
Abstract
Background:
Cardiovascular events are known to be the leading cause of death among on-duty firefighters. Implementing fitness standards may help reduce the incidence of cardiovascular deaths; however, standards vary between firefighter type and states. We aimed to investigate the rate of cardiovascular events among firefighters across states.
Methods:
Using publicly available data from the United States Fire Administration, we explored the rates of cardiovascular deaths between firefighter type (e.g., career, volunteer, and wildland) and state. Specifically, we examined rates of cardiovascular deaths between California and Tennessee, which have fitness standards for all firefighters, and New York, which does not have fitness standards for volunteer firefighters. We used descriptive statistics and trend analysis to examine the data.
Findings:
Most cardiovascular events occur among volunteer firefighters (60.6%, n = 877). Volunteer firefighters had 7.5 (95% CI = [4.8, 11.7], p < .001) greater odds of cardiovascular events compared to wildland firefighters, who had the lowest incidence of cardiovascular events (1.7%, n = 24). New York reported the most cardiovascular events (n = 161), primarily among volunteer firefighters (73.9%, n = 119). After the passage of legislation mandating fitness standards in California, a downtrend in the number of volunteer firefighter fatalities is observed. However, a null effect was observed in Tennessee after the passage of similar fitness standards as in California.
Conclusions/Applications to Practice:
Volunteer firefighters are significantly more likely to die of a cardiovascular event than career and wildland firefighters, both of which have stricter fitness standards. However, the effect of legislation mandating stricter fitness standards among volunteers did not produce a clear benefit for preventing fatalities. Nurses need to promote cardiovascular health among volunteer firefighters.
Keywords
Background
Cardiovascular events are the leading cause of death among firefighters in the United States and disproportionately occur around fire suppression duties despite these duties accounting for less than 5% of total occupational time (Kales et al., 2007; Soteriades et al., 2011). During fire suppression activities, high ambient temperatures, extreme physical exertion, noxious air pollutants, and psychological stress heightened sympathetic activity, induce ischemia, and propagate coagulation, which are triggers for cardiovascular events (Haller & Smith, 2019). Fitness testing and cardiovascular health assessments may be an effective strategy to identify firefighters at risk of cardiovascular events (Fortier et al., 2022).
In the United States, fitness testing requirements differ based on the type of firefighter: volunteer, career, or wildland professionals (Fahy et al., 2022). Volunteer firefighters volunteer their time for little to no pay and typically serve rural and suburban communities. Volunteers make up the majority (~65%) of firefighters in the United States (Fahy et al., 2022). Since volunteer firefighters are volunteers, they are exempt from Occupational Safety and Health Administration (OSHA) regulations (OSHA; CFR1910.156. section b, part 2), which mandates firefighters be physically fit to perform their duties (Wimberley, 2016). It is estimated that approximately 30% of volunteer firefighters in the United States undergo a fitness assessment, which can vary significantly from a simple medical evaluation to a standardized assessment (National Fire Protection Association, 2020). In contrast, career firefighters earn compensation for their service and protect more densely populated areas. OSHA and the National Fire Protection Association Standard 1582 mandate fitness testing for career firefighters (National Fire Protection Association, 2013). Approximately 85% of career firefighters in the United States undergo a fitness assessment (National Fire Protection Association, 2020). Wildland firefighters also earn compensation and protect communities from wildfires during the summer season. Wildland firefighters have the most rigorous fitness assessment as they must undergo an extremely challenging Work Capacity Test (e.g., a 3-mile hike with a 45-pound pack within 45 minutes) annually (Petersen et al., 2010).
In the last 20 years, some states have passed legislation mandating volunteer firefighters undergo fitness testing similar to career and wildland firefighters. The objective of this legislation is to protect firefighters and ensure their competence when completing their duties. In 2002, California passed Senate Bill 1207 mandating volunteer firefighters to undergo the same physical ability test as career firefighters. Similar legislation was enacted in Tennessee in 2009.
