
Abstract
In this issue, Sacheck and Hall discussed the key findings from the Final Report “Fitness Measures and Health Outcomes in Youth” developed by an expert committee appointed by the Institute of Medicine in 2011 and published in 2012. The findings from this report are more valuable when interpreted together with those from the EU-funded ALPHA project (conducted from 2007 to 2010). The ALPHA project aimed to provide an evidence-based set of valid, reliable, feasible, and safe field-based fitness tests for the assessment of health-related physical fitness in youth to be used in public health monitoring in a comparable way within the European Union and around the globe. The ALPHA team conducted 4 reviews (3 of them systematic reviews) and 11 methodological studies, tested the battery in the school setting, and had several meetings with an international expert board to further discuss the development of the work. The evidence-based ALPHA fitness test battery was finally published in 2011. Several important methodological issues related to fitness assessment and its clinical value mainly derived from this project are discussed in the present article: the ALPHA-fitness test battery; Slaughter’s equations and normalization of fat indicators by height; absolute versus relative muscular strength; physical fitness reference data; health-related fitness cut-points; Self-reported fitness assessment: The International FItness Scale-IFIS; and fitness assessment in preschoolers: The PREFIT project.
“Although the IOM report on fitness in youth is a key document in this field, its findings should be interpreted together with those of another major project, the EU-funded ALPHA . . .”
Current evidence strongly supports the idea that physical fitness is a powerful marker of health in youth. 1 This notion is consistent regardless of body weight status, and it has recently been proposed that physical fitness also plays a key role in metabolic health of the obese phenotype and its future prognosis. 2 In this issue, Sacheck and Hall did an in-depth review of the key findings from the Final Report “Fitness Measures and Health Outcomes in Youth” developed by an expert committee appointed by the Institute of Medicine (IOM) in 2011 and published in 2012. 3 Although the IOM report on fitness in youth is a key document in this field, its findings should be interpreted together with those of another major project, the EU-funded ALPHA (Assessing Levels of Physical Activity and Fitness) project, which was conducted and had its results published earlier than the IOM report. Taken collectively, the findings from both ALPHA and IOM projects provide the most comprehensive and updated understanding of key methodological issues when assessing fitness in youth and their clinical value.
The ALPHA Project
The ALPHA project was funded by the European Commission from 2007 to 2010 with the aim of providing a set of instruments for assessing different physical activity domains as well as health-related physical fitness in a comparable way (see Web site at: http://www.thealphaproject.net). Particularly, the aim of the Work Package 6 (Assessing Health-Related Physical Fitness) was to provide an evidence-based set of valid, reliable, feasible, and safe field-based fitness tests for the assessment of health-related physical fitness in children and adolescents to be used in public health monitoring in a comparable way within the European Union and around the globe.
The ALPHA Fitness Test Battery for Children and Adolescents
There are more than 15 different fitness test batteries to assess fitness in youth (see table 1 in Castro-Piñero et al 4 ), and for some of the fitness components such as cardiorespiratory fitness, there are more than 10 different field-based tests. It was unknown which of the existing tests were more valid, reliable, and related to future health. To address this need, we set up a roadmap that ended with an evidence-based fitness test battery, the so-called ALPHA health-related physical fitness test battery for children and adolescents. A detailed description of the entire process of developing the ALPHA test battery as well as its key findings were reported in 2011. 5 In summary, we first reviewed the evidence on (1) the association between physical fitness and health in childhood and adolescence (a narrative review) 1 ; (2) the association of physical fitness in childhood and adolescence with health later in life (systematic review) 6 ; and (3) the validity 4 and reliability 7 of the available field-based fitness tests (2 additional systematic reviews). Second, we also carried out 11 methodological studies to determine the criterion validity and the reliability of several field-based fitness tests for young people (see references for these methodological studies in the ALPHA summary paper). 5 Third, we conducted a study to examine the reliability, feasibility, and safety of the evidence-based selected tests at school settings. Finally, the methods used as well as the outcomes of this work were discussed with an International Expert Board comprising Robert M. Malina from the United States, Willem van Mechelen and Han C. G. Kemper from the Netherlands, Jorge Mota from Portugal, and Kari Bø and Pekka Oja from Finland. This whole protocol is summarized in Figure 1.
