged from 0 to 30 minutes, 31 to 60 minutes, and more than 60 minutes. EMT-Bs were asked whether they believed they were sometimes falsely accused of mistakes made by others (e.g., supervisors, ambulance team members, firefighters, police). Four available responses were yes and for this reason, I blame others; yes, I am at times falsely accused but I don’t believe that fellow colleagues are either insensitive or malicious; no; and no comment. Regarding vocational training and pre-licensure education, the two responses were sufficient and insufficient. Similarly, EMT-Bs were asked whether they had the opportunity to make informed career choices. Three answer choices were yes, no, and partially. EMT-Bs were asked whether they had experienced work-related injuries or occupational diseases to which respondents could answer yes or no. Responses to the question about work-related permanent disabilities were yes, no, or unaware/uninformed. In the presence of work-related injuries or occupational diseases, EMT-Bs were asked about the extent of organizational support they received. Respondents answered either no such experience, adequate organizational support, or inadequate organizational support with regard to work-related injury or occupational disease.
In the private sector, time spent commuting to and from work (p < .05 on all MBI subscales), false accusations (p < .05 on all MBI subscales), vocational training or education (p < .05 on GHQ, WRSI, MBI-EE), informed career choice (p < .05 on GHQ, all MBI subscales), and work-related permanent disabilities (p < .05 on GHQ, MBI-EE, MBI-PA) were found to significantly influence EMT-Bs’ reported well-being (Table 2).
In the public and private sectors, priority expectations were related to higher earnings (17.5%; 16.7%) and better social opportunities (17,4%; 16,8%). Of 3,073 responses in the public sector, increased wages, improved social amenities, better physical conditions in the work environment, professional dignity and respectability, and career development and promotional opportunities received 538 (17.5%), 536 (17.4%), 467 (15.2%), 443 (14.4%), and 389 (12.7%) responses, respectively. Of a total of 835 responses in the private sector, increased wages, improved social amenities, better physical conditions in the work environment, professional dignity and respectability, and career development and promotional opportunities received 139 (16.7%), 140 (16.8%), 68 (8.1%), 111 (13.3%), and 140 (16.8%) responses, respectively (Figure 1).
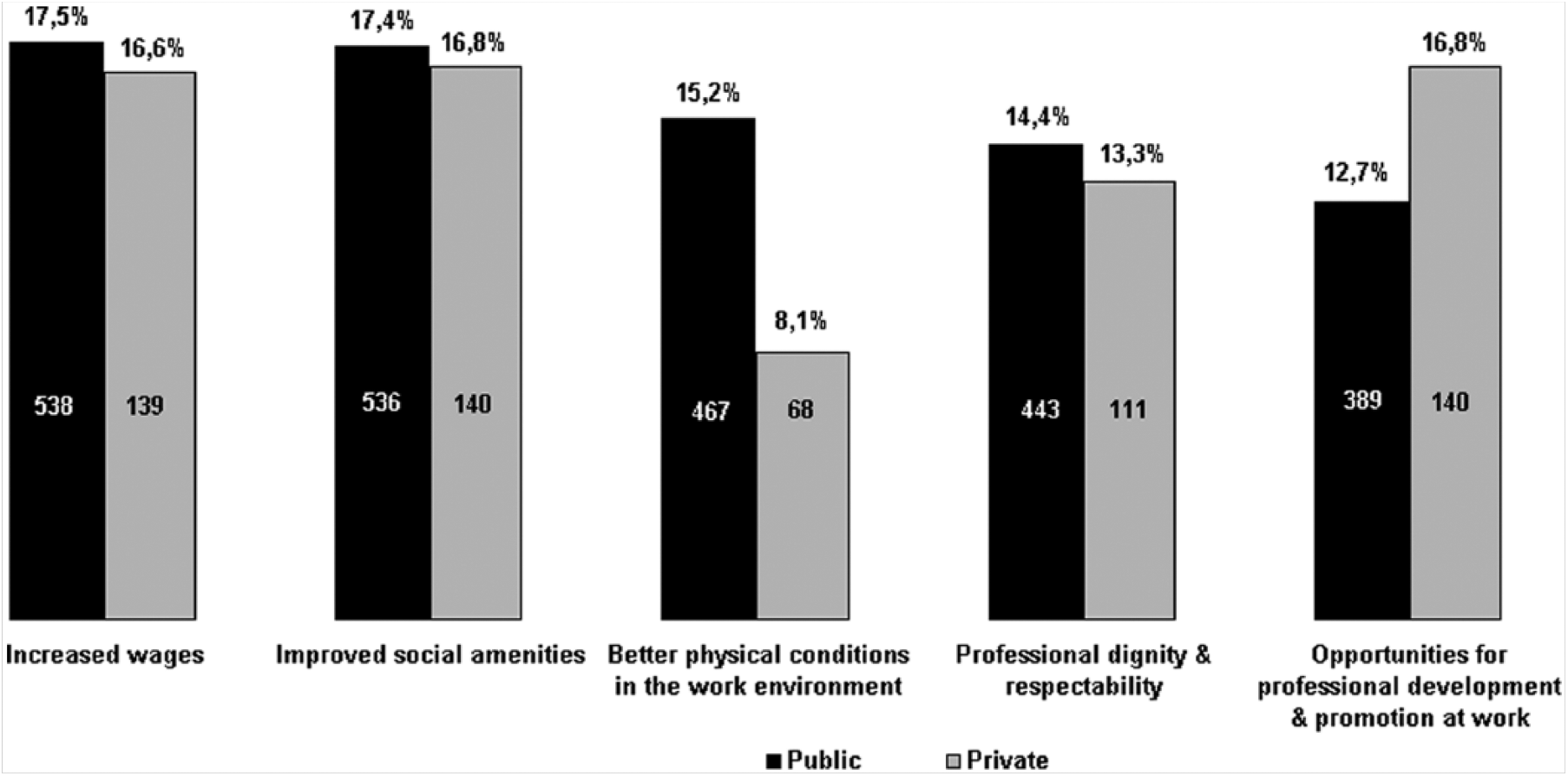
Priority expectations in the public and private sectors (number of responses with percentage equivalents)
