
Abstract
Keywords
‘Religion and spirituality are also associated with higher levels of social support, which buffers the negative effects of stress on health, particularly for African Americans.’
In the United States, obesity is a major public health problem, with approximately 69% of adults being overweight and/or obese. 1 Individuals who are obese have an increased risk for morbidity and mortality associated with weight-related chronic illnesses, including heart disease, diabetes, and hypertension.2,3 The prevalence of obesity-related illnesses is higher among women, racial/ethnic minorities, and individuals from low-income populations.2,4,5
Past research suggests that religion and spirituality may influence health and health behaviors.6,7 A selective review exploring the associations between religion and spirituality, and physical health provides evidence that higher levels of religious strength are associated with lower mortality for healthy individuals and with increased preventive health behaviors, including flu shots, breast self-exams, and prostate and cholesterol screening among older adults.8,9 Religion and spirituality may influence health through several pathways.6,7 Both are a major source of personal strength and contribute a sense of purpose and meaning in life.6,7 Religion and spirituality are also associated with higher levels of social support, which buffers the negative effects of stress on health, particularly for African Americans. 10
The widely disseminated Diabetes Prevention Program (DPP) was designed to provide communities with evidence-based lifestyle change programs focused on preventing type 2 diabetes mellitus and has been successfully adapted for low-income and ethnic minority populations.11-13 The 1-year program consists of 16 weekly groups and 6 monthly sessions. The DPP aims to help participants lose 5% to 7% of their body fat by teaching them strategies for incorporating physical activity, developing healthy eating habits, and identifying barriers that interfere with success. There are multiple factors that contribute to success in achieving the outcomes of the DPP, including psychosocial health, particularly depression and anxiety, as well as eating habits, including binge eating.14-16 Psychosocial health and self-care are important modifiable predictors of weight loss.15,17 The DPP’s curriculum allows participants to enhance their abilities using problem-focused and emotion-focused coping, which have both been shown to be effective in weight loss outcomes.17,18 The focus on improving depression, anxiety, and healthy eating behaviors is effective for weight loss, but the implementations and adaptations of the DPP rarely incorporate spiritual or stress management components. Activating participants’ spirituality may enhance their motivation, goal striving, and self-regulation, which could then result in additional weight loss and weight loss maintenance.19,20
In the current study, we tested the feasibility and potential for effectiveness of a Health Empowerment Program (HEP) that combines components of the DPP program with a biopsychosocial-spiritual approach to promote behavior change and emotional well-being. Although the program was offered through a clinic run by the Sisters of St Joseph, the introduction of spirituality took a nondenominational perspective.
To test whether the aims of the program were being met by this intervention, we conducted an evaluation of behavioral and psychological data collected at baseline, posttest, and 3-month follow-up. The main outcomes of interest included individual changes in food consumption, exercise, motivation, mental health, and self-regulation.
Methods
The community-based participatory research (CBPR) approach was used to develop the HEP with both researchers and community partners taking an active role in the program development and research process. 21 CBPR has 9 principles, and in our partnership, we focused on the following aims: recognizing the community’s identity and their specific needs, fostering the community’s assets, creating an equal and collaborative partnership, colearning, distributing the results, and sustainability.21,22 The researchers initially approached St Joseph’s Neighborhood Center (SJNC) as part of the Rochester Program of Research and Innovation in Disparities Education, an innovative, experiential model for research and health disparities education. 23 SJNC is a nonprofit organization in Rochester, NY, that provides comprehensive health care, counseling, adult education, and social work to individuals and families who have no or insufficient health insurance and lack access to health care. SJNC serves approximately 3500 individuals per year.
The HEP was adapted from a 3-session, individual weight loss program that was created for patients at SJNC by a medical student volunteer. Feedback from the original program participants and from SJNC staff resulted in 5 major adaptations: (1) increasing the number of sessions to 7; (2) supporting maintenance adding a booster session 3 months after the last group, which includes strategies for maintaining weight loss and a cooking demonstration; (3) focusing on healthy lifestyle changes instead of weight loss solely; (4) addressing some of the economic, socioemotional (eg, stress), and psychological factors (eg, depression) that often create barriers for low-income individuals to make healthy lifestyle changes; and (5) explicitly incorporating spiritual factors, without limiting them to certain religions or denominations.6,7,9,24
Throughout the intervention development phase, SJNC was actively involved in revisions, data collection, and evaluation of the intervention effects. The aims of the program were as follows: (1) to promote weight loss through lifestyle change, including healthy eating and physical activity, (2) to promote biological, psychological, social, and spiritual health and well-being, and (3) to identify ways to reduce barriers.
A unique aspect of HEP is that it uses a biopsychosocial-spiritual approach to promote behavior change. The biological aspects of the program focused on education about obesity-related health risks and the promotion of health behaviors to reduce the risk for obesity-related illnesses. The social aspects of the program were using the group setting as a source of support anddiscussing the difficulties of making healthy changes in the context of family and friend networks (particularly around holidays), and open discussions of financial issues encouraged affordable approaches to health improvement. The psychological aspects included discussions about how depression and anxiety may lead to overeating and how stress reduction may reduce unhealthy behaviors. We demonstrated approaches to stress reduction through mindfulness exercises (visualization and meditation). Mindfulness exercises also focused on changing the particiant’s attitude about how they experience food and were aimed at helping participants develop heightened respect for the process of eating.
