
Abstract
This systematic review examines literature regarding the relationship between workplace psychosocial factors and musculoskeletal disorders (MSDs). Musculoskeletal disorders are the leading cause of work disability, resulting in billions of dollars of financial losses. Evidence suggests that workplace psychosocial factors can lead to the development and progression of MSDs. A data search was conducted in MEDLINE, EMBASE, PsychINFO, Scopus, and CINAHL (Cumulative Index to Nursing and Allied Health Literature) from August 2009 to May 2020 inclusive. Other eligibility criteria included studies published in English, conducted on adults within a workplace setting, conducted in developed economies, and were stability-control longitudinal observational studies. Studies were independently screened for eligibility, using COVIDENCE (software for managing and streamlining systematic reviews) and assessed for quality by multiple authors, using the JBI Evidence synthesis tool. From 6,812 studies, 47 articles were included in the final analysis. The most common MSDs investigated were lower back pain, neck and shoulder pain, and upper extremity symptoms and disorders. Included articles identified that psychosocial workplace factors of support, collaboration, job control, and job demands were statistically significantly associated with risk and progression of MSDs. Review of the articles included in this article supports the theory that MSDs have a multifactorial, complex etiology that includes psychosocial factors. Interventions to enhance psychosocial work environment provide opportunities to reduce the risk of MSDs.
Keywords
Introduction
Musculoskeletal disorders (MSDs) refer to a group of conditions that have the potential to cause long-term pain and may result in permanent and disabling damage to the motor organs (including bones, cartilage, ligaments, muscles, nerves, and tendons; Gómez-Galán et al., 2017). Among the most prevalent MSDs are lower back pain (LBP; Chen et al., 2022) and neck pain (Hurwitz et al., 2018), which are said to make up two thirds of workplace MSD claims in Australia (Oakman et al., 2019). The pervasive nature of these conditions is widespread, with the 2017 global burden of disease study ranking MSDs fifth among all diseases in terms of disability-adjusted life years, and first with regard to years lost due to disability globally (GBD 2017 DALYs and HALE Collaborators, 2018). The economic cost of these conditions is also significant, with healthcare spending due to MSDs within the United States alone reaching an estimated US$380.9 billion year-over-year (Dieleman et al., 2020). These figures are echoed within Europe, with combined productivity and healthcare losses exceeding €240 billion annually (Bevan, 2015), underscoring the need for action. Many studies suggest that workplace psychosocial factors can lead to the development and progression of MSDs; however, the causal relationship remains inconclusive (Gallagher & Barbe, 2022; Thiese et al., 2020; Yang et al., 2023).
The International Labor Organization (ILO) defines psychosocial factors at work as (a) interactions among job content, work organization and management, and other environmental and organizational conditions, and (b) employees’ competencies, needs, and culture (ILO, 1986; Oakman et al., 2022). Psychosocial stressors refer to interactions that are a hazard to employees’ health through their perceptions and experience (ILO, 1986). In MSDs research, psychosocial factors are commonly measured with the job demand–control–support model, with some studies using effort-reward imbalance (ERI) as an alternative. Typically, high job demands and low job control have been demonstrated to be associated with onset and progression of MSDs (Buruck et al., 2019). The chronic nature of MSDs can have serious ramifications for an individual, implicating the economic, physical, emotional, and social aspects of a person’s life (Oakman et al., 2017). This highlights the necessity for workplaces to minimize the risk of developing MSDs, with one potential method being a reduction in psychosocial stressors.
Although the links between workplace psychosocial factors and MSDs are well researched (Afsharian et al., 2023; Budnik et al., 2018; López-González et al., 2022; Taibi et al., 2021), knowledge gaps remain in relation to characteristics of the relationship. The causal direction of the relationship between MSDs and psychosocial factors in the workplace remains undecided (Åhlin et al., 2021; Magnusson Hanson et al., 2017). To address this gap within the literature, there has been a call to arms for more studies to employ a longitudinal study design to help infer the direction of this relationship (Lang et al., 2012). Although it must be said for many reasons (including funding and time constraints), a lot of the literature within this space continues to access MSDs and psychosocial risk factors through a cross-sectional lens (Lachowski et al., 2017; Roja et al., 2018; Tang et al., 2022).