With regard to the original research question, educational background, working conditions, and OHS were identified as predictors of mental, physical, and emotional strain in EMT-Bs. Educational background specifically related to counseling prior to making informed career choices and the quality of education received while in training; working conditions specifically related to regional differences, proximity of work to place of residence, being falsely accused; OHS specifically related to occupational diseases or injuries, work-related permanent disabilities, and adequacy of organizational support were the identified determinants of strain. The study determined that public versus private ambulance services generally did not predict the mental, physical, and emotional well-being of EMT-Bs in Istanbul.
Discussion
The overall differences between total mean scores and standard deviations between the public and private sectors were not statistically significant (p > .05 on all scales), indicating that public versus private employment did not predict worker well-being, supporting the findings of previous studies (Dolphin, 1978; Homedes & Ugalde, 2005).
Predictors of Physical and Psychosocial Well-Being
The study identified educational background, working conditions, and OHS as the determinants of general health, work-related strain, and burnout in public and private ambulance EMT-Bs in Istanbul.
Educational background
Receiving career counseling prior to choosing a career and the quality of education were significant determinants of well-being. EMT-Bs’ perceptions of their formal training influenced general health and caused strain and emotional exhaustion in the private sector (p < .05 on GHQ, WRSI, MBI-EE; Table 2). Making informed career choices influenced EMT-Bs’ emotional well-being (public: p < .05 on GHQ, WRSI, MBI-EE, MBI-DP; private: p < .050 on GHQ, all MBI subscales; Tables 1 and 2).
Working conditions
As predictors of psychosocial well-being, ambulance personnel’s concerns about working conditions should be taken into consideration (Aasa et al., 2005). For EMT-Bs in the public sector, work locations significantly influence general health, reported strain, and burnout (p < .05 on all scales; Table 1). Excess workload and operationally inconvenient demands weighed heavily on public employees. Time spent commuting to and from work was a determinant of burnout among EMT-Bs who worked on commercially operated ambulances (p < .05 on all MBI subscales; Table 2). It may be relatively easy for public ambulance EMT-Bs to work at suitably located stations; however, private company EMT-Bs had fewer location choices.
