
Abstract
Background:
Chronic health conditions are highly prevalent among truck drivers due to many unique occupational and environmental stressors. Health promotion programs are shown to be effective in improving truck driver health outcomes; however, there is no research on whether such programs can increase the length of a driver’s Department of Transportation (DOT) medical certificate. The purpose of this quality improvement project was to evaluate Fit to Pass (FTP), a remotely accessible health promotion program available for truck drivers on improved health outcomes and increased DOT medical certificate length.
Method:
Program evaluation included an evaluation of the FTP coaching guide against evidence-based practice guidelines. An analysis of a limited dataset of 22 truck driver records examined the effectiveness of the program in achieving improved health outcomes and increased medical certification length.
Findings:
A review of the literature revealed three major themes: (a) motivational interviewing to increase driver intention and self-efficacy; (b) mobile health care technology to connect hard-to-reach truck drivers; and (c) effectiveness of structured multicomponent health promotion programs. After participation in FTP, truck drivers experienced a mean decrease in weight and body mass index (BMI) of 4.6 lbs and 1.3 kg/m2, respectively. The lengths of initial DOT medical certificates were compared with DOT medical certificates received at the time of recertification (post—FTP). Only eight participants had the potential for improvement in certificate length. Of those, three truck drivers achieved an increased DOT medical certificate length at the time of recertification.
Conclusion/Applications to Practice:
FTP offers tailored and comprehensive health coaching for truck drivers using current evidence-based practice guidelines to educate and reinforce healthy lifestyle habits. Analysis of a limited dataset revealed a mean decrease in BMI and a trend of increased DOT medical certification lengths after participation in FTP; however, further research with larger sample sizes is recommended.
Background
By 2030, a 6% growth rate in the trucking industry will require more than 230,000 additional drivers each year (U.S. Bureau of Labor Statistics, 2021). Deficits in the number of drivers combined with turnover due to restricted medical certification result in a driver shortage that negatively impacts the nation’s supply chain.
Commercial motor vehicle (CMV) drivers must obtain a Department of Transportation (DOT) physical exam by a certified medical examiner (CME) at least every 2 years (Federal Motor Carrier Safety Administration [FMCSA], 2019). The CME determines whether the driver is physically qualified to drive a CMV for up to 2 years using medical judgment in accordance with FMCSA regulations and guidance (FMCSA, 2019).
CMV drivers are at high risk for poor health outcomes compared with other workers due to the physical rigors and stress of driving, social isolation, low job control, erratic schedules, and long hours behind the wheel (Hege et al., 2019). The sedentary nature of the job, poor sleep hygiene, and lack of nutritious foods limit healthy behaviors (Bachmann et al., 2018; Birdsey et al., 2015). Barriers to access including lack of insurance (Apostolopoulos et al., 2013; Sieber et al., 2014), paid sick time (Bachmann et al., 2018; Peters et al., 2021), primary care providers (Sieber et al., 2014); appointment scheduling difficulties, and limited or inconveniently located parking (Bachmann et al., 2018; Peters et al., 2021) have all been reported by CMV drivers.
Obesity, smoking, hypertension, diabetes, and sleep apnea are highly prevalent among truck drivers (Bachmann et al., 2018; Robbins et al., 2020; Sieber et al., 2014; Thiese, Moffitt, et al., 2015). Eighty-eight percent of truck drivers reported at least one of three conditions: hypertension, smoking, or obesity (Sieber et al., 2014). Obesity and cigarette smoking were twice as prevalent among truck drivers compared with the general population (Sieber et al., 2014). Nearly 70% of drivers are considered overweight or obese and an additional 17% are morbidly obese (Hege et al., 2017; Sieber et al., 2014). Hypertension prevalence ranges from 18% to 48% (Bachmann et al., 2018; Ronna et al., 2016; Sieber et al., 2014; Thiese et al., 2018). Combined patterns of smoking, obesity, and hypertension are the most common modifiable risk factors for cardiovascular disease morbidity and mortality (Yandrapalli et al., 2019). Furthermore, CMV drivers with chronic health conditions are disproportionately more likely involved in preventable truck crashes and crashes with injuries (Ronna et al., 2016; Thiese et al., 2017).