Previous reviews by Lang and colleagues (2012) have concluded that most identified psychosocial stressors had a small yet significant lag effect on the development of MSDs within the workplace. Other, more recent reviews within this space have also commented on this relationship as evidenced by Buruck and colleagues (2019), which illustrated that LBP was significantly positively related to workload (odds ratio [OR] = 1.32). Considering this, the present review endeavors to provide a timely follow-up that augments these previous studies via an analysis of the contemporary and current relationships between workplace psychosocial factors and MSDs. In addition, focusing specially on stability adjusted, longitudinal studies to elucidate the causal links in this relationship. This review was guided by the following research question:
Methods
The review protocol was registered with Open Science Framework (https://osf.io/uv75b/) and the methods are consistent with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Moher et al., 2009) and the Johanna Briggs Institute guidelines (Aromataris & Munn, 2020b).
Search Strategy
An online search was conducted of articles published from August 2009 to May 2020 in the following databases: MEDLINE, EMBASE, PsycINFO, Scopus, and CINAHL (Cumulative Index to Nursing and Allied Health Literature). The PICO (Population, Intervention, Comparator, and Outcome) model was used to operationalize the search (Santos et al., 2007). The search strategy was developed by the research team in consultation with a medical librarian. Articles were limited to English and publication type (peer-reviewed journal articles). In addition, as this review was only concerned with contemporary literature, only articles published since August 2009 were accepted for inclusion.
Keywords and Medical Subject Headings regarding MSDs, psychosocial risk factors, and workplace settings were used. Examples of the search terms include musculoskeletal disease, musculoskeletal pain, backache, neck pain, arm pain, psychosocial, demands, control, strain, support, security, psychological, work, workplace, occupation (truncation and proximity searching were applied to some terms). A full search strategy for the database searches can be found in the online supplemental materials (Supplemental Materials 1).
Article Screening
The full-text screening selected articles for inclusion if they were (a) full-text original articles, in press, and accepted or published from August 2009 to May 2020; (b) studies conducted on adults (mean age of population 16–65 years) within a work place setting; (c) reporting on original data on the relationship between any type of psychosocial work stressor and any type of musculoskeletal problem; (d) conducted in developed economies (as per the United Nation’s developed economies list; United Nations, 2020) to ensure the results would be applicable and generalizable in similar work situations, noting that developed economies and developing economies have very different workplace practices, and (e) stability-control longitudinal observational studies. Each article was assessed to see whether stability was controlled for. This was done by checking whether included articles excluded all persons with or without musculoskeletal problems at baseline or, whether articles used a statistical technique to control for the effect of initial musculoskeletal problems. Articles were excluded if they reported on studies that (a) included patients hospitalized due to MSDs, (b) did not control for baseline levels of MSDs, (c) assessed MSDs with etiology of cancer or neurology (e.g., spinal cord injury or stroke), and (d) assessed psychosocial work stressors in populations with severe mental illness (e.g., schizophrenia, borderline personality disorder, and bipolar disorder).
Utilizing Covidence (Covidence systematic review software, 2020, Veritas Health Innovation, Melbourne, Australia), title and abstract screening was done in tandem by two independent reviewers (A.B. and E.A.). In the case of conflicts, a third reviewer (H.N.) resolved any disagreements. Those articles that were deemed to meet the inclusion criteria underwent full-text screening in Covidence by at least two independent reviewers (A.B., E.A., and H.N.). A third reviewer was involved when there were discrepancies between the first two reviewers.
Quality Assessment and Data Extraction
Articles that passed full-text screening formed the final set of articles for extraction and inclusion within this study. Two independent reviewers (E.A. and H.N.) conducted a quality assessment of these final articles using the National Institutes of Health quality assessment tool (National Heart, Lung and Blood Institute, 2013). This tool has since been appraised and recommended for systematic reviews (Ma et al., 2020). The quality assessment was guided by questions designed to evaluate the internal validity of a study and test for any potential bias. Specifically, authors determined whether the results reported in the study could be attributed to the exposure being evaluated and was not a result of a flawed study design. Studies were ranked highly if a causal relationship between the exposure and the outcome was determined.
The reference lists of included articles were also searched. Articles were cataloged and screened using the referencing software Endnote (The EndNote Team, 2013; Clarivate Analytics: Philadelpha, PA) and the web-based software platform Covidence that streamlines the production of reviews. Data were extracted from the final set of articles as suggested by Aromataris and Munn (2020a). Authors devised categories for both psychosocial factors and MSDs based on the available information in the studies.
