
Abstract
Background
Occurrence and underreporting of needlesticks and other sharps injuries (NSIs) are still immediate concerns among nursing students. This study examined the relationship between occupational health and safety (OHS) awareness and empowerment levels of nursing students and the occurrence and reporting of NSIs.
Methods
This cross-sectional study was conducted among purposively selected 840 students in a nursing school in 2018–2019. A self-report questionnaire was used to collect data about students’ sociodemographic characteristics, OHS awareness and empowerment levels, and NSIs characteristics. After bivariate analyses, multivariate logistic regression was used.
Results
The number of evaluated questionnaires was 469, for a response rate of 55.8%. Participants, 21.2% (n = 99), had suffered NSIs, and 47.8% had reported their injuries. The NSIs were statistically related to age, academic year, working night shift, OHS awareness level of students, and the number of clinical placements completed by students. The odds of experiencing NSIs was 2.3 (95% confidence interval [CI] = [1.0, 5.3]) times higher in male students, 4.3 (95% CI = [2.4, 7.4]) times higher in those beyond the second academic year, and 2.5 (95% CI = [1.4, 4.4]) times higher in those who had received OHS training for a shorter period than the average duration.
Conclusion/Application to practice
The levels of awareness and empowerment were higher in students who received OHS and NSIs prevention training and those who received OHS training for the above-average duration. Increasing awareness and empowerment levels of nursing students through training can reduce the occurrence and the underreporting of NSIs.
Background
Nursing is a practice profession with known occupational health and safety (OHS) risks (European Union [EU], 2011), and registered nurses have high rates of occupational injury and illness (Dressner & Kissinger, 2018). Nursing education focuses on improving students’ skills based on patient care services during clinical placements with theoretical education. Nevertheless, nursing students are also exposed to occupational injuries while performing clinical practices, similar to registered nurses (Graj et al., 2019; Huang et al., 2016; Nabil et al., 2018). Needlesticks and other sharps injuries (NSIs), which are one of the leading causes of occupational injuries in the health care sector (EU, 2011), are also primary safety issues for nursing students because these injuries can cause various blood-borne infections (Bouya et al., 2020). Underreporting of NSIs is another serious issue because reporting is critical for identifying and eliminating deficiencies in OHS measures (Boucaut & Knobben, 2020; Centers for Disease Control and Prevention, 2015; Rezaei et al., 2017).
It is known that avoiding unsafe injection practices such as overuse of injections or needle recapping, using safety-engineered devices such as auto-disabled or retractable needles, complying with safe work and infection control guidelines (Kazi & Bhuiyan, 2018), and using gloves (Handiyani et al., 2018) can reduce NSIs. Also, establishing an internal surveillance system, increasing students’ knowledge and awareness of OHS issues through training, and creating effective communication between students and instructors or staff are interventions recommended for reducing the occurrence and underreporting of NSIs (Handiyani et al., 2018; Kazi & Bhuiyan, 2018).
Despite the implementation of existing interventions to prevent NSIs, recent studies have reported that the occurrence and underreporting of NSIs continue to be primary concerns among nursing students (Bouya et al., 2020; García-Gámez et al., 2019; Mossburg et al., 2019). Moreover, it has been indicated that nursing students are more vulnerable to occupational injuries than health care workers because of their limited experience in the profession and lower knowledge and awareness of OHS issues. In other words, they have a higher OHS vulnerability to injuries (Boucaut & Cusack, 2016; Eyi & Eyi, 2020; Hada et al., 2018; Zhang et al., 2018).
The OHS vulnerability, which refers to a state of susceptibility for exposure to occupational risks (Smith et al., 2015; Yanar et al., 2019), is traditionally identified based on workers’ sociodemographic and working life characteristics such as age, gender, employment status, educational status, occupation, and sector (Belin et al., 2011; International Labour Office, 2017). Unlike this traditional approach, Smith et al. (2015) have stated that four dimensions are associated with OHS vulnerability: (a) the level of workplace hazards faced by the worker, (b) workplace-level policies and protections in place to protect workers, (c) worker OHS awareness, and (d) worker empowerment to participate in injury prevention. At the same time, Smith et al. (2015) have developed a scale named OHS Vulnerability Measure to evaluate these dimensions based on workers’ self-reports.