The presence of legislation mandating physical fitness testing for firefighters varies across the United States, and this inconsistency provides a unique opportunity for comparative analysis. By examining fatality rates in states that differ in their approach to legislating fitness testing, we can potentially discern the impact and effectiveness of such laws. The primary aim of this analysis was to scrutinize the incidence of cardiovascular events among different types of firefighters—volunteer, career, and wildland—and to compare these rates across states that do and do not require mandated fitness testing for volunteer firefighters. This study particularly focused on California, which instituted physical fitness standards for its volunteer firefighters in 2002, and Tennessee, which followed similar requirements in 2009. These states were contrasted with New York, a state without any mandated physical fitness requirements for volunteer firefighters. The selection of these specific states allows for an in-depth look at the potential correlations between mandated fitness testing and the rate of cardiovascular incidents among firefighters. By analyzing the data from these differing legislative landscapes, the research aims to offer insights into the possible protective effects of fitness requirements on firefighter health and safety.
Methods
Study Design
This is a retrospective analysis of publicly available data. Since the data contains no protected health information, this research was considered to not be human subjects research and therefore not required to undergo review by the institutional review board. All analyses were completed at the University of Rochester.
Firefighter Mortality Data
Data was extracted from the United States Fire Administration, Firefighter Fatalities in the United States database (https://apps.usfa.fema.gov/firefighter-fatalities/) on June 28, 2023. The purpose of the database is to be a transparent source of data regarding firefighter fatalities. Data is added to the database by individual fire departments and reviewed by the United States Fire Administration. Note, the definition of a firefighter fatality changed in 2003 when the Hometown Heroes Act (HHA) included any firefighter that died within 24 hours of a shift where “nonroutine stressful or strenuous” physical activity was performed. Before 2003, firefighters who died within 24 hours of completing a shift were not considered line-of-duty fatalities unless the firefighter reported symptoms during their shift. Data included are the date of the incident, date of death, age, classification (volunteer, career, and wildland), cause of fatal injury (e.g., stress/overexertion), nature of fatal injury (e.g., cardiovascular event), task during the fatal injury, and the city and state of the firefighter’s department.
After extracting the data, we removed cases that (1) occurred before January 1, 1990 (n = 13 cases) due to a lack of systematic reporting in the database, (2) occurred in New York City on September 11, 2001 (n = 346 cases), and (3) occurred due to COVID-19 (n = 99 cases) between 2020 and 2023 to remove historical bias in the data. In total, this left 3,184 cases of firefighter fatality over a 31-year period (1990–2021).
Data Cleaning
For this analysis, we simplified the classification of firefighters. Volunteer firefighters included only those considered to be volunteers. Career firefighters included those considered career as well as industrial, paid-on-call, and part-time (paid). Wildland firefighters included those who were full-time, part-time, and wildland contractors. We did not adjust our analysis for missing data.
State Fitness Requirements
We identified 21 states with OSHA-approved state plans (https://www.osha.gov/stateplans/), and used Law ChatGPT 1 (https://lawchatgpt.com/) to systematically analyze each OSHA-approved state plan for provisions for volunteer firefighters. We used the following search terms: “volunteer firefighter,” “fitness test,” “fitness testing,” “fitness examination,” “physical fitness,” “requirement,” and “standard” within Law ChatGPT to review the state plans. Law ChatGPT utilizes OpenAI’s (see Note 1; San Francisco, CA) natural language processing and machine learning algorithms to review legislation and create a layman summary. A recent paper demonstrated that Law ChatGPT adequately summarized law documents related to employee benefits and torts, like the documents we reviewed (Choi et al., 2023).
