
Abstract
Health behaviors, including physical activity (PA), of registered nurses (RNs) and medical assistants (MAs) are suboptimal but may improve with worksite programs. Using a repeated-measures crossover design, the authors explored if integrating a 6-month worksite non-exercise activity thermogenesis (NEAT) intervention, with and without personalized health coaching via text messaging into workflow could positively affect sedentary time, PA, and body composition of nursing staff without jeopardizing work productivity. Two ambulatory clinics were randomly assigned to an environmental NEAT intervention plus a mobile text message coaching for either the first 3 months (early texting group, n = 27) or the last 3 months (delayed texting group, n = 13), with baseline 3-month and 6-month measurements. Sedentary and PA levels, fat mass, and weight improved for both groups, significantly only for the early text group. Productivity did not decline for either group. This worksite intervention is feasible and may benefit nursing staff.
Keywords
Health care workers, considered experts in health behavior benefits and health promotion education, are expected to be role models for healthy behaviors, including physical activity (PA; Blake, Malik, Mo, & Pisano, 2011). However, this expectation is often not the case, especially for nursing staff for whom strong evidence demonstrates suboptimal health behaviors and overweight/obesity rates that parallel the general population (Blake et al., 2011; Letvak, 2013; Tucker, Harris, Pipe, & Stevens, 2010; Tucker, Weymiller, Cutshall, Rhudy, & Lohse, 2012). Specific factors contributing to poor health behaviors and obesity among nurses are multi-faceted and include fatigue, rotating and night shifts, multiple home life responsibilities, poor self-image, and time pressures from second jobs and school enrollment (C. W. Chan & Perry, 2012; Clissold, Smith, Accutt, & Di Milia, 2002; Hensel, 2011; Letvak, 2013; Smith-Miller, Shaw-Kokot, Curro, & Jones, 2014). The limited research on nurses and medical assistants (MAs) suggests that their health behaviors are the poorest among all health care team members (Schult, Awosika, Hodgson, & Dyrenforth, 2011). In a study of Veteran’s Administration health care team members, licensed practical nurses and nursing assistants reported the poorest health behaviors, including smoking rates, dietary patterns, physical inactivity, obesity rates, and chronic diseases, such as diabetes (Schult et al., 2011).
Physical activity is indisputably essential for promoting and maintaining health and preventing illness (Penedo & Dahn, 2005; Warburton, Nicol, & Bredin, 2006). Distinct from PA, less sedentary time has also been shown to improve health outcomes independent of other PA (Biswas et al., 2015; Healy, Matthews, Dunstan, Winkler, & Owen, 2011). Worksite programs designed to increase PA and reduce sedentary time for nursing staff could facilitate these behaviors by addressing time constraints and other barriers to PA for this demanding profession. Physical activity programs specifically for the nursing workforce in general, and for ambulatory care in particular, are limited.
A few worksite wellness programs for registered nurses (RNs) have demonstrated an increase in self-reported overall health promotion (McElligott, Capitulo, Morris, & Click, 2010), reductions in body mass index (BMI), and improvements in muscle strength and flexibility, cardiopulmonary function (Speroni et al., 2012), and abdominal girth (Yuan et al., 2009). Although very limited, occupational studies of home care aides/workers, female shift workers, and nursing assistants also suggest that worksite programs have positive effects on muscle strength, cardiorespiratory fitness, body weight, body fat, musculoskeletal symptoms, job strain, work-related fatigue, work ability (Flannery, Resnick, Galik, & Lipscomb, 2011), blood pressure, lipids, depressive symptoms, and diet (Flannery et al., 2012). These findings are consistent with other general worksite studies that focused specifically on PA and reported positive effects on cardiometabolic and obesity markers (C. B. Chan, Ryan, & Tudor-Locke, 2004), musculoskeletal injuries (Proper et al., 2003), work attendance, and job stress (Conn, Hafdahl, Cooper, Brown, & Lusk, 2009).
Although these worksite PA programs are promising, they include off hour and/or structured exercise programs that may interrupt daily workflow and do not specifically address the time constraints of nurses. In contrast to most other worksite PA programs, the authors developed a program that focuses on non-exercise activity thermogenesis (NEAT) and low intensity/light purposeful PA, which the authors labeled NEAT+. NEAT is distinct from purposeful exercise and includes the energy expended in daily activities, such as standing and walking. NEAT+ is purposeful light PA completed in brief periods within nurses’ workflow during work hours. Levine and colleagues (Levine, Eberhardt, & Jensen, 1999; Levine et al., 2005) were the first to coin the term NEAT and the first to test the program in research studies. In a seminal study, they found obese adults sat 164 minutes longer per day than lean participants and the propensity to be seated or to remain standing was not changed following weight loss or weight gain in obese and lean individuals, respectively. Further studies of women supported the observation that obese women are more sedentary and sit more compared to lean women (Johannsen, Welk, Sharp, & Flakoll, 2008). Thus, researchers have recommended targeting NEAT/NEAT+ activities, which are not cardiorespiratory intensive, as a strategy to reduce overall sedentary behavior and weight-related problems while improving cardiometabolic markers (Levine & Miller, 2007; McAlpine, Manohar, McCrady, Hensrud, & Levine, 2007; McCrady & Levine, 2009).
Previously, the authors tested the feasibility of integrating a NEAT-based intervention into the workflow of 58 hospital nurses, finding small but significant reductions in fat mass and increases in PA for intervention participants compared with control participants (Lanningham-Foster & Tucker, 2011; Tucker, Lanningham-Foster, & Murphy, 2011; Tucker, Lanningham-Foster, Murphy, Thompson, et al., 2011). This study was limited to inpatient RNs and did not include other nursing staff or address work productivity which must be addressed if worksite interventions are to be sustainable.
Purpose
The primary purpose of this study was to explore the feasibility, preliminary effects, and barriers and facilitators of integrating a 6-month worksite NEAT+ PA intervention, with personalized health coaching via text messaging, into the workflow of ambulatory clinic nursing staff (RNs and MAs). The study hypotheses were as follows:
The authors added health coaching reinforcement through mobile phone text messaging. Research has indicated that mobile text coaching can improve intervention outcomes and sustainability through tailored, interactive, and person-centered messages that augment clinical practice (Cole-Lewis & Kershaw, 2010; Free et al., 2013; Wei, Hollin, & Kachnowski, 2011). The authors hypothesized that the NEAT+ environment modification plus reinforcement text messages for increasing NEAT+ would be more robust interventions.
