
Abstract
Background:
Despite safety mandates and interventions, sharps injuries remain an occupational risk for registered nurses (RNs). Sharps and needlestick injuries increase the risk of exposure to blood-borne pathogens. Post-exposure direct and indirect costs of these percutaneous injuries have been estimated at about US$700 per incident. The goal of this quality improvement project was to identify root causes of sharps injuries for RNs at a large urban hospital system.
Methods:
A retrospective evaluation of sharps injuries sustained by RNs, identification epsication of themes or root causes, and the development of a fishbone diagram to sort the causes into categories to identify workable solutions were conducted. Fisher’s exact tests were performed to identify association between variables and root causes.
Findings:
A total of 47 sharps injuries were reported from January 2020 through June 2020. Among sharps injuries sustained by nurses, 68.1% were among nurses 19 to 25 years of age and 57.4% reported job tenure of 1 to 2 years. There was a statistically significant association between root causes and tenure range, gender, and procedure type (p < .05) with moderate effect size (Cramer’s V = 0.35-0.60). Technique also was a primary cause of sharps injuries for blood draw (77%), discontinuing line (75%), injection (46%), intravenous (IV) start (100%), and suturing (50%).
Conclusions/Applications to Practice:
Technique and patient behavior were primary root causes of sharps injuries in this study. More sharps injuries caused by technique occurred among nurses with job tenure of 1 to 10 years, female, blood draw, discontinuing line, injection, IV start, and suturing procedures. The root cause analysis identified tenure, technique, and behavior as potential root causes of sharps injuries specifically occurring most during blood draw and injections at a large urban hospital system. These findings will inform nurses, especially new nurses in the proper use of safety devices and behaviors to prevent injury.
Background
Despite safety mandates and interventions, sharps injuries, including needlesticks, remain an occupational risk for RNs. Needlestick injuries rank highest among healthcare staff compared with other sharps injuries, such as those associated with the use of suture needles and scalpels (Kahriman et al., 2016). In the United States, there are still 300,000 documented sharps injuries annually among hospital workers (Reddy et al., 2017) of which 34% are sustained by RNs (International Safety Center: EPInet, 2018). Both needlestick and sharps injuries are considered percutaneous exposure incidents and increase the risk of exposure to blood-borne pathogens, specifically hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) (Mannocci et al., 2016). As far back as 2007, Leigh and colleagues estimated 645,000 needlestick injuries in the healthcare industry in a year, which resulted in 34 people developing HBV, 143 with chronic HCV, and one with HIV. Incidence rate of HIV after needlestick exposure is 0.3%, HBV is 0.8%, and HCV is 1.6% with a decreased HBV incidence rate due to hepatitis B vaccination (King & Strony, n.d.). The post-exposure direct and indirect costs of these percutaneous injuries have been estimated at about US$700 per incident (Mannocci et al., 2016).
Risk factors for sharps injuries include the type of procedure, availability of personal protective equipment (PPE), training on PPE and infection control, fatigue, amount of work, and location of the procedure (Reddy et al., 2017). A global response to needlestick and sharps injuries was the development and implementation of safe medical devices that either remove the needle or surround the needles, such as needleless intravenous access devices, safety needles, and so on (Reddy et al., 2017). In a recent study, there was inconclusive evidence to support reduction of needlestick injuries with safety systems in place; however, there were more blood splashes associated with the use of these systems (Reddy et al., 2017). In another study, combining safety devices with training was statistically significant in reducing needlestick injuries (de Jager et al., 2018). Healthcare workers who received training on prevention of infection showed a significant decrease in sharps injuries, compared with those who did not receive the training (Belachew et al., 2017). In addition, the level of nurse experience has shown to directly impact the number of sharps injuries experienced (Singh et al., 2017). Many times, the needlestick occurs before workers engage the safety device (Chambers et al., 2015). Many healthcare workers report that patient behavior, disposal methods, and the way the safety device engages are risks for further needlesticks (Chambers et al., 2015). While not a risk factor for injury, there is an elevated level of underreporting of sharps injuries, which implicates a lack of education about the importance and necessity of reporting these types of injuries (Boden et al., 2015). Boden et al. (2015) reported that workers were hesitant to report work related injuries due to concern of losing their job, potential pressure from coworkers, difficulty of the workers compensation system, and potential negative impact on site safety record.
