
Abstract
Background:
Work-related musculoskeletal disorders (WMSDs) are prevalent among healthcare professionals, including nurses, therapists, doctors, and paramedics, due to the potential injuries incurred during patient transfer and handling. This review aimed to assess the effectiveness of existing interventions in reducing the risks of WMSDs in this population.
Methods:
Four databases including PubMed/MEDLINE, Web of Science, Scopus, and ScienceDirect were searched to identify randomized and nonrandomized controlled trials, as well as studies with pre-post design. Two reviewers independently extracted data and assessed the quality of the included studies using the Effective Public Health Practice Project criteria. A meta-analysis was performed to obtain quantitative results.
Results:
A total of 40 studies were included in the review. Among the interventions, motorized assistive devices showed the most significant relative reduction in WMSD risks (p < .0000; standardized mean difference [SMD] = −3.32, 95% confidence interval [CI] = [−4.53, −2.12]), followed by combined interventions of cognitive and exercise (p < .0001; SMD = −0.62, 95% CI = [−0.91, −0.33]), combined intervention of cognitive and assistive device intervention (p = .02; SMD = −0.77, 95% CI = [−1.42, −0.12]), nonmotorized assistive device (p = .02; SMD = −0.63, 95% CI = [−1.15, −0.12]), cognitive intervention (p < .0001; SMD = −0.62, 95% CI = [−0.91, −0.33]), and physical exercise (p = .06; SMD = −0.16, 95% CI = [−0.32, 0.00]) intervention.
Conclusion:
The overall evidence indicates that interventions have a significant effect in reducing the risk of WMSDs among healthcare workers, with motorized assistive devices showing the most promising results. The findings from this review can provide valuable guidance for hospital administrators, policymakers, and other experts in implementing effective strategies to prevent WMSDs among healthcare professionals.
Keywords
Background
Work-related musculoskeletal disorders (WMSDs) are a major health issue affecting healthcare professionals. According to the U.S. Bureau of Labor Statistics, in 2018, as many as 56,360 healthcare professionals in the United States reported occupational injuries, one of which being musculoskeletal discomfort. Among all the healthcare professionals, nursing aides and registered nurses recorded the highest percentage of WMSDs due to their high exposure to such injuries in their daily work (U.S. Bureau of Labor Statistics, 2020). They are often predisposed to the most physically demanding tasks such as manual handling of patients, and rapid repetitive work movement. Furthermore, these tasks often involve overexertion and awkward postures (Davis & Kotowski, 2015). For example, patient handling requires lifting and bending, twisting, pushing, or pulling postures (U.S. Bureau of Labor Statistics, 2020). These awkward postures can lead to a higher risk of musculoskeletal injuries, particularly over the lower back region (Jäger et al., 2013).
Apart from physical injuries, WMSDs can also result in considerable indirect effects such as financial consequences. For instance, absenteeism resulting from WMSDs causes reduced earnings for individuals and an increased healthcare service costs (Suni et al., 2018). In the United States, such absenteeism was significant as it accounted for 34% of all workdays lost. In addition, WMSDs increase the entire amount of employees’ remuneration by 33% due to the compensation for their injuries (U.S. Bureau of Labor Statistics, 2020). To safeguard the welfare of healthcare professionals, proper management of WMSDs is essential so that high-quality care can be provided to those in need so that the expenses associated with absence from work can be kept to a minimum (Andersen & Mikkelsen, 2008; Koklonis et al., 2021).
All healthcare institutions are required to implement health, safety, and environmental policy that can ensure the worker safety of. A data-driven approach to identify effective interventions can lead to sound guidelines and implementation. Interventions for WMSDs can come in various forms of varying effectiveness, including assistive devices, exercises, training, as well as policies and procedures. Most studies that evaluated assistive devices, educational, physical activity, or policy interventions on patient handling have been associated with some success in reducing healthcare workers’ injuries (Aslam et al., 2015). Yet, there was conflicting evidence concerning the efficacy of these interventions (Richardson et al., 2018). For example, randomized trials (randomized controlled trial [RCT]) showed that mechanical and other assistive devices for patient handling could improve fatigue, back and shoulder pain, and physical discomfort in nurses (Yassi et al., 2001). However, two other RCTs found no effects of these interventions (Knibbe & Friele, 1999; Koppelaar et al., 2012). Therefore, a meta-analysis on this subject would be beneficial to provide an in-depth understanding of relevant research, especially the statistical impact of interventions used to prevent or minimize WMSDs among healthcare workers.