Smith et al. (2015) have suggested that dimensions of OHS Vulnerability Measure are related to each other but conceptually dissimilar, and independently measuring these dimensions can be used to determine inadequacies and direct the required prevention interventions to reduce the risk of occupational injuries. Also, Kazi and Bhuiyan (2018) have emphasized that no one intervention is sufficient to prevent NSIs, and implementing a combination of the prevention interventions is more effective than a single intervention. In addition to available interventions for preventing NSIs, measuring the OHS vulnerability of nursing students and implementing the required interventions can provide an opportunity to reduce NSIs experienced in nursing practices.
Among the dimensions of OHS vulnerability, both OHS awareness and empowerment are significant because these dimensions can be separately measured and increased by providing training. In general, OHS awareness refers to a worker’s knowledge of OHS issues, and empowerment defines a worker’s ability to participate in OHS practices and capacity to protect themselves from hazards at work (Smith et al., 2015; Yanar et al., 2019). Studies have demonstrated that inadequate OHS awareness and empowerment are independently associated with the increased risk of injuries (Lay et al., 2016, 2017; Yanar et al., 2019). Nonetheless, Konijn et al. (2018) have emphasized the importance of the positive impact of training intervention on OHS awareness and empowerment dimensions.
Providing OHS training is one of the most common interventions to reduce injuries as its positive impact on students’ knowledge, attitudes, beliefs, and behaviors (Motaarefi et al., 2016; Ricci et al., 2016; Robson et al., 2012; Xiong et al., 2017), and the education period is efficient in shaping students’ behaviors toward protecting their health and safety. Furthermore, the European Agency for Occupational Health and Safety has highlighted that integrating OHS training into the curriculum and enhancing students’ knowledge and awareness about OHS issues such as identifying workplace hazards, risk assessment, and principles of prevention measures can promote a prevention culture and reduce injuries in their education term and future working life (European Agency for Safety and Health at Work, 2009). Therefore, considering OHS as one of the principal aspects of clinical placements and enhancing students’ OHS awareness and empowerment during the education period can contribute to protecting their health and safety (Boucaut & Cusack, 2016; Eyi & Eyi, 2020; O’Keeffe et al., 2020).
The present study aimed to assess the relationship between OHS awareness and empowerment levels of nursing students and the occurrence and reporting of NSIs. It also evaluated the impact of OHS and NSIs prevention training on OHS awareness and empowerment levels of nursing students.
Methods
This cross-sectional study was conducted among undergraduate nursing students invited to participate in the study at Hacettepe University Faculty of Nursing, Ankara, Turkey, in the 2018–2019 academic year. The nursing program at Hacettepe University is completed over 5 years, including 1 year of English preparatory education and 4 academic years of general nursing education. Students begin clinical placements from the first academic year and continue until the fourth academic year, and perform their clinical placements in Hacettepe University Hospitals and different health care organizations close to the university.
Purposive convenience sampling was used for this study. All students who had the experience of working in the clinical setting were targeted, and students who had completed or were currently working in at least one clinical placement were included in the study. Preparatory education students were excluded because they have not yet attended clinical placements. The total number of students was obtained from the school administration, and the population of the study consisted of 840 students in the general nurse education program.
Nursing students included in the study population were invited to the study after their regular lectures. The students were informed about voluntary participation, and the written informed consent was obtained prior to participation. No personal identifiers were collected, and confidentiality and privacy were ensured. A paper-based questionnaire survey was used to collect data. The researchers prepared a survey form about students’ sociodemographic characteristics and NSIs characteristics based on the variables. In addition, the OHS Vulnerability Measure developed by Smith et al. (2015) was used for collecting data about OHS awareness and empowerment levels of students. One of the researchers distributed the questionnaire to each student in the classrooms and collected the answered questionnaires after 20 minutes.
The questionnaire consisted of three sections. Students’ sociodemographic characteristics such as gender, age, academic year, and the number of completed clinical placements were in the first section. This section also examined whether students had worked on the night shift and had received OHS training, and how long they received OHS training.
The second section was related to whether students had received NSIs prevention training, they had used gloves during their clinical practices, and health care organizations had supplied personal protective equipment (PPE). It also included questions about frequency, type, and reporting status of NSIs experienced by students. In this study, all types of clean and contaminated NSIs were examined. Items related to OHS awareness and empowerment dimensions of the OHS Vulnerability Measure were in the third section.