Teamwork is an essential part of emergency care (Williams, Rose, & Simon, 1999). EMT-Bs were asked whether they felt they were sometimes falsely accused of mistakes made by others (e.g., supervisors, ambulance team members, firefighters, police). False accusations appeared to be major issues in both sectors. EMT-Bs who felt they were sometimes falsely accused and blamed those around them were more negatively influenced in terms of their general health and mental well-being than EMT-Bs who did not report that others were either insensitive or malicious (public: p < .05 on all scales; private: p < .05 on all MBI subscales; Tables 1 and 2).
Occupational Health and Workplace Safety
EMS should ideally be delivered by healthy employees who work in healthy environments. EMT-Bs were asked whether they previously experienced work-related injuries or occupational diseases. Occupational injuries and diseases significantly influenced EMT-Bs’ well-being, especially in the public sector (p < .05 on all scales; Table 1). Work-related permanent disabilities significantly influence EMT-Bs’ well-being, with critical impact on both sectors (public: p < .05 on all scales; private: p < .05 on GHQ, MBI-EE, MBI-PA; Tables 1 & 2). The nature and severity of the injuries and illnesses, procedural formalities, professional consequences (e.g., effects on continuity of employment, costs and expenses incurred by the employer, and institutional attitudes) and overall implications of the event may show sector variations. Organizational factors are important in managing occupational stress (Visser, Smets, Oort, & De Haes, 2003). EMT-Bs were asked whether they received adequate health care, management support, and legal assistance after an occupational injury or work-related illness. Having a history of an occupational disease, injury, or permanent disability, without adequate organizational support, increased mental and emotional strain in EMT-Bs. Evidence was clear (public: p < .050 on all scales; private: p < .050 on GHQ, MBI-EE, MBI-PA; Tables 1 & 2), in spite of the statement by the chief medical officer overseeing 112 public ambulance services that coping skills trainings and professional care are available to staff. Findings comply with evidence from earlier studies that job conditions, the work environment, psychological demands, and limited support from colleagues and supervisors are significant risks to workers’ mental health (Aasa et al., 2005; Revicki & Gershon, 1996; van der Ploeg & Kleber, 2003).
Priority Expectations
Wage satisfaction and perceptions of income adequacy may be associated with job contentment. Psychosocial problems and physical complaints among EMTs are also often related to the work environment (Hogya & Ellis, 1990; Maguire, Hunting, Guidotti et al., 2005; Okada et al., 2005). EMT-Bs were asked which aspects of their occupational life should be improved to positively influence their sense of well-being at work. Multiple answers were accepted. In the public and private sectors, priority expectations were higher earnings (17.5%; 16.7%), better social opportunities (17.4%; 16.8%), better work environments (15.2%; 8.1%), professional respectability (14.4%; 13.3%), and career development and promotional opportunities (12.7%; 16.8%; Figure 1).
Implications for Policy Development
Policy recommendations are based on the objective that new legislation is developed, under the current National OHS Law 2012 and in compliance with existing legislation, designed specifically to address OHS issues in PHEC. The aim was to reduce excessive levels of occupational stress, which affect workers’ health, implement measures to prevent occupational injury and disease, and promote psychological and physiological well-being as an integral part of the organizational culture in all ambulance services. The law provides a general legislative and policy framework for the protection of all employees. The act should recognize the risky exhausting nature of health care professionals’ work and grant them risk-related early retirement (RER) privileges.
