
Abstract
Background:
Workplace violence and harassment are commonplace for healthcare workers and most incidents are unreported. Normalization of these experiences, lack of confidence in reporting systems, and fear of the consequences of reporting contribute to the invisibility of these experiences. Challenges are exacerbated in homecare settings and for precarious workforces including Personal Support Workers (PSWs). We created, piloted, and evaluated an intervention to enhance safety culture and encourage reporting of workplace violence and harassment.
Methods:
A multi-stakeholder steering committee designed an intervention combining policy changes, a pre-visit screening tool, education, and brief end-of-visit reporting. This was piloted with a PSW care team which provided >55,000 client visits during the 32-week intervention. Operational metrics characterized screening, education, and reporting uptake. Pre- and post-intervention surveys characterized PSWs’ experiences with workplace violence and harassment, reporting experiences, training history and intervention feedback.
Findings:
PSWs reported increased comfort discussing workplace violence and harassment, and increased confidence managing client-to-worker incidents. The screening went smoothly with most clients in private homes. Most PSWs (75%) engaged at least once with end-of-visit reporting and nearly half submitted reports regularly. During the pilot, 21% of PSWs reported incidents and 52% of reports shared client-specific strategies for managing these situations.
Application to Practice:
Changes in comfort and behavior with reporting indicated a shift toward a more open culture surrounding workplace violence and harassment. Tools created for this intervention and lessons for implementation are shared for consideration by occupational health practitioners throughout the homecare sector.
Keywords
Background
Workplace violence and harassment are commonplace for healthcare workers and account for 13% of lost-time injuries to healthcare workers in Ontario (Government of Ontario, 2021). With > 60% of surveyed healthcare workers sharing that they experienced abuse and/or violence annually (Lu et al., 2020), it has become normalized and is tolerated as a part of the job (Byon et al., 2020; Kelly, 2017; King et al., 2018; Lim et al., 2022). Although it is normalized, violence negatively impacts the physical and mental health of exposed healthcare workers, decreases their job satisfaction and performance, reduces the quality of patient care, and increases the likelihood that they will quit their jobs or leave healthcare work entirely (Pariona-Cabrera et al., 2020).
This culture of normalizing and tolerating violence and harassment contributes to severe underreporting of these incidents (Byon et al., 2020). In one survey, only 12% of healthcare worker respondents who said they had experienced a violent event in the past year had reported it (Arnetz et al., 2015); other estimates are that only 19% of incidents are officially reported (Pompeii et al., 2016). Underreporting of violence and harassment makes prevalence hard to estimate, undermines the effective development and targeting of prevention strategies, and makes the impact of interventions difficult to measure.
The prevalence of violence and harassment in home care is thought to be even higher than in institutional settings. The majority of paid home care (70–80%) is provided by unregulated direct care workers known in Ontario as Personal Support Workers (PSWs) who provide assistance with personal care and other common daily activities (Saari et al., 2018; Sinn et al., 2022). They work alone, with limited access to peer and supervisory support (Barken et al., 2020), and in the social context of the client’s private home, rather than an institution (Angus et al., 2005). In addition, this homecare PSW workforce is highly precarious, comprised in large part of racialized (> 50%) and immigrant (nearly 50%) women (> 90%) with low wages and little structural power (Barken et al., 2020; Butler, 2018; Denton et al., 2018; Kelly & Bourgeault, 2015; Lum et al., 2010; Saari et al., 2018; Zagrodney & Saks, 2017).
PSWs working in home care have shared through numerous research studies that they do not perceive reporting to be valuable, find the processes for reporting to be unclear, complex, and time-consuming, and are concerned about potential consequences of reporting—including risks to job security, income, reputation, and client relationships (Craven et al., 2012; King et al., 2018; Lang et al., 2014; Stevenson et al., 2012). Other barriers to reporting include lack of clarity on what constitutes violence that should be reported, lack of training on how to report, and concerns that supervisors will not be supportive (Byon et al., 2020; Craven et al., 2012; Lang et al., 2014; Sims-Gould & Martin-Matthews, 2010; Stevenson et al., 2012).