The OHS Vulnerability Measure consists of four sections, namely, hazards (nine items), policies and procedures (seven items), awareness (six items), and empowerment (five items). Each item is measured by the level of agreement with a series of statements such as strongly agree, agree, disagree, strongly disagree, and do not know or not applicable (DK/NA; Smith et al., 2015). In this study, the Turkish version of awareness and empowerment sections was used. Each item of awareness and empowerment was translated into Turkish and adapted for nursing students. Also, each agreement was scored like the 5-point Likert-type scale (4 = strongly agree, 3 = agree, 2 = disagree, 1 = strongly disagrees, 0 = DK/NA). Then, language and content validity and reliability studies were carried out in conformity with standard translation and testing procedures. After the Turkish version had been determined valid and reliable, awareness and empowerment sections were applied.
The awareness section consisted of six items (a total of 24 points) related to the extent to which students are aware of OHS issues such as rights and responsibility of workers and employers, safe working, safety precautions, and procedures for reporting risks. For example, “I know how to perform safely the professional practices expected from me within the education program” or “If I became aware of a health or safety hazard during professional practices, I know who I would report it to.”
The empowerment section included five items (a total of 20 points). Four of them were about students’ ability to participate in OHS practices, voice concerns about OHS issues, ask questions about perceived workplace hazards, and refuse unsafe duties. For instance, “I know that I can stop my professional practice if I think something is unsafe and management will not give me a hard time” or “I feel free to voice my concerns about workplace health and safety or make suggestions in my professional practices.” Also, one item was related to they have enough time to complete their professional practices safely. The points of the students’ answers given to the items were summed, and the total score was calculated for each dimension. High scores have been assessed as adequate OHS awareness and empowerment levels, in other words, low OHS vulnerability.
Data Analysis
Data were analyzed using the IBM SPSS Statistics (Version 23). Numeric variables were presented as means, standard deviations, and ranges (minimum–maximum); categorical variables were presented as frequencies and percentages. Continuous variables were categorized for the bivariate analysis. The academic year was grouped as the second academic year and below and beyond the second academic year. Age, OHS training duration, and awareness and empowerment scores were also grouped as below and above average. Second, the distributions of awareness and empowerment scores were compared by selected descriptive characteristic groups of students. According to the Kolmogorov–Smirnov test, which confirmed the normality of data distribution, parametric conditions were not provided in intergroup comparisons. The Mann–Whitney U test was used to compare bivariate independent groups.
The differences in frequency and reporting status of NSIs by selected descriptive characteristic groups were tested. Cross-tabulation analysis (chi-square tests) was used to examine the distributions of differences between categorical variables. Finally, after analyzing the differences between groups, the binary logistic regression model was applied using the backward method. Odds ratios (ORs) and 95% confidence intervals (CIs) were presented.
Ethical approval was obtained from the Hacettepe University Non-Interventional Clinical Research Ethics Committee (Decision No: GO 18/768-23, Date of Decision: September 11, 2018). Also, institutional permission was received from Hacettepe University Faculty of Nursing.
Results
Of the 840 nursing students invited, 469 (55%) completed the questionnaire (Table 1). Of those, 99.1% were single, 90.2% were female, and the average age was 21.6 ± 1.5 (18–30) years. Less than half (33.7%) were in their third academic year, 32.0% worked night shift, and the average number of clinical placements was 3.9 ± 2.4 (1–8). Almost all of the students (98.7%) had received OHS training, and 70.1% had received NSIs prevention training. Although 95.0% of the students stated that PPE had been supplied, only 54.4% had used gloves in their clinical practices.