We identified California, Tennessee, Washington, Oregon, Michigan, and Minnesota as having state legislation mandating some form of fitness testing or physical examination for volunteer firefighters. The latter (e.g., Washington, Oregon, Michigan, and Minnesota) either enabled municipalities to enact fitness requirements or required physical examination for compensation coverage or pension but did not directly specify fitness testing requirements for volunteers. The former, California (Title 8, Cal-OSHA, enacted January 1, 2002) and Tennessee (Title 4, Chapter 24, Firefighting Training and Standard, enacted January 1, 2009) had clear expectations that volunteer firefighters meet the same fitness requirements as career firefighters. Interestingly, California and Tennessee differ in the density of volunteers (California 54.6%, Tennessee 86.9%) and career firefighters (California 45.4%, Tennessee 13.0%) (United States Fire Administration, n.d.). The 7-year time difference in which their respective legislation was enacted (California 2002; Tennessee 2009) enabled us to examine the potential impact of legislation for each state.
To compare, we assessed data from New York, which does not have a physical fitness requirement for volunteer firefighters but does have a physical fitness requirement for career firefighters (Part 426, Minimum Standards for Firefighting Personnel). Like Tennessee, New York is largely volunteer-based (5.9% career firefighters, 94.2% volunteer) but has a large urban-rural interface like California.
Definitions of Fitness Requirements
Most fitness tests assess cardiorespiratory fitness, muscular strength and endurance, and flexibility (International Association of Fire Fighters [IAFF] & International Association of Fire Chiefs [IAFC], 2018). The most common and standardized fitness test accepted by both volunteer and career fire departments in California and Tennessee includes the Candidate Physical Ability Test (CPAT) (IAFF & IAFC, 2018). The CPAT includes eight separate events: stair climb, hose drag, equipment carry, ladder raise and extension, forcible entry, search, rescue drag, and ceiling breach and pull, which must be completed by the firefighter within a span of 10 minutes and 20 seconds. During the CPAT, the firefighter must wear a helmet, gloves, and 50-pound weighted vests, designed to simulate the weight of firefighter personal protective equipment. In addition, for the stair climb portion of the CPAT, the firefighter must also carry an additional 25 pounds, to simulate the carrying of a hose pack into a high-rise fire. The physical fitness requirements for wildland firefighters are more rigorous. Wildland firefighters must complete the Work Capacity Test which requires wildland firefighters walk 3 miles with a 45-pound pack within 45 minutes.
Data Analysis
Descriptive data are reported as means and standard deviations. We used logistic regression with simple contrast to examine the odds ratio of cardiovascular events between career and volunteer firefighters compared to wildland firefighters. We used wildland firefighters as the reference because they have the strictest fitness testing requirements (Petersen et al., 2010). One-way ANOVA was used to compare the mean age at the time of the fatal event across volunteer, career, and wildland firefighters. Comparisons between states and across years were used to assess the impact of state-wide physical fitness requirements for career, volunteer, and wildland firefighters. All analyses were completed in SPSS (see Note 1; Version 29; IBM, Armonk, NY).
Results
Overview
Between January 1, 1990, and December 31, 2021, 3,184 firefighter fatalities were reported in the national database, which includes all fatal deaths. The year 1999 both had the highest number of fatalities (n = 136), followed by the year 2007 (n = 125). The average number of fatalities was (99.5 ± 17.4) firefighters per year. Figure 1 depicts the general trend of fatalities among all firefighters and stratified by volunteer, career, and wildland firefighters. Approximately half (52.4%, n = 1,669) of all fatalities were among volunteer firefighters, compared to career firefighters (39.9%, n = 1,272) and (5.9%, n = 187) wildland firefighters. Most of the fatal events occurred on-scene (45.4%, n = 1,444) or responding to the scene (16.2%, n = 515). Physical stress and overexertion were the precursors to most fatalities (47.8%, n = 1,523). New York had the greatest share of firefighter fatalities (n = 291, 9.1%), followed by Pennsylvania (n = 254, 8.0%) and California (n = 194, 6.1%). Cardiovascular events were the leading cause of death, responsible for 45.5% (n = 1,449) of all firefighter fatalities. Cardiovascular events were responsible for 52.5% (n = 877) of volunteer firefighter fatalities, 40.5% (n = 515) of all career firefighter fatalities, and 12.8% (n = 24) of wildland firefighter fatalities (p < .01).