A secondary aim was to explore the effects of incorporating NEAT+ activities plus text message reinforcement at the worksite on work productivity and absenteeism. Finally, this study explored barriers and facilitators to increasing PA within the workflow of ambulatory clinic nursing staff. This study extended previous research by examining a NEAT+ intervention with ambulatory clinic RNs and MAs and exploring the influence of the intervention on work productivity and illness-related absenteeism.
Method
A repeated-measures design was used to address the study aims. All participants received the environmental NEAT+ intervention during the 6 months of the study. In addition, participant clinics were randomized to the (a) early texting group who received personalized health coaching via text messaging during months 1 to 3 or (b) delayed texting group who received personalized health coaching via text messaging during months 4 to 6.
The study included an outpatient cancer chemotherapy infusion clinic and a medicine specialty clinic at an academic medical center. Eighteen female RNs and nine female MAs were recruited from the cancer chemotherapy infusion clinic (early texting group, n = 27). Four RNs and nine MAs were recruited from the medicine specialty clinic (delayed texting group, n = 13).
Participants were between 20 and 65 years of age, worked at least 0.5 full-time equivalent (FTE; 20 hours a week), had all acute or chronic illnesses under control, and were willing to use their own cellular phone plan for text messages. Pregnant women were excluded. Figure 1 includes the enrollment flowchart.
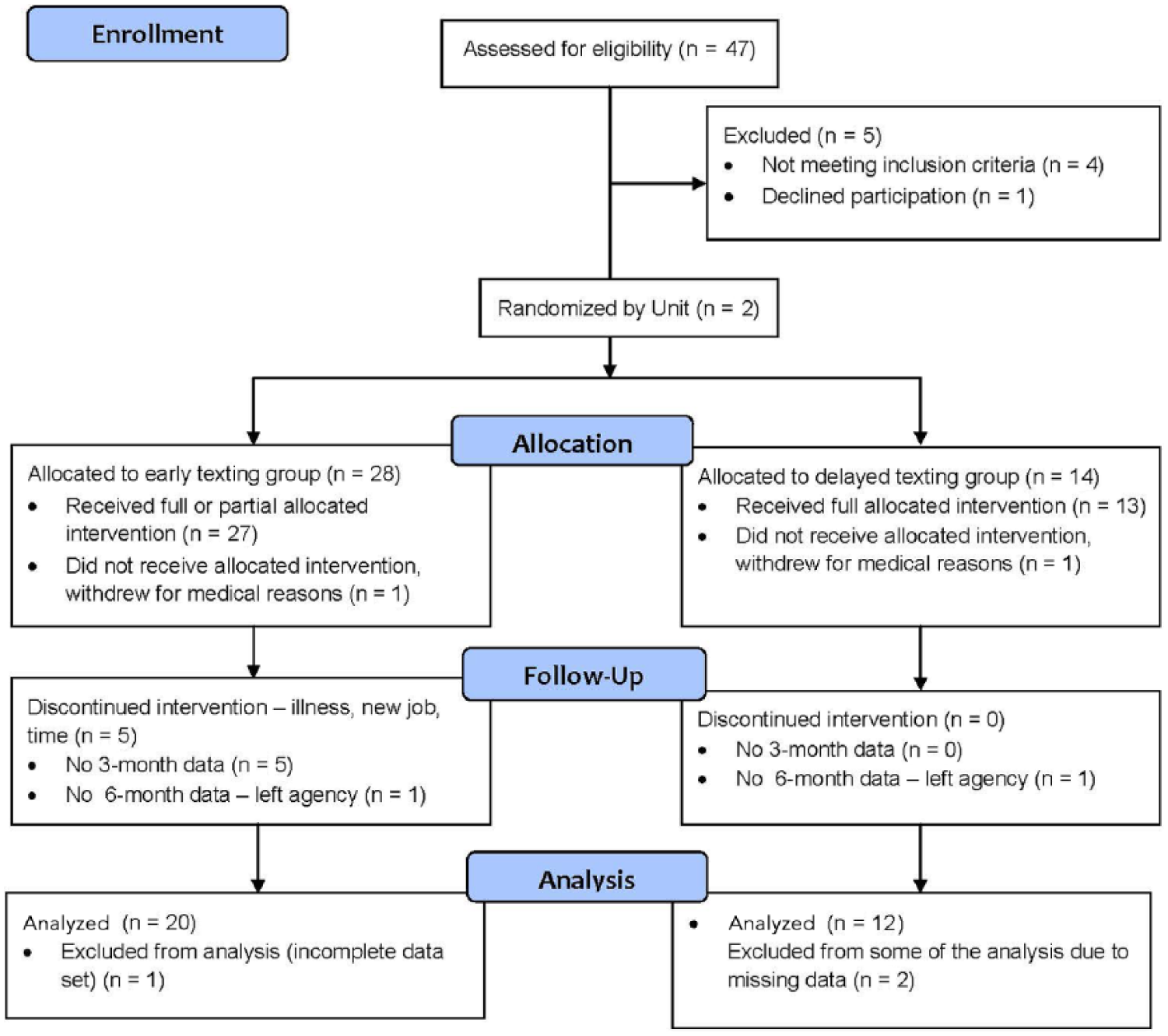
Study flow diagram.
The intervention, designed to promote PA within the daily workflow, was adapted from the investigators’ previous hospital-based NEAT study (Tucker, Lanningham-Foster, Murphy, Thompson, et al., 2011) and included environmental and coaching components. The environmental component included a menu of options for each clinic: workstation treadmill (a computer desk adapted, so that the user walks on a treadmill while performing desk and computer tasks), Wii™ video game system, WellMe in 3™ video clips (3-minute video clips created by the investigators to allow quick bursts of PA in any setting, wearing any attire), stair climbing and walking meetings. Participants designed a personalized program to increase their NEAT+ by 1 hour each day (at least 30 minutes during work hours) using the menu of options and were encouraged to engage in activities with other staff in their clinic to support a team approach.