The Descriptive Characteristics of Nursing Students (N = 469)
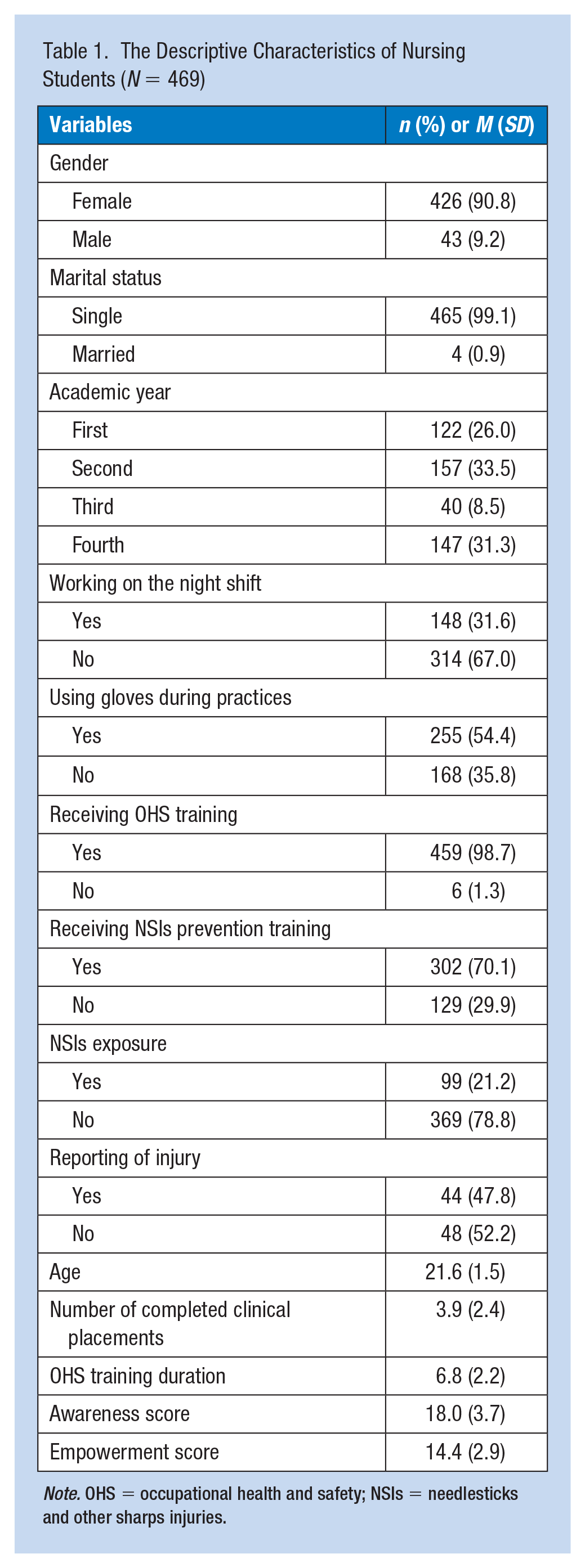
Note. OHS = occupational health and safety; NSIs = needlesticks and other sharps injuries.
Compared with students in the second academic year and below, those beyond the second academic years had more frequently received OHS training (98.6% and 99.5%, respectively) but less frequently NSIs prevention training (73.3% and 65.7%, respectively). High proportions of female and male students received OHS (99.1% and 95.2%, respectively), with differences in NSIs prevention training (71.2% and 57.9%, respectively). The average duration of OHS training provided for students was 6.8 ± 2.2 (1–16) hours.
Average scores for awareness and empowerment were 18.0 ± 3.7 (6–24) and 14.4 ± 2.9 (6–20) points, respectively (Table 2). Both awareness and empowerment average scores were lower in students beyond the second academic year (17.0 ± 3.5 and 14.0 ± 2.8) than those in the lower academic years (18.5 ± 3.7 and 14.5 ± 2.9). These levels were also lower in older students, those who had not received OHS or NSIs prevention training, and those who received OHS training for the below-average duration.
The Distribution of Awareness and Empowerment Scores by Descriptive Characteristic Groups of Nursing Students (N = 469)
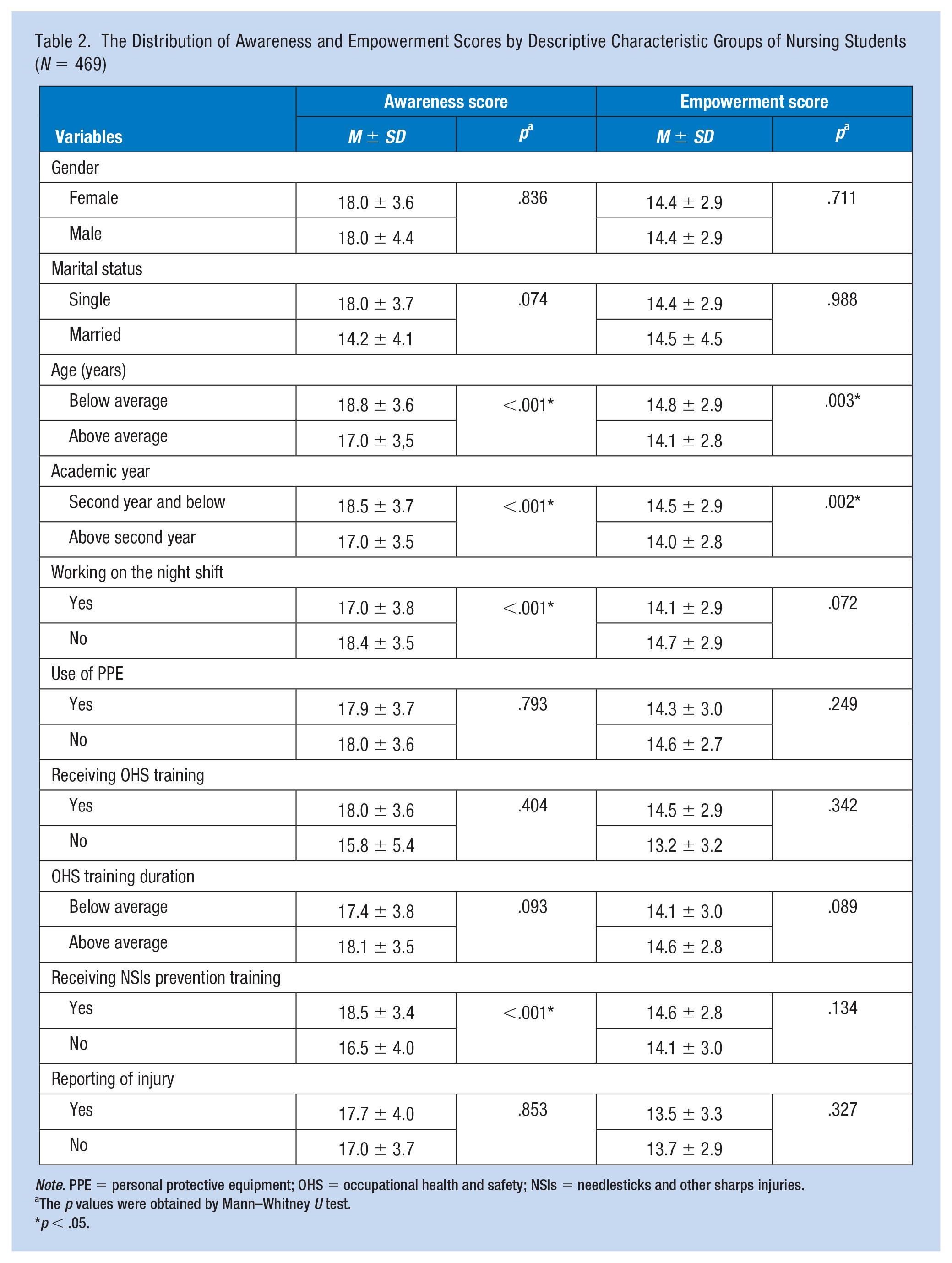
Note. PPE = personal protective equipment; OHS = occupational health and safety; NSIs = needlesticks and other sharps injuries.