Fit to Pass® ([FTP], 2021) is a remotely accessible proprietary health coaching program for truck drivers available through Espyr®, a behavioral health care organization. FTP targets modifiable risk factors related to eating habits, physical activity, sleep hygiene, and other lifestyle behaviors to ensure CMV drivers receive the optimum medical certificate length and stay on the road. Certified health coaches trained in motivational techniques work one-on-one with drivers to develop customized plans that create and reinforce healthy lifestyle habits and behaviors. The FTP health and wellness coaching guide (coaching guide) provides a structured manual designed to prepare health coaches for their role and responsibilities in improving drivers’ health both on and off the road. Health coaches are in place to help drivers build confidence; identify desires to change lifestyle habits; and provide tips and support on establishing goals; they do not prescribe individualized exercise programs, diet plans, or pharmacological treatments (FTP, 2021).
The purpose of this quality improvement project was to conduct an initial evaluation of the FTP program, including a comparison of the recommendations provided in the coaching guide with current evidence-based practice guidelines (Phase 1) and a preliminary analysis of a limited data set from a sample of drivers who have participated in the program (Phase 2). Recommendations for program improvement based on project findings were provided to administrators of the program.
Method
Evaluation of the FTP program included two phases. First, an in-depth review of the FTP coaching guide with a comparison to evidence-based practice guidelines and a literature review on health promotion programs for truck drivers was completed. The second phase included an analysis of data with recommendations for improvement in the FTP program.
Phase 1: Comparison of FTP® Guidance With Best Practice Guidelines
A review of the FTP coaching guide revealed an in-depth overview of information on the intricacies of truck drivers and recommendations for strategies to improve mental and physical health. The coaching guide was broken down into major topics including blood pressure, target heart rate during aerobic exercise, glucose control, diagnosing diabetes, and healthy eating. Evidenced-based practice guidelines referenced in the coaching guide included the American Heart Association (AHA); American Diabetes Association (ADA); National Heart, Lung, and Blood Institute (NHLBI); and the U.S. Department of Agriculture (Table 1). The references provided in each educational area were compared to current evidence-based practice guidelines by conducting a literature search and review of each topic.
Evidenced-Based Practice Guidelines Utilized in the Fit to Pass® Coaching Guide
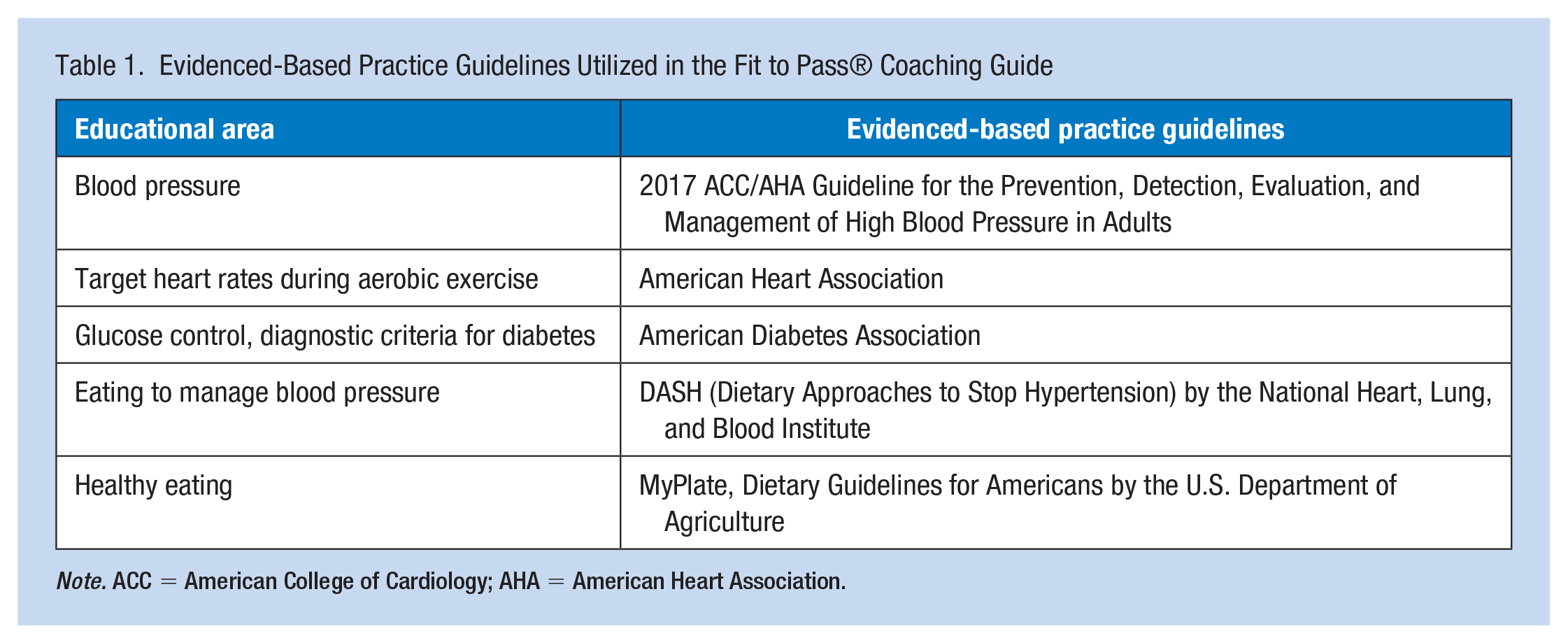
Note. ACC = American College of Cardiology; AHA = American Heart Association.
Phase 2: Preliminary Data Analysis
Design