Mobile health coaching was provided via text messaging using a commercially available text messaging platform, HealthCrowd™, which enabled the researchers to send interactive, personalized health coaching messages. This platform included built-in “intelligence” to allow automation of some of the features (Cole-Lewis & Kershaw, 2010). Intervention participants received one to two text messages per day during their assigned 3 months of intervention. The messages focused on PA and included questions asking participants to text back specific responses (e.g., How much activity they had completed that day?).
Variables and Instruments
Fat and lean mass were measured using dual energy x-ray absorptiometry (DXA; GE Lunar DPX—Prodigy). DXA is a means of measuring bone mineral density through use of two x-ray beams with different energy levels aimed at the individual’s bones. Information from DXA is relevant to diagnosing osteoporosis. DXA uses two low energy x-ray sources to measure bone mass, fat mass, and non-bone lean mass. Estimated precision for fat and lean mass is between 1% and 2% (Hind, Oldroyd, & Truscott, 2010). Percentage fat was calculated as total fat mass/total fat mass plus total lean mass. The instrument was calibrated daily by a trained research assistant using a calibration block consisting of tissue equivalent material with known density values. This procedure assured consistency of measurement over time. Weight and height were measured (shoes removed, limited clothing) using a calibrated scale and stadiometer, respectively, and these measurements were used to calculate BMI (weight/height2).
Physical activity was measured using the Sensewear monitor (SWA; Sensewear® Mini Armband; BodyMedia, Pittsburgh, Pennsylvania), which records data from five sensors, including a three-axis accelerometer, heat flux sensor, galvanic skin response sensor, skin temperature sensor, near-body ambient temperature sensor, and an optional heart rate sensor. Validity and reliability have been shown with the SWA using gold standard doubly labeled water methodology (Johannson et al., 2010). One of the study investigators trained the study coordinator (SC) who managed all PA data collection. Physical activity was reported in averages per day of (a) percentage time of sedentary (1-1.5 metabolic equivalent of tasks or metabolic equivalents [METS]), moderate (3.0-6.0 METS), and vigorous activity (>6 METS); (b) active energy expenditure reported in METS; and (c) number of steps per hour of wake time.
Worker productivity was measured using the 25-item Work Limitation Questionnaire (WLQ) developed by Lerner, Amick, and Glaxo Wellcome (1998) to measure the degree to which health problems interfere with specific aspects of job performance and the productivity impact of these work limitations (Lerner et al., 1998). A WLQ Index Score and Productivity Loss Score were generated along with scores from four subscales: Time Management, Physical Demands, Mental/Interpersonal Demands, and Output Demands. Reliability and validity estimates have been established (Lerner et al., 1998; Munir, 2008).
Absences (hours/month) related to illness, but not pregnancy leave, were retrieved from the human resources database during the 6-month intervention period.
All participants were invited to join an audiotaped post-intervention focus group, led by the principal investigator (PI), to evaluate intervention facilitators and barriers experienced by participants as well as to guide future interventions. The SC was also present during the focus group to take notes.
Study Procedures
Following approval of the protocol by the Institutional Review Board, the project was presented to personnel at staff meetings for each clinic and shared through e-mail. Eligible participants met with the SC who secured informed consent, distributed questionnaires (demographic form and WLQ), and instructed RNs and MAs on the placement and use of the accelerometer. Accelerometers were worn on 4 days, two of which were required to be workdays. Subsequently, participants had their baseline height, weight, and body composition measured at the nursing research laboratory.
Randomization to condition sequence occurred following baseline data collection. The cancer/chemotherapy infusion clinic group was assigned to text messaging the first 3 months (early texting group), and the medicine specialty clinic group was assigned to the combined condition the last 3 months (delayed texting group); both groups received environmental intervention the full 6 months. Both clinics were equipped for the intervention, and all participants were provided instruction on the equipment, where it was located, and how to use it. After the first 3 months of the intervention, the same outcome measures collected at baseline were repeated followed by crossover of the groups into the other condition for 3 months. A final repeated-measures assessment was completed along with the post-intervention focus groups at 6 months.
To ensure that data collection and interventions were implemented as intended, the study investigators provided the SC training in data collection and intervention implementation. Participants were provided contact information to report any equipment failure or other concerns. For the text messaging condition, the texting platform automatically logged outgoing messages and replies from participants, including self-reported adherence to PA recommendations and any free-text comments about their PA at work or at home.
Data Analysis and Interpretation
As a feasibility study, this study was not powered to determine definitive effects. Findings from this study were intended to estimate effects and sample sizes for a larger study.
SAS 9.3 was used for statistical analysis. Descriptive statistics were calculated for all study variables, and distributions of continuous outcome variables were examined for normality and homogeneity of variance. Natural log transformations were applied to improve distributions of percentage time in moderate and sedentary activity, active energy expenditure, and overall productivity index. Because percentage time in sedentary activity was left skewed, it was reversed prior to the transformation. Early texting and delayed texting groups were compared at baseline using independent-samples t tests on age and variables representing years of experience (e.g., MA, RN, and on the study unit), and Fisher’s exact test on role/position, employment hours, education, and marital status.
To test study hypotheses, SAS procedure GLIMMIX was used to fit linear mixed models (LMM) to all outcome variables. To account for dependency in repeated measurements on the same participant, the compound symmetry covariance pattern was fit to the data. The LMMs developed for this study provided adequate fit as judged by examination of standardized residuals. The fixed effects in the models were texting groups (early and delayed), time (baseline, 3 months, and 6 months), and interaction between them. Age, role/position (MA vs. RN), and employment hours (full-time vs. half-time) were considered for inclusion in the models as covariates, but they were not significant at p < .05. To make specific comparisons of between groups, or in outcome changes from baseline, tests of mean contrasts were calculated using parameter estimates from the fitted LMMs. The changes in outcomes from baseline to 6 months for early texting, delayed texting, and combined groups were also tested using parameter estimates from the LMMs. A simulation-based approach for adjusting p values for multiple comparisons was employed (Westfall, Tobias, & Wolfinger, 2011).