The p values were obtained by Mann–Whitney U test.
p < .05.
Twenty-one percent of participants experienced at least one sharps injury and 47.8% reported their injuries (Table 3). The frequency of NSIs was statistically significantly higher in students who have been older than the average age (30.6%), have been in above the second academic year (33.7%), had completed four or more clinical placements (33.5%), had worked on the night shift (39.7%), and had awareness scores for below average (26.6%).
The Distribution of Frequency and Reporting Status of NSIs by Descriptive Characteristic Groups of Nursing Students (N = 469)
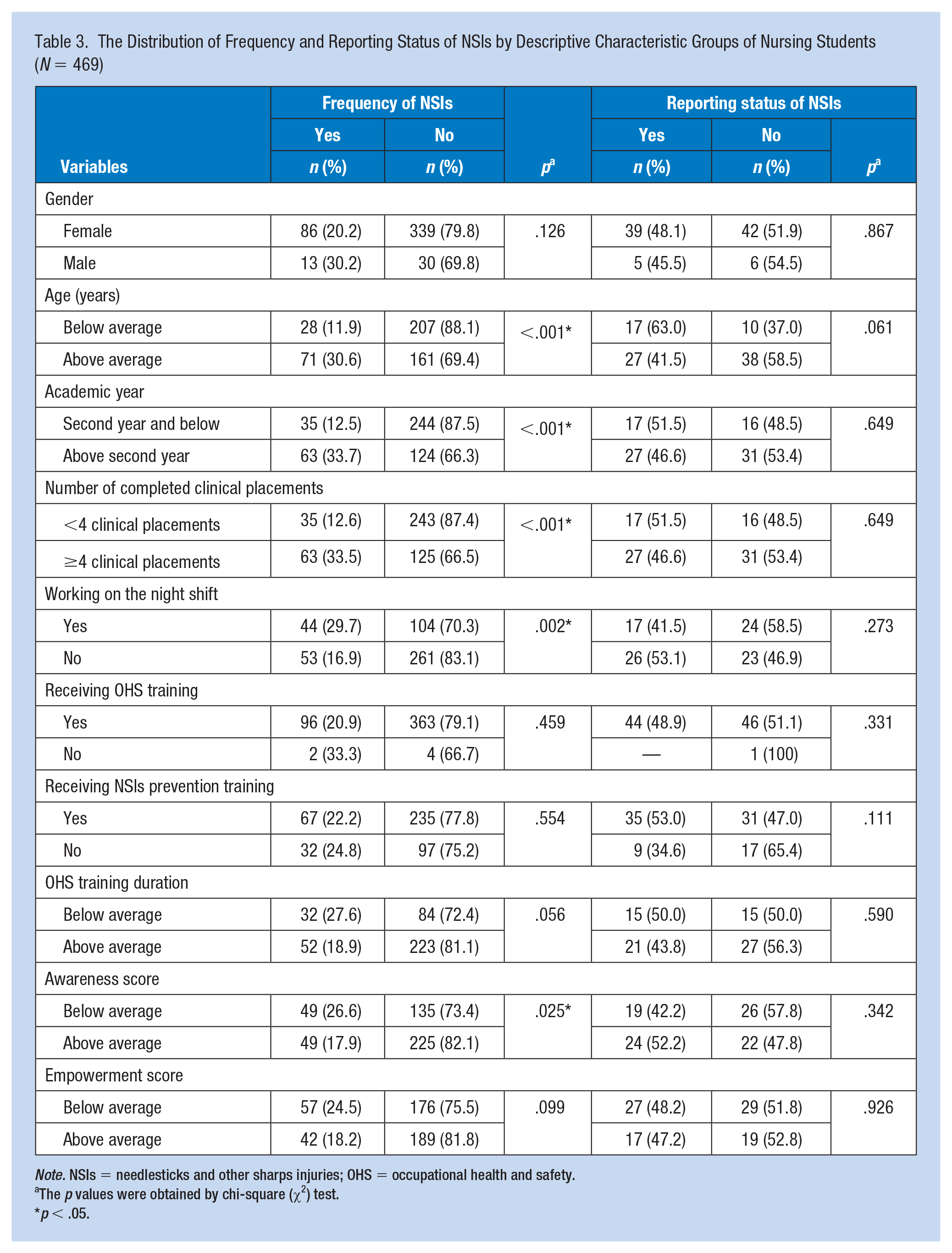
Note. NSIs = needlesticks and other sharps injuries; OHS = occupational health and safety.
The p values were obtained by chi-square (χ2) test.
p < .05.
Although the difference was not statistically significant, the frequency of NSIs was found higher in students who had not received OHS and NSIs prevention training (33.3% and 24.8%, respectively) than in those who had received these trainings (20.9% and 22.2%, respectively). The frequency of NSIs was also higher in students who had OHS training for the below-average duration (27.6%) than in those who had OHS training for the above-average duration (18.9%). The NSIs were more frequent among students who had empowerment scores for below average (24.5%) than those who had empowerment scores for the above average (18.2%). In addition, the