Factors related to injuries in the workplace can be multifactorial, including behavior, training, policies, culture, type of work, and hazards present (Batty et al., 2003). A useful tool to evaluate sharps injuries is a root cause analysis, which allows for a full methodical evaluation of all potential causes of sharps injuries (Batty et al., 2003). Recommended processes for root cause analysis are human factor analysis, casual chain diagram or a fishbone diagram (Batty et al., 2003). The casual chain or fishbone diagram allows you to drill down to all the potential causes of the incidents including those requiring immediate attention (Batty et al., 2003).
At a large urban hospital system, 42% of the sharps injuries were sustained by RNs—which is greater than the national average of 34% (International Safety Center: EPInet, 2018). Sharps injuries increase risk of blood-borne pathogen exposure, increase financial burden for the hospital, and posed potential lifelong problems for RNs (Mannocci et al., 2016). The purpose of this quality improvement (QI) project was to identify the causes of injuries through a root cause analysis with the long-term goal of reducing sharps injuries among RNs at a large urban hospital system.
Methods
This QI project was a retrospective evaluation of sharps injuries sustained by RNs, identification of themes or root causes, and the development of a fishbone diagram to sort the causes into categories to identify workable solutions. The setting for the project was a 1,100-bed urban hospital system, and the population were RNs who sustained sharps injuries over a period of 6 months from January 2020 through June 2020. The Employee Health Department provided de-identified data regarding sharps injuries specific to RNs.
Data were recoded to include patient number, date seen, age, sex, nurse tenure, sharp type, discipline, work location (where injury occurred), associated procedure, labs obtained, prophylaxis, and event description. Age and tenure were recoded into ranges. Age ranges were in 5-year increments from 19 to 25, 26 to 30, 31 to 35, 36 to 40, 