
Abstract
Background:
Healthcare and social assistance workers are at increased risk for obesity. This industry has limited access to workplace health promotion resources and reports low rates of physical activity programs for workers.
Methods:
This article describes the application of the PRECEDE–PROCEED Model (PPM) to plan, implement, and evaluate a pilot physical activity intervention, Project Move, tailored to promote occupational physical activity and reduce sedentary behaviors among female workers. Actions taken by the community-based participatory research partnership assisted in the identification of the predisposing, reinforcing, and enabling factors that influenced the physical activity behaviors of female workers. The resources and capacities of the partnership were leveraged to implement and evaluate the pilot intervention.
Findings:
After the 12-week intervention, the participants’ daily average steps while at work met the recommended minimum 7,000 steps/day, and the time spent sitting decreased along with positive changes in health-related psychosocial measures.
Conclusions/Application to Practice:
The PPM represents a feasible approach for community-based participatory partnerships to create a tailored intervention to address the occupational physical activity and sedentary behaviors of at-risk female healthcare and social assistance workforce.
Keywords
Background
Healthcare and social assistance industry workers are at an increased risk for obesity. The healthcare and social assistance industry has the highest overall age-standardized prevalence of obesity at 32% (Jackson et al., 2016). Only 28.5% of U.S. worksites offer any type of physical activity (PA) programs, with 33.3% of those programs within the healthcare and social assistance industry (Centers for Disease Control and Prevention [CDC], 2018). Out of the worksites that offer PA programs, less than 20% use evidence-based strategies, which may account for the estimate that less than 50% of employees participated in PA programs.
Updated guidelines for PA have called for adults to move more and sit less throughout the day (U.S. Department of Health and Human Services [HHS], 2018). Recommendations incorporate the need to not only increase amounts of regular moderate-to-vigorous PA (MVPA) but to also reduce the amount of sedentary behavior (SB). Some health benefits are gained for adults who sit less and do any MVPA. Substantial health benefits can be gained for adults who do at least 150 minutes to 300 minutes of MVPA. Despite these recommendations, most U.S. adults do not meet the PA guidelines (Elgaddal et al., 2020).
Researchers have explored the differing health effects of leisure time physical activity (LTPA) and occupational physical activity (OPA; Cillekens et al., 2022; Parker et al., 2021; Prince et al., 2021). Occupational tasks, such as carrying and lifting, have been shown to increase the risk of cardiovascular disease, mortality, and long-term sickness absence. High-stress occupational workloads, such as during the COVID-19 pandemic, led to dramatic reductions in LTPA for frontline workers (Magnavita et al., 2020). Independent of PA, risks for morbidity and mortality are higher for those who engage in greater amounts of SB (Cavallo et al., 2022; Gomez et al., 2022; Silveira et al., 2022). There is emerging evidence that PA interventions should include a focus on reducing SB (Dunstan et al., 2021). Workplace health promotion efforts may be able to reduce health risks by developing interventions that address the PA paradox (LTPA vs. OPA) as well as the SB of workers.
Workplace PA research has shown evidence that worksite policies promoting PA reduce sedentary time and improve work performance (Pronk, 2022; Pronk et al., 2012). Strategies for encouraging active workplaces include active workstations, portable exercise machines, PA breaks, prompting software, and skip-stop elevator use (Pronk, 2022). Examples of workplace policies supporting PA include active meetings (e.g., walking, standing, moving, and stretching), allowing 10 to 15 minutes per day allocated either as intentional activity while on the clock or a movement break at a specified time and location, flextime to incorporate PA into workday, subsides for active commuting, and promoting walkable locations around the worksite (Ablah et al., 2019). The 2018 Physical Activity Guidelines Advisory Committee (PAGAC, 2018) found strong support for using wearable devices, web-based interventions, and mobile phone strategies in worksite PA interventions.
The probability of employees meeting PA guidelines is increased when worksite PA policies address the worksite barriers and facilitators to PA (Bailey et al., 2018). Incorporating environmental worksite supports, such as maps of walking/biking routes, shower facilities, and the encouragement of workers to stay active while at work can contribute to increased PA (Dale et al., 2019; Hye-Jin & Choo, 2018; Suhaimi et al., 2022). Incidental PA and increasing the number of steps taken during the day could be a viable means to enhance cardiorespiratory fitness, decrease sedentary time, and lower all-cause mortality (Forberger et al., 2022; Saint-Maurice et al., 2020). Inexpensive innovations that call for policies that support OPA, including scheduled movement breaks, stair prompts, and routinized stretching have been suggested (Ablah et al., 2019).