Policy objectives in education should prioritize accreditation and quality assurance in EMT training. Programs in Turkey should emphasize universal precautions, OHS procedures, prevention techniques, treatment of on-the-job injuries, exposures to infectious agents and hazardous materials, skills needed for collaborative practice, strategies to cope with agitated or violent patients, and competencies to solve complex health care situations in a variety of settings. Working conditions, proximity of work to place of residence, and the convenience of work location should be taken into consideration whenever possible. Organizational policies for housing assistance may be explored. Efforts should be made to improve the physical and psychosocial work environments of EMT-Bs and diversify social opportunities available to staff. Communication skills and strategies should be developed to overcome the problem of false accusations. Prevention programs and provision of adequate support in case of an occupational injury or illness are organizational obligations. Risk assessment interviews, examinations of the effects of traumatic events, staff consultations, and trainings should be practiced to reduce stress reactions (Awa, Plaumann, & Walter, 2010). Attention must be drawn to the importance of professional respectability. Violence reduction must be declared a policy priority by the MoH.
The National OHS Law 2012 generally acknowledges the role of the certified occupational health nurse. This research supports the need to employ occupational health nurses, a novelty presented to ambulance service administrative boards in Turkey. As in other developed countries, occupational health nurses can collaborate with employers to establish a culture of OHS. The occupational health nurse is equipped with appropriate authority, expertise, and resources to manage OHS operations, assume a broad array of responsibilities, and positively influence EMTs’ performance. As OHS specialists in ambulance services, occupational health nurses are expected to advise employers and employees on occupational health control strategies and best practices, risk assessment, hazard identification, absenteeism, target injury reductions, disease management and health promotion programs, occupational health surveillance, staff’s health status, communication problems, and health education programs. Nurses can also raise awareness of the occupational determinants of health and social well-being, increase compliance with principles and standards, establish ethical guidelines, observe quality of work life, prepare objective observational checklists, conduct independent research, and gather information for policy development based on unbiased observations (Perhats et al., 2012; WHO Regional Office for Europe, 2001).
Suggestions for Future Research
The present study has been a valuable tool and the first of its kind to screen for major EMT risk factors associated with occupational well-being, comparing public versus private practice. Although self-report questionnaires are limited by design in that they raise questions of validity, their practical value is contributed feedback on a wide range of topics from a study population of considerable size. Researchers protected the anonymity and confidentiality of the respondents, which brought honesty to the feedback. Results may be used as starting points for future research endeavors to reduce confounding factors and gain further insights into integrated methods of self-report questionnaires combined with observational data (e.g., checklist data structured by occupational health nurses), which may be a useful design for future studies. Longitudinal intervention studies can note changes over time and capture those changes. The short- and long-term effects of interventions such as improving the physical work environment, integrating trainings into the basic curriculum of EMTs, adding educational modules on topics such as personal protective equipment (PPE) use, coping skills, and self-protective behavior models can be studied. Objective measures may include saliva cortisol and blood pressure measurements, physician-diagnosed conditions, health status evaluations, sickness reports, “late to or missing from work” forms, absenteeism, turnover rates, lawsuits, patient complaints, checklists of stressors at work prepared by independent parties (e.g., occupational health nurses), and quality standards inspections. Unbiased investigations are mandates for positive progress. Survey studies can be used to examine EMTs’ safety practices and test for their knowledge about the risks and hazards surrounding those practices. Cohort studies can elaborate on the causes of and circumstances related to job injuries and vehicle crashes. Broad-based international epidemiological studies, comparing world statistics with national data, will offer decision-makers realistic perspectives on issues such as work-related accidents, injuries, and illnesses. In depth research must be designed to study organizational factors, construct policy details, and guide legislative actions.
Conclusion
From a broad scale perspective, self-reported occupational stress among ambulance EMT-Bs was comparable, whether employed by public services or private companies. Educational background, working conditions, and OHS emerged as topics that merit priority attention. Vocational training and pre-licensure education must be improved to prepare candidates for a challenging career. Accreditation and quality assurance are policy priorities. Emergency medical technician training programs in Turkey must emphasize OHS best practices; policies must establish an OHS culture. Working conditions such as work locations, commute time, and false accusations adversely affected overall worker well-being. Where the community relies heavily on local public employees, national policies and institutional regulations are crucial for optimal workload distribution. Promoting institutional and governmental strategies to explore the opportunities for professional development, and recognizing the need for improvement in the work environment are essential steps toward positive transformations. Occupational health and safety is evidently definitive in determining the overall well-being of EMT-Bs in Istanbul. Healthy communications within the organization, effective interactions with outside collaborators, and strategic interventions for violence reduction are tipping points. Public health communication is important, as EMT-Bs seek improvements in professional respectability.