Results
The search identified 6,812 articles for screening, of which 1,826 were duplicates. Title and abstract screening were conducted for 4,986 articles, with articles appraised against the review’s inclusion and exclusion criteria. Articles that met the inclusion criteria (n = 236) progressed to full-text screening. As highlighted in the PRISMA flow diagram (Figure 1), the top five reasons that articles were excluded during this phase of screening were due to the study design (n = 86), the setting of the study conducted within a non-developed economy (n = 23), the article type (n = 23), the study not controlling for baseline MSDs (n = 22), or the study reporting the wrong outcome (n = 18). The other reasons for exclusion are reported within the PRISMA flow diagram (Figure 1). Following the full-text screening, a total of 47 articles were included in the study, as shown in Figure 1 (Andersen et al., 2019; Bodin et al., 2018; Bovenzi, 2009, 2015; Bovenzi et al., 2015, 2016; Christensen et al., 2018; Christensen & Knardahl, 2010, 2014; Clausen et al., 2013; Dragioti et al., 2019; Garg et al., 2012, 2014; Gerr et al., 2014; Halonen et al., 2018, 2019; Harris et al., 2011; Herin et al., 2012, 2014; Hooftman et al., 2009; Hush et al., 2009; Janssens et al., 2014; Jun et al., 2020; Kaaria et al., 2011; Lamy et al., 2014; Lapointe et al., 2009, 2013; Larsman et al., 2011; Larsman & Hanse, 2009a, 2009; Lu et al., 2014; Madsen et al., 2018; Magnusson Hanson et al., 2017; Matsudaira et al., 2012; Mierswa & Kellmann, 2017; Neupane & Nygard, 2017; Oakman et al., 2017; Plouvier et al., 2009; Prakash et al., 2017; Shahidi et al., 2015; Smith et al., 2009; Solidaki et al., 2013; Vandergrift et al., 2012; Van Nieuwenhuyse et al., 2013; Vargas-Prada et al., 2013, 2016; Wigaeus Tornqvist et al., 2009). Most studies were conducted in Europe (n = 34, 72%), followed by the Americas (n = 10, 21%) and Asia/Australia (n = 3, 7%). These articles are summarized in the online supplemental materials (Supplemental Materials 2). Common reasons for articles being excluded during the full-text screening included incorrect study design, population from a nonindustrialized country, not an original research article, did not control for baseline MSDs, wrong outcome was measured, or participants were not from a working population.