The audiotapes were transcribed by the SC who added comments to the transcription from the notes taken during the focus groups. Both the SC and PI who led the groups then reviewed the notes looking for themes of overall acceptance and support for the approach, as well as barriers and facilitators. Together, they compared their identification of themes and shared the themes with the entire research team who approved the themes identified.
Results
Study participants were predominantly White (n = 24, 96%). The two groups of participants differed significantly in the distribution of role types (p = .05) and education (p = .04). The early texting group included largely RN staff (n = 18, 66.7%) with nursing degrees (n = 19, 70.4%), while the delayed texting group included largely MA staff (n = 9, 69.2%) and only 4 (30.8%) had a nursing degree. The two groups did not differ significantly on their employment hours or marital status. The early texting RN participants had fewer years of experience than the delayed texting RN participants (M = 19.2, SD = 12.1 vs. M = 35.5, SD = 4.8, p = .02); however, MA experience and overall experience in the respective clinics for early texting and delayed texting were similar for both groups (Table 1).
Demographic Characteristics and Self-Reported Physical Activity
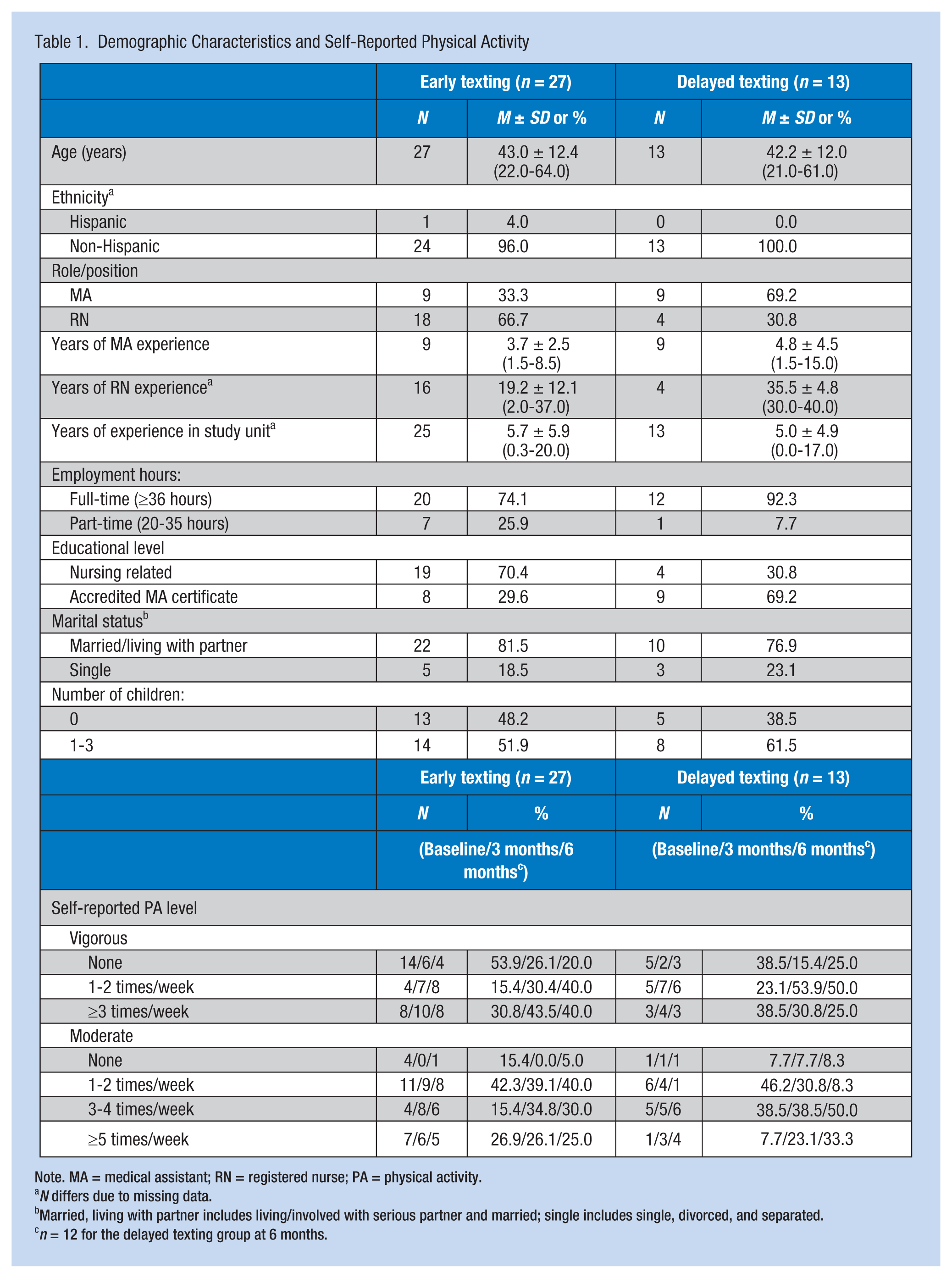
Note. MA = medical assistant; RN = registered nurse; PA = physical activity.
N differs due to missing data.
Married, living with partner includes living/involved with serious partner and married; single includes single, divorced, and separated.
n = 12 for the delayed texting group at 6 months.
At baseline, groups differed on BMI and BMI categories (using Centers for Disease Control and Prevention [CDC] standards; CDC, 2015): weight, total fat and lean mass (p < .01), and percentage body fat (p < .02). Average baseline BMI (M = 26.8, SD = 6.3) for early texting participants was in the overweight category (25-29.9 kg/m2), and the average BMI (M = 34.3, SD = 7.8) for the delayed texting group was in the obese category (>30 kg/m2). Early texting participants also had less baseline body fat and more lean mass than the delayed texting participants (Table 2).