41 to 45, and over 45. The tenure ranges were divided into 1 to 2, 3 to 5, 6 to 10, and 11 to 15 years. The specific findings for event description were also sorted into themes of environment, technique, material/device, people, and waste/cleaning (Figure 1). Environmental causes included a needle being dislodged or being on a bed or pillowcase, and technique causes included sharp injuries during intravenous (IV) starts, injections and transferring blood. Material/device root causes were describing injuries while RNs were engaging the safety device, not realizing that the safety was not on and while loading a suture into a device. People cause included being stuck by a surgeon, suture injury while retracting, and when a patient moved during blood draw. Finally, waste/cleaning category described causes, such as cleaning up after surgery, after an IV start or disposing sharps. The Employee Health Department Manager also provided the date when the first COVID-19 patient was admitted into the hospital. This allowed us to indicate if the sharps injuries occurring before or after the first COVID patient.
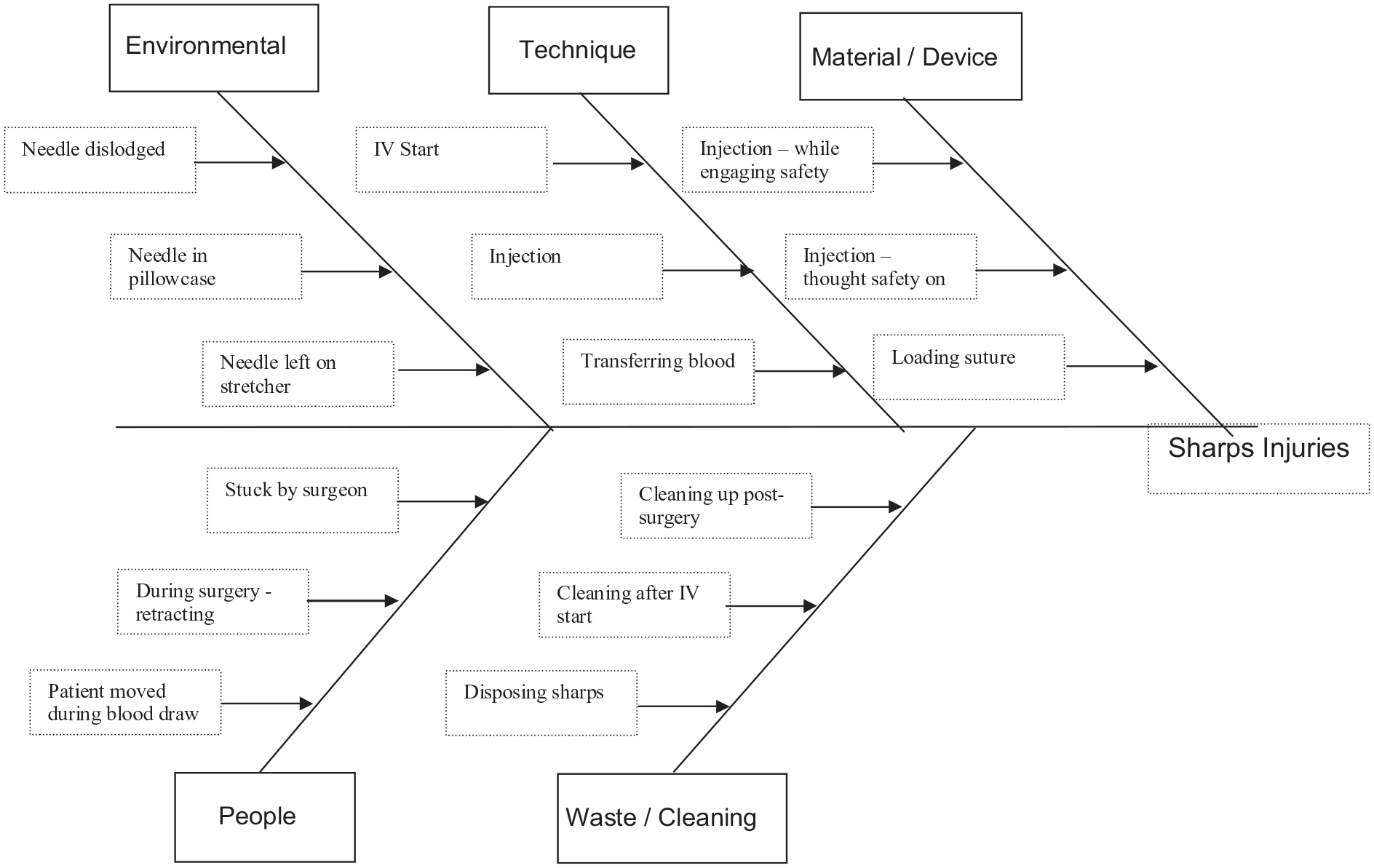
Fishbone Diagram.
The University of Alabama (UAB) Institutional Review Board, after consultation with DNP leadership, determined this project to be a QI project and not subject to Institutional Review Board’s (IRB) Review.
Descriptive statistics for the demographic variables were tabulated to characterize the sample. For continuous variables, average, standard deviation (SD), and median were reported, whereas frequency and percentages were reported for categorical variables. Because the small observed frequency in cells (< 5) were presented in contingency tables, Fisher’s exact tests were performed to identify associations between variables (e.g., age range, tenure range, gender, work location, before and after COVID-19, sharp type, and procedure type) and root causes. Effect sizes (Cramer’s V) were also performed for all tests. All analyses were performed using SPSS version 27 (IBM Corp., 2020) and SAS version 9.4 (SAS Institute Inc., 2013).