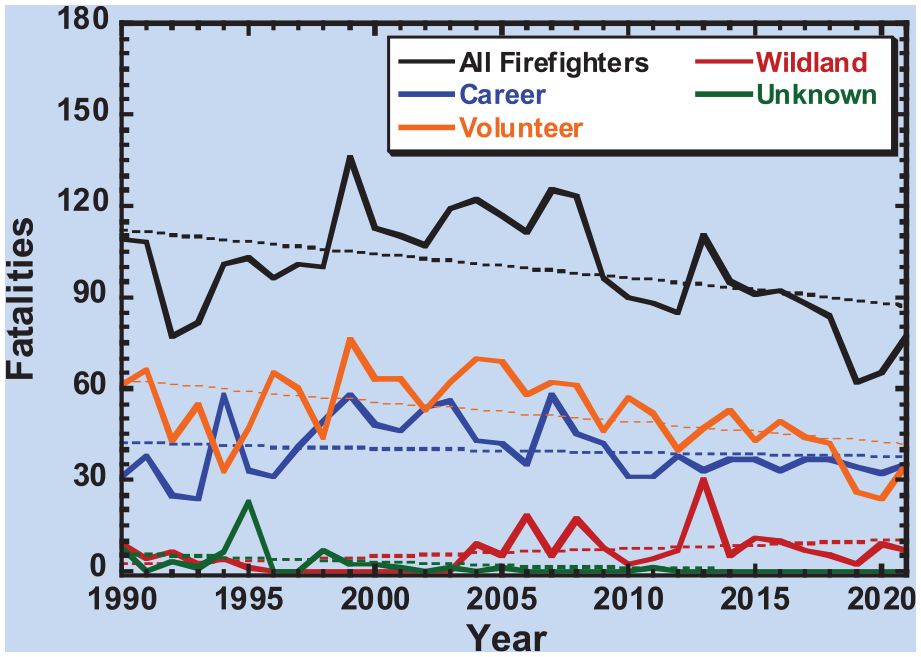
Number of Firefighter Fatalities From 1990–2021.
Fatal Cardiovascular Events
Volunteer firefighters experienced the most fatal cardiovascular events (60.6%, n = 877), followed by career firefighters (35.5%, n = 515) and wildland firefighters (1.7%, n = 24) (p < .01). Figure 2 depicts the overall trend in the number of cardiovascular deaths between volunteer, career, and wildland firefighters. Overall, the number of cardiac deaths has declined among volunteer firefighters but has steadily risen among career firefighters. When contrasted with wildland firefighters, career firefighters had 4.6 (95% CI = [3.0, 7.2], p < .001) greater odds of cardiac deaths, and volunteer firefighters had 7.521 (95% CI = [4.8, 11.7], p < .001) greater odds of cardiac deaths.