To date, several published systematic reviews addressing strategies in the form of mechanical assistive devices, nondevices (i.e., training, exercises, and policy), and combined strategies to lessen or prevent WMSDs among healthcare professionals have been published (Albanesi et al., 2022; Wåhlin et al., 2022). Some studies focused on one particular intervention (e.g., manual handling training) (Clemes et al., 2010) or the use of small aids (Freiberg et al., 2016), whereas the remaining studies focused on a specific group of medical specialists, that is, nurses or physical therapists (Anderson & Oakman, 2016; Clari et al., 2021; Gideon Asuquo et al., 2021; Richardson et al., 2018). One study only examined pain as the outcome (Van Hoof et al., 2018). Even though some published systematic reviews have shown the overall effectiveness of certain interventions to prevent WMSDs among healthcare workers, meta-analyses on this subject remain limited. Thus, the relative merit of each intervention has not been ranked. Teeple et al. (2017) performed a meta-analysis on safe patient handling and mobility programs. However, no comparison on the effectiveness of each intervention based on the primary outcomes of WMSDs was available from the published studies.
This article, to our knowledge, was the first to apply a meta-analysis to statistically evaluate and rank the effectiveness of the available interventions to reduce the incidence of WMSDs among healthcare professionals. The findings will be a crucial risk management tool for healthcare professionals to decide which intervention should be utilized to lower the risk of WMSDs among healthcare professionals. This review also aimed to identify strategies that might prevent WMSDs and their associated morbidity so that absenteeism can be reduced, and patient care will not be compromised.
Methods
This systematic review was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. Table 1 lists the inclusion and exclusion criteria for the review based on the research question that was generated using the Population, Intervention, Comparison, and Outcome (PICO) framework. The various interventions to lessen WMSDs were described after relevant published literature was retrieved, summarized, and assessed. The Quality Assessment Tool for Quantitative Studies of Effective Public Health Practice Project (EPHPP) was utilized to assess the quality of the studies.
PICO and Inclusion Criteria
Note. PICO = Population, Intervention, Comparison, and Outcome; WMSD = work-related musculoskeletal disorder.
A systematic search of the literature was performed using PubMed/MEDLINE, Scopus, Web of Science, and ScienceDirect. Articles published between January 2000 and September 2022 were screened. The details of the search terms are shown in Supplemental File 1. The search was conducted using Boolean operators (AND, OR). However, for PubMed/MEDLINE, truncation and Boolean operators (such as nurs* for the nurse, nurses, and nursing) were combined. The various search techniques were used in accordance with the respective database. An additional manual search of the list of references in each study was also performed to further identify any relevant studies. Peer-reviewed articles reporting RCT and non-RCT, as well as research employing pre-post designs were included. In contrast, articles in the form of reviews, case reports, commentaries, dissertations, guidelines on safety practice (handling and positioning), as well as research of prevalence or retrospective studies with no intervention or among nonhealthcare worker population were excluded.
Definition of Intervention
There was a wide range of interventions being evaluated in the literature. Therefore, we categorized the interventions into six groups based on the features of the interventions, that is, (a) motorized assistive devices (powered lift systems such as ceiling lifts); (b) nonmotorized assistive devices (sliding board, foot gel pad, and others); (c) cognitive (education and training of healthcare workers in practical, safe patient handling and movement training, ergonomics, stress management, and coaching); (d) exercise (physical exercise intervention such as neuromuscular exercise); (e) a combination of cognitive and exercise; and (f) a combination of cognitive and assistive devices. Health-related primary outcomes assessed in this study include awkward postures, low back pain, spine compression load, muscle activity, discomfort, and perceived exertion. In this study, the variable awkward posture was used as an outcome variable rather than an exposure variable that contributes to the development of WMSDs. This was done to assess the effectiveness of interventions in improving or reducing the occurrence of awkward postures among healthcare workers. In the included studies, awkward posture was measured or assessed to determine the impact of the interventions on reducing the occurrence of awkward postures, which may in turn reduce the risk of developing WMSDs among healthcare workers.
Analysis
Two reviewers (N.S.S.A.H. and M.I.Z.R.) independently extracted the relevant data from the studies, including subject characteristics, number of participants, outcome measures, intervention protocols, and relevant results. To perform the meta-analysis, the number of participants, mean differences, and standard deviations were inserted into the template of Review Manager 5.3 software (The Nordic Cochrane Centre, Copenhagen, Denmark). Missing data or nonusable data were excluded from the meta-analysis. Missing numerical result data such as standard deviations were computed manually or replaced with accessible data using the Review Manager calculator. The inverse variance was used as a statistical method. Inverse variance is a statistical method used in meta-analyses to combine effect sizes from individual studies. It involves using the reciprocal of the variance (or standard error) of each study’s effect size as a weight for pooling the effect sizes in a meta-analysis. The rationale behind using inverse variance is that it accounted for the precision of individual study estimates and gave more weight to studies with larger sample sizes, which can help increase the statistical power of the meta-analysis. The random effects model was used to account for potential heterogeneity among the included studies. The random effects model takes into consideration both within-study and between-study variability and provides a more conservative estimate by accounting for the possibility that the true effect size may vary across studies due to differences in study design, population characteristics, and other factors. Standardized mean differences (SMDs) were calculated for the outcomes based on the change in the scores of means (postintervention minus preintervention) and standard deviations from the included studies as the effect measure.