Objectively Measured Body Composition and Physical Activity at Baseline, 3 and 6 Months
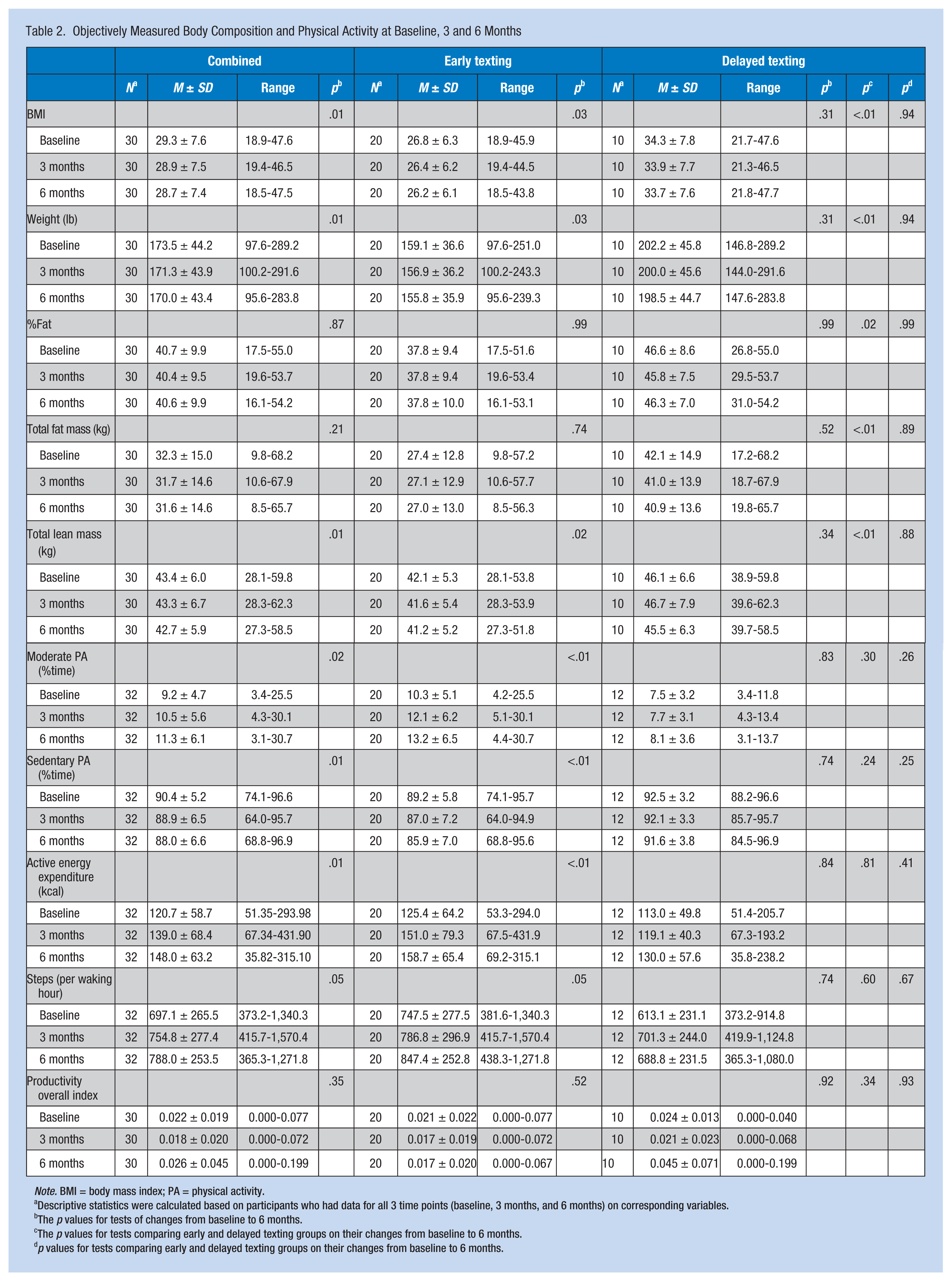
Note. BMI = body mass index; PA = physical activity.
Descriptive statistics were calculated based on participants who had data for all 3 time points (baseline, 3 months, and 6 months) on corresponding variables.
The p values for tests of changes from baseline to 6 months.
The p values for tests comparing early and delayed texting groups on their changes from baseline to 6 months.
p values for tests comparing early and delayed texting groups on their changes from baseline to 6 months.
No significant baseline differences in PA measures or work limitations between the early and late texting groups were found. Of note, at baseline the nursing staff was quite sedentary. On average, 90.4% (SD = 5.2%) of their total day was spent in sedentary or very light intensity activity (≤1.0-1.5 METS) with an average of 691.1 (SD = 265.5) steps per waking hour. Similarly, more than half of the participants self-reported (see Table 1) limited vigorous or moderate PA.
Intervention Effects
Most outcomes changed in the desired direction for both groups over the 6-month intervention period; however, the changes were statistically significant only for the early texting group. Body mass index decreased on average 0.6 (SD = 1.2, p = .03) for the early texting group and 0.6 (SD = 1.5, p = .31) for the delayed texting group. Weight decreased by 3.3 pounds (SD = 7.1, p = .03) for the early texting group and 3.6 pounds (SD = 8.4, p = .31) for the delayed texting group. Total lean mass decreased by 0.9 kg (SD = 1.6, p = .02) for the early texting group and 0.6 kg (SD = 1.1, p = .34) for the delayed texting group. Over time, fat mass and percentage fat were lower but not statistically significant for either group (Table 2).
With respect to PA, both groups changed in the desired direction. Percentage time in moderate PA increased by 2.9% (SD = 4.5, p < .01) for the early texting group and 0.6% (SD = 4.0, p = .83) for the delayed texting group. At the same time, percentage time in sedentary PA decreased by 3.3% (SD = 4.6, p < .01) for the early texting group and 0.8% (SD = 4.1, p = .74) for the delayed texting group. Active energy expenditure and the number of steps increased by 33.3 steps (SD = 51.7, p < .01) and 99.9 steps (SD = 311.8, p = .05) for the early texting group and 17.1 steps (SD = 63.0, p = .84) and 75.8 steps (SD = 314.9, p = .74) for the delayed texting group (Table 2).