Although the program is offered through a clinic run by the Sisters of St Joseph, the introduction of spirituality took a nondenominational perspective. Program leaders discussed the possibility of using one’s relationship with a higher power to help with adherence to dietary and exercise recommendations. Specifically, group leaders focus on helping participants use their spiritual beliefs to identify their values and goals for healthy living as well as identify how their spiritual beliefs and practices can be a source of strength in their efforts to make healthy lifestyle changes.
The HEP consisted of 7 weekly 2-hour sessions and an hour-long booster session at 3 months. Sessions covered were as follows: (1) psychological, physical, social, and spiritual benefits of healthy living; (2) goals and obstacles to healthy living; (3) strategies for healthy living (nutrition, physical activity, and community resources); (4) how to budget for healthy living; and (5) maintaining a healthy lifestyle. Sessions were facilitated by study coordinators (ie, a psychology postdoctoral fellow and a registered nurse) and cofacilitated by a master’s or doctoral level mental health clinician. Guest speakers included a nutrition educator and a mental health counselor, both from SJNC. A repeated-measures, uncontrolled quasiexperimental design was used in this feasibility and evaluation study to assess individual change over time in variables of interest.
Participants (n = 153) were recruited from 2010 to 2013 through flyers at SJNC and by health professionals providing services at SJNC. All participants completed an initial interview and assessment after they signed informed consent. The original inclusion criteria were (1) individuals who were at least 18 years old and (2) had received medical and/or mental health care at SJNC. In the subsequent years of the program, individuals from other agencies, faith-based settings, and clinics were included if they signed a release of information to obtain health information from their health care providers. Individuals who were unable to communicate in English, pregnant women (because of medical concerns), and individuals who had moderate to severe cognitive impairments were excluded. SJNC serves approximately 3500 individuals per year. The required sample size (calculated using GPower V.3.1.6. to detect an effect size of d =0.20 at 95% power, α =.05, with 3 data points in a repeated-measure analysis) was 94. 25
Data were collected during the initial appointment (baseline), after completion of the 7 group meetings (posttest; week 7), and at a 3-month booster session, initially by the researchers and later by SJNC staff. Demographic information (gender, age, race/ethnicity, employment status, income, education level, and marital status) was collected during the initial meeting. At each time point, participants completed an assessment packet to self-report mental and physical health (ie, anxiety, depression, perceived stress, and activity level), spirituality, goal-directed behaviors, and self-regulation. Research assistants were available to assist participants in completing the questionnaires if any literacy or health literacy concerns arose. Body mass index, obesity-related health indicators, and open-ended questions regarding participant perception of the program were also collected at preintervention and postintervention and at 3-month follow-up. However, these data are not the focus of the current study. All scales were deemed valid and reliable in previous research and were chosen based on use in prior research and in diminishing participant burden.26-33 Demographic information was assessed using preset categories, and they were analyzed as categorical variables in all analyses. All outcome measures, as described below, were analyzed as continuous variables in the current study.
Mental Health Variables
Depression
The Patient Health Questionnaire (PHQ-9) is a 9-item self-report measure that assesses depressive symptoms within the past 2 weeks and was developed for primary care clinicians to diagnose depression. 34 Each item is rated on a 4-point scale ranging from 0 (not at all) to 3 (nearly every day). The PHQ-9 has been found to be valid and reliable in assessing depressive symptoms in samples comparable to the current study, including a high proportion of African American individuals and women.26,35 In our study, the Cronbach α was .88 for the PHQ-9.
Anxiety
Generalized Anxiety Disorder Questionnaire-7 (GAD-7) is a 7-item self-report scale that assesses anxiety symptoms within the past 2 weeks and was developed for primary care clinicians to diagnose generalized anxiety. Items are rated on a 4-point scale ranging from 0 (not at all) to 3 (nearly every day). 27 The GAD-7 has been found to be valid and reliable in assessing anxiety symptoms in multiple ethnic groups, both men and women, and early to older adulthood. 27 In our study, the Cronbach α was .92 for the GAD-7.
Current Stress Levels
The Perceived Stress Scale (PSS) is a 14-item scale that measures the degree to which one appraises situations in one’s life as stressful. It is designed for use with community samples with at least a junior high school education. 28 The PSS is composed of 7 positive items and 7 negative items. Responses are obtained using a Likert-type scale ranging from 0 (never) to 4 (very often). The PSS has been found to be valid and reliable in older adults as well as racial and ethnic populations similar to the current sample.28,36 In our study, the Cronbach α was .85 for the PSS.
Intrapersonal Variables
Self-regulation
Self-regulation Questionnaire, short form (SSRQ) is a 31-item measure that assesses self-regulatory processes that are related to behavior self-control and was derived from the Self-Regulation Questionnaire (SRQ).29,37 Each item is scored on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Higher scores on this measure represent increased self-regulation capacity. The SSRQ has been found to be valid and reliable, particularly in addiction studies.29,38 In our study, the Cronbach α was .95 for the SSRQ.
Goal Orientation
The Tenacious Goal Pursuit (TGP) Scale is a 15-item scale that assesses the tendency to persistently pursue goals even in the face of obstacles and a high risk of failure. 30 Each item is rated on a 5-point Likert-type scale ranging from strongly disagree (0) to strongly agree (4). The TGP had been found to be valid and reliable in samples similar to the current study (Mueller and Kim). 30 The Cronbach α was .75 for the TGP.