To determine whether the results were robust to the assumptions of the meta-analysis, a funnel plot was generated and the heterogeneity between the studies was analyzed using I2 statistics (Higgins & Thompson, 2002). Based on the Cochrane guidelines, 0% to 40% may not be important; 30% to 60% may indicate moderate heterogeneity; 50% to 90% may indicate substantial heterogeneity; and 75% to 100% may indicate considerable heterogeneity. In this study, higher levels of heterogeneity may be expected due to variations in study designs, populations, interventions, or outcomes. Apart from that, effect sizes were estimated and reported on pooled forest plots for primary outcomes of WMSDs. Effect sizes were divided into four categories: no change (standard mean effect size = 0), minor effect (standard mean impact size = −0.2), medium effect (standard mean effect size = −0.5), and substantial effect (standard mean effect size = −0.8). Confidence intervals (CIs) were set at 95%.
Quality Assessment of Relevant Studies
To assess the methodological quality of each eligible study, the EPHPP was used (EPHPP, 2010). Six criteria graded on “1 = strong,” “2 = moderate,” or “3 = weak” are included in this tool for (a) selection bias; (b) research design; (c) confounders; (d) blinding; (e) data collection method; and (f) withdrawals/dropouts. Studies with no weak ratings and a minimum of four strong ratings were categorized as strong studies; studies with four strong/moderate evaluations and one weak rating were categorized as moderate studies; and finally, studies with two or more poor ratings were categorized as weak studies. In addition, the integrity of interventions and the use of appropriate statistical analysis were also taken into account. Each article was evaluated independently by N.S.S.A.H. and M.I.Z.R. Any disagreement was resolved by a third reviewer (Z.M.R.).
Results
A total of 156 records were retrieved when combining the results of each database search (Figure 1). Following the removal of duplicate records (n = 46), 110 unique records were identified. Of these, 55 were removed based on the title and abstract, leaving 55 potentially relevant publications for full review. After review, 25 publications were included, and 30 publications were excluded. Reasons for exclusion included the following: no specific intervention being tested, a non-nursing population was used, outcome(s) was irrelevant, country/language, not a peer-reviewed article (e.g., news report), or because the publication was a thesis/conference abstract. However, another 15 papers were identified from the screening of the reference lists. As a result, a total of 40 publications describing the efficacy of interventions in reducing WMSDs among healthcare workers were included in the final review meta-analyses. The meta-analysis excluded certain studies with missing data and unique outcome measures.
Flowchart Illustrating the Process of Identifying Relevant Literature.
A total of 40 articles assessing the efficacy of the interventions in reducing the primary outcomes of WMSDs compared with manual methods or no intervention were included. Table 2 shows the characteristics of the included studies as categorized into six groups according to the type of intervention. The majority of the studies focused on nonmotorized assistive device intervention (n = 14; 35.9%), followed by motorized assistive device intervention (n = 9; 25.6%) and cognitive (n = 8; 20.5%). Five of the studies (12.8%) focused on exercise and another five on combined interventions of cognitive and exercise (12.8%). The remaining four studies applied combined intervention of cognitive and assistive devices (n = 4; 10.3%).
Characteristics of the Included Studies
Note. CI = confidence interval; WMSD = work-related musculoskeletal disorder; EMG = electromyography; REBA = Rapid Entire Body Assessment ; FFP = firefighters/paramedics; MVC = maximum voluntary contraction; RR = rate ratio; RPE = rating of perceived exertion; ISO = International Organization for Standardization; LBP = low back pain; NRS = numerical rating scale.
In terms of study design, about one third (n = 23; 30.8%) used a pre-post research design. Another 12 studies were RCTs (n = 12; 33.3%), five were controlled clinical trials (n = 5; 33.3%), while one study (2.6%) was a non-RCT. All the studies encompassed a wide variation of study populations including nurses, nonregistered nurses, nurses’ aides, physical therapists, dentists, surgeons, paramedics, and healthcare employees. The studies also incorporated various interventions and reported a broad range of health-related primary outcomes, such as awkward postures, low back pain, spine compression load, muscle activity, discomfort, and perceived exertion.