When the groups were combined, changes from baseline to 6 months were significant for BMI (p = .01), weight (p = .01), total lean mass (p = .01), percentage time in moderate PA (p = .02), percentage time in sedentary PA (p = .01), active energy expenditure (p = .01), and steps (p = .05; Table 2).
For both the early and late texting groups, the WLQ index (M = 0.02, 0.02; SD = 0.01, 0.02), productivity loss (M = 0.02, 0.02; SD = 0.01, 0.02), and subscale scores (M = 1.24-1.39 for the four subscales) were all low at baseline for both groups, indicating that work limitations were few. These levels did not change significantly over time.
The average number of sick days ranged from 9 to 14 for both groups for each 3-month period. The changes in absence days did not differ significantly for groups over time (p = .55 for early text participants and p = .09 for delayed text participants; Table 3).
Changes in Sick Leave Hours During Study Period
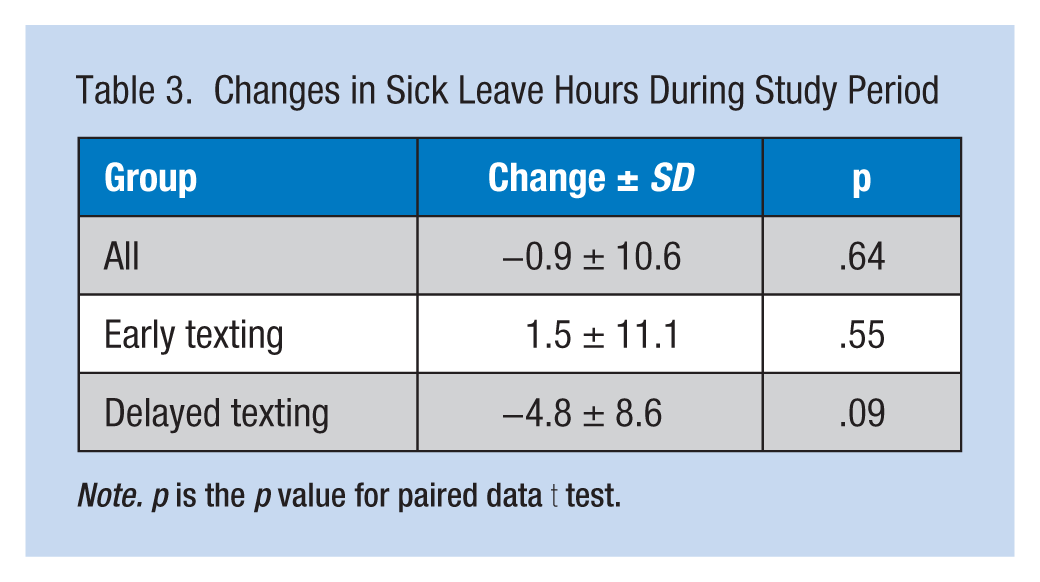
Note. p is the p value for paired data t test.
Focus Group Data
Themes generated from the focus groups included the following: (a) preferences for PA options varied by participants, (b) the intervention increased morale and productivity, (c) nurse manager and equipment availability were facilitators, and (d) competition for equipment and workload/breaking up routines were barriers. Examples of comments for each theme are presented in Table 4. Overall, the program was rated as very favorable with multiple benefits at and away from work, including participating in other wellness pursuits.
Focus Group Themes and Example Comments
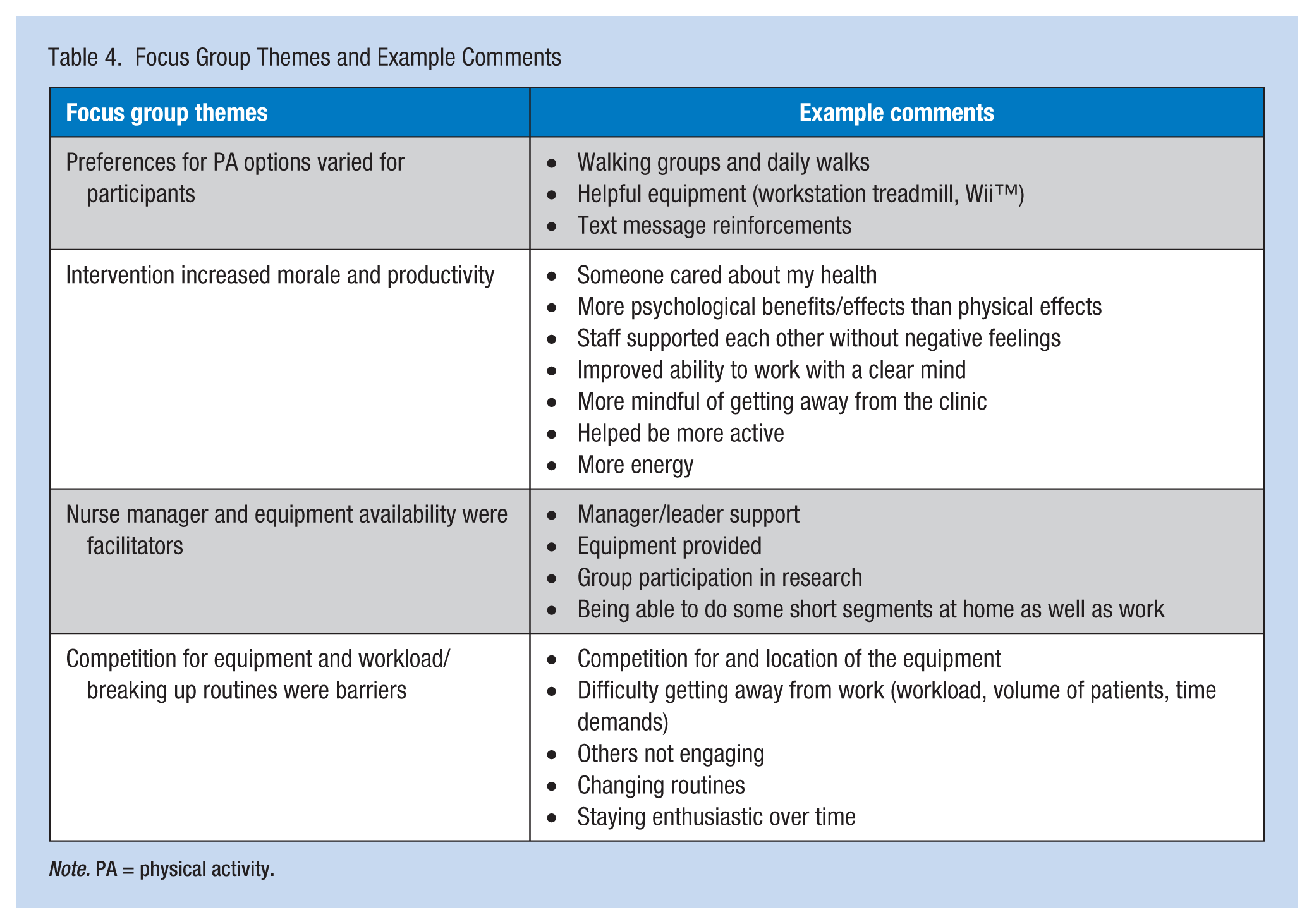
Note. PA = physical activity.