To create a supportive safety culture and encourage reporting of workplace violence and harassment, an intervention designed to address these barriers was created and piloted at an organization that employs PSWs to provide homecare services. This infrastructure combined policy, screening, education, and reporting to de-normalize and track the occurrence of these incidents. This paper will report on the development and evaluation of this pilot.
Methods
This intervention was developed and evaluated at a large, not-for-profit homecare provider organization based in Ontario, Canada, that offers community-based personal support, nursing, and rehabilitation services. The 7-month open cohort pilot was conducted with all members of one personal support team that provides care in private residences and retirement homes. The team is comprised at any time of up to 69 PSWs, a supervising Registered Practical Nurse, a clinical lead (also a Registered Practical Nurse), and two scheduling coordinators. Administrative and survey-based data were used to evaluate the pilot.
Intervention Development
A structured approach to intervention development was guided by the Registered Nurse Association of Ontario’s (RNAO)’s “Best Practice Guideline: Preventing Violence, Harassment and Bullying Against Health Workers” (Campbell et al., 2014; Registered Nurses’ Association of Ontario [RNAO], 2019). Intervention design was led by a steering committee that included best practice leadership; Human Resource leads for health and safety and diversity, equity, and inclusion; operations leadership; supervisors; client partners; and a researcher. Based on a gap analysis of existing organizational practices and resources, the steering committee elected to focus on strengthening policies, screening, education, and reporting. Working groups drafted each element of the intervention and all were reviewed by the steering committee prior to implementation. All tools and the full implementation plan were also reviewed by the leadership of the team in which the project was implemented, including the supervisor, clinical lead, scheduling coordinators and a PSW peer coach. This team also engaged in ongoing monitoring of the intervention progress through weekly meetings with the implementation team. The reporting tool was reviewed and piloted by three PSWs prior to implementation.