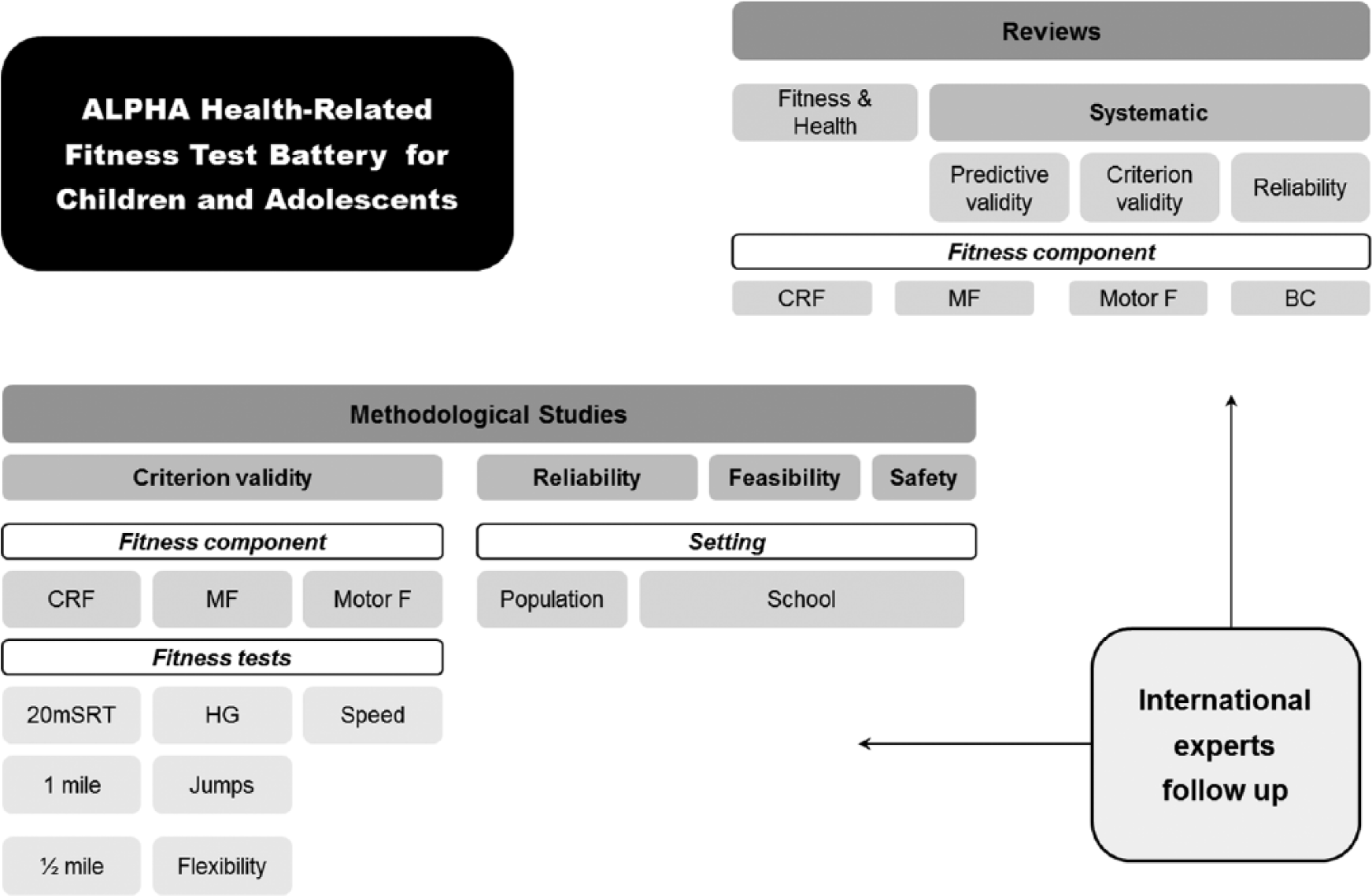
Steps During the ALPHA Project to Propose an Evidence-Based ALPHA Health-Related Physical Fitness Test Battery for Children and Adolescents.a
The final outcome was an evidence-based health-related physical fitness test battery for children and adolescents (Figure 2). The selected fitness tests were (1) the 20 m shuttle run test to assess cardiorespiratory fitness, (2) the handgrip strength and (3) standing broad jump to assess musculoskeletal fitness, (4) body mass index (BMI), (5) skinfold thickness (triceps and subscapular), and (6) waist circumference to assess body composition. In those situations when there are time or budget constraints, the authors propose the high-priority ALPHA health-related fitness test battery, which skips the measurement of the skinfold thickness because it requires more training and time than other measures, and the caliper is expensive. The time required to administer this high-priority battery to a group of 20 children by one physical education teacher is <2 hours. On the other hand, when time and budget are not so limited, the authors propose the use of an extended version of the battery, which includes all the evidence-based fitness tests plus the 4 × 10 m shuttle run test to assess speed-agility. This test was not included in the evidence-based battery because there were fewer studies on it, but the results regarding its validity, reliability, and relationship with health were promising. Figure 2 represents these 3 versions of the ALPHA health-related fitness test battery.