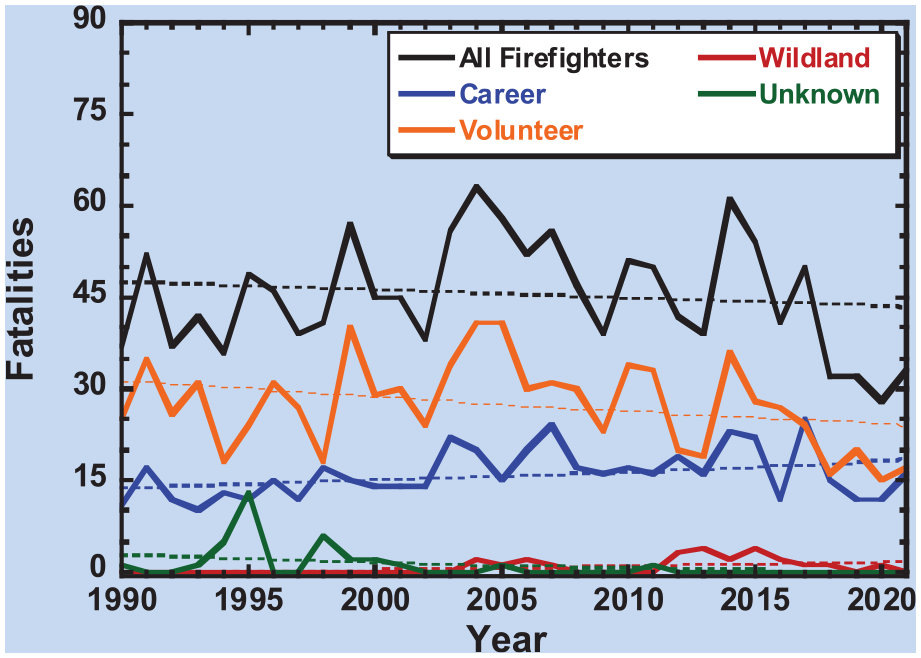
Number of Cardiovascular Fatalities From 1990 to 2021 Across Firefighter Type.
The supermajority of cardiac deaths was due to stress and overexertion (96%, n = 1,391). Of the firefighters’ duties during the fatal cardiovascular events, 27.1% (n = 392) occurred on-scene of a fire, 12.4% (n = 180) occurred responding to a call, and 18% (n = 261) occurred after or returning from a call.
The mean age of a firefighter experiencing a cardiovascular event was 52.71 ± 11.84 years. Volunteer firefighters were the oldest at the time of the cardiovascular event (55.49 ± 12.31 years, n = 854) compared to career (48.40 ± 9.38 years, n = 504) and wildland firefighters (48.26 ± 11.96 years, n = 23) (p < .001). Figure 3 depicts the mean age of firefighters at the time of fatal cardiovascular events among all firefighters as well as stratified by volunteer and career. Wildland firefighters were excluded from the figure due to the low count. As observed in the figure, the mean age at the time of a fatal cardiovascular event is rising among both volunteer and career firefighters.
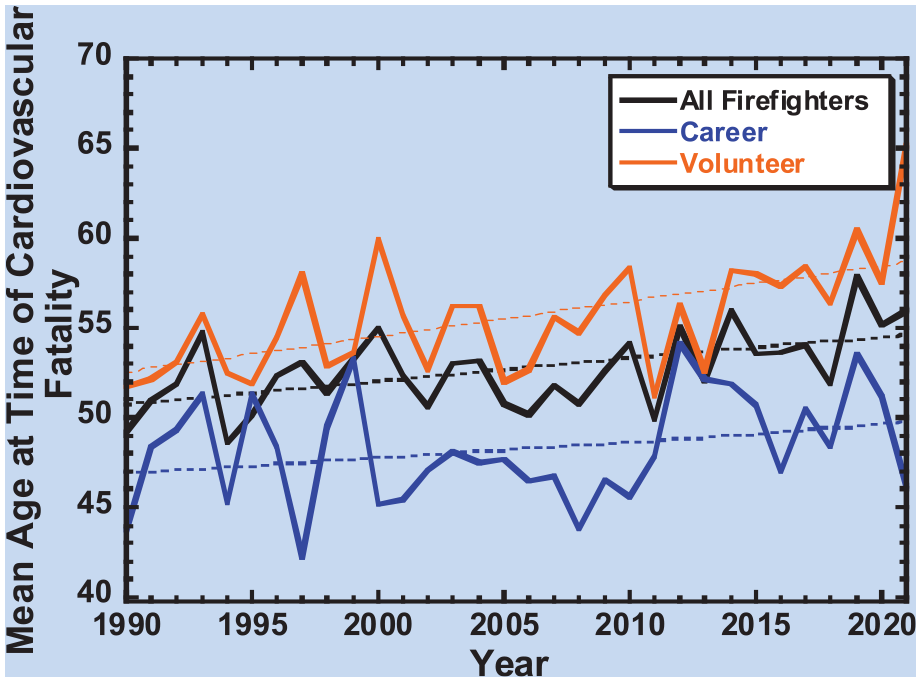
Mean Age at Time of Cardiovascular Fatalities From 1990–2021 Across Firefighter Type.