This article describes the application of the PRECEDE–PROCEED Model (PPM) to plan, implement, and evaluate a pilot intervention tailored to promote OPA and reduce SB among female workers (Green & Kreuter, 2005). The pilot project was approved by the university’s institutional review board. This work addresses a gap in literature by describing how a community-based participatory research partnership used a health promotion framework to address the OPA and SBs of at-risk female healthcare and social assistance workforce.
Project/Program Methods
Project Move encouraged “moves” to reduce sitting and increase OPA among female workers at a multifaceted nonprofit community healthcare and social assistance provider. Project Move continues a community-based partnership between university faculty and this organization (Fetherman et al., 2020). The PPM addresses the multiple factors that contribute to health and health risks to improve quality of life and were applied to provide a structure for designing, implementing, and evaluating the project (Green & Kreuter, 2005). PRECEDE characterizes the processes that lead to the developing of the intervention (Phases 1–4), whereas PROCEED outlines the processes to consider when implementing and evaluating the intervention (Phases 5–8).
Social and Epidemiological Assessment (Phases 1 and 2)
Highlighted previously in this article, a review of PA literature, along with previous actions carried out by the research partnership through prior formative evaluations, informed social and epidemiological assessment (e.g., employee needs and interest survey, health fair survey, employee satisfaction survey, wellness champion feedback, site visit report, and the CDC’s Health ScoreCard; Fetherman et al., 2020). Most employee respondents were interested in self-managed (52%), onsite (67%) wellness activities in the areas of PA (67%) and weight management (61%) offered during work (38%; Fetherman et al.).
Behavioral, Environmental, Educational, and Ecological Assessment (Phases 3 and 4)