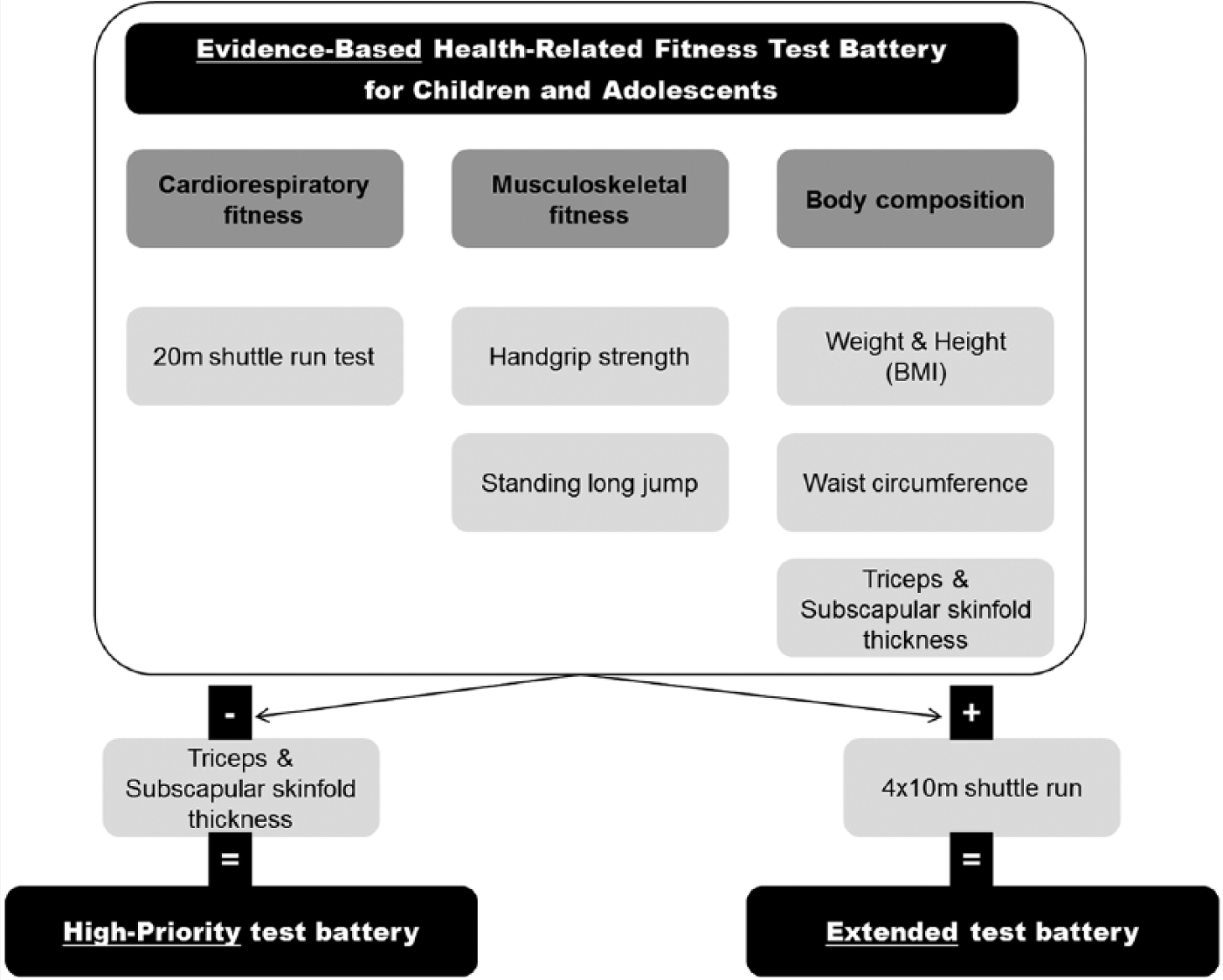
The 3 Versions of the ALPHA Fitness Test Battery for Children and Adolescents.