Spirituality
The Santa Clara Strength of Religious Faith Questionnaire (SCSORFQ) is a 10-item assessment, and it measures the strength of religious faith independent of one’ religious affiliation. 31 Each item is scored on a 4-point Likert-type scale, ranging from 1 (strongly disagree) to 4 (strongly agree). Higher scores on this measure represent increased religious faith. The SCSORFQ has been found to be valid and reliable in samples similar to the current study, including in ages ranging from young to older adulthood. 31 The Cronbach α was .96 for the SCSORFQ.
Health Behaviors
Exercise
The Godin Leisure-Time Exercise Questionnaire (GLTEQ) was used to assess participants’ weekly exercise behavior. The GLTEQ assesses participants’ frequency of mild, moderate, and strenuous exercise performed for more than 15 minutes during a typical week. 32 A total weekly leisure activity score is calculated by multiplying the frequency of mild, moderate, or strenuous exercise by 3, 5, and 9, respectively, and then summing the totals to obtain a numerical value. The GLTEQ has been found to be a valid and reliable measure with adults. 39 The Cronbach α was .62 for the GLTEQ.
Food Consumption
The Food Behavior Checklist (FBC) is a 16-item checklist that assesses fruit and vegetable consumption, food shopping, and preparation. 33 A numerical value is assigned for each endorsed response on the FBC; these values are then added to together to create subscale scores (eg, fat intake, diet quality) as well as a total FBC score. In regard to food consumption, this study specifically explored fat, cholesterol, and dairy intake as well as diet quality and security. The measure was developed for use with low-income populations. The FBC has been found to be valid and reliable for use in community nutrition interventions.33,40 The Cronbach α was .68 for the FBC.
A series of generalized estimating equations (GEEs) with repeated observations and identity link function were conducted to determine whether the HEP intervention predicted behavioral and psychological changes over time (using 3 time points), from baseline to 3-month follow-up. A GEE was fit to each outcome. GEE requires the specification of a repeated correlation structure (ie, working correlation structure) for each outcome variable, and each model was run with each of the 5 working correlation structures (ie, independent structure, exchangeable structure, m-dependent structure [or stationary structure], autoregressive correlation structure, and unstructured correlation structure) to determine the best-fitting structure. 41 There is no systematic way to determine the best correlation structure in GEE analyses. 41 However, it is suggested to use the Corrected Quasi Likelihood under Independence Model Criterion or QICC to guide the choice in the repeated correlation structure to fit each model in conjunction with an a priori decision on which structure best represents the correlations you would expect to find in the data. 41 Covariate selection was also theoretically driven and confirmed with use of QICC values to determine the best-fitting model for each outcome. We chose our models using the exchangeable working correlation structure matrix based on the assumption that the correlations between subsequent measurements were the same. 41 Models using all 5 working correlation matrix structures resulted in similar interpretations and, therefore, we chose to use the Exchangeable working correlation structure matrix. This decision was based on the QICC values and the assumption that the correlations between each subsequent measure would be the same. 41 χ2 Analyses of demographic variables were calculated to compare individuals who dropped out with those still enrolled at posttest through 3-month follow-up. A priori we decided that demographics, including socioeconomic status, would influence the association between the HEP program and mental health, health behavior, and intrapersonal variables. Thus, the potential covariates included income level, marital status, education, employment status, and racial/ethnic identity. With each outcome we analyzed, we fit an unadjusted model and then added potential covariates one at a time until we achieved the lowest QICC value. The most parsimonious models for each outcome included controlling for marital status, income, and ethnicity. Therefore, we chose to control for these 3 variables in each of our final adjusted models.
This study was approved by the University of Rochester Medical Center’s institutional review board (IRB) and SJNC received a Federalwide Assurance that requires SJNC to uphold the university’s IRB requirements. All analyses were conducted using IBM SPSS Statistics 24.