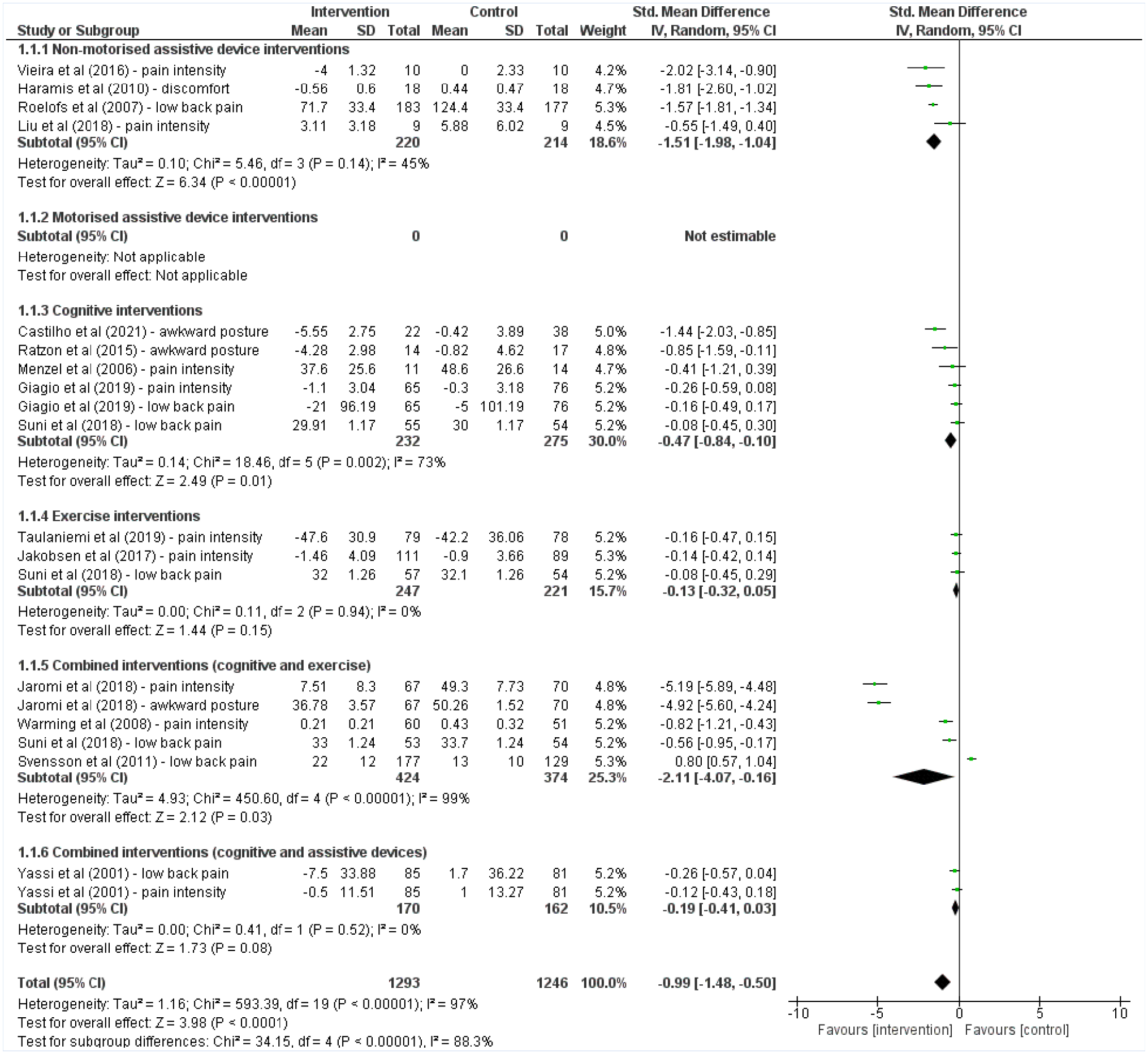
Overall, the results from the meta-analysis highlighted the effectiveness of the interventions in reducing the primary outcomes of WMSDs including awkward postures, low back pain, spine compression load, muscle activity, and discomfort related to WMSDs among healthcare workers. When ranking the efficacy of the interventions, the forest plot revealed that the reduction of primary outcomes of WMSDs among healthcare workers was most significant for motorized assistive devices (p < .0000; SMD = −3.32, 95% CI = [−4.53, −2.12]), followed by combined intervention of cognitive and exercise (p = .01; SMD = −2.42, 95% CI = [−4.26, −0.57]), combined intervention of cognitive and assistive device intervention (p = .02; SMD = −0.77, 95% CI = [−1.42, −0.12]), nonmotorized assistive device (p = .02; SMD = −0.63, 95% CI = [−1.15, −0.12]), cognitive intervention (p < .0001; SMD = −0.62, 95% CI = [−0.91, −0.33]), and finally, the physical exercise (p = .06; SMD = −0.16, 95% CI = [−0.32, 0.00]) as shown in Figure 2.
Forest Plot of the Impact of the Interventions on the Primary Outcomes of WMSDs (Awkward Postures, WMSD Injuries, General WMSD Pain Intensity, Low Back Pain Intensity, Muscle Activity, Discomfort, Perceived Exertion, and Spine Compression Load) Among Healthcare Workers.