Body Composition: Slaughter’s Equations and Normalization of Fat Indicators by Height
In their article, Sacheck and Hall describe BMI and waist circumference as the measures recommended by the IOM report, 3 which completely agrees with the ALPHA report previously published. 5 Also in agreement with the ALPHA test battery, the IOM report recommended the assessment of skinfold thickness, and Sacheck and Hall indicated that the most-used skinfolds are triceps and subscapular skinfolds. The reason why these 2 skinfolds were selected for the ALPHA battery was because they are used in Slaughter’s equations for estimating body fat, which are the most accurate for estimating body fat in youth. 8 What is important to note is that despite percentage body fat being most commonly used as an indicator of total adiposity, it might not be the best choice. Cole et al 9 recommended not using percentage body fat as a proxy for adiposity because (1) it fails to adjust correctly for weight; dividing body fat by weight overadjusts because weight is the sum of fat mass + fat-free mass, so that percentage body fat includes fat mass in both the numerator and the denominator, complicating its interpretation; (2) weight is inappropriate as a proxy for body size. 9 Normalizing fat mass by height seems to be a much better choice, and the already well-known fat-mass index—FMI = body fat (kg)/height (m) 2 —can be a good alternative to percentage body fat.10,11
Waist circumference is also mentioned by Sacheck and Hall as an indicator of abdominal adiposity, also according to the ALPHA test battery. It is important, however, to consider that waist circumference is strongly correlated with height, so that a taller child has larger bones (both linearly and widely) and could have a larger waist circumference (ie, because of a larger pelvis) but not necessarily more abdominal adiposity. To minimize this potential error, the waist-to-height ratio has been proposed and widely used in the literature, and it might be an appropriate index for abdominal adiposity, particularly in children and adolescents because they are continuously growing.12-14 This index is not age or sex dependent, and the same cut-point can be used for everyone. The easy-to-remember 0.5 cutoff has been proposed, which could lead to the simple public health message of “Keep your waist circumference to less than half your height” (both expressed in cm). 12
Musculoskeletal Fitness: Absolute Versus Relative Strength
The association of muscular strength with health outcomes is dependent on how muscular strength is expressed—that is, in absolute versus relative (to body weight) terms. A measure of absolute strength is handgrip strength or a bench press repetition maximum (ie, they are not dependent on the person’s body weight), whereas a measure of relative strength could be any movement that requires moving the body weight against gravity such as jumps. Another indicator of relative strength would also be handgrip divided by body weight. Most of the current studies supporting an inverse association between muscular strength and cardiovascular disease risk factors in youth have been done expressing muscular strength in relative terms.15,16 Of note is that the association between muscular strength and health outcomes can be completely inverted depending on how muscular strength is expressed.17,18 This has important implications when assessing muscular strength in relation to health in youth.
Physical Fitness Reference Data in Youth
Once fitness assessment has been conducted, fitness reference data are fundamental for understanding the meaning of the results obtained, according to a specific age and sex. In our opinion, reference data are extremely valuable for healthy physical education. Reference data reported, for instance, as 10th, 20th, 30th, 40th, 50th, 60th, 70th, 80th, 90th, and 100th percentiles can be used for educational purposes and health promotion in schools and sport centers. As an example, a physical educator might perform fitness assessment, score the fitness level of every child from 1 to 10 (using the percentiles mentioned above), and then settle as a goal that every child in the class, regardless of the score obtained, should improve their fitness by 1 point (eg, from 2 to 3 = from 20th to 30th percentile) by the end of the semester. Large national or continental surveys will help provide these reference data that can be used for interpretation of fitness assessment. Examples of these surveys are the following: the NHANES (National Health and Nutrition Examination Survey) for US children and adolescents, the IDEFICS (Identification and Prevention of Dietary and Lifestyle-Induced Health Effects in Children and Infants), 19 and HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) 20 for EU children and adolescents, respectively.