Results
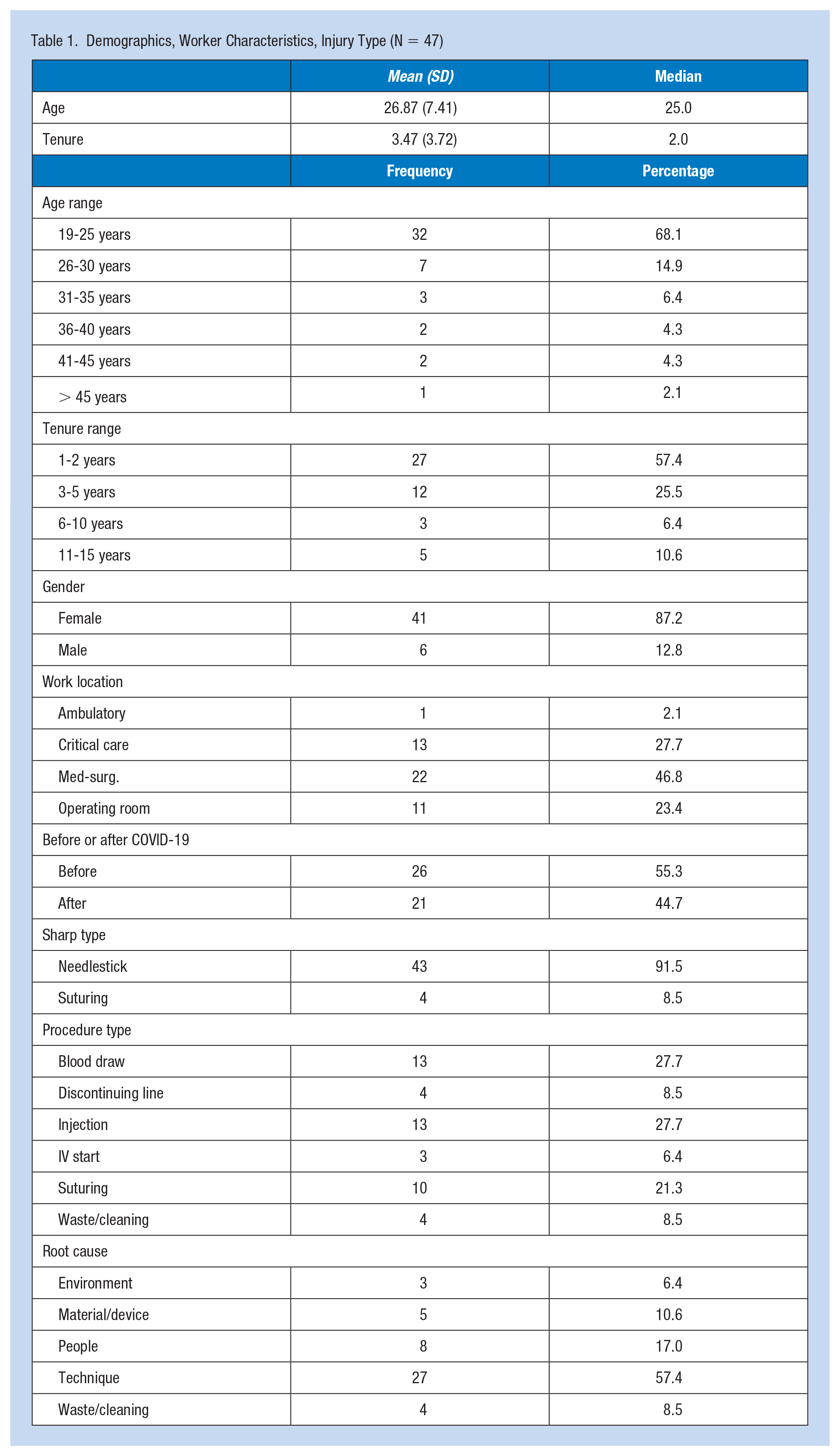
In total, 47 RNs sustained sharps injuries between January 2020 and May 2020. The root causes were documented on a fishbone diagram in Figure 1 and all test results were reported in Tables 1 and 2. Most of the injured RNs were females between the ages of 19 and 25, and 82.9% of RNs had been employed in the facility 5 years or less. Ninety-two percent of sharps injuries were needlestick injuries. Most sharps injuries occurred in the medical/surgical areas and critical care. Many sharps injuries were noted to have occurred while RNs were drawing blood and giving an injection. Documentation of the event description by the employee health department was sorted into five groups: technique, people issues, including patient behavior, material/device problems or failures, wasting needles or cleaning, and environmental causes.