Next, a total of 23 studies evaluated the effectiveness of assistive device intervention in mitigating the risks of WMSDs. Nine of the studies assessed motorized assistive devices, while 14 focused on nonmotorized assistive devices. All the 23 studies compared assistive devices with the manual method or no intervention. The most common outcomes reported in these studies were spine compression load, awkward posture, and muscle activation. One study also reported perceived exertion and pain intensity as outcomes. All nine studies that evaluated motorized assistive device were designed as pre-post research designs. They included the use of mechanically powered lift systems such as floor lifts (Iridiastadi et al., 2020), ceiling lifts (Miller et al., 2006), portable full-body or stand-up lifts (Li et al., 2004), powered beds with air-assisted device and the turn assist features (Budarick et al., 2020; Wiggermann, 2016, 2017; Zhou & Wiggermann, 2021), and tilting operating room table (Al-Qaisi et al., 2020) as interventions. Based on the results, most studies reported a significant improvement in the primary outcomes of WMSDs (SMD = −3.32, 95% CI = [−4.53, −2.12]).
In contrast, the use of the nonmotorized assistive device as an intervention to reduce the risk of WMSDs was evaluated in three RCTs, seven pre-post designs, two controlled clinical trials, and one non-RCT study. These studies focused on low-tech nonmotorized assistive devices aimed at minimizing the primary outcome of WMSDs, including a mat with an attached handle (Muto et al., 2008); unstable shoes (Vieira & Brunt, 2016); foot gel pads (Haramis et al., 2010); trouser with kneepads (Muto et al., 2008); friction-reducing sheet (Wiggermann et al., 2021); sliding board; walking belts (Muto et al., 2008; Zhuang et al., 2000); arm support exosuit (Liu et al., 2018); passive back-support exoskeletons (Hwang et al., 2021); postural monitoring and feedback device (Ribeiro et al., 2020); patient-handling slings (Elford et al., 2000); lumbar support (Roelofs et al., 2010); as well as extended handle stair chair, backboard wheeler, and descent control system for a stretcher (Lavender, Conrad, Reichelt, Kohok, et al., 2007). Similarly, most studies in this category also reported a significant improvement in the primary outcome of WMSDs (SMD = −0.63, 95% CI = [−1.15, −0.12]).
Next, the effectiveness of nondevice interventions compared with the manual method, or no intervention was investigated in 13 studies, whereby eight studies used cognitive interventions and five applied exercise interventions. Incidence or frequency of pain, pain intensity, and perceived exertion were the most commonly reported outcomes. A few studies also reported injury claims and costs. Moreover, five RCTs and three pre-post studies evaluated cognitive interventions that involved education and theoretical training in ergonomics, practical inward activities on safe patient handling, and cognitive behavioral therapy. From the findings, cognitive intervention was found to be effective in improving the primary outcomes of WMSDs (SMD = −0.63, 95% CI = [−0.91, −0.33]). However, the opposite was observed for exercise intervention as there were no significant differences between the experimental and control groups (SMD = −0.16, 95% CI = [−0.32, 0.00]) based on the results of the three RCTs and two pre-post studies.
In addition, nine studies evaluated the effectiveness of combined interventions in reducing the risks of WMSDs. The most common outcomes were incidence or frequency of pain, pain intensity, and perceived exertion. Five studies assessed a combination of cognitive and physical exercises (Járomi et al., 2018; Sezgin & Esin, 2018; Suni et al., 2018; Svensson et al., 2011; Warming et al., 2008), and four focused on combined interventions of cognitive and assistive devices (Dennerlein et al., 2017; Powell-Cope et al., 2014; Yassi et al., 2001). For combined interventions of cognitive and physical activity, two studies were designed as RCTs and pre-posts, respectively, while one study was a controlled clinical trial. Most studies reported significant primary outcomes of WMSDs (SMD = −2.42, 95% CI = [−4.26, −0.57]). Similarly, the combination of cognitive and assistive device interventions was evaluated in one RCT and three pre-post designs. All studies reported significant treatment effects on the risk of WMSDs (SMD = −0.77, 95% CI = [−1.42, −0.12]).
Based on the results of 40 studies evaluating the effectiveness of various interventions in reducing the risks of WMSDs, a funnel plot of the intervention effect against standard error was plotted (Figure 3). It was relatively symmetrical with a slight left skew, thus indicating the absence of or low publication bias. The largest studies with the smallest standard errors were located at the top of the plot. In the absence of bias, the results from small studies were scattered widely at the bottom of the graph, with a narrowing spread observed among larger studies. Four studies on motorized assistive devices had extremely large effects.
Forest Plot of Sensitivity Analysis Including Only RCTs (Impact of Study Design on Meta-Analysis Results).