frequency of NSIs among students who had used gloves during clinical practices was statistically significantly higher than those who had not (27.8% and 15.5%). However, the use of gloves was statistically significantly higher during clinical placements which the frequency of NSIs was statistically significantly higher. The frequency of NSIs was also higher in males (30.2%) than in females (20.2%), while the reporting frequency of NSIs was lower in males than in females (45.5% and 48.1%).
The frequency of reporting NSIs was higher in students who had received NSIs prevention training (24.8%), had received OHS training for the below-average duration (50.0%), had awareness scores for above average (52.2%), and had empowerment scores for below average (48.2%). The NSIs had been reported to the OHS unit (9.7%), tutors (36.6%), registered nurses (34.1%), the infection control committee (14.6%), doctors (4.9%), and other units or persons (7.3%). Of students who had experienced NSIs, 56.6% had been exposed to only one injury. The most common type of NSIs experienced by students was needlestick injuries (63.5%).
The logistic regression analysis showed that the odds of experiencing NSIs was 4.3 (95% CI = [2.4, 7.4]) times higher in students above the second academic year, 2.3 (95% CI = [1.0, 5.3]) times higher in males relative to females, and 2.5 (95% CI = [1.4, 4.4]) times higher in students who had received OHS training for the below-average duration (Table 4).