Evaluation results, coupled with a review of literature and partnership discussions, identified the ultimate desired targeted population of the PA intervention (e.g., female workers) and the most important and changeable factors that predispose, enable, and reinforce OPA behaviors at the workplace (Figure 1). More than 87% of the organization’s workers are women, with a high incidence of prolonged occupational sitting (Fetherman et al., 2020). Previous surveys also revealed that female employees faced barriers to LTPA and, as such, may find OPA interventions more appealing (i.e., fatigue/tiredness, childcare/family responsibilities, or second job responsibilities). Only obese, female workers were recruited through completion of the Physical Activity Readiness Questionnaire, self-reported PA levels of less than 10 minutes at a time, and a body mass index (BMI) range from 30.0 to 34.9 (Thomas et al., 1992). Twelve obese White female workers met eligibility requirements and volunteered for the pilot intervention. The average participant was 46 years old (SD = 9.40) and had a BMI of 32.80 kg/m2 (SD = 2.18). Participants included certified nursing assistants, nurses, and administrative office-based workers.
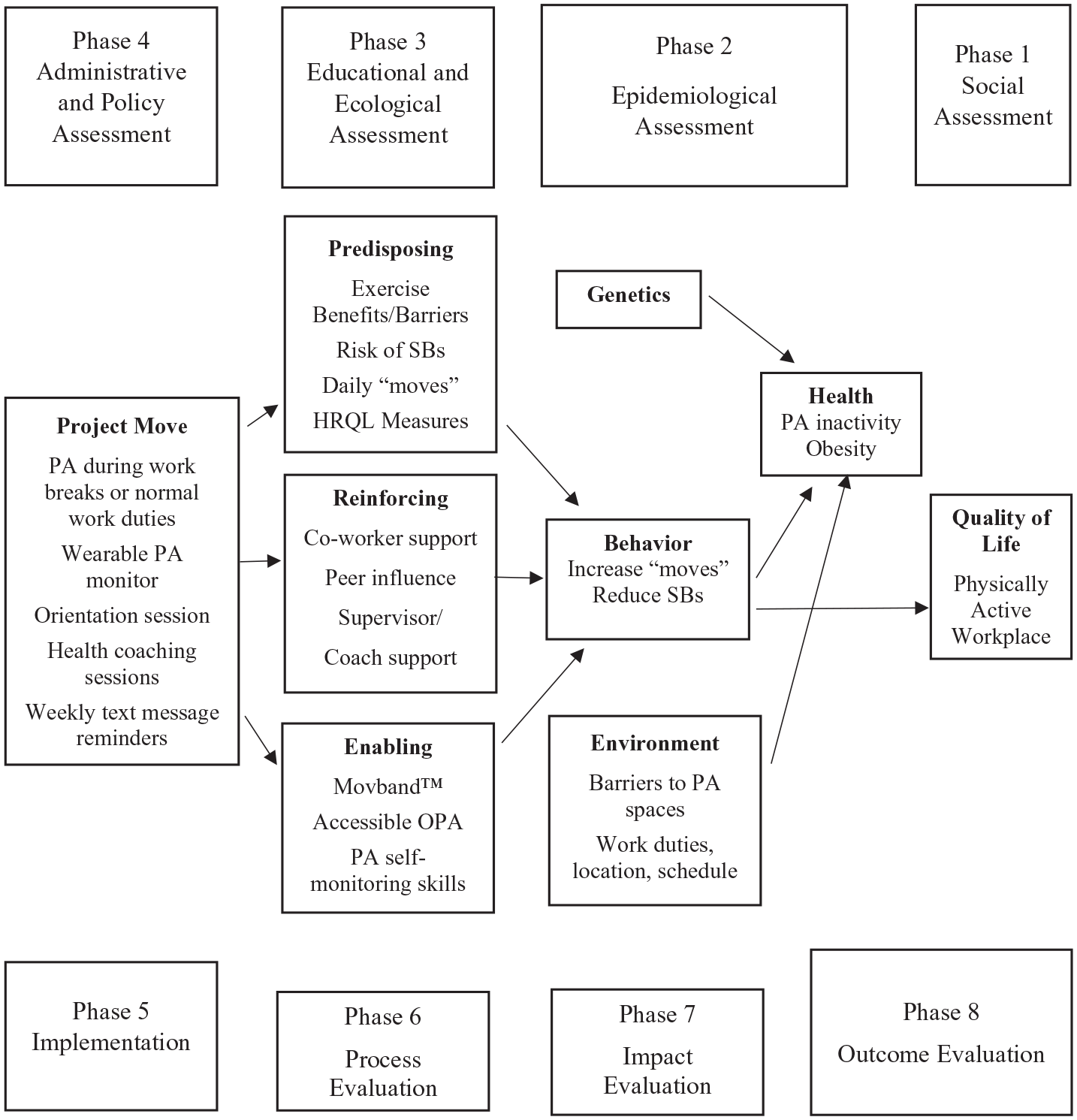
Application of PRECEDE–PROCEED to Project Move Intervention.
Behavioral strategies were embedded in the design to increase motivation and adherence to PA (i.e., key messaging, coaching, text messages, and wearable PA technology). See Table 1. Key messaging recommendations to promote PA were followed (Williamson et al., 2020). The intervention was simply named Project Move to increase “moves,” and a flyer announcing the project was disseminated throughout the organization and in the employee electronic newsletter.
Project Move Components.
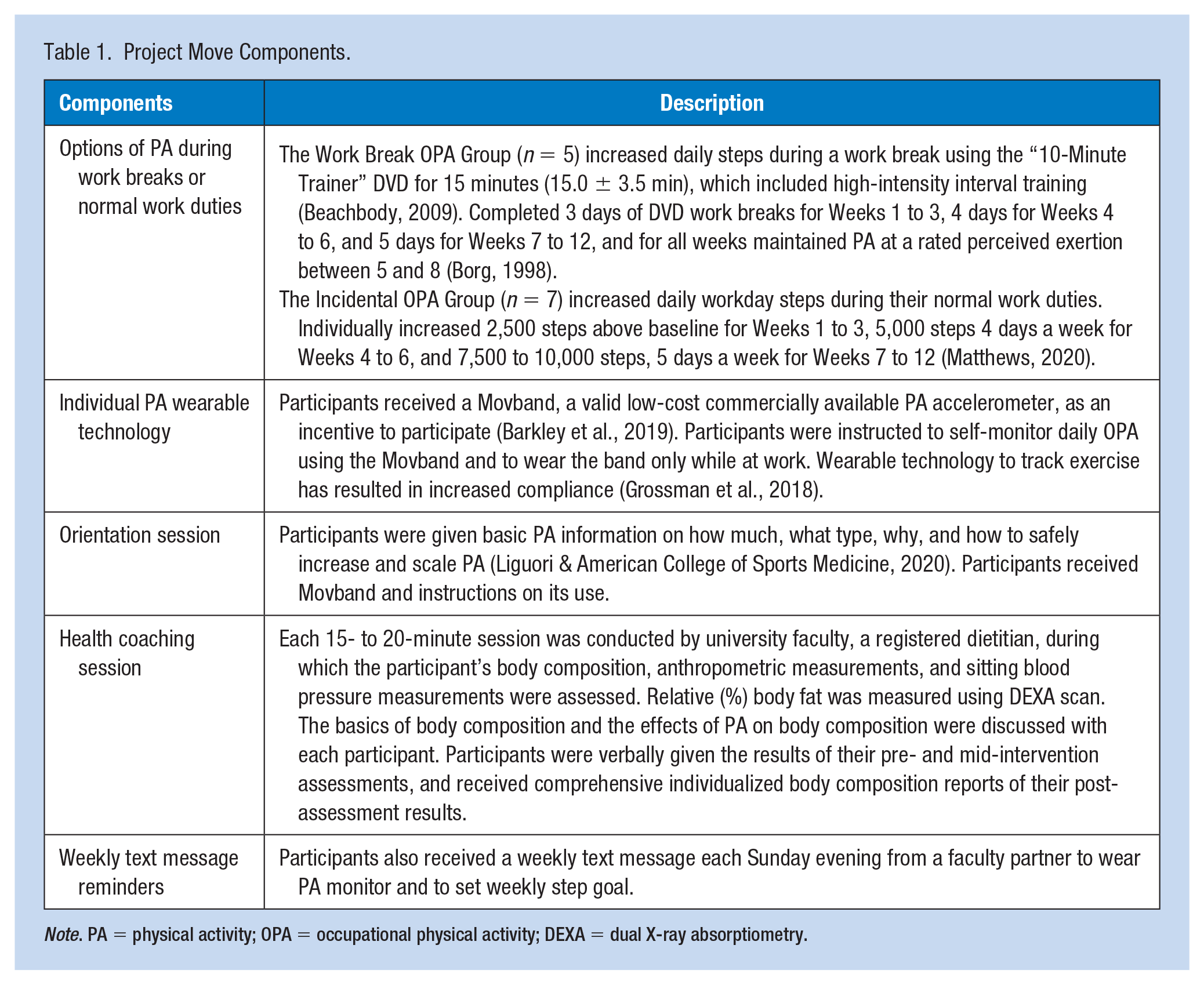
Note. PA = physical activity; OPA = occupational physical activity; DEXA = dual X-ray absorptiometry.