Results
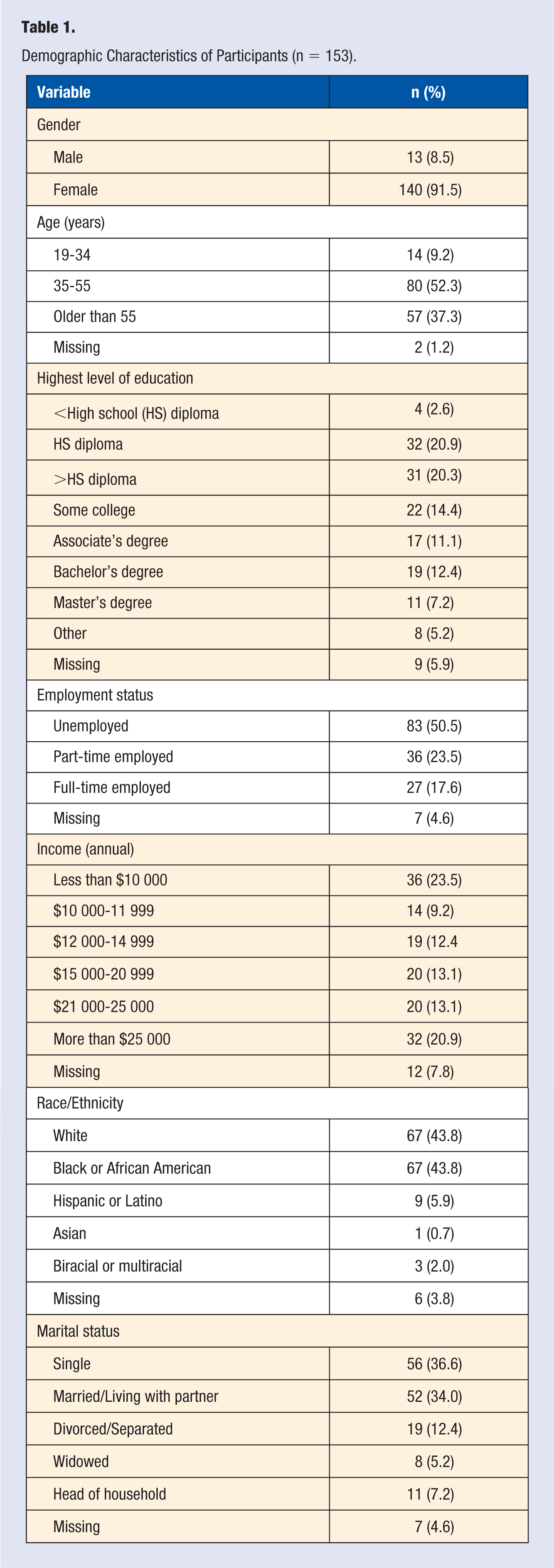
Participants were predominantly female (92%), and the mean age was 51.7 years (SD = 10.9), with more than half of the participants falling in the age range of 35 to 55 years (52.3%). Race was evenly divided between whites (43.8%) and blacks (43.8%), and about a third of the sample were married. More than half of the participants were unemployed (54.2%), and most participants had received at least a high school diploma. Approximately one-quarter of the sample reported annual incomes of less than $10 000. Sample characteristics are found in Table 1.
Demographic Characteristics of Participants (n = 153).
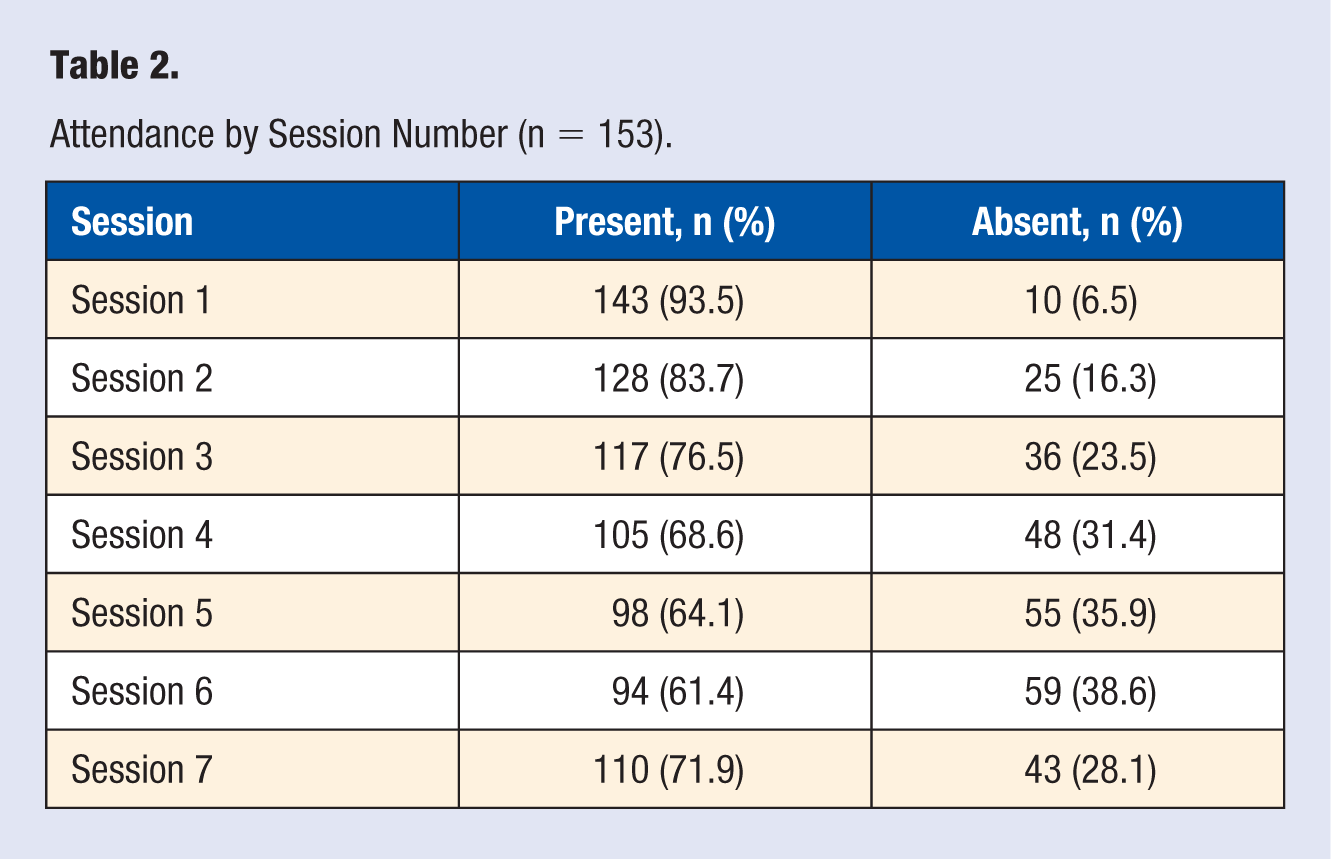
There were no significant differences between individuals who remained in the program compared with those who dropped out, based on gender [χ(1, n = 82) = 1.19, P = .28], age [χ(1, n = 80) = 1.10, P = .29], education level [χ(1, n = 75) = 1.92, P = .17], income level [χ(1, n = 73) = 1.82, P = .18], racial/ethnic identity [χ(1, n = 78) = 1.39, P = .24], or employment status [χ(1, n = 77) = 1.55, P = .21]. Session attendance differed for all 7 sessions but ranged from about 61% to 94% (Table 2). A total of 23 participants also attended drop-in make-up sessions over the course of the 7 weeks (15.0%).