State Analysis
During the study period, New York had the greatest share of cardiovascular events. New York reported 161 cardiovascular events primarily among volunteer firefighters (73.9%, n = 119), followed by career (21.7%, n = 35) and wildland (0.6%, n = 1) firefighters (unknown 3.7%, n = 6). In contrast, California reported 59 cardiovascular events during the study period, and many cardiovascular events occurred among career firefighters (66.1%, n = 39) followed by volunteer (20.3%, n = 12) and wildland (11.9%, n = 7) firefighters (unknown 1.7%, n = 1). Tennessee (1.7%, n = 25) had cardiovascular events primarily among career (52%, n = 13) followed by volunteer (28%, n = 7) and wildland firefighters (4%, n = 1) (unknown 16%, n = 4). Figure 4 depicts the geographical variation in cardiovascular events among firefighters across states.

Number of Fatal Cardiovascular Events Among All Firefighters, Then Stratified by Volunteer and Career Firefighters.
New York consistently had the highest amount of firefighter fatalities due to cardiovascular events during the entire study period. After the passage of California (Title 8, Cal-OSHA) in 2002, volunteer firefighter fatalities declined by 40% (1990–2001 0.5 fatal cardiovascular events per year; 2002–2021 0.3 fatal cardiovascular events per year). In contrast, volunteer firefighter fatalities declined by 27.8% in New York over the same period (1990–2001 4.5 fatal cardiovascular events per year; 2002–2021 3.25 fatal cardiovascular events per year) (p < .05). After the passage of Tennessee (Title 4, Chapter 24) in 2009, volunteer firefighter fatalities rose by 9.6% (1990–2008 0.21 fatal cardiovascular events per year; 2009–2021 0.23 fatal cardiovascular events per year). In contrast, volunteer firefighter fatalities declined by 43.9% in New York over the same time (1990–2008 4.53 fatal cardiovascular events per year; 2009–2021 2.54 fatal cardiovascular events per year) (p < .05). Figure 5 shows the trend in volunteer and career firefighter fatalities in New York, California, and Tennessee from 1990 to 2021.
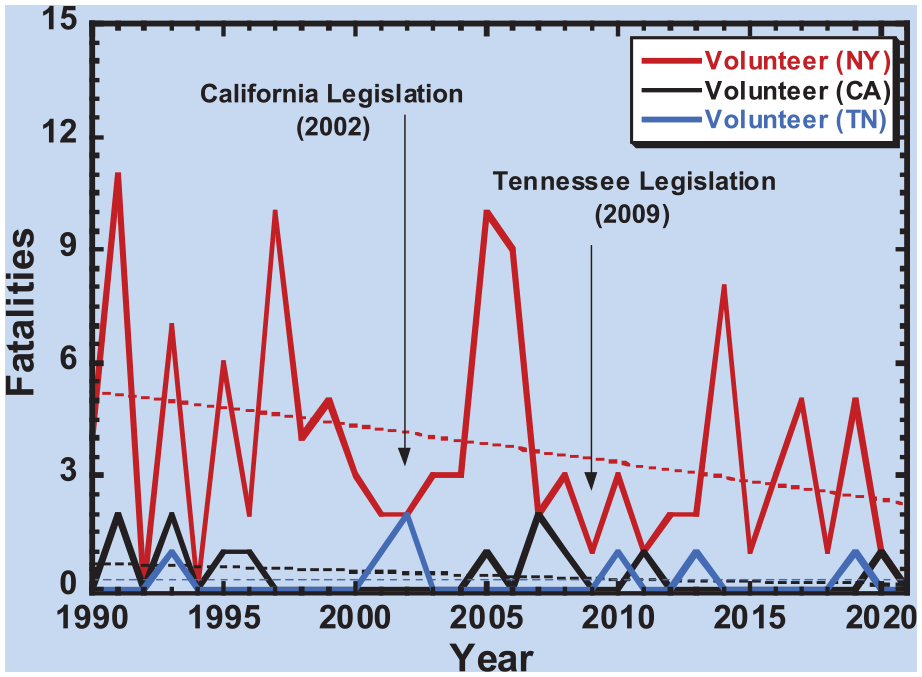
Number of Cardiovascular Fatalities From 1990 to 2021 Among Volunteers Across the States of New York, California, and Tennessee.