Intervention
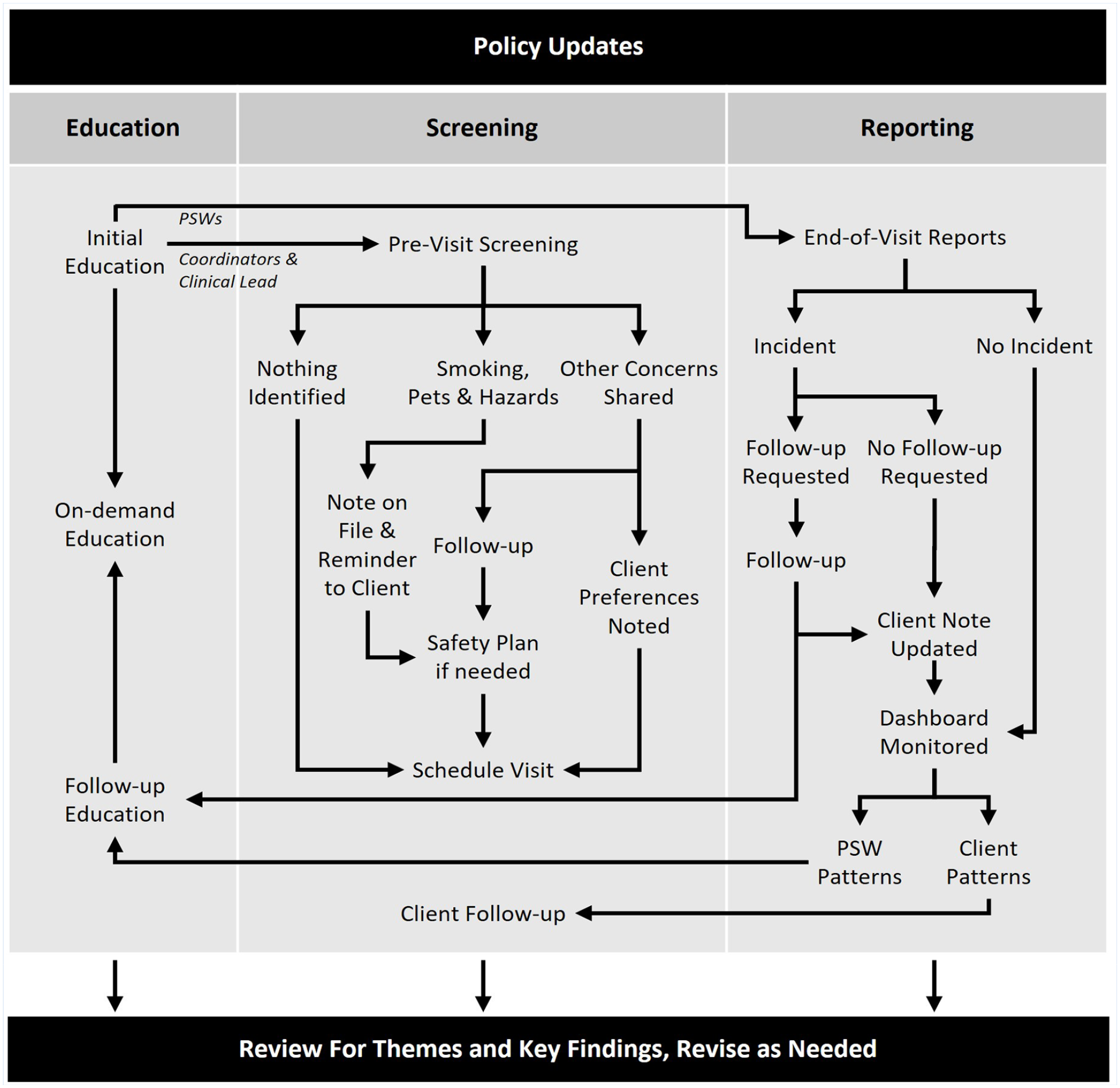
The three pillars of this intervention were screening, education, and reporting, and the intervention was supported by an updated policy framework (Figure 1). Policy enhancements clarified definitions and gave examples of harassment, provided guidance on supervisory follow-up in response to reports of violence or harassment, and formalized the organization’s commitment to creating an inclusive, psychologically safe work environment.
Description of Intervention
Screening new clients before a healthcare worker’s initial visit is a common and well-supported recommendation to reduce the potential for violence and harassment (Campbell et al., 2014; RNAO, 2019). The only organizational contact prior to a PSW’s first visit is a scheduling call. The steering committee’s review of existing screening tools designed for use in long-term care and community settings determined that they would not be appropriate in content, tone, or length for use during this call (Kim et al., 2017; Public Services Health & Safety Association [PSHSA], 2017, 2021; Woods & Almvik, 2002). Consequently, a novel screening tool (Table 1) was developed with the goal of initiating a client-centered conversation about the upcoming visit and addressing potential risks while reminding clients that the home is also a workplace for visiting PSWs (Angus et al., 2005). The first screening question was designed to create space for family caregivers to express any concern about the potential for responsive behaviors that may be exhibited by clients with dementia—a common contributor to homecare PSWs’ experiences of workplace violence and harassment (Galinsky et al., 2010; Karlsson et al., 2019; Schnelli et al., 2020). It was used based on providers’ previous experiences in screening for such risks during pre-visit phone calls with new clients. A more direct/explicit approach was deemed by the steering committee to be both unsuccessful and offensive to clients. The presence of other specific hazards was addressed through the second question. Potential hazards were noted in the client’s file and shared with the clinical lead and PSW before the first client visit.