Administrative and Policy Assessment, and Implementation (Phases 5 and 6)
Administrative and policy assessment included reviewing lessons learned from the broader health promotion literature along with ongoing discussions with the organization’s chief executive officer, human resources director, wellness champions, and the wellness committee. Grounded in self-determination theory and goal-setting theory, the primary implementation considerations included policies and social and environmental strategies that supported OPA and, as highlighted earlier, evidence-based strategies such as individual PA self-monitoring and wearable PA devices (Locke & Latham, 1990; Ryan & Deci, 2000). For Project Move, a 12-week period was selected to be consistent with previous workplace PA interventions and to allow for evaluation of the impact of the intervention on OPA and SB. The interventions also included an orientation session, weekly text message reminders, and three health coaching sessions (pre-, mid-, and post-intervention; see Table 1).
To ensure accessibility to OPA and use of organizational facilities, female employees participated in Project Move during the workday, either during work breaks or nonessential workday activity. As PA can be impeded by work-specific demands, conditions, and resources, it was important to pilot these two strategies (Matthews, 2020). Based on worksite location and duties, the Work Break OPA group (n = 5) included administrative staff who had convenient access to a conference room and exercised either in a group of two or more, or individually, depending on the time of their work break. The Incidental OPA group (n = 7), comprising direct care staff, increased daily workday steps during their normal work duties. All participants were instructed to not engage in LTPA. Worksite PA interventions should be designed to consider employees’ control over factors influencing participation to ensure that participating in the intervention outweighs the disadvantages (Bredahl et al., 2019).