Attendance by Session Number (n = 153).
The amount of exercise participants reported significantly increased from baseline to posttest and 3-month follow-up (β = 3.56; SE = 1.48; P = .016). Fruit and vegetable consumption (β = 0. 78; SE = 0.22; P < .001), fat and cholesterol consumption (β = 0.27; SE = 0.05; P < .001), and overall food quality (β = 0.97; SE = 0.16; P < .001) significantly increased from baseline to posttest and 3-month follow-up, after controlling for marital status, income, and ethnicity. There were no changes in dairy consumption or food security from baseline to posttest and 3-month follow-up. Means and SDs for mental health, intrapersonal variables, and health behaviors and cognition are shown for each time point in Table 3. Parameter estimates are shown in Table 4.
Measures of Central Tendency for Outcomes at Baseline, Posttest, and 3-Month Follow-up.
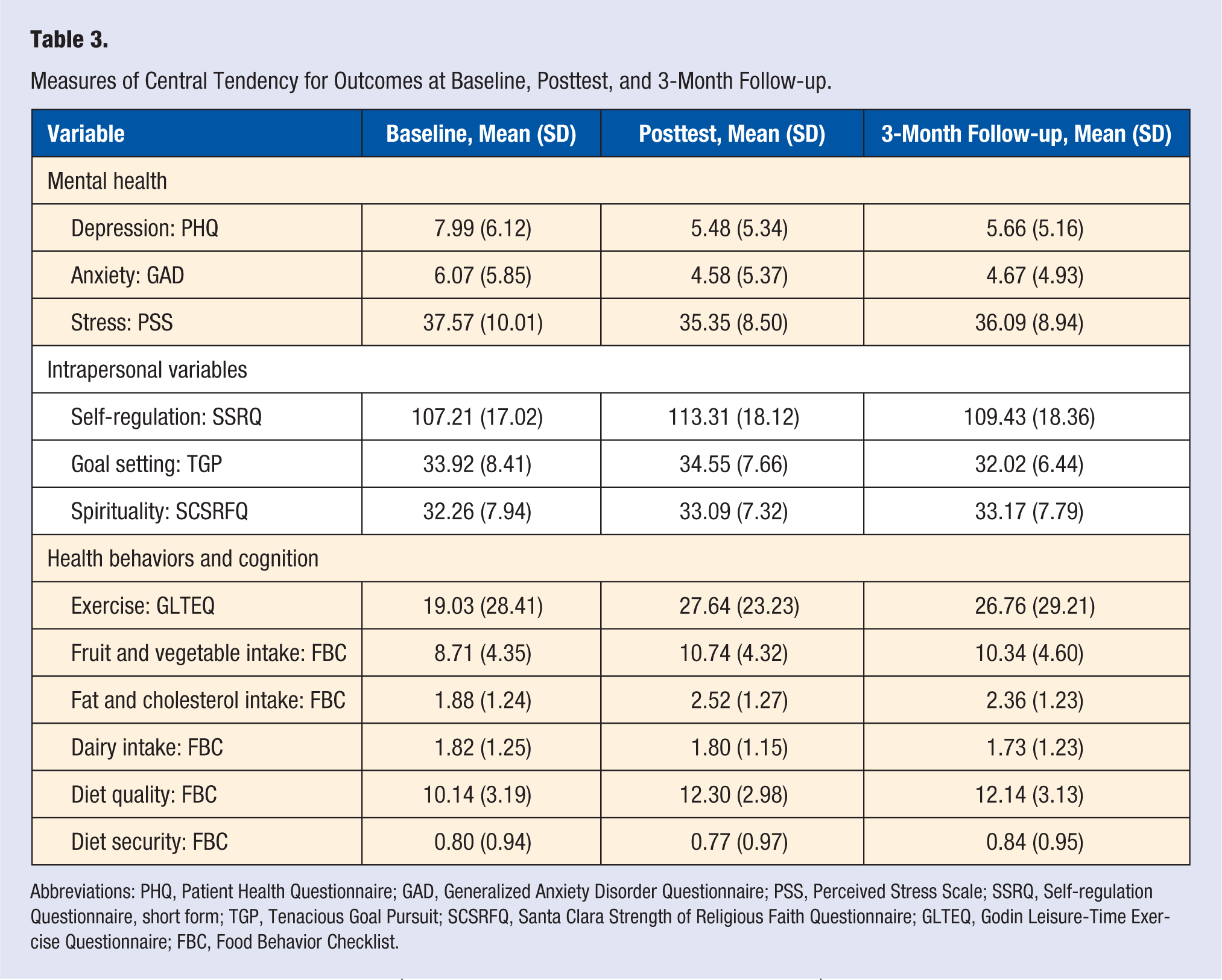
Abbreviations: PHQ, Patient Health Questionnaire; GAD, Generalized Anxiety Disorder Questionnaire; PSS, Perceived Stress Scale; SSRQ, Self-regulation Questionnaire, short form; TGP, Tenacious Goal Pursuit; SCSRFQ, Santa Clara Strength of Religious Faith Questionnaire; GLTEQ, Godin Leisure-Time Exercise Questionnaire; FBC, Food Behavior Checklist.