Intervention Tools
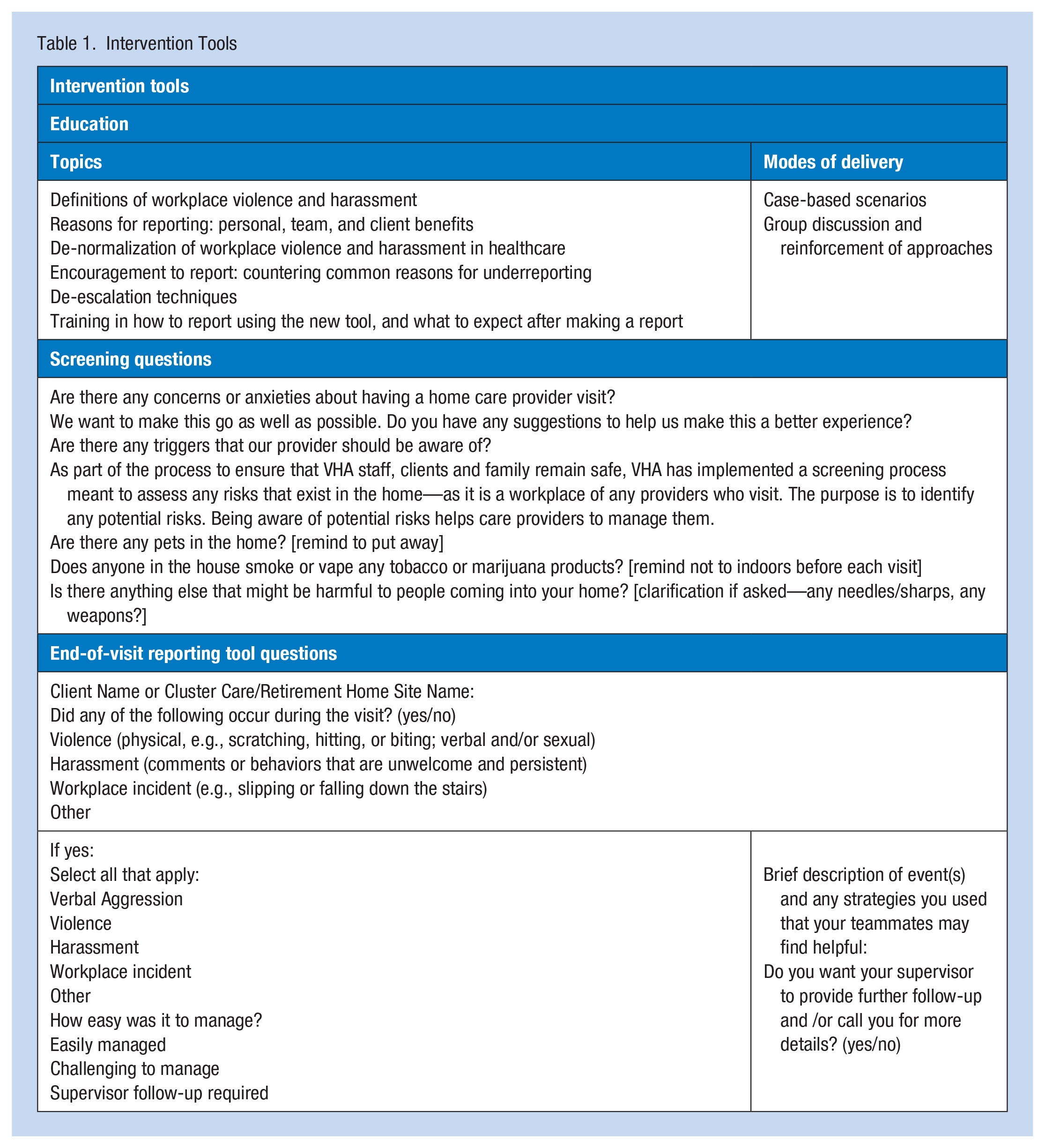
The education and reporting were designed to address the need for organizations to have a clear definition of workplace violence and harassment, a formal reporting system that is easy to use, and supportive responses from supervisors to incident reports (Byon et al., 2020; Campbell et al., 2014; Small et al., 2020). They were structured according to the MARS model which emphasizes the influence of motivation, ability, role perceptions, and situational factors on individual behavior (McShane & Von Glinow, 2015).