Process, Impact, and Outcome Evaluation (Phases 7–9)
Process evaluation focused on program adherence and how well intervention components were being implemented. Assessment of OPA was tracked using the Movband that each participant wore only during work hours. Participants maintained their normal daily OPA, the week prior to the intervention, to determine baseline OPA. Participants’ “moves” were downloaded weekly from the manufacturer’s site and recorded into an Excel spreadsheet with daily participant “moves” converted into daily “steps” as a daily step count is a more convenient way to monitor and set daily PA goals (Williamson et al., 2020). There is increasing evidence to support an inverse dose–relationship between daily steps and positive health outcomes (Kraus et al., 2018). Post-intervention participants’ daily average steps were used to assess the impact of Project Move on participants’ OPA (see Table 2).
Project Move Evaluation.
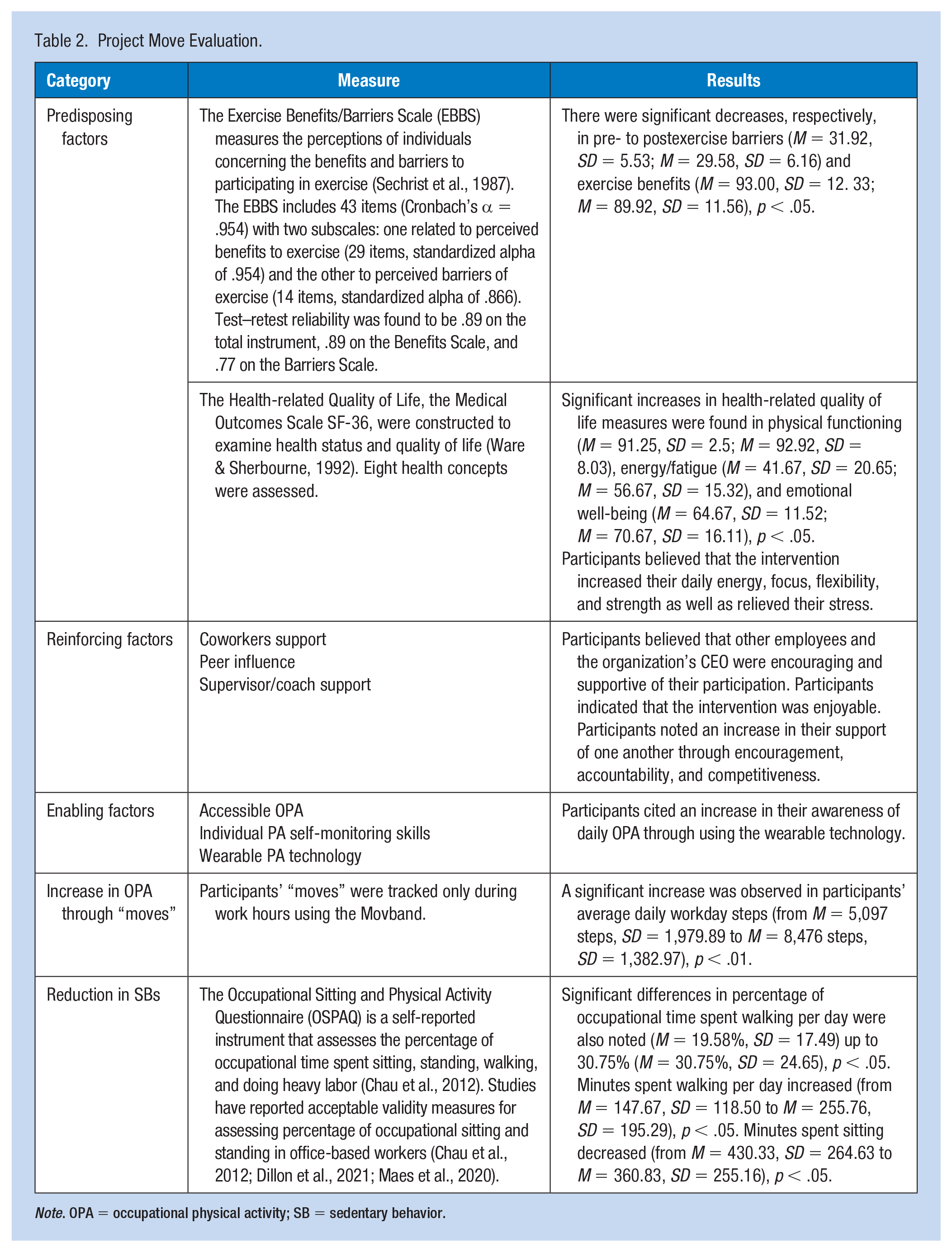
Note. OPA = occupational physical activity; SB = sedentary behavior.