Changes in Outcomes From Baseline to Posttest to 3-Month Follow-up, From Generalized Estimating Equation Results. a .
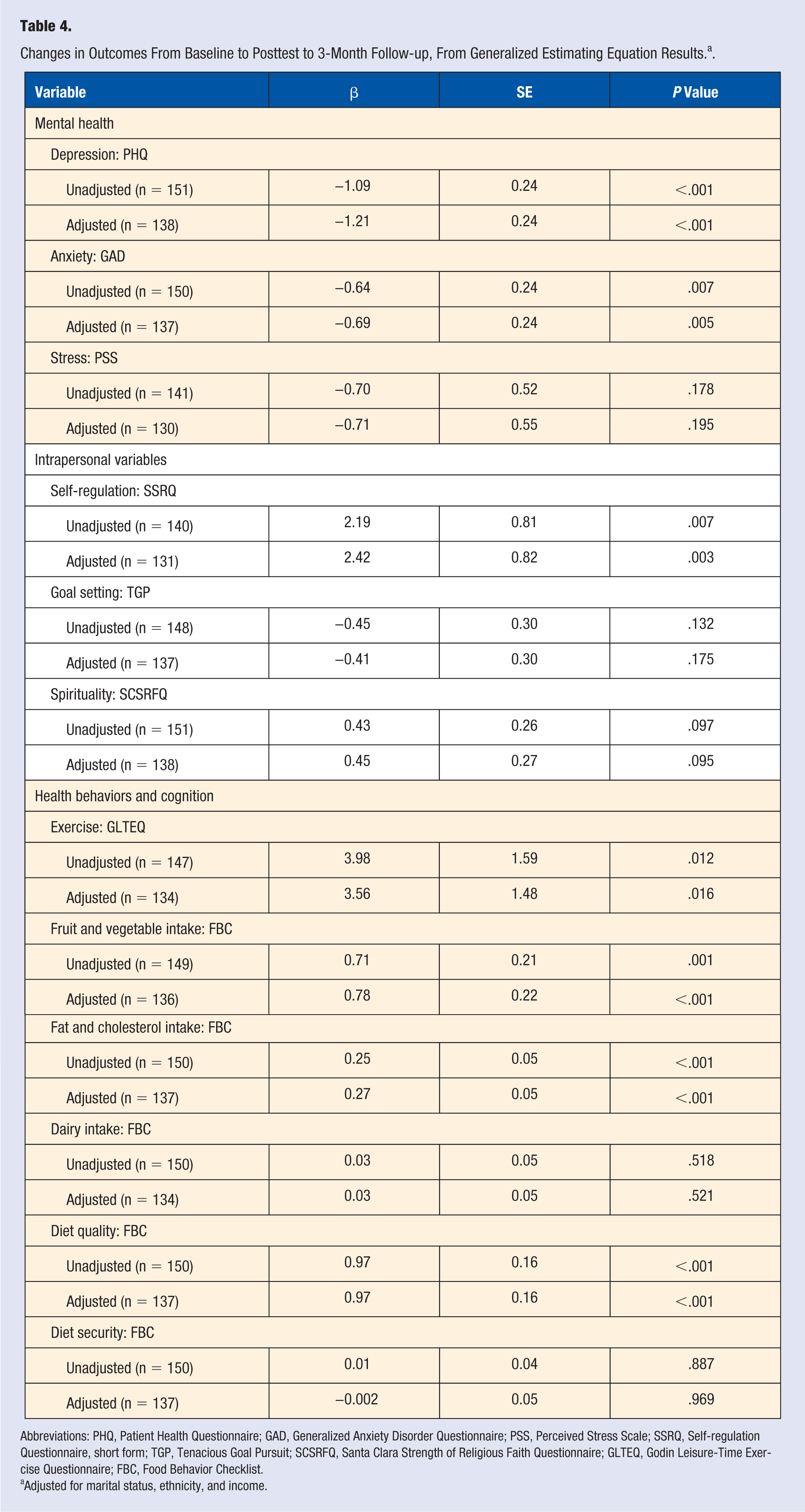
Abbreviations: PHQ, Patient Health Questionnaire; GAD, Generalized Anxiety Disorder Questionnaire; PSS, Perceived Stress Scale; SSRQ, Self-regulation Questionnaire, short form; TGP, Tenacious Goal Pursuit; SCSRFQ, Santa Clara Strength of Religious Faith Questionnaire; GLTEQ, Godin Leisure-Time Exercise Questionnaire; FBC, Food Behavior Checklist.
Adjusted for marital status, ethnicity, and income.