Support for future programming was strong with recommendations for ongoing support from leaders and physicians, making the equipment more visible, allowing time, and adding healthy vending options. Participants also encouraged use of social media, email instead of text messaging, upgraded treadmills and pedometers, more prescriptive activity guidelines, and unit competitions.
Discussion
Nurse obesity and related health problems have been associated with rotating and long work hours, work intensity, and suboptimal self-care activities, including inadequate PA (Hensel, 2011; McElligott, Siemers, Thomas, & Kohn, 2009; Nahm, Warren, Zhu, An, & Brown, 2012; Zapka, Lemon, Magner, & Hale, 2009). Perhaps contrary to the public’s perception of the nursing workforce, the nursing staff in this study spent the vast majority of their day in sedentary or very light activity including light energy expenditure and sitting time. Although not formally studied, these data support anecdotal observations that suggest inpatient nurses are more active than ambulatory nurses, likely due to differences in work activities and setting layouts. These findings suggest that sedentary time, daily PA levels, and some body composition measures can be improved through innovatively integrating NEAT-based PA with text messaging into the workflow and work setting of RNs and MAs, without jeopardizing work productivity. This study extends previous research (Tucker, Lanningham-Foster, & Murphy, 2011; Tucker, Lanningham-Foster, Murphy, Thompson, et al., 2011) to an ambulatory setting with all nursing staff and added text messaging support.
The findings address the growing concern in health care about the dangers of sedentary activity regardless of other PA levels. Healy and colleagues (2011) published the first population-based study associating prolonged sedentary time with cardiometabolic and inflammatory biomarkers (Healy et al., 2011). This study has since been supported by a systematic review and meta-analysis which reported additional associations between sedentary time and hospitalizations, mortality, cardiovascular disease, and cancers in adults independent of PA (Biswas et al., 2015).
The menu-driven NEAT and NEAT+ intervention provides opportunities for nursing staff to participate in a variety of activities for short periods of time throughout the workday using treadmill workstations, Wii™ gaming, and other activities. Growing evidence suggests that shorter more frequent bouts of activity (Armstrong et al., 2015) throughout the day can reduce sedentary time by as much as 2 hours per 8-hour workday (Healy et al., 2011; Taylor et al., 2013) and can lower weight and cholesterol levels (Taylor et al., 2010). Moreover, for desk-based occupations, the evidence suggests that seated-based work should be regularly altered with the goal of accumulating 2 hours per day of standing and light activity (light walking) during work hours, eventually progressing to a total accumulation of 4 hours per day (Buckley et al., 2015).
The finding that NEAT and light activity can be incorporated into the workflow without affecting work productivity is critical and consistent with other literature. Torbeyns and colleagues evaluated the literature on active workstations and found no detriment to work performance (Torbeyns, Bailey, Bos, & Meeusen, 2014). More recently, Sliter and Yuan (2015) reported that walking workstations had no effect on work performance, and Carr and colleagues (2016) reported no negative effects on productivity from an ergonomic workstation optimization plus seated activity permissive workstation. Moreover, in the Carr et al. study, greater adherence to workstation activity was associated with better health and work productivity outcomes.
Worker acceptance and satisfaction are key to the success and sustainability of any worksite program. Study participants were positive about the intervention, as reflected in the focus groups, with one major theme being improved group morale. Having RNs and MAs included in the study might have contributed to this outcome by enhancing team cohesion. Other benefits noted by participants were creation of walking groups and daily walks, helping participants leave the unit, improving ability to work with a clear mind, and providing PA equipment (e.g., workstation treadmill, Wii™). Support for future programming was strongly recommended with an emphasis on support from leaders and physicians, making the equipment visible, and adding healthy vending options. This feedback is similar to the feedback received by Taylor and colleagues who found that participant perceptions of worksite booster breaks included less stress, more enjoyment and health awareness, and behavior change (Taylor et al., 2010). The “menu of options,” which allowed for variety and individual preferences throughout the workday, matched recommendations by Taylor’s study participants. Like the Taylor study, these participants also stressed the importance of leadership and management support to facilitate the intervention.
Of note, the researchers also elicited participant feedback about the barriers to participation in the program, including workload, patient volume, time demands, lack of engagement, and changing routines. In the future, the menu of activity options should be expanded to address these concerns.
The refined intervention included text messaging. Although the researchers did find that text support early in the intervention resulted in significant increases in PA and reductions in sedentary activity, fat mass, and weight, no differences were found in these outcomes between the early and delayed texting groups. Several studies have identified text messaging as an ideal channel for promoting health behavior change and integrating PA into the workday (Cole-Lewis & Kershaw, 2010; Free et al., 2013; Wei et al., 2011). The sample size was small, and the groups differed in number of participants, which could, in part, explain the lack of significant differences in outcomes. The researchers also did not have a non-texting control group, which would have better identified the incremental effect of texting.
This study was designed to test the feasibility and initial effects of integrating a NEAT-based intervention into the workflow of nursing staff in an ambulatory care setting. The findings inform employers and managers about the surprisingly sedentary nature of ambulatory nursing as well as the potential benefits of a NEAT-based intervention integrated into the workflow of nursing staff. Further research with a larger sample, control group, more robust work productivity and absence measures, and a longitudinal design to observe the magnitude of effects over time is recommended.