A primary suggestion is for comprehensive OHS policy development, specifically for PHEC services under the current National OHS Law 2012 and in compliance with existing legislation, to ensure staff are not exposed to excessive levels of occupational stress and that entities are held accountable for the responsibilities defined by policy. The provision of adequate support, health care, and legal assistance is an organizational obligation. Overdue policy revision should be officially endorsed for health care workers in general, and EMS personnel in particular. Due to the risky and exhausting nature of their work, EMT-Bs should be granted RER privileges. Because of the core competencies and areas of expertise of occupational health nurses, these professionals should become integral to the organizational structure of ambulance services in Turkey.
Applying Research to Practice
The impact of working for public versus private ambulance services in Istanbul, Turkey was investigated, elaborating on the predictors of mental, physical, and emotional well-being in emergency medical technicians (EMT). In the observational cross-sectional study, a self-report survey was used to gather information about employee demographics, socioeconomic status, educational background, working conditions, occupational health and workplace safety (OHS), followed by the GHQ-12, WRSI, and MBI questionnaires. In 2011 1,038 EMT-Bs worked for public and 483 EMT-Bs worked for private ambulance services in Istanbul. EMTs were asked about aspects of their working lives that needed improvements; priority expectations were higher earnings and better social opportunities. Educational background, working conditions, and OHS emerged as topics that merit priority attention. From a broad scale perspective, self-reported occupational stress among ambulance EMTs was comparable in both sectors. A primary suggestion is for comprehensive EMS/OHS policy development, under the current National OHS Law 2012.
Footnotes
Acknowledgements
Thanks are due to the authorities at the Republic of Turkey Ministry of Health (TR MoH) Health Directorate of Istanbul for sharing their professional experiences and facilitating the process of data collection. Deserving of particular acknowledgment is the staff’s commitment at the Department of Emergency Medical Services (EMS) and the R&D Unit to the completion of the survey forms in an accurate and timely manner. Words fail to express EMTs’ altruism and selfless devotion to the welfare of individuals in critical need. Efforts and sacrifices in EMS are highly appreciated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Verda Tunaligil, MD, MPH, PhD, is currently the Founding Department Chief of Monitoring and Evaluation (M&E) at the Republic of Turkey (TR) Ministry of Health’s (MoH) Health Directorate of Istanbul, with responsibilities to oversee entire M&E activity in the provision of Istanbul’s health care services and overall compliance with health policy objectives. Formerly, she inaugurated the Research and Development (R&D) Unit, reported directly to the Health Director of Istanbul, initiated international collaborations and networks, promoted advancements and research activities, and launched foremost innovations in public health and medical sciences. She received her MD, MPH in health policy and management, and PhD degrees from Istanbul University and Harvard University School of Public Health, lived and trained internationally for many years, and worked at Harvard Medical School–affiliated Children’s Hospital Boston. Dr. Tunaligil’s research interest focuses on disasters and complex humanitarian emergencies.
Ali Ihsan Dokucu, MD, MBA, is currently in clinical practice at the TR MoH Istanbul Sisli Hamidiye Etfal Research and Training (R&T) Hospital, was the former TR MoH Health Director of Istanbul and the former Chairman of the Public Hospitals Institution of Turkey. He completed his residency training at Vth, XIth, and XIIIth University of Paris, is European Board-certified (UEMS) in Pediatric Surgery in Rotterdam/Holland, and worked as “Chef de Clinique” at the Hospital of Necker in Paris, France.
Mehmet Sarper Erdogan, MD, PhD, is faculty at the Cerrahpasa Medical Faculty, Dept. of Public Health at Istanbul University, where he initiated the discipline of occupational health and safety. He received his MD and PhD diplomas from Istanbul University and Justus Liebig University’s Institute of Occupational and Social Medicine in Giessen (Germany), and teaches post-graduate courses and is academic advisor for degree programs.