To assess the robustness of our findings, we performed a sensitivity analysis by excluding non-RCT studies from our meta-analysis. The forest plot of intervention effects for reducing the risk of WMSDs among healthcare workers showed that motorized assistive devices ranked first in the original analysis, followed by combined interventions of cognitive and exercise, combined interventions of cognitive and assistive devices, nonmotorized assistive devices, and exercise interventions as illustrated in Figure 2. However, in the sensitivity analysis where only RCT studies were included, the ranking of interventions changed. The combined interventions of cognitive and exercise ranked first, followed by nonmotorized assistive devices, combined interventions of cognitive and assistive devices, and exercise interventions as shown in Figure 4. Notably, motorized assistive devices, which were included in the original analysis but not in the sensitivity analysis as they were non-RCT studies, did not appear in the sensitivity analysis. This suggests that the inclusion of non-RCT studies may have influenced the ranking of interventions in the original analysis and highlights the importance of considering study design in interpreting the results of our meta-analysis.
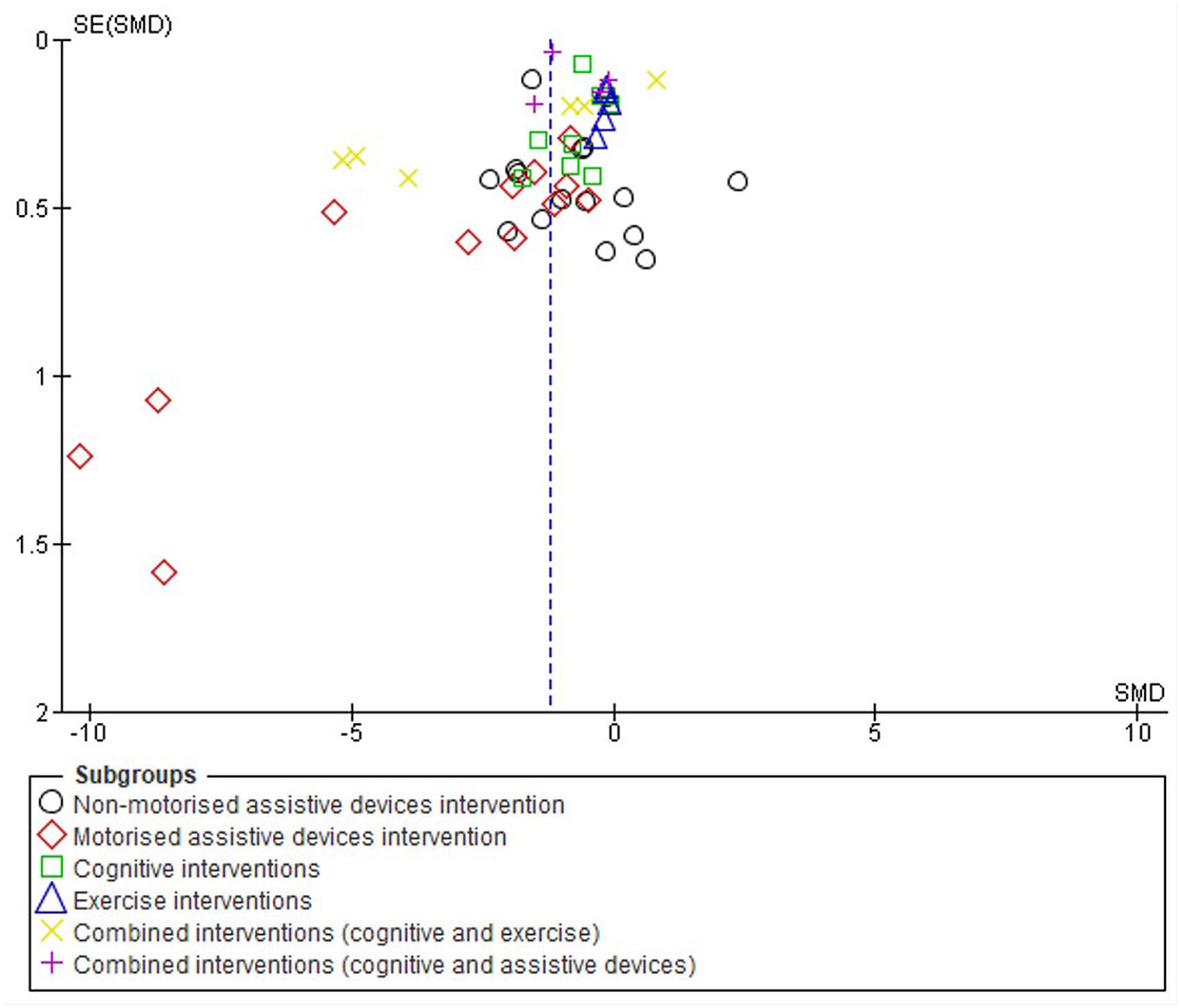
Funnel Plot for Publication Bias of Included Study by Standardized Mean Difference (SMD) and Weight. Note the Symmetry With Slight Left Skewness.