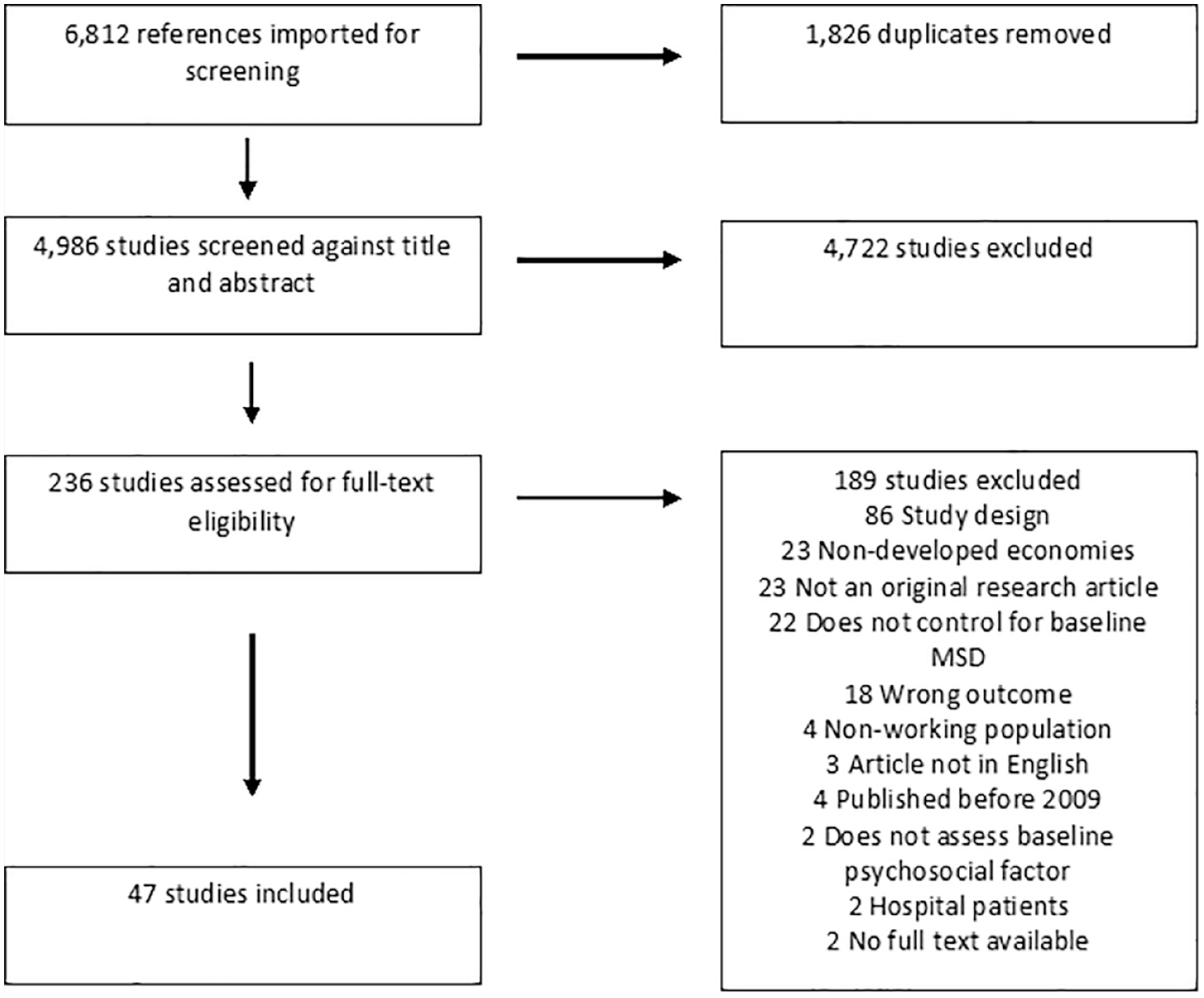
PRISMA Flow Diagram of Included Studies
Most studies included in this analysis tested psychosocial factors in terms of job demands, control, and support. These can be grouped into passive jobs (low demand, low control), high strain jobs (high demand, low control), and low strain jobs (low demand, high control; Shahidi et al., 2015). Workers were professional drivers, manufacturing and production, and office workers. Sample size ranged from 53 to 12,714 participants. Follow-up times and regularity varied from every 14 days for 12 months to biannual follow-ups for 6 years. The longest time lag was 28 years. The most common MSDs investigated were LBP, neck and shoulder pain, and upper extremity symptoms and disorders. The majority of workplace industries represented were general workers (n = 21), healthcare workers (n = 7), office-workers (n = 7), manufacturing and production (n = 6), drivers (n = 3), blue-collar workers (n = 2), and education (n = 1). Table 1 summarizes the statistically significant effects between workplace psychosocial factors and MSDs from included studies, providing details of the OR, risk ratio (RR), and the hazard ratio (HR).
Statistically Significant Associations Between Workplace Psychosocial Factors and Musculoskeletal Disorders
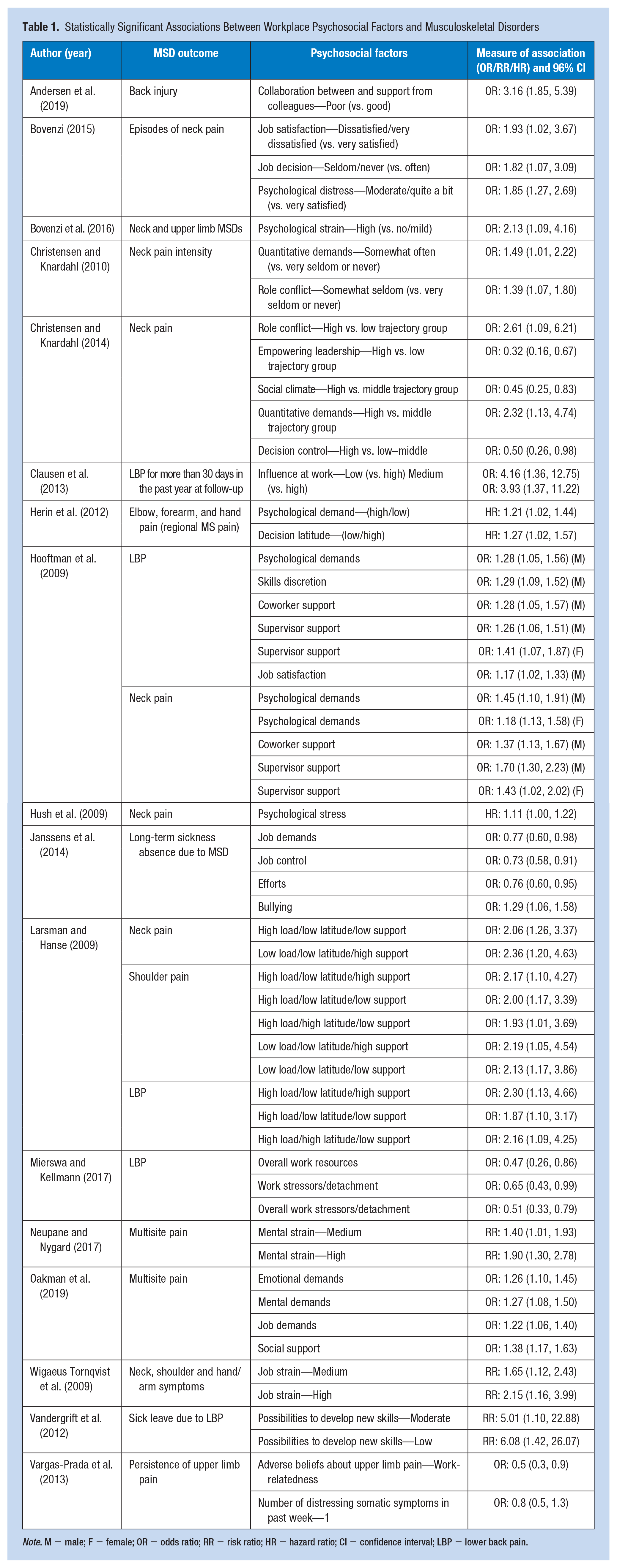
Note. M = male; F = female; OR = odds ratio; RR = risk ratio; HR = hazard ratio; CI = confidence interval; LBP = lower back pain.
Workplace factors of low support and lack of collaboration were found to be associated with an increased risk of MSDs (Andersen et al., 2019; Bovenzi, 2015; Dragioti et al., 2019) although Garg and associates (2014) found no association between MSDs and social support from colleagues and supervisors. Low job control was significantly associated with an increase in the number of anatomical regions with pain and long-term sickness absence (Janssens et al., 2014), as well as low job decision and high job dissatisfaction being associated with increased risk of neck and shoulder pain (Bovenzi, 2015). Bovenzi et al. (2015) found that an adverse psychosocial work environment was poorly associated with sciatic pain.