Interactive paid education sessions addressing the topics summarized in Table 1 focused on PSWs’ role perceptions and motivations related to reporting. Education included the Ontario Human Rights Code definitions of workplace violence and harassment, while clarifying that even if it was not part of a pattern of behavior, any instance of verbal aggression (e.g., shouting, swearing, verbal hostility) should be reported. In support of a culture of collective responsibility for team safety, education aimed to increase motivation for reporting and connect this to participants’ role perception by emphasizing the importance of reporting incidents regardless of the client’s medical condition (such as responsive behaviors associated with dementia or poorly-controlled pain) and the impact of providing information to support team members managing similar situations or highlight an opportunity for clinical intervention. PSWs were taught how to use the new end-of-visit reporting tool, designed to increase their ability to report easily. These sessions also addressed common situational barriers to reporting by providing clarity about how supervisors and the organization would respond to reports, and that PSWs would continue to have agency regarding the nature of the follow-up.
The end-of-visit reporting tool (Table 1) was a brief digital form, a link to which was emailed to PSWs after each client visit, that asked if any incident had occurred. If an incident was reported, PSWs were asked to briefly describe it, indicate whether they wanted supervisory follow-up, and share strategies for managing the situation. Descriptions and strategies were shared in the electronic client record where they could be viewed by other PSWs in the circle of care. All reports were shared with supervisors (and Human Resources as appropriate) and reflected in a digital dashboard for leadership that showed report rates and supported supervisors to identify and act on concerning patterns (e.g., frequent incident reports from individual providers or about certain clients). The quick, simple design of this form was intended to increase PSWs’ ability to rapidly share information that could enhance team safety and the quality of client care.
Intervention Implementation
Screening of new clients during scheduling calls was initiated in parallel with the introduction of education sessions. Four education sessions were offered in the 2 weeks prior to the launch of the end-of-visit reporting tool. During an initial 7-week “trained user phase,” only PSWs who had completed the education were invited to report. Three supplementary sessions were offered during this time; attendees were sent end-of-visit reporting invitations once they had completed the education. Attendance at the education sessions was encouraged through supervisory email blasts and outreach calls to each PSW. After the 7-week “trained user phase,” a 25-week “open phase” was launched in which all PSWs on the team were invited to complete reports regardless of training status. Four microlearning opportunities (brief newsletters) were emailed to PSWs during the first month of the “open phase” to encourage reporting and reinforce key ideas.
Data Collection and Analysis
Screening data recorded by the scheduling coordinators included how many new clients were screened per week, whether risks were identified, and impressions of the screening tool; these were shared weekly with the project implementation team. Attendance at education sessions was tracked. End-of-visit report completion and indicators related to content were reviewed to understand PSWs’ engagement and experiences. Pre- and post-intervention surveys were used to understand PSW demographics, predominant sites of care, history of workplace violence and harassment, experiences and comfort levels reporting such experiences (on Likert-type scales), and participation in related education. The post-intervention survey asked about experiences of workplace violence and harassment and used the same Likert-type scales as the initial survey to capture comfort responding to and reporting these experiences. Additional questions with Likert-type scales were used to capture the perceived value and user experience associated with the reporting tool. Finally, the survey sought opportunities for improvement before spreading the intervention. These surveys were anonymous and were administered by a member of the research team who had no prior relationship with the care team. Quantitative data were summarized using descriptive statistics; t-tests and Fischer’s Exact Tests (significance p < .05) were used to assess the significance of differences between pre- and post-intervention survey findings and qualitative data were summarized using content analysis.
Results
During the 32-week intervention, 69 PSWs provided > 55,000 care visits to 410 clients. Of these, 110 clients living in retirement homes received 23,110 visits.
Baseline
PSWs who completed the baseline survey (n = 36) were predominantly middle-aged (80% aged 36–55), women (97%), and 46% had been hired within the previous 5 years. All identified as being part of a racialized group: 34% identified as South Asian, 40% as East/Southeast Asian, and the remaining individuals identified as African, Caribbean, or choose not to respond. They cared for clients in private homes (38%), retirement homes (31%), or a mix of both (31%). As a condition of employment, all had sufficient English language proficiency to read and contribute to client documentation and to provide care in English.