Depressive symptoms (β = −1.21; SE = 0.24; P < .001) and anxiety symptoms (β = −0.69; SE = 0.24; P = .005) decreased significantly from baseline to posttest and 3-month follow-up, after controlling for marital status, income, and ethnicity. There were no changes in perceived stress scores over time. Participants’ self-regulation increased significantly over time (β = 2.42; SE = 0.82; P = .003) after adjusting for marital status, income, and ethnicity. There were no changes in spirituality or goal setting from baseline to posttest and 3-month follow-up.
Discussion
The purpose of this study was to test whether including spirituality components into a health promotion program is feasible and leads to measurable change in health behaviors and indicators of psychological well-being. The HEP—a health promotion curriculum for people with low income who are concerned about their weight—was developed collaboratively by university researchers and health care professionals in a faith-based clinic, with input from clinic patients. Unique aspects of the program include that it directly uses spirituality as a tool to strengthen healthy behaviors and addresses issues of psychological stress and its relationship to eating behaviors, financial barriers to healthy living, and affordable strategies for weight loss maintenance. Program leaders were attentive to the stated needs of clinic patients and mindful of findings that low-income and ethnic minority clients often use spirituality as a means of coping. 42
We evaluated the program using longitudinal analyses for each outcome. Although the original intent of the program was to help participants make lifestyle changes with regard to health behaviors, change in mental health and intrapersonal variables were evident as well both at posttest and during the 3-month follow-up period of the study. Specifically, self-reported levels of depression and anxiety decreased significantly over time. The amount of exercise reported by participants, as well as fruit and vegetable consumption and overall food quality, significantly increased over time. In the current sample, physical activity was increased from moderately active (14-23 units) to active (>24 units), as interpreted by the Godin Scale Score. 43 Although these measures do not translate into whether the participants were meeting current physical activity recommendations, any increase in physical activity is an advantage. In light of current nutritional guidelines, the increases reported in fruit and vegetable consumption are also positive. Our findings are consistent with those of Jordan et al, 2 who showed that participants in their health promotion program had improvements in eating habits such as increased fruit and vegetable consumption. Congruent with the Faith on the Move program and the WORD program, the HEP results also found increased physical activity.44,45
Fat and cholesterol also significantly increased; however, the effect was small, and given that overall food quality increased as well, perhaps the types of fat and cholesterol being consumed were healthier. A detailed food diary would have allowed a more thorough examination of the types of foods being consumed. Self-regulation increased significantly over time. We found no changes over time in perceived stress, dairy consumption, food security, spirituality, or goal-oriented cognitions.
Davis et al 5 used qualitative methods to understand the weight loss experiences of women, and among the emerging themes were the need for weight loss programs to include not only psychological and spiritual components, but also to address the social and cultural concerns related to weight loss while considering the cost of weight loss programs. The HEP used the biopsychosocial-spiritual approach; therefore, a number of these concerns were included as elements of the program (ie, getting through the holidays and changing one’s lifestyle on a budget). As results included improvements in mental health symptoms, our findings suggest that some of these barriers were indeed addressed.
A surprising finding was that despite changes in self-regulation, there were no changes in the levels of goal pursuit or spirituality. Ceiling effects for the spirituality measure suggested that a number of individuals were already at the top of the range of spiritual orientation when beginning the program. The result for goal pursuit is more puzzling. It is possible that in setting and pursuing specific goals, the participants became more aware that their goals needed to be more realistic and responsive to the multiple barriers that may arise, thus limiting the intensity of their goal pursuit over time. 46
In addition to promoting lifestyle changes, another aim of the HEP was to maintain these changes in behavior. Focus groups have examined the weight loss strategies of African American women and found that changes in eating habits, portion control, and food preparation techniques were all successful strategies for sustaining weight loss. 47 In developing the HEP, we used similar strategies (ie, cooking class and portion control) to help prepare participants to maintain their lifestyle changes. Furthermore, the follow-up results suggest that the participants who completed the HEP were slowly changing and sustaining their new lifestyles. Specifically, improvements in mental health (eg, depression and anxiety) as well as some health behaviors (ie, eating more fruits and vegetables, improved nutritional quality of their diet) were maintained at follow-up. It was interesting to note that the range in depressive symptoms continued to fall from baseline (PHQ range 0-27), posttest (PHQ range 0-25), and 3-month follow-up (PHQ range 0-21). In terms of thresholds for determining the severity of depressive symptoms, a score of 5 or below on the PHQ indicates mild depressive symptoms and a score of between 5 and 10 indicates moderate depressive symptoms. 35 Although the mean of all 3 time points for depressive symptoms fell in the moderate depressive symptoms category, posttest and 3-month follow-up were both only slightly above the 5 cut-point. Additionally, from baseline to posttest to 3-month follow-up, the number of participants who were scoring above a 20 (severe depressive symptoms) decreased from 13 (8.5%), to 5 (3.3%), to 2 (1.3%), respectively. There were no changes in the range of anxiety symptoms over time (0-21 at all 3 time points). Cutoff points for the GAD score include 5, 10, and 15 for mild anxiety symptoms, moderate anxiety symptoms, and severe anxiety symptoms, respectively. 27 Based on mean scores for the GAD, participants’ mean score indicated moderate anxiety symptoms at baseline, with mild anxiety symptoms at both posttest and 3-month follow-up. Additionally, from baseline to posttest to 3-month follow-up, the number of participants scoring above a 15 (severe anxiety symptoms) decreased from 26 (17.0%), to 10 (6.5%), to 8 (5.2%), respectively.