Logistic Regression Analysis of Nursing Student Characteristics and Training and Needlesticks and Other Sharps Injuries (N = 469)
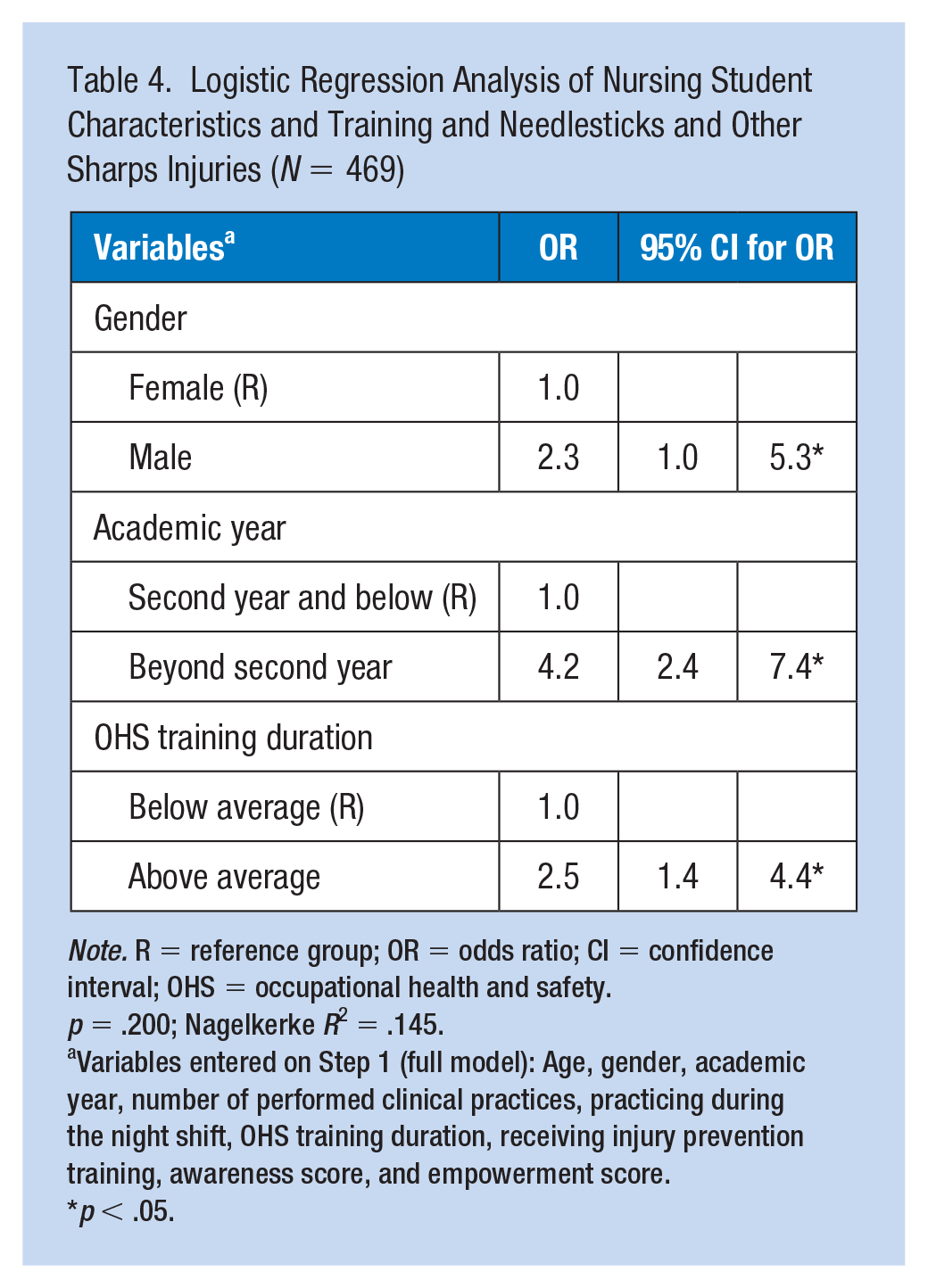
Note. R = reference group; OR = odds ratio; CI = confidence interval; OHS = occupational health and safety.
p = .200; Nagelkerke R2 = .145.
Variables entered on Step 1 (full model): Age, gender, academic year, number of performed clinical practices, practicing during the night shift, OHS training duration, receiving injury prevention training, awareness score, and empowerment score.
p < .05.