Most (81%) PSWs shared that they had previously experienced violence or harassment, of whom 93% had experienced client-to-worker violence or harassment. All PSWs who had experienced client-to-worker violence or harassment had incidents related to the client’s medical condition; 63% had experiences not attributed to the client’s medical condition, and 26% had incidents involving a client’s family member. In addition, 38% reported incidents involving other paid caregivers, of which 82% reported incidents related to caregivers with different employers, and 27% had incidents involving colleagues.
At baseline, 72% of PSWs had reported at least one incident of violence or harassment to the organization. Conversely, 32% had experienced but not reported harassment, and 20% had experienced but not reported violence. The majority of non-reporting was linked to incidents where a client’s medical condition was a contributing factor (64% and 86% of cases, respectively). When reporting, the majority told their supervisors (78%); others shared with peer coaches, scheduling coordinators, or Human Resources. Of those who had reported, 78% believed that their reports were taken seriously.
Among survey respondents, previous engagement with workplace violence and harassment education was high: 97% had supplementary education, beyond that provided at orientation: 22% had taken external courses, 69% had taken internal courses, 56% had received education in team meetings and/or through team emails, and 14% had received one-to-one coaching.
Education
Seven paid, synchronous education sessions were offered: five virtual (2 hours) and two in-person during regularly scheduled team meetings (1 hour). All team leaders and 62% of team PSWs attended education sessions.
Screening
During the intervention period, 56% of new clients who lived in private residences were screened (59 screenings). Of these new clients, four (7%) had potential risks identified, recorded in the client file, and communicated to affected team members (Figure 1). Coordinators did not screen new clients from retirement homes, for whom the questions were redundant due to existing facility practices and procedures for controlling (e.g., by prohibiting pets, weapons, and smoking) and documenting potential hazards (e.g., related to responsive behaviors). For clients in private homes, coordinators reported that the screening usually went smoothly. In some cases (often involving language barriers), clients were confused or offended by the questions and responded aggressively. Not all clients received the full screening either because the scheduling coordinators forgot to conduct the screening (because it was not integrated into their workflow) or in some cases (e.g., when there were language barriers), scheduling coordinators chose to ask only the simplest questions (about pets and smoking).
Reporting and Follow-Up
Overall engagement was high: 75% of PSWs engaged at least once with the system, and 48% submitted reports for at least one-quarter of their visits. Most PSWs who never used the reporting system had also not engaged with the education (88%). The overall response rate as a proportion of total reporting opportunities was 31%.
PSWs overwhelmingly agreed that the system was quick (98%) and easy to use (98%). Over the 32-week pilot, 21% of PSWs reported incidents through the end-of-visit reporting system: 3% violence, 4% harassment, 11% verbal aggression, and 3% other incidents. PSWs requested follow-up for 41% of incidents, reporting that they had already managed the remaining 59% of incidents. Incident details were included in 78% of reports and 52% included PSWs’ suggestions for peers on managing the situation.
Follow-up was provided in all instances where it was requested. Most PSWs (87%) reported that this occurred within the expected 3-day timeline; 91% were satisfied or very satisfied with the quality of the follow-up with the remainder neutral. All PSWs who reported incidents believed that their reports were taken seriously—a significant improvement from 78% pre-intervention (Fisher’s exact p = .021).
All PSWs who had used the reporting tool at least once found it valuable. Most post-intervention survey respondents said the tool should be kept the same; the most commonly requested change was to incorporate the questions into the regular end-of-visit reporting workflow rather than a separate system. A few respondents also requested shorter supervisor response times.
In the post-intervention survey, four PSWs, all of whom had attended the education, shared that they chose not to report incidents of harassment by clients—because they were confident in how they had managed it, because they attributed it to a medical condition, or because they perceived that reporting could create further conflict with the client or family; two of these PSWs also chose not to report violence, as they were confident that they had managed the situations.