High psychological demand or stress, low psychological well-being (Bodin et al., 2018; Bovenzi et al., 2016), and depression were significantly associated with an increase in the occurrence of MSDs (Garg et al., 2012; Halonen et al., 2019). Shahidi et al. (2015) found that depressed mood was a predictor for the onset of neck pain in office workers. Workplace bullying was related to long-term sickness and absence due to both MSDs and mental health problems (Janssens et al., 2014). A range of protective factors were identified, including empowering leadership and decision control (Christensen & Knardahl, 2010), as well as low role conflict (Christensen & Knardahl, 2014). Additional studies have identified that there are gender differences in the experiences of MSDs as a result of psychosocial factors (Garg et al., 2014; Herin et al., 2014; Hooftman et al., 2009; Lapointe et al., 2013).
In addition to conflicting findings regarding the causation of MSDs from psychosocial factors, the direction of the relationship has also been questioned. Halonen et al. (2019) tested the relationship between ERI and neck/shoulder pain and LBP, and found there was a bidirectional association between the MSDs and ERI (RR 1.22, 95% confidence interval [CI] = [1.00, 1.48]). An examination into the articles included in this study supports the theory that MSDs have a multifactorial, complex etiology that includes psychosocial factors.
Discussion
An individual’s MSDs outcome is determined by the unique combination of quantitative workload (mechanical and physical) and psychosocial (demand, control, and support) influences (Christensen & Knardahl, 2010; Dragioti et al., 2019). The majority of studies included in this review tested psychosocial factors using these three elements. Although many studies claim that the relationship between psychosocial factors and MSDs is unequivocal (Herin et al., 2014; Mehrdad et al., 2010; Ng et al., 2019), there remains uncertainties around specifics of the associations. Hence, many studies detected significant associations between psychosocial factors and a range of MSDs, whereas others did not adjust for physical workload and depressive symptoms (Bovenzi, 2009; Clausen et al., 2013).