Table 1 and Supplemental File 2 outline the study quality. According to the EPHPP criteria, seven (17.5%) of the 40 studies were rated as strong, while another 14 (35.0%) and 19 (47.5%) were rated as moderate and poor quality, respectively. Most studies did not meet the requirements of blinding the individuals and the healthcare workers as it did not seem possible with respect to the study method. In addition, the blinding of assessors was not reported in most cases, thus resulting in a weak score for this item. Most pre-post design studies were rated as high risk of bias compared with studies with control groups, due to several reasons, including insufficient description of the randomization, confounding bias, regression to the mean, and Hawthorne effect.
Discussion
The systematic review and meta-analysis of interventions to reduce the risk of WMSDs were performed to estimate the quantitative impact on primary outcomes of WMSDs among healthcare workers and to identify the interventions with greater efficacy. The results showed that the overall intervention effect significantly reduced the primary outcomes of WMSDs (p < .00001). Across various types of interventions, the most significant WMSD risk reduction was observed for motorized assistive device interventions, followed by cognitive interventions. Combined interventions of cognitive and exercises, nonmotorized assistive devices, and combined interventions of cognitive and assistive devices were also found to be effective in reducing the risk of WMSDs. In contrast, physical exercise intervention was comparatively less effective.
In accordance with previous studies, significant intervention effects were observed for assistive devices, of which motorized assistive devices were found to be the most effective intervention in reducing the risk of WMSDs (Abdul Halim et al., 2023; Aslam et al., 2015). The use of technologically advanced assistive devices like a motorized portable lift, air-assisted devices, and powered beds imposed less awkward postures, physical demand, pain intensity, and discomfort than a nonmotorized assistive device (Budarick et al., 2020; Hwang et al., 2019; Iridiastadi et al., 2020; Miller et al., 2006; Wiggermann, 2017; Zhuang et al., 2000). Nevertheless, our analysis found that nonmotorized assistive devices were also effective in reducing WMSD risks. A recent study showed that the use of unstable shoes reduced pain intensity in nurses by strengthening muscle function, consequently ameliorating the stability of the body and reducing spinal tension (Lerebourg et al., 2020; Vieira & Brunt, 2016). Unstable shoes refer to shoes that have rounded soles that promote continual activation of stabilizing muscles in the lower limb and back for balance. They expose individuals to instability, aiming to train ankle muscles and improve postural control and are being evaluated as a potential intervention for managing low back pain. However, the use of a more manual and hands-on approach when operating nonpowered assistive devices such as applying walking belts to transfer patients generally demonstrated a greater degree of muscular activity. Similarly, the use of friction-reducing sheets and sliding board for patient transfer also showed similar muscle activity in the erector spinae compared with the nonassistive device condition associated with the L5/S1 moment (Zhuang et al., 1999). Therefore, regular use of appropriate assistive devices is essential to lower physical load accumulation so that the prevalence of WMSDs can be reduced.
Very often, poor knowledge among healthcare workers on correct manual handling or the use of aids and procedures predisposes their musculoskeletal system to lifting trauma. Garzillo et al. (2020) noted that healthcare workers who have received inadequate training were at a greater risk of developing WMSDs. Knowledge and information on safe patient handling should be communicated in a timely manner and updated regularly. Our analysis showed that cognitive intervention involving education and training approaches in practical and safe patient handling, coupled with movement training, ergonomics, stress management, and a coaching program, significantly reduced musculoskeletal pain. This is in line with previous studies in which healthcare professionals who received intervention managed to improve their postures and performed less biomechanical mistakes compared with the control group that received no intervention (Aslam et al., 2015). An individually customized education and training program is considered the primary level of prevention because it strengthens healthcare workers’ awareness of safe patient-handling procedures and enables them to develop proper handling techniques and skills (Garzillo et al., 2020).
The importance of strengthening the physical capacity of healthcare workers through physical exercises has been emphasized in previous research as it may prevent WMSDs (Jakobsen et al., 2017; Suni et al., 2018; Taulaniemi et al., 2019). However, our results showed that physical exercise was a comparatively less effective intervention in reducing low back pain among healthcare workers. One possible reason could be the long duration of the exercise program which lasted 6 weeks and up to 6 months in several studies, causing a low compliance rate and making it less effective in reducing low back pain and other work-related measurements (Jakobsen et al., 2017; Suni et al., 2018; Taulaniemi et al., 2019). A supervised exercise program of 6 months could also be expensive (Suni et al., 2018) to implement. It remains unknown whether a shorter program would have been as effective. Therefore, further research is needed to evaluate the successful components of this exercise intervention.