Comfort Sharing Experiences of Workplace Violence and Harassment
PSWs’ comfort in sharing their concerns about how they were treated at work increased over the course of the intervention. Their self-rated confidence in responding to incidents involving clients and families increased significantly, from 1.86 (SD 0.65) to 2.23 (SD 0.73), on a 4-point scale from “not confident” (0) to “very confident” (3), t(77) = -2.47, p = .016, and 89% of PSWs indicated that they felt confident or very confident knowing how to report such incidents. Average ratings of comfort speaking with each available support (peers, PSW peer coaches, clinical lead, scheduling coordinators, supervisor, manager/director, and Human Resources) showed increasing trends. There were significant increases in the number of PSWs reporting extreme comfort speaking about workplace violence and harassment concerns with their scheduling coordinator (Fisher’s exact p = .026, OR = 3.46 [95% CI 1.13—11.04]), and a near-significant number of respondents reporting increased comfort in speaking with their manager/regional director (Fisher’s exact p = .053, OR = 3.37 [95% CI 0.97—13.05])—individuals with whom very few PSWs initially reported this level of comfort. Following the intervention, 95% of PSWs reported comfort speaking with at least one member of the leadership team, with nearly two-thirds (65%) reporting that they were “Extremely comfortable” speaking to at least one of these leaders, compared to approximately one half (53%) in the pre-intervention survey.
Discussion
This intervention was designed to change culture to de-normalize workplace violence and harassment experienced by PSWs in home healthcare through the creation of an enabling infrastructure that combined policy, screening, education, and reporting. A supportive culture is particularly important given the precarity of the homecare PSW workforce (Barken et al., 2020; Butler, 2018; Denton et al., 2018; Kelly & Bourgeault, 2015; Lum et al., 2010; Saari et al., 2018; Zagrodney & Saks, 2017), who are at greater risk of violence and harassment and are often less empowered to respond. Several key indicators suggest that this intervention did create culture change: PSWs reported increased comfort and confidence talking about workplace violence and harassment experiences, including with their leaders, and increased confidence responding to the most common types of incidents—those which involve clients and their families. The high number of PSWs who engaged with reporting and the high frequency with which about half completed their reports, despite a lack of integration of these reports into existing workflows, highlights PSWs’ eagerness to share their experiences. This success increases the accuracy with which we can estimate the prevalence of workplace violence and harassment, which remains extremely challenging across healthcare settings (Arnetz et al., 2015; Byon et al., 2020; Pompeii et al., 2016). In addition, collecting all reports in a centralized system facilitated identification and follow-up on problematic patterns of activity related to individual client situations (e.g., if behaviors are related to unmet clinical and/or social needs). Still, some PSWs chose not to report some experiences of violence or harassment. Although the importance of reporting was emphasized during the education sessions, it is clear that continued conversations around shared responsibility for safety and an emphasis on the value of reporting is required to continue to shift the culture to one in which all incidents are made visible and this safety-related information is shared freely within the care team.
To be effective, screening needs to occur prior to the PSW’s first visit. This meant that it had to be included as part of the intake and scheduling conversation. Scheduling coordinators reported that the novel screening tool was appropriate for clients living in private homes, and unnecessary for those who lived in retirement residences (where other screenings and risk management measures are in place). Screening conversations with clients in private homes were typically brief and well-received, although some clients and caregivers with limited English language proficiency struggled to understand the intent of the questions, suggesting an opportunity to continue to refine and simplify the language of the tool. To ensure that screening is conducted consistently, the screening tool should be embedded into scheduling coordinators’ workflows. While the evaluation in this pilot implementation allowed assessment of the usability of the screening tool, it did not provide insight into its effectiveness at identifying potential hazards; further evaluation during larger-scale implementation should compare hazard reporting by PSWs to those identified through screening.
The end-of-visit reporting system was designed to motivate reporting and reduce barriers to doing so, including fear of losing the esteem of their supervisor (e.g., being perceived as whining, lacking resilience, or incompetent), a fear of losing control of the situation (including concerns about negative repercussions for clients), skepticism about the potential for change, and a sense that the inconvenience and burden associated with reporting are too high or that reporting lacks value (Barken et al., 2020; Butler, 2018; Byon et al., 2020; Campbell et al., 2014; Craven et al., 2012; Denton et al., 2018; Kelly & Bourgeault, 2015; King et al., 2018; Lang et al., 2014; Lum et al., 2010; Saari et al., 2018; Sims-Gould & Martin-Matthews, 2010; Small et al., 2020; Stevenson et al., 2012; Zagrodney & Saks, 2017). The reporting system used in this pilot empowered PSWs by allowing them to quickly report each incident (98% said reporting was quick), share their expertise about strategies for managing the individual client situation (present in 50% of reports), and identify the desired degree of supervisory involvement (<50% requested follow-up). PSWs’ reports highlighted that in half of situations, their training and skills were sufficient to manage the challenging client behaviors. Documenting this important safety-related information for their peers reflected an understanding of shared responsibility for team wellbeing.