Demographics, Worker Characteristics, Injury Type (N = 47)
Frequency by Root Cause and the Relationship Between Root Cause and Other Factors
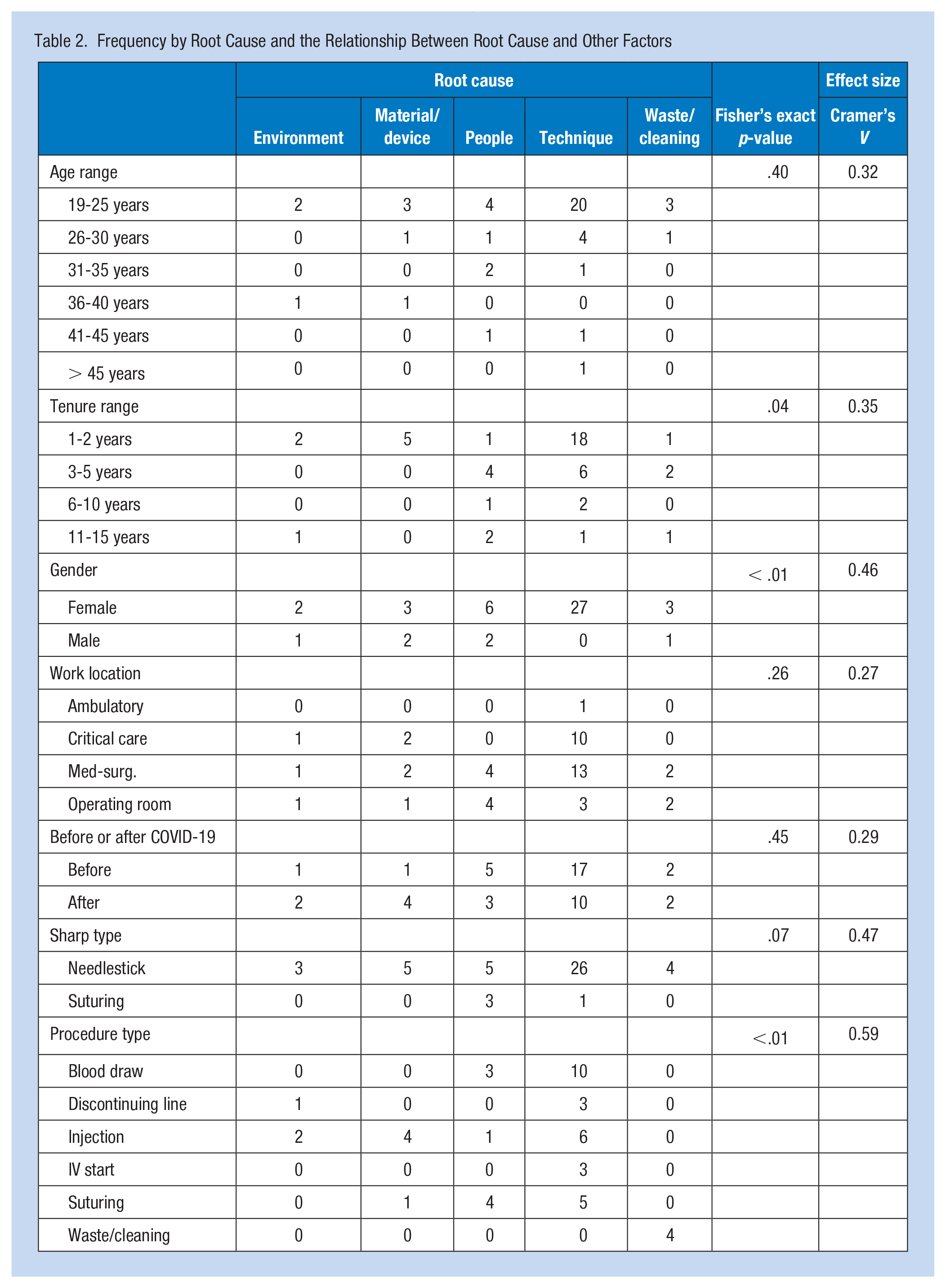
There were no associations between the distributions of root causes and age range, work location, before and after COVID admission, and sharp type (p > .05) with small effect size (Cramer’s V = .279-.474). However, there were statistically significant associations between root causes and tenure range, gender, and procedure type (p < .05) with moderate effect size (Cramer’s V = .351-.596). For tenure range, technique was a main cause of sharps injuries for nurses who had nursing experience for 1 to 2 years, 3 to 5 years, and 6 to 10 years (67%, 50%, and 67%, respectively) while those with 11 to 15 years of nursing experience, people experienced surgeon suture injury while retracting, and when a patient moved during blood draw was a reason. Technique was also a primary cause of sharps injuries in female nurses while material/device and people were causes for male nurses. Furthermore, technique was a primary cause of sharps injuries for blood draw, discontinuing line, injection, IV start, and suturing. However, waste/cleaning was a cause of sharps injuries for waste/cleaning procedures, including cleaning up post-surgery, after IV starts, and when disposing sharps.