Upon enrollment into FTP, CMV drivers receive a health kit containing a cooler bag, water bottle, workout bands, and general nutrition information. The FTP program included a combination of remote or in-person coaching sessions determined by individual needs, health-related education, unlimited access to a mobile health application, and access to mental health services from licensed behavioral health professionals. Health coaching intensifies 90 days prior to a scheduled DOT medical exam to prepare drivers and maximize health improvements (FTP, 2021).
FTP evaluation included an analysis of data from 22 truck drivers, aged 21 and older, including all genders and races. Individuals with secondary hypertension were excluded. De-identified data for analysis was provided by the FTP health coaching program manager.
Data Analysis
Descriptive statistics were used to analyze the data (Table 2). Frequencies and percentages for gender, lengths of initial DOT medical certificate, and DOT recertification lengths are presented (Table 3). The lengths of the initial medical certificate and the medical certificate received at time of recertification after participating in FTP were compared. A paired t test was used to compare pre- and post-participation body mass indexes (BMIs). All data analyses were performed using SPSS for Mac Version 29.
Characteristics of Truck Drivers Participating in Fit to Pass®
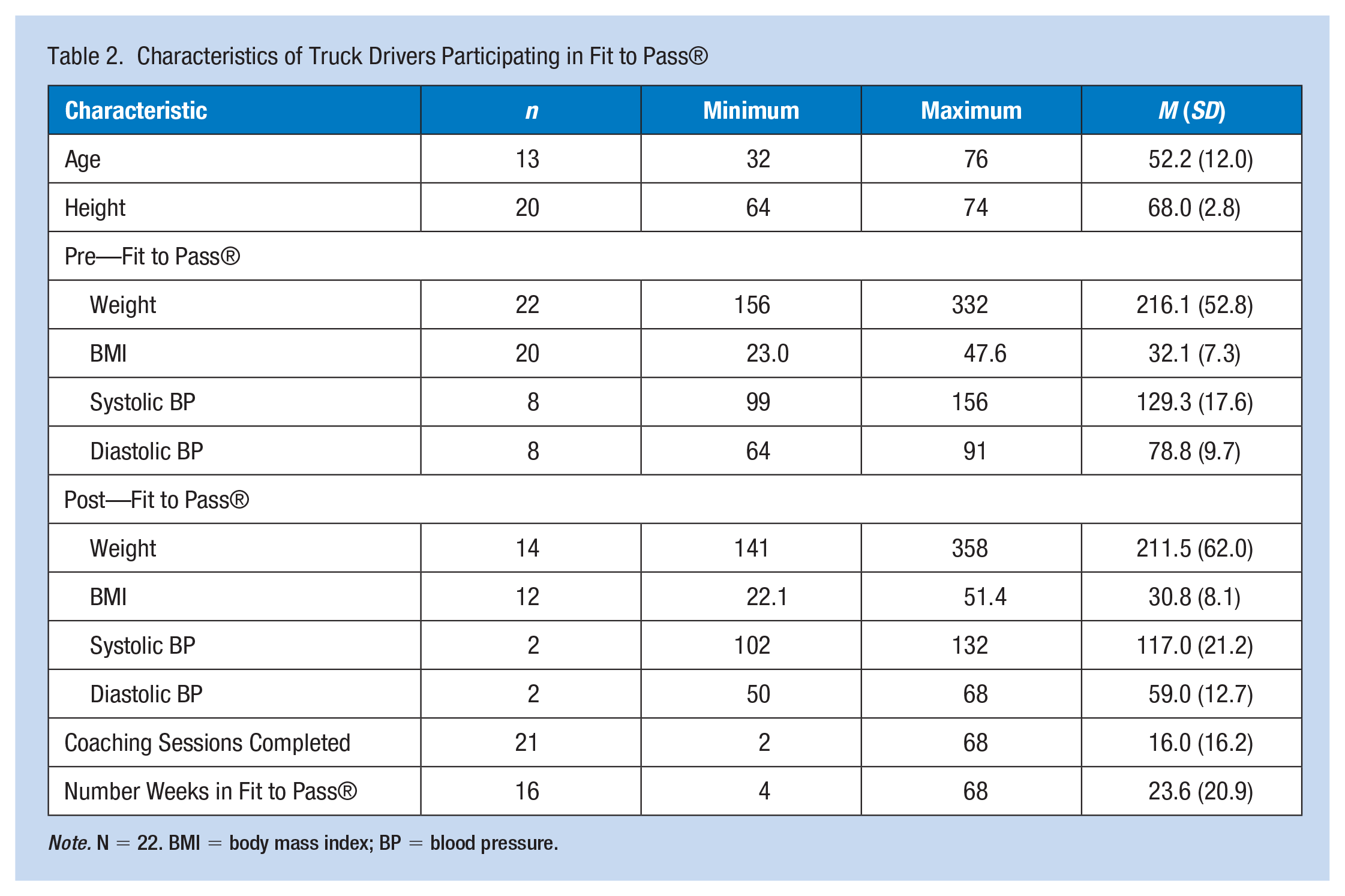
Note. N = 22. BMI = body mass index; BP = blood pressure.
Frequencies of Gender and Lengths of DOT Medical Certificates for Truck Drivers Participating in Fit to Pass®
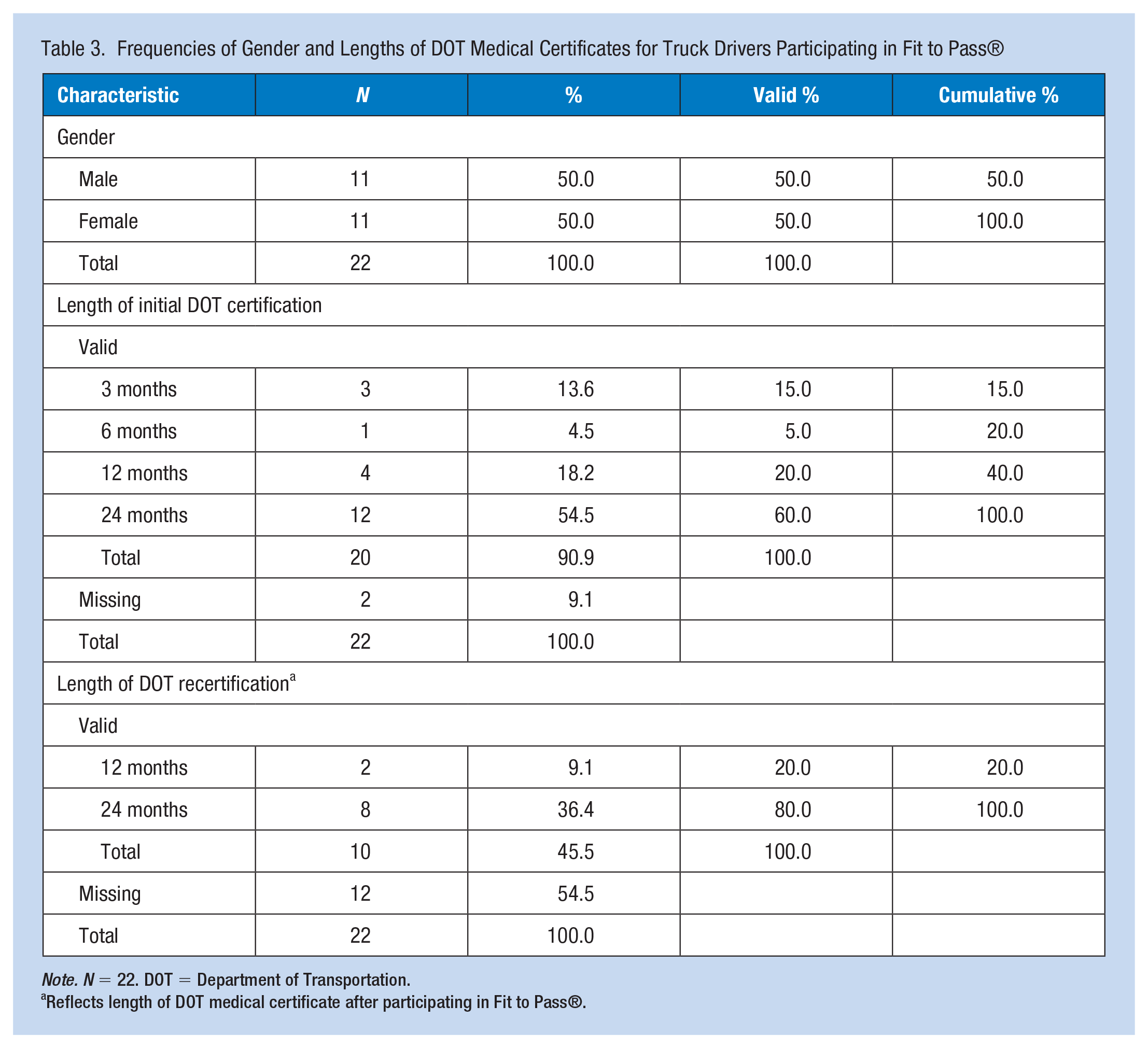
Note. N = 22. DOT = Department of Transportation.
Reflects length of DOT medical certificate after participating in Fit to Pass®.
Results
Phase 1: Comparison of FTP Guidance With Best Practice Guidelines
Review of the Literature
A literature search on health promotion programs for truck drivers was conducted using CINAHL and PubMed electronic databases. Boolean search strings included “health promotion AND long-haul truck drivers OR truck drivers” and “truck driver health AND wellness program.” Electronic database filters included (a) peer-reviewed, (b) English language, (c) full-text, and (d) articles published in the last 10 years. After initial searches of the databases for articles published in the last 5 years did not produce sufficient results, the search was extended to include the past 10 years. The titles and abstracts of all articles were scanned to identify content-specific inclusion and exclusion criteria. Inclusion criteria included articles related to health promotion interventions or wellness programs targeted toward truck drivers in the United States or internationally. Exclusion criteria included (a) studies related to bus transportation, passenger transit drivers, or professional car drivers; (b) studies related to the sexual health of drivers; and (c) opinion-based articles. All the articles reviewed were related to the structure, process, or outcomes of health promotion programs for truck drivers. Synthesis of evidence revealed three major themes: (a) motivational interviewing to increase driver intention and self-efficacy; (b) mobile health care technology to connect hard-to-reach truck drivers; and (c) effectiveness of structured multicomponent health promotion programs.