We were concerned that locating the intervention in a neighborhood center associated with a specific religion may result in selection bias of one religion or spirituality over another. However, many of our participants were not of the same religious denomination as the clinic’s sponsors. Therefore, we believe that our sample was an unbiased representation of the target population—low-income adults of various faith backgrounds residing in the SJNC’s neighborhood. Future studies should test the HEP in various locations to determine if participants are engaged differently in the faith and spiritual aspects of the program depending on the type of clinic.
A limitation of the current study includes the lack of a control group. We were interested in determining whether we could change health behaviors and cognition in this real-world, high-need setting in which randomization was neither feasible nor ethical. Without a randomized controlled trial, we cannot conclude unequivocally that the content of the HEP intervention, rather than additional factors (eg, increased attention, regular weight checks, or group support), was responsible for changes in participant health behaviors. However, it is unlikely that individuals would experience improved mental health, make lifestyle changes, and maintain that change at follow-up completely independent of the content they were provided.
Additionally, various members of the research team were involved in providing the lifestyle sessions, and therefore, there could have been a reduction in fidelity to the program. However, extensive training and a detailed program manual was provided for each leader to reduce variation in delivery. Fidelity was not measured directly, although team meetings were used to debrief from sessions and potential issues were addressed.
Finally, selection bias may have been a problem in the current study based on 2 factors: (1) exclusion of non–English speaking individuals and (2) the majority of participants being women. In regard to excluding non–English speaking individuals in the HEP program, there is a chance for limited external validity. The population around SJNC is a mixed population, with a moderate prevalence of Spanish speakers. However, there is no reason to believe that language delivery would have altered program outcomes. In regard to the high proportion of women in our study, men were either hesitant to sign up or dropped out of the intervention early. Studies are needed to determine whether specific program adjustments would be more effective for recruiting and retaining men in lifestyle change programs and to explore any potential gender differences in outcomes.
A strength of this study is that we were able to recruit, serve, and follow up with hard-to-reach uninsured and underinsured individuals with low incomes. This is in part a result of the mission of SJNC and its openness to programming innovation as well as research. Although the SJNC is a neighborhood health center run by a faith-based organization, it is not a center of worship and is staffed by volunteers of many creeds, and patients are not routinely exposed to religious or spiritual content. The HEP program’s focus on encouraging the use of each individual’s spirituality as a source of strength and assistance from a nondenominational perspective played an important role in the positive reception of the spiritual component by participants. Based on the experience of delivering the HEP in this neighborhood setting, we suggest that future research uses a waitlist-design. Using a waitlist design would allow everyone who is interested in participating a chance to eventually enroll in the program. The drawback from this type of design is that when looking at motivation for behavior change, people are ready when they are ready, and missing that window of opportunity may result in dropouts once enrolled in the program. Although using a control group is not ethical in lifestyle change programs, we propose a control condition that would offer individual sessions of nutrition and exercise consulting (as compared with a group setting of HEP), with no discussion/inclusion of spirituality. A limitation may be that some individuals thrive in one-on-one sessions more than group settings, therefore, possibly reducing the effect size of the intervention. Additional recommendations include group sessions both with and without spirituality as well as one-on-one sessions (with and without spirituality). We also recommend that incentives should be given for every assessment and possible for each class session attended. Future research may also explore the effectiveness of the individual HEP components and potential enhancements. For example, participants noted that being accountable to the group was helpful in making changes. They also suggested that ongoing drop-in group sessions may help them maintain their positive health outcomes. Finally, given the excess burden of obesity and related medical complications about African Americans and other minority groups, future researchers may wish to study the effects of HEP versus traditional healthy lifestyle programs in minority groups. Although the current study had a moderate proportion of African American participants, the power to detect a difference using GEE models is lacking. Additionally, the main focus of this intervention was addressing lifestyle changes in low economic communities and not specifically targeting racial differences.
The HEP was developed to promote lifestyle changes (ie, healthy eating and physical activity); encourage biological, psychological, social and spiritual health and well-being; and provide strategies for managing barriers to weight loss (ie, economic, social, and emotional concerns). This program used a nondenominational spiritual focus as a source of support as well as a way to help participants identify goals. The positive changes toward healthful eating and behaviors speak to the notion that a biopsychosocial-spiritual approach may be particularly empowering for participants to take steps toward engaging in healthier behaviors, including increased fruit and vegetable consumption, and decreasing levels of depression. In addition, because our research process and program implementation were successfully guided by community input, we believe that such an approach can make programs more acceptable at local levels. Using a CBPR framework allowed common goals from both researchers and community workers to be congruent and created a synergistic environment. The health of the community can be improved through these types of partnerships, and it is imperative that researchers continue to find ways to work with the community they serve.
Footnotes
Acknowledgements
Special thanks to the directors, administrators, and mentors on the Rochester Program of Research and Innovation in Disparities Education Grant (R25MH074898, Duberstein, PI), including Paul Duberstein, Kathryn Castle, Deborah King, and Ellen Poleshuck, and to the administrative staff at St Joseph’s Neighborhood Center, including Sister Christine Wagner.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: St Joseph’s Neighborhood Center received a grant from Excellus Blue Cross and Blue Shield and from the Program of Research and Innovation in Disparities Education (PRIDE) funded by the National Institute of Mental Health (R25MH074898). This work was also supported by a National Research Service Award from the National Institute of Health (2T32MH020061). The authors have no conflicts of interest to report.