Discussion
This QI project aimed to identify the causes of injuries through a root cause analysis with the long-term goal of reducing sharps injuries among RNs at a large urban hospital system. In this study, the root causes of sharps injuries were found to be technique, people, material/device problems or failures, disposing of sharps or cleaning, and environmental causes. Tenure, gender, and type of procedure were found to have a strong association with these root causes. Demographic results indicated that the majority of sharps injuries were sustained by female RNs with short work tenure at the facility. The association of female gender with more frequent sharps injuries is not surprising given that data from only six males were included in the analyses. However, this finding is consistent with other studies by Kahriman et al. (2016) and Matsubara et al. (2017) that show greater likelihood of females being injured by sharps. Findings from this study were not consistent with some of the studies conducted outside the United States. That is, our study indicated a higher prevalence of sharps injuries in registered nurses (RNs) ages 19 to 25, compared with prevalence rates in older groups of RNs. Singh et al. (2017) suggested that the age group with the highest prevalence for sharps injuries was the 20- to 30-year-old age group. However, according to Kahriman et al. (2016), the largest numbers of sharps injuries occurred in those over age 30. Belachew et al. (2017) noted high numbers of sharps injuries in those with tenure of less than 5 years. Separating the 5 years into two groups in this study further suggested the importance of tenure because nurses with 1 to 2 years of tenure had the highest numbers of sharps injuries. The results indicated that most sharps injuries for these RNs involved needlesticks, occurring mostly in the medical /surgical area or at the bedside, which is consistent with studies by Ersin et al. (2016) and Cui et al. (2018). Activities or procedures associated with a high number of sharps injuries by nurses in this study were drawing blood and giving an injection. Belachew et al. (2017) also noted injections and blood draws as being high-risk procedures for nurses related to sharps injuries. This study identified root causes that were presented on a fishbone diagram according to categories. However, these categories should be investigated further to gain insight on potential solutions to prevent sharps injuries and to inform other QI projects.
Although we believe this project yielded important information about sharps injuries among a group of RNs, we do acknowledge limitations in the work. First, the scope of the project was limited to include only RNs. Had it been feasible for us to include all nursing personnel who provide direct care, it may have enabled us to make comparisons across groups and to determine any unique mechanisms of injury or other characteristics that would inform the design of future prevention interventions. This study also included a small sample size, limiting our ability to make generalizations from the findings. Another limitation is that data were not collected on procedures conducted involving sharps without sharps injures. Therefore, it is difficult to know the actual magnitude of the injuries we were able to capture. Because the study took place at the beginning of the COVID-19 pandemic, when elective surgeries, and hospitalizations were limited, the data collection environment may not have reflected the normal operational environment of the facility. It is also possible that there might have been changes in RN and others’ behaviors or practices because of the altered work environment and demands associated with the pandemic.
Implications for Occupational Health Nursing Practice
The root cause analysis revealed some specific areas to focus improvement, including tenure and technique as potential causes of sharps injuries occurring most during blood draw and injections at a large urban health system. These findings should be used by occupational health nurses to inform the education of RNs, especially new RNs, in the proper use of safety devices and other techniques, as well as safety behaviors to prevent injury to themselves or others. Some interventions that may prove to be successful would include longer orientation times for new graduates, which include education about preventing sharps injuries, more frequent sharps injury prevention education for the current staff, and hospital-wide campaigns promoting sharps injuries safety.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tuition support from Deep South Center for Occupational Health and Safety ERC (Grant No. T42OH008436). Dr. Hammond and Dr. Heaton receive salary support from the NIOSH grant.
Ethical Approval
The UAB Institutional Review Board, after consultation with DNP leadership, determined this project to be QI only and not subject to IRB Review.