Health-Related Fitness Cut-points
Health-related fitness cut-points are important because they can be used by pediatricians, physical education teachers, or other health agents as part of surveillance and/or screening systems to identify youth with poor health behaviors or cardiovascular health who could benefit from intervention programs. Whereas there seems to exist a consensus about the cardiorespiratory fitness threshold associated with cardiovascular health, 21 less information exists regarding the capacity of handgrip strength or standing long jump for detecting poor cardiovascular health in youth.
FITNESSGRAM has contributed to great advances in this area by establishing a sex- and age-specific healthy fitness zone linked to adult mortality/chronic disease risk for each fitness dimension (https://www.cooperinstitute.org/youth/fitnessgram). FITNESSGRAM actually uses the fitness measurements for diagnostics or screening. Youth receive different feedback depending on whether they are in the “Healthy Fitness Zone” or the “Needs Improvement Zone.”
Self-reported Fitness Assessment: The International Fitness Scale—IFIS
There might be a number of situations in which fitness assessment is not feasible. Examples of this are the following: large surveys with limited time for measurements; settings where there are no appropriate facilities to conduct the recommended field-based fitness tests; and limited budget, such that the equipment needed for measuring fitness cannot be bought. In these and other similar situations, a self-report physical fitness assessment would be a much better choice than no fitness assessment at all. Under the umbrella of the HELENA project, the International Fitness Scale (IFIS) was developed. 22 IFIS is composed of 5 Likert-type questions about the adolescents’ self-reported overall fitness, and its main components are cardiorespiratory fitness, muscular strength, speed-agility, and flexibility. IFIS is completed in a very short time (roughly 2 minutes) and has been shown to be a valid and reliable tool for accurately classifying children and adolescents into fitness level groups.17,22 In addition, IFIS evaluates cardiovascular disease risk factors in both children and adolescents17,22 as well as in young adults. 18 It is currently being validated in other countries. 23 IFIS is available in 9 different languages (English, German, Austrian German, Greek, Flemish, French, Hungarian, Italian, Spanish, and Swedish. IFIS is free of use and it was included in the different languages as supplementary material in the original paper published (Ref. 22); any person interested in using it is most welcome to download it directly from that reference).
Fitness Assessment in Preschoolers: The PREFIT Fitness Test Battery
Physical fitness is a health indicator in children 6 years and older, and there is no reason to believe that it might be less relevant for health in younger children. We recently conducted a systematic review aiming to describe the available field-based fitness tests in preschool children, and examine their (1) reliability, (2) validity, and (3) relationship with health outcomes. 24 The final goal was to propose a field-based physical fitness-test battery to be used in preschool children (the so-called PREFIT battery, field-based FITness testing in PREschool children aged 3 to 5 years old). The PREFIT battery is composed of the following tests: the 20 m shuttle-run test for assessing cardiorespiratory fitness, the handgrip strength and standing long-jump tests for assessing musculoskeletal fitness, and the 4 × 10 m shuttle run and the one-leg-stance tests for assessing motor fitness—that is, speed/agility and balance, respectively. Based on several pilot studies conducted by our group, adaptations and recommendations when using these tests in preschool children need to be taken into account. As an example, the initial speed of the 20-m shuttle-run test used in the original test is 8.5 km/h, which proved to be too fast for preschool children, especially for the 3-year-olds; consequently, we reduced the speed to 6.5 km/h, which after testing proved to be an optimal initial speed, leading to an average total time of the test similar to that achieved in older children and adolescents. 25 We have also proved that this text is maximal also in preschool children aged 3 to 5 years, as shown by the maximal heart rate achieved at the end of the test. 25 Additional considerations to be taken into account when using this test in preschoolers are discussed in this study.
Conclusions
The ALPHA project, conducted between 2007 and 2010, the results of which were published in 2010-2011, provided the most comprehensive information at that time about which were the most valid, reliable, and related-to-health physical fitness tests to be used in youth. The IOM report about fitness and health outcomes in youth published 1 to 2 years later arrived at identical conclusions regarding which fitness tests should be used in youth. These 2 major projects together provide solid and consistent guidelines about fitness testing in youth. Researchers and practitioners may want to follow these guidelines to obtain the most valid, reliable, and health-related fitness data and to improve future comparability of the data.
Footnotes
Acknowledgements
FBO and JRR are supported by grants from the Spanish Ministry of Science and Innovation, MINECO (RYC-2011-09011, RYC-2010-05957), and their research activity was additionally supported by the MINECO with the projects ActiveBrains (DEP2013-47540-R) and ACTIBATE (PI13/01393).