Discussion
Our results demonstrate that volunteer firefighters are most susceptible to cardiovascular events and that legislation aimed at mandating fitness requirements has produced mixed results. Ample research demonstrates that fire suppression activities are strenuous on the cardiovascular system and precipitate cardiovascular events (Dzikowicz & Carey, 2019, 2020, 2021, 2023). Our lab has previously published reports demonstrating that arrhythmogenic ectopy, ventricular hypertrophy, electrical-mechanical dyssynchrony, and autonomic dysregulation during strenuous activity like firefighting are precursors to cardiovascular events among firefighters (Dzikowicz & Carey, 2019, 2020, 2021, 2023). Smith and colleagues (2022) have recently demonstrated that even subclinical cardiac dysfunction is associated with reduced cardiorespiratory fitness and increased risk for cardiovascular events among firefighters.
We found that volunteer firefighters are the least likely to undergo any type of fitness testing and therefore most prone to cardiovascular events. The data presented here demonstrate that volunteers are significantly more likely to die of a cardiovascular event than career and wildland firefighters, both of which have stricter fitness standards. Routine fitness tests and assessment of exercise training routines may be able to screen out firefighters who are more likely to experience a cardiovascular event (Fortier et al., 2022). Martin et al. (2019) recently showed that nearly 70% of volunteer firefighters harbor cardiovascular risk factors including obesity, hypertension, and hypercholesterolemia. Morris et al. (2022) highlighted that volunteer firefighters have worse health and physical fitness profiles than career firefighters yet perform similar duties.
To protect volunteer firefighters and ensure their fitness for duty, California and Tennessee have implemented fitness requirements for volunteer firefighters. We found mixed effects of the legislation on firefighter fatalities. While we saw a substantial decline in the number of volunteer firefighter fatalities in California after the passage of their fitness requirement legislation, a similar pattern was observed in New York which did not pass such legislation. In comparison, Tennessee saw a rise in the number of volunteer firefighter fatalities after the passage of their fitness requirement legislation. There are many potential reasons for the mixed results including the relatively low number of fatalities in both California and Tennessee, poor fire department compliance with fitness standards, high rates of cardiometabolic risk factors specifically age harbored, greater awareness and education on heart health, and implementing workplace health and safety programs (Wimberley, 2016). For example, the National Volunteer Fire Council launched the Heart-Healthy Firefighter Program in 2003 to combat the number of fatal cardiac events among firefighters. Exploration of data in more detail will be necessary in order to fully understand the effects of these factors and decipher the impact of state-wide legislation.
While the protection of lives should be of the utmost importance, implementation of fitness standards may be detrimental to volunteer fire departments. Stocker (2004) noted that after the implementation of OSHA Standard 29 CFR 1910.134 mandating that firefighters entering a fire wear a self-contained breathing apparatus, the number of volunteer firefighters in the United States steadily declined. The reasons for the decline in the number of volunteer firefighters were the additional training, education, and time to devote to volunteering (Stocker, 2004). This is an important consideration given that 65% of firefighters in the United States are volunteers, and the volunteer force is declining (United States Fire Administration, n.d.). In addition, physical fitness requirements are difficult to enforce. For example, in Connecticut, volunteer firefighters sued the Connecticut Department of Labor over the state’s OSHA-sponsored plan and won their case in the State’s Supreme Court in 2011 (Mayfield v. Goshen Volunteer Fire Company, Inc). In this case, the volunteer firefighters demonstrated that they cannot be subject to OSHA regulations because they are not political subdivisions. Thus, further examination of the impact of these physical fitness requirements on the recruitment and retention of volunteer firefighters is needed to fully understand their impact on firefighter fatalities and the larger communities.