Motivational Interviewing
Truck drivers desire good health and are aware that stress and unhealthy lifestyle behaviors impact overall health (Greenfield et al., 2016; Passey et al., 2014). However, there is a disconnect between self-awareness and driver’s efforts at improving health (Greenfield et al., 2016; Lemke & Apostolopoulos, 2015; Passey et al., 2014). Strategies to increase self-awareness and intention can reduce self-limiting barriers to realistic goal achievement (Yen et al., 2019). Motivational interviewing by health coaches was identified as an intervention used to increase truck drivers’ self-efficacy and potentially improve their intention to pursue healthy lifestyle behaviors (Greenfield et al., 2016; Passey et al., 2014; Thiese, Effiong, et al., 2015; Wilson et al., 2018; Yen et al., 2019). By teaching the importance of individual goal setting, drivers learn the steps needed to change resistant behaviors and overcome obstacles (Wilson et al., 2018).
Mobile Health Care Technology and Telehealth
Mobile health care technology uses mobile phones, wearable devices, and web-based applications to monitor health and provide remote health care (Greenfield et al., 2016). Incorporating mobile health care technology into health promotion programs provides person-to-person connection, easy access to preventive health education, and the ability to track health behaviors remotely in this hard-to-reach population (Greenfield et al., 2016; Sendall et al., 2018). Smartphone accessible self-monitoring of body weight, eating habits, physical activity, and sleep have been found to be strong predictors of weight loss and behavior change, providing convenience for remote drivers (Olson et al., 2016; Wilson et al., 2018; Wipfli et al., 2019).
Structured Multicomponent Health Promotion Programs
Nearly 40% of trucking companies in the United States lack any type of formal health promotion program (Lemke & Apostolopoulos, 2015). Among health promotion programs available, there is a large variation, with many lacking essential elements necessary to achieve positive health outcomes (Lemke & Apostolopoulos, 2015). Truck drivers need programs that provide mobile and flexible interventions with a broad range of applicability (Passey et al., 2014). Multicomponent programs include a combination of evidence-based practices such as weight loss competitions, incentives, self-monitoring of eating behaviors and body weight, computer-based training, and motivational interviewing from health coaches (Lemke & Apostolopoulos, 2015; Olson et al., 2016; Thiese, Effiong, et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018; Wipfli et al., 2019).
Drivers completing multicomponent health promotions programs had statistically significant changes in body weight, waist circumference, neck circumference, and BMI (Olson et al., 2016; Thiese, Effiong, et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018; Wipfli et al., 2019). Behavioral changes including increased amounts of physical activity, increased consumption of fruits and vegetables, decreased dietary fat intake, and an overall decrease in total daily calories were also noted (Olson et al., 2016; Thiese, Effiong, et al., 2015; Wilson et al., 2018; Wipfli et al., 2019). Favorable cardiometabolic changes included a decrease in fasting blood sugar, low-density lipoprotein (LDL) cholesterol, and total cholesterol, as well as a 12% reduction in the 10-year cardiovascular risk in drivers whose risk was greater than 10% (Varela Mato et al., 2018). These outcomes highlight the potential benefits of multicomponent health promotion programs (Olson et al., 2016; Thiese, Effiong, et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018; Wipfli et al., 2019).
The increased incidence of chronic health conditions in CMV drivers coupled with limited access and low utilization of health care resources suggests the need for effective health promotion programs for this at-risk population (Apostolopoulos et al., 2013). A review of the literature supports the use of motivational interviewing, mobile health technology and telehealth, and structured health promotion programs to improve CMV driver health. Currently, there is a lack of literature evaluating the impact health promotion programs have on increasing DOT medical certification length among CMV drivers.
Phase 2: Preliminary Data Analysis
The dataset contained 22 truck drivers (n =11 males [50%]; n = 11 females [50%]). Ages ranged from 32 to 76 years (M = 52.2; SD = 12.0). The number of health coaching sessions completed ranged from two to 68, with a mean of 16 sessions (n = 21, SD = 16.2). The mean length of participation in FTP was 23.6 weeks (n = 16, SD = 20.9).