Implications for Occupational Health Nurses
These study findings inform occupational health nurses about the growing concerns of sedentary occupational time and strategies for reducing the amount of daily sedentary time for all employees but especially for those with highly sedentary roles. A first step for occupational health nurses may be to develop educational offerings to bring awareness to employees and organizational leaders, given the support needed for reconstructing work settings and workflow. A second step for occupational health nurses is to consider use of an assessment tool (e.g., a pedometer or other activity monitor) to assist employees in identifying their degree of occupational activity and any associated health risks (e.g., musculoskeletal concerns, overweight or obesity, and cardiovascular risks).
A third step for occupational health nurses is to develop programs and opportunities for increasing activity. Convening a taskforce to shape the programs could also be a useful step. The program could include suggested low-cost workflow ideas such as establishing set breaks away from workstations, scheduled group walks, walking meetings (with designated nametags), shortening meeting times and resulting seat time, promoting a stairwell campaign in lieu of using elevators, encouraging parking further away from the building to increase steps, and promoting quality time away from work. Inexpensive work setting changes can also be considered. For example, offices can be rearranged to create physical movement such as moving printers or trash cans so that employees must walk to reach them. Other options with associated costs to consider include workstation treadmills (Figure 2) if the workspace can accommodate the equipment, elliptical devices under desks (Figure 3), or standing workstations.
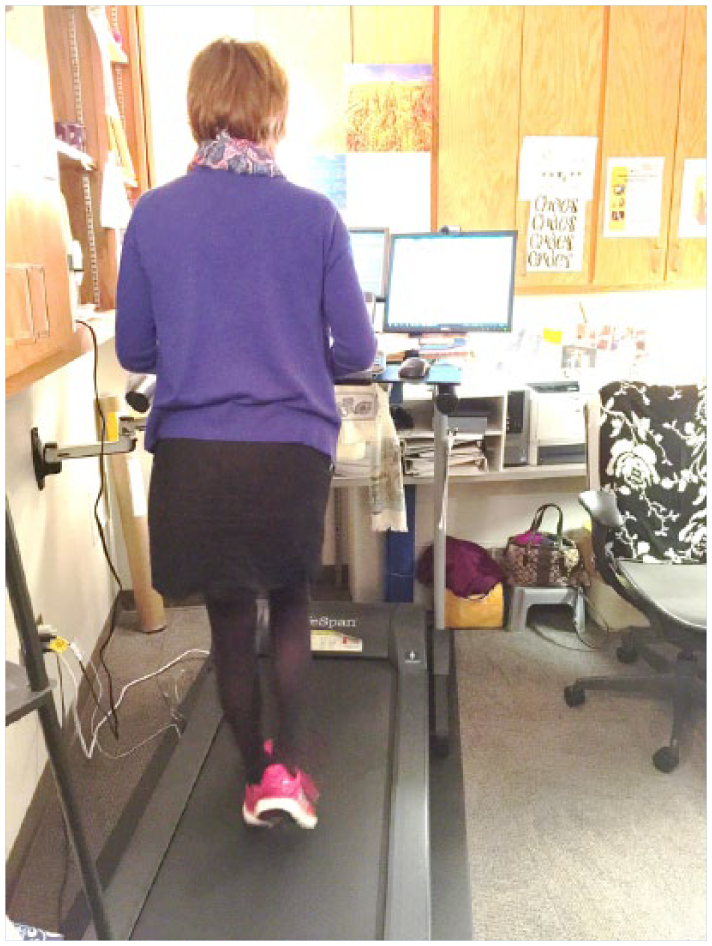
Workstation treadmill.

Workstation elliptical.
Applying Research to Practice
Health concerns associated with sedentary occupational time for employees, and especially for those with highly sedentary desk roles, are growing. Occupational health nurses can implement many strategies to reduce these concerns. Strategies may include development of educational offerings to bring awareness to employees and organizational leaders, and use an assessment tool to assist employees in identifying their degree of occupational activity and any associated health risks. Additional action strategies are low-cost workflow ideas such a establishing set breaks away from workstations, scheduled group walks, walking meetings (with designated nametags), shortening meeting times and resulting seat time, promoting a stairwell campaign in lieu of using elevators, encouraging parking further away from the building to increase steps, and promoting quality time away from work.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sharon Tucker is director for nursing research, EBP & quality at the University of Iowa Hospital and Clinics. She directs research and evidence-based practice focused on testing and implementing behavioral interventions for women and children, worksite health and wellness, and quality and safety, including reducing and preventing hospital-associated conditions.
Michele Farrington is a certified pediatric hematology/oncology nurse and works as a clinical health care research associate at the University of Iowa Hospitals and Clinics. She serves as a study coordinator and EBP mentor with experience and expertise in pediatric oncology and EBP, leading/co-leading initiatives since 2003.
Lorraine M. Lanningham-Foster is an associate professor of human nutrition at Iowa State University. Her research focuses on simple obesity prevention strategies related to both physical activity and diet for children and families.
M. Kathleen Clark is a professor at the University of Iowa College of Nursing. Her current research focuses on the integration of biological and behavioral factors that contribute to healthy weight.
Cindy Dawson is director of clinical functions for ambulatory nursing at the University of Iowa Hospitals and Clinics. She has practiced for 40 years in ambulatory otolaryngology nursing with a focus on research and evidence-based practice.
Trudy Laffoon is nurse manager for the Pain Management and Medicine Specialty Clinics at the University of Iowa Hospitals and Clinics. She has extensive nursing experience in perioperative, telehealth, and ambulatory nursing care and is a strong proponent of innovation.
Geralyn J. Quinn is nurse manager for the University of Iowa Holden Comprehensive Cancer Center Clinic and Infusion Suite. She promotes continuous improvement strategies to benefit both patients and staff.
Yelena Perkhounkova is the statistician manager for the University of Iowa College of Nursing. She provides dedicated support for the research efforts of collegiate faculty and nurse researchers at the University of Iowa Hospitals and Clinics.