This intervention was piloted within one care team at one organization where care is provided in an urban environment and leveraged existing mobile devices and client records accessible to all PSWs in the circle of care. Trialing this intervention with only one team created practical limitations on the ability to integrate changes into PSWs’ and coordinators’ workflows, as will be possible during scale-up to the full organization. Even PSWs who had not attended the education were able to use the end-of-visit reporting; however, there may have been gaps in their understanding of what should be reported and how reports are used. Culture change and accessibility may be enhanced through additional asynchronous training, embedding linked information in the reporting system, and offering additional microlearning opportunities. Attendance of synchronous group meetings is a long-standing challenge in home care, where teams include many part-time and casual members with multiple employers and highly varied schedules. Further, PSWs are geographically dispersed, often rely on public transportation, and must manage unexpected client needs that take priority. This preliminary evaluation of the screening tool focused on feasibility. Future evaluation should address how effectively the screening tool identifies potential risks. Finally, while perspectives from two client partners influenced intervention design, it was beyond the scope of this project to solicit feedback from clients who participated in screening or were engaged in follow-up related to reported incidents.
Conclusion
Throughout health care, workplace violence and harassment are too often perceived as “part of the job” and not worth reporting. A first step in addressing these incidents is to give them visibility. This pilot presents a template and tools (policy, educational content, screening tool, and a low-barrier reporting system) designed to promote a culture of reporting. Multiple pieces of complementary evidence suggest that this intervention was effective in changing team culture and creating visibility surrounding workplace violence and harassment. The evaluation identified a need for continued conversation around the value of reporting, even when one has adequately managed a challenging situation, to support colleagues’ responses in similar situations. Occupational health practitioners may consider applying this approach and tools to contribute to a culture shift focused on de-normalization of workplace violence across the homecare sector.
Applications to Professional Practice
Workplace violence and harassment are commonplace for healthcare workers and most incidents are unreported. Normalization of these experiences, lack of confidence in reporting systems, and fear of the consequences of reporting contribute to the invisibility of these experiences. These challenges are exacerbated in homecare settings, and for precarious workforces including Personal Support Workers (PSWs). To enhance visibility and create a more open reporting culture that de-normalizes violence and harassment, we created and implemented an intervention combining policy changes, a novel pre-visit screening tool, education, and end-of-visit reporting with a team of PSWs working in homecare. Multiple pieces of complementary evidence suggest that this was effective at changing team culture, promoting sharing of incidents, and client-specific strategies for managing challenging situations. Occupational health practitioners may consider applying this approach and tools to contribute to a culture shift focused on de-normalization of workplace violence across the homecare sector.
Footnotes
Acknowledgements
The authors thank Lakshmi Venkatesan for her contributions to survey preparation and data collection and Simran Baliga for data collection assistance.
Author Contributions
E.C.K., J.C., and A.B. led the design and implementation of the intervention. E.C.K. and S.M.M. designed the evaluation, which was conducted by E.C.K., M.B.M., T.A.V.B., and S.M.M. with support and input from J.C. and A.B. All authors contributed to the analysis of findings and to writing the manuscript, have reviewed and approved the final version, and agree to be accountable for the work.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors are employed by the organization at which the quality improvement initiative was conducted.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support was provided by the Centre for Research Expertise in Occupational Disease at the University of Toronto, which is funded by the Ontario Ministry of Labour, Training and Skills Development.
Human Right
Human subjects review was not required for this quality improvement project.