The introduction of assistive devices or physical exercises within a cognitive approach, including training and coaching, resulted in better outcomes in terms of WMSDs. The benefits of a combined intervention approach were reported for both intervention combination patterns in this review. This was in line with two other studies on WMSDs (Soler-Font et al., 2019; Zinzen et al., 2000) in which effective management required integrated and comprehensive strategies rather than isolated intervention (Macdonald & Oakman, 2015). Staff education on proper patient-handling techniques together with the use of appropriate assistive devices has been shown to reduce the rate of repeated musculoskeletal injuries (Lim et al., 2011). Improving healthcare workers’ awareness and knowledge of safe patient handling also enhanced their confidence in using assistive devices and other injury prevention practices. These results emphasize the need to practice combined interventions of cognitive and assistive devices or physical exercise interventions as they can increase work ability and reduce musculoskeletal symptoms, ultimately reducing the number of sick leave days for healthcare workers.
One limitation of our study is that a majority of the included studies were of pre-post design, which may have inherent limitations and a higher risk of bias compared with other study designs such as RCTs. The decision to include studies judged as weak was based on several factors. First, the availability of data on relevant outcome variables in the included studies, which contributed to the overall evidence base. Second, the need to capture a wide range of study designs and settings to provide a comprehensive overview of the topic was considered. Third, practical challenges in conducting controlled studies, particularly in the field of engineering controls, where blinding and randomization may not always be feasible or ethical due to the nature of the interventions and study population. Therefore, we conducted a sensitivity analysis that only included RCTs to examine the impact of these studies on the overall results. By including studies rated as weak, we were able to provide a more complete picture of the available evidence, even if some studies were of lower quality.
Conclusion
This systematic review provided important up-to-date evidence of the interventions used in reducing the risks of WMSDs among healthcare workers. This review followed a broad approach that encompassed a diversity of interventions and healthcare worker populations. The meta-analysis showed strong evidence that the interventions were beneficial in improving the primary outcomes of WMSDs. Assistive device intervention, particularly motorized assistive devices, and combined interventions were associated with the greatest effect on outcomes. Nonmotorized assistive devices and adequate cognitive programs for healthcare workers may also be beneficial. Hence, more efforts should be made to implement and expand these interventions in the healthcare setting. This review provided vital guidance for policymakers and healthcare managers in identifying the appropriate strategies to prevent and reduce WMSDs to safeguard the well-being of all healthcare professionals.
Implications for Occupational Health Practice
All healthcare institutions should implement comprehensive health, safety, and environmental policies to safeguard the health and safety of workers. This review used an evidence-based approach to identify effective interventions to mitigate the risks of WMSDs among healthcare workers. The findings provide important guidance for policymakers and healthcare managers to identify and implement the appropriate strategies to prevent WMSDs and their associated morbidity. By ensuring the health and well-being of all healthcare professionals, it is hoped that absenteeism can be reduced, and patient care will not be compromised.
In Summary
A meta-analysis statistically evaluates and ranks the effectiveness of the available interventions to reduce the incidence of work-related musculoskeletal disorders (WMSDs) among healthcare professionals.
Across various types of interventions, the most significant WMSD risk reduction was observed for motorized assistive device interventions, followed by cognitive interventions.
Combined interventions of cognitive and exercises, nonmotorized assistive devices, and combined interventions of cognitive and assistive devices were also effective in reducing the risk of WMSDs.
In contrast, physical exercise intervention was comparatively less effective.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231185335 – Supplemental material for Efficacy of Interventions in Reducing the Risks of Work-Related Musculoskeletal Disorders Among Healthcare Workers: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-whs-10.1177_21650799231185335 for Efficacy of Interventions in Reducing the Risks of Work-Related Musculoskeletal Disorders Among Healthcare Workers: A Systematic Review and Meta-Analysis by Nur Shuhaidatul Sarmiza Abdul Halim, Zaidi Mohd Ripin and Mohamad Ikhwan Zaini Ridzwan in Workplace Health & Safety
Supplemental Material
sj-docx-2-whs-10.1177_21650799231185335 – Supplemental material for Efficacy of Interventions in Reducing the Risks of Work-Related Musculoskeletal Disorders Among Healthcare Workers: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-whs-10.1177_21650799231185335 for Efficacy of Interventions in Reducing the Risks of Work-Related Musculoskeletal Disorders Among Healthcare Workers: A Systematic Review and Meta-Analysis by Nur Shuhaidatul Sarmiza Abdul Halim, Zaidi Mohd Ripin and Mohamad Ikhwan Zaini Ridzwan in Workplace Health & Safety
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Collaborative Research in Engineering, Science and Technology Center (CREST) (T11C2-18), Freedom Med International Sdn. Bhd. (T11C2-18), and Universiti Sains Malaysia (304/PMEKANIK/6050413/C121).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.