One area this review reinforces pertains to high job demand, low job control, high job strain, and low job security as an antecedent for LBP symptoms. As previously highlighted in reviews by Lang et al. (2012) and Hauke et al. (2011), there is a significant association with this anatomical region to become compromised in the presence of the aforementioned workplace psychosocial factors. In fact, within Australia, around one in three (35%) MSDs claims involve the back (Oakman et al., 2017). This bodily region is the most aggravated area in terms of reported MSDs, surpassing other bodily locations, including the shoulder (16%), the knee (13%), and the ankle (6%; Oakman et al., 2017). There are several hypotheses as to why MSDs such as LBP are so pervasive in the presence of high job demand, low job control, high job strain, and low job security. One such hypothesis centers around the physiological response to stress induced from these types of workplace environments (McEwen, 1998). According to the allostatic load framework, chronic stressors such as those found in the workplace can cause a “wear and tear” phenomenon among several linked physiological systems (Glei et al., 2007). Such fatigue within these systems is associated with dysregulated levels of biological parameters that are responsible for the function of the sympathetic nervous system, hypothalamic–pituitary–adrenal axis and the immune system (McEwen, 2002). If an individual is repeatedly exposed to ongoing stressors, over time it can result in a physical complaint such as LBP (Lang et al., 2012). Work environments that look to alleviate work stressors by redesigning job aspects, changing the organizational culture, and allowing flexible working arrangements could see improvements in overall MSDs risks (Bhui et al., 2016).
The findings of this review highlight the under examination of MSDs concerned with the knee, when compared with other bodily regions that were more commonly explored. The shoulder, lower back, and neck were the most reported regions of examination, with only one study investigating the knee (Madsen et al., 2018). This is in contrast to statistics from Safe Work Australia, which report MSDs of the knee being the third most commonly reported, only surpassed by the back (35%) and the shoulder (16%; Oakman et al., 2017). The under examination of MSDs locations that are more traditionally associated with manual handling jobs foreshadows the changing nature of how work is being conducted (Padula et al., 2017), with a greater focus on job automatization and the use of computer workstations (Moore, 2019). Notably, research has confirmed the dose–response association with the number of hours per day working on a computer workstation and MSDs risk in regions including the neck, shoulder, and lower back (Gerr et al., 2004; Van Eerd et al., 2016; Yang et al., 2016). This review underscores this notion when considering the workplace characteristics of included studies. The majority of studies were concentrated (n = 21) in mixed worker cohorts that were more weighted on individuals who work office jobs. In terms of reported individual industries, manufacturing, and production (n = 6) was third to healthcare (n = 7), and studies that specifically examined office workers (n = 7), which further reiterates the research gap between blue-collar and white-collar settings. Research should continue to evaluate the relationship between workplace psychosocial factors and their association with MSDs in blue-collar industries, so as to not segregate a vital part of the global workforce.
The review of the articles included in this study supports the theory that MSDs have a multifactorial, complex etiology that includes psychosocial factors (e.g., Christensen et al., 2018; Clausen et al., 2013; Garg et al., 2012, 2014). As a result, targeted workplace interventions that minimize psychosocial stressors can have potential gains in alleviating the prevalence of MSDs, hence improving well-being for workers and achieving significant economic savings. Consequently, interventions to reduce psychosocial stressors will not only reduce cases of MSDs but will also lessen the occurrence of mental health. Modifiable risk factors, some of which are more easily adapted than others, include physical actions (e.g., greater mobility and increasing exercise for neck pain in office workers), whereas adjustments to the psychosocial work environment are more complex. Implementing effective interventions to mitigate psychosocial stressors and other workload and organizational factors requires the use of methods that are evidence based (Gerr et al., 2014). As highlighted by Halonen et al. (2019), there can be a bidirectional association between the MSDs and ERI (RR 1.22, 95% CI = [1.00, 1.48]) and this should be considered in intervention design.