There are a number of limitations to our analysis. First, heterogeneity exists between state laws regarding firefighter physical fitness requirements making it challenging to comprehensively understand the effect of legislation on fatalities. Second, while state laws may require physical fitness requirements, fire department compliance is unclear. Third, individual-level data regarding comorbidities, biological sex, and other factors associated with cardiovascular events were absent in the database.
The findings of this study underscore the crucial role that occupational health nurses play in the health and safety of firefighters, a group that may not consistently have access to a wide range of health care providers. These nurses are often the primary health professionals firefighters interact with on a regular basis, placing them in a unique position to influence positive health outcomes (Wimberley, 2016). Given the diversity in physical fitness standards among fire departments, occupational health nurses have a responsibility to familiarize themselves with the specific requirements and challenges faced by the firefighters they serve. By doing so, they can deliver targeted education and support, helping to mitigate the risks associated with firefighting duties. Occupational health nurses are also well-positioned to lead and advocate for comprehensive wellness programs. They can champion initiatives such as fitness programs specifically designed for the physical demands of firefighting, thereby contributing to the reduction of duty-related morbidity and mortality. Moreover, these nurses should be informed about and engage with broader initiatives focused on firefighter health, such as the Heart-Healthy Firefighter Program and the NIOSH Total Worker Health Program (National Volunteer Fire Council, 2003; Tamers et al., 2019). Participation in such programs allows occupational health nurses to align their efforts with national movements aimed at promoting cardiovascular health and overall well-being among firefighters. In summary, the importance of occupational health nurses in the firefighting community cannot be overstated.
Conclusions
In the United States, cardiovascular events were the leading cause of volunteer firefighter fatalities between 1990 and 2021. Almost all cardiovascular events were related to stress and overexertion and occurred in correspondence to fire suppression activities. New York State had the highest number of overall firefighter fatalities and the highest rate of cardiovascular fatalities among volunteer firefighters. Implementation of state laws in California and Tennessee to mandate physical fitness testing among volunteer firefighters has had an inconclusive effect on reducing fatalities among volunteer firefighters.
There has been growing interest in occupational health practices for firefighters because of their risks for death while on duty as well as long-term health risks. Research like this analysis, which includes a national database of up-to-date data on firefighter fatalities, provides occupational health nurses the current evidence to improve their practice. The most important finding from this research is that among the different causes of death, cardiovascular events were the leading cause of volunteer firefighter fatalities over a 30-year period. Almost all cardiovascular fatalities were related to stress and overexertion and occurred in correspondence to fire suppression activities. Thus, occupational health nurses can better advise firefighters who are at great risk of cardiovascular events with prevention strategies.
Footnotes
Author Contributions
Dillon J. Dzikowicz designed the work; acquired, analyzed, and interpreted the data; drafted the manuscript; approved the final version of the publication; and agreed to be accountable for all aspects of the work. Sankalp Babarao Saoji interpreted the data; reviewed the manuscript, approved of the final version of the publication; and agreed to be accountable for all aspects of the work. Wai Cheong Tam interpreted the data; reviewed the manuscript, approved of the final version of the publication; and agreed to be accountable for all aspects of the work. Wendy M. Brunner interpreted the data; reviewed the manuscript, approved of the final version of the publication; and agreed to be accountable for all aspects of the work. Mary G. Carey interpreted the data; reviewed the manuscript, approved of the final version of the publication; and agreed to be accountable for all aspects of the work.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects
This study used publicly available data and was deemed not human subjects’ research.