Prior to participating in FTP, 12 of the 20 drivers held the maximum DOT medical certificate length; only eight had the potential to increase the length of medical certificate certification (n = 20). After participating in FTP, DOT medical recertification lengths included two 12-month and eight 24-month certificates (n = 10). Three of the eight drivers with improvement potential increased the length of their DOT medical certificate. No driver received a decreased medical certificate length.
The average driver weight prior to participating in FTP was 216.1 lbs (n = 22, SD = 52.8) with an average BMI of 32.1 kg/m2 (n = 20, SD = 7.3). After participation, the average driver weight was 211.5 lbs (n = 14, SD = 62.0) with an average BMI of 30.8 kg/m2 (n = 12, SD = 8.1). The mean post-participation BMI decreased 1.3 kg/m2, t (11) = 1.736, df = 11, p = .110.
Discussion
Phase 1: Comparison of FTP Guidance With Best Practice Guidelines
The 2017 ACC/AHA hypertension guidelines define normal blood pressure, stage 1 and stage 2 hypertension, and hypertensive urgency (Whelton et al., 2018). The coaching guide outlines associated risk factors for elevated blood pressure and recommendations for the prevention and treatment of hypertension according to the ACC/AHA practice guidelines.
The coaching guide references Dietary Approaches to Stop Hypertension (DASH) by the NHLBI. Evidence-based practice guidelines validate the DASH eating plan has been found to lower blood pressure, lower LDL levels, and reduce weight when combined with exercise (National Heart, Lung, and Blood Institute [NHLBI], 2021).
The ADA Standards of Medical Care in Diabetes are referenced within the coaching guide. The coaching guide suggests to health coaches an A1C of 10% or greater is disqualifying and drivers requiring insulin often do not qualify for medical certification. FMCSA regulatory requirements for insulin-treated drivers, published in 2018, permit drivers with a stable insulin regimen and properly controlled insulin-treated diabetes as attested by their treating clinician to be medically qualified up to 12 months (FMCSA, 2022). No specific A1C is required.
While no additional supportive research was found on target heart rate during aerobic exercise, references in the coaching guide reflect current AHA (AHA, n.d.) website information. The Dietary Guidelines for Americans, 2020–2025 promotes MyPlate, a visual aid used to help Americans eat, as the recommended approach to healthy eating at any age (U.S. Department of Agriculture, n.d.).
Phase 2: Preliminary Data Analysis
Of the eight drivers who had the ability to improve medical certification length, three drivers with initial 3-month medical certificates were able to obtain 12- or 24-month medical certificates after participating in FTP (38%). The trend showing an increased length of medical certification after participation in FTP suggests the possibility that a statistically significant difference in pre-/post-program medical certificate lengths may be observed, given a larger sample. In addition, CMV drivers participating in FTP experienced a decrease in mean weight and BMI of 4.6 lbs and 1.3 kg/m2, respectively, which is comparable to findings from previous studies (Wilson et al., 2018; Wipfli et al., 2019).
Recommendations for program improvement include documentation of clinical measures (blood pressure, weight, and BMI) at regular intervals throughout participation, allowing for tracking of health improvements and longitudinal follow-up of program effectiveness. The FTP coaching guide should be updated to reflect current FMCSA regulations for insulin-treated truck drivers.
Applications to Professional Practice
Structured health promotion programs designed for CMV drivers target their unique occupational needs and research has shown improved health outcomes. However, no research is available on whether health promotion programs can increase a driver’s DOT medical certification length. FTP offers CMV drivers an individualized comprehensive health promotion program. Based on the findings from this program evaluation, we conclude that FTP is a health promotion tool based on nationally recognized evidence-based practice guidelines and may optimize DOT medical certification length among CMV drivers who have medical certification lengths of less than 2 years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deep South Center for Occupational Health and Safety ERC for tuition (Snyder and Carbone) and salary (Hammond and Heaton) (Grant T42OH008436).