Psychosocial factors and MSDs are a global issue, as evidenced by this review that included articles from 16 different countries. Considering the different approaches to how work is performed, alongside varying forms of legislation governing workplaces practices in different countries, it is important to consider the global perspective when discussing this theme. Psychosocial factors continue to affect MSDs, notwithstanding recent policy agendas outlined by the ILO (Aleksynska et al., 2019). This underscores the pervasive nature of this relationship, despite recent efforts to curb its impact. The importance of social supports in workplaces and the associations with teams, as well as support from managers and supervisors must be acknowledged and these staff must be trained appropriately. Impactful, multicomponent interventions should be delivered at differing levels, that is, individual and organizational, to enhance the psychosocial work environment and reduce MSDs.
A strength of this study is the systematic review methodology employed. In addition, the inclusion of only longitudinal, stability-controlled studies enhances the value of this study. Other strengths include the focus on contemporary literature, further reinforcing the persistent relationship between MSDs and psychosocial factors. A limitation of the study is the inclusion of some studies that did not specify the industry or type of workers in the study population, making it difficult to include the context of the physical work environment. The authors, to the best of their ability, aggregated industries based on what was described in included articles, and these results were described in the “Results” section. A further limitation is the lack of documentation of effect sizes for some stressors and the absence of lower extremity MSDs, which is similar to the findings of Lang et al. (2012). In addition, there was no consideration given to shift work or overtime and the impact of these workplace factors on MSDs. Finally, the lag time from search to submission is acknowledged, and that it is likely that additional studies have been published since May 2020 that would meet the inclusion criteria for the review.
Future longitudinal research should consider the bidirectional associations between psychosocial workplace factors and MSDs (Halonen et al., 2018; Magnusson Hanson et al., 2017). There is scope to implement interventions that buffer the impacts of an adverse psychosocial work environment to minimize the risk of MSDs. Interventions need to include both mechanical and psychological components (Herin et al., 2012). Existing and novel interventions need to be evaluated to ensure efficacy.
Conclusion
This review supports the theory that MSDs have a multifactorial, complex etiology that includes psychosocial factors that exist within a global framework as noted with the various locations of studies included in this review.
This article identified that there were more studies that had investigated MSDs associated with office environments and computer workstations, which may be a result of the increased use of computers in the workplace more globally. Other studies considered professional drivers, manufacturing, and production; however, it is important to also consider blue-collar industries where other factors may influence the incidence of MSDs, including factors such as job demands, job control, job strain, job type, and job security, which have been highlighted across industries. In addition, increasing automation is permeating into blue-collar industries, with greater emphasis on operators using computerized systems, and this warrants further investigation of the unique psychosocial factors associated with these changing work roles.
This study highlights the disproportionate examination into some anatomical body regions (lower back, shoulder, and neck), which may be related to the incidence of workplace injuries. However, consideration of other body regions is recommended in future research to foster a more homogenized evidence base and establish the link between psychosocial factors and various MSDs. This review posits that the workplace has a significant role in the MSDs and psychosocial interface and therefore the workplace is in an ideal position to change work practices and policies to mitigate and reduce these risk factors.
Implications for Occupational Health Practice
This review underscores the notion that MSDs have a complex etiology, with psychosocial factors potentially playing an underlying role in their development. This article highlights that studies that were in office environments, and utilized computer workstations, were associated with MSDs in anatomical body regions including the lower back, shoulder, and neck. This was in conjunction with psychosocial factors, such as job demands, job control, job strain, job type, and job security. This relationship presents a future challenge for occupational health and safety practitioners, considering increasing automation associated with modern occupations. Potential remedies may include appropriate office ergonomics and training to mitigate MSDs in upper body anatomical regions that are more synonymous with office work and, in addition, understanding the role of the supervisor in work delegation and job demands.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231193578 – Supplemental material for Workplace Psychosocial Factors and Their Association With Musculoskeletal Disorders: A Systematic Review of Longitudinal Studies
Supplemental material, sj-docx-1-whs-10.1177_21650799231193578 for Workplace Psychosocial Factors and Their Association With Musculoskeletal Disorders: A Systematic Review of Longitudinal Studies by Aaron Bezzina, Emma Austin, Ha Nguyen and Carole James in Workplace Health & Safety
Footnotes
Acknowledgements
The authors wish to acknowledge and thank Debbie Booth, medical librarian, for her help in formulating the search strategy. In addition, the authors wish to thank Ishanka Weerasekara for her assistance with article screening.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by funding from the Center for Work, Health and Safety G2000210.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.