As described in Table 2, impact evaluation was also conducted using evidence-based measures that were embedded into the intervention’s pre- and post-health coaching sessions and post-intervention. One-hour focus groups were also held for each OPA group during the workday at the organization’s conference room. Led by university faculty, the focus group discussion included seven semi-structured questions concerning participants’ beliefs and attitudes related to their participation in Project Move.
Findings
The primary desired impact of the intervention was achieved to increase participants’ OPA and reduce SBs. After the 12-week intervention, the participants’ daily average steps while at work met the recommended minimum 7,000 steps/day and time spent sitting decreased along with positive changes in predisposing, reinforcing, and enabling factors. Faculty partners created a simplified, two-page report on the impact of the intervention on participants, which included aggregate data on changes in occupational sitting, daily steps, health-related quality of life, exercise benefits/barriers, body composition, and participants’ perceptions. Descriptive and statistical analyses were examined using SPSS, Version 24. Impact evaluation was conducted using dependent t tests to determine the significance of participant changes from pre- to post-intervention, regardless of whether OPA was accomplished through a work break or daily work activity. Similarly, across focus groups, the intervention had position impacts on reinforcing and enabling factors. See Table 2 for impact results.
Discussion
The healthcare and social assistance workforce is at increased risk for obesity (Jackson et al., 2016). This industry has limited access to resources and reports low rates of PA programs among workers. Most worksite PA programs are difficult to implement and maintain; however, the implementation of PA programs can be enhanced using theoretical frameworks and planning models (Grønningsæter & Kiland, 2022). Research partnerships represent an approach to developing, implementing, and evaluating evidence-based worksite PA programs to meet workers’ needs (Magnavita, 2018). The Project Move partnership used the PPM to tailor the intervention to increase OPA and reduce SBs of female employees.
The partnership recognized the need to ensure accessibility to participants during their workday either during work breaks or incidental workday activity, use organizational facilities, and promote individual PA self-monitoring. The partnership used evidence-based strategies, such as wearable PA devices, policies that support OPA, as well as social and environmental supports to increase PA among participants. Behavioral strategies were embedded in the design to increase motivation and adherence to PA (e.g., key messaging, coaching, and text messages). Valid and reliable measures were used to evaluate the intervention’s impact (see Table 2).
There were limitations to the 12-week pilot intervention. Due to the length of the intervention and small group sizes, pre- and post-differences between groups were not evaluated and outcome evaluation was not feasible. It was not feasible to conduct outcome evaluation as a much longer follow-up period and larger sample would have been required. There were no changes in relative body measures, such as (percent) body fat or BMI. However, reductions, although not significant, were observed in body weight, biceps, waist, abdomen, hips, and thighs, all trending downward in movement toward reduced health risk. In addition, dietary behaviors were not measured during the intervention. Participants anecdotally noted reductions in stress; however, there were no direct measures of stress levels pre- or post-intervention. Future research could include larger group sizes participating in longer duration interventions that include pre- and post-measures of dietary behaviors, BMI, and stress levels.
Through a research partnership, the aim of this project was to tailor and pilot an OPA intervention that encouraged “moves” to reduce sitting and increase OPA. The participants’ daily average steps while at work met the recommended minimum 7,000 steps/day and time spent sitting also decreased, which may result in health benefits. Positive changes in health-related psychosocial measures were also found. Different types of OPA interventions may be effective for increasing PA, reducing SB, and enhancing health-related quality of life among female health and social assistance workers. Long-term partnership goals include implementing different types of PA interventions that encourage all employees to increase their “moves” through individual and group challenges using smartphone PA apps, wearable technology, and electronic or paper-based PA logs.
Applications to Professional Practice
Community-based research partnerships represent a feasible approach to translate the capacities and resources of each partner as they work together to reduce barriers and facilitate OPA among workers. Health promotion planning methods, such as the PPM, may assist in tailoring these interventions to meet workers’ OPA needs. Research partnerships may be essential methods to achieve adequate levels of OPA and reduce SBs in at-risk female workers.