Discussion
This study, which examines the OHS awareness and empowerment dimensions of the OHS Vulnerability Measure in nursing practices, observed that one out of every five nursing students in our sample experienced NSIs, and more than half did not report their injuries. These are similar to recent studies (Çakar et al., 2019; Doğru & Akyol, 2018; Kaya & Gök Uğur, 2019) and demonstrate that the occurrence and underreporting of NSIs continue to be problems among nursing students.
In this study, the frequency of NSIs was statistically significantly higher in older students, those beyond the second year, those who had the below-average OHS awareness level, those who had completed four or more clinical placements, and those who had worked on the night shift. Also, results suggested that although the difference was not statistically significant, the high frequency of NSIs could be associated with having a below-average empowerment level, not receiving OHS or NSIs prevention training, receiving OHS training for the below-average duration, and being male. In addition, the logistic regression analysis showed that being beyond the second year, being male, and receiving OHS training for the below-average duration were positively associated with experiencing NSIs.
Smith et al. (2015) have suggested that the level of workplace hazards faced by workers, OHS awareness, and empowerment dimensions are independent of each other in identifying workers’ OHS vulnerability to injuries. Also, previous studies have mentioned that the high exposure to workplace hazards and the lower levels of OHS awareness and empowerment synergistically increase the OHS vulnerability, and so this increase causes higher injury risk (Lay et al., 2016, 2017; Smith et al., 2015; Yanar et al., 2019).
Students beyond their second year had completed more clinical placements and had worked more night shift. In addition, the levels of OHS awareness and empowerment were lower in those students. So, the high prevalence of NSIs among students in the upper academic years could be related to their high exposure to occupational hazards and lower levels of OHS awareness and empowerment. Presumably, the relation between the risk of experiencing NSIs and the age variable was due to the older students in the upper academic years.
In Turkey, the Occupational Health and Safety Law (Ministry of Labour and Social Security [MLSS], 2012a) applies to all workplaces in the public and private sectors and all workers, including apprentices and interns, and mandates employers to ensure a safe and healthful workplace. Within this sense, employers shall provide a minimum of 16 hours of basic OHS training once a year for workers, including students, in workplaces identified as “very dangerous” such as hospitals (MLSS, 2013). In practice, according to the current conditions, universities or health care organizations provide this training for students. Besides, the infection control committees of health care organizations have a legal duty to ensure training, which is commonly known as NSIs prevention training, for workers, including students (Ministry of Health, 2005). The NSIs prevention training includes subjects related to risk factors of NSIs, infection prevention and control measures, biological hazardous waste management, and the process of reporting an injury, while OHS training generally provides information on all of the workplace injuries (Ministry of Health, 2005; MLSS, 2013).
Konijn et al. (2018) has emphasized the additive effect of training on OHS awareness and empowerment levels of workers. In addition, researchers have mentioned that increasing workers’ OHS awareness and empowerment levels through training can reduce injuries (Eyi & Eyi, 2020; Handiyani et al., 2018; Kazi & Bhuiyan, 2018). Probably, for legal obligations, almost all students who participated in this study had received the OHS training, and most of them had received NSIs prevention training. However, students, particularly those in the upper academic years, had not received OHS training for a sufficient period specified in the legal regulations. Accordingly, students’ OHS awareness and empowerment levels were low in general. That is, their knowledge of OHS issues and participation in OHS practices were inadequate. Hence, the occurrence of NSIs was frequent among students.
These findings are significant because they demonstrate that increasing the students’ OHS awareness and empowerment levels through training can reduce the occurrence of NSIs during the nursing education period. Nevertheless, the frequency of NSIs was unexpectedly found higher in male students than in females, although both their levels of OHS awareness and empowerment were nearly equal. Results have demonstrated that male students had less frequently received OHS and NSIs prevention training and more frequently received OHS training for the below-average duration.
The higher prevalence of NSIs among males might be due to they had received less training. But even so, further research is needed to understand why male students had the same levels of OHS awareness and empowerment as females, although they had received less training. Within this context, in future studies, examining the factors which might affect the effectiveness of training, such as recency, technique, date, duration, content, and trainer, can be helpful to clarify the impact of training on students’ awareness and empowerment levels.
The present study has also demonstrated that underreporting of NSIs might be related to students’ awareness and empowerment levels. According to the results, students in the lower academic years had higher levels of OHS awareness and empowerment, and they had reported their injuries more frequently than students in the upper academic years. This finding has suggested that increasing students’ awareness and empowerment levels can reduce underreporting of injuries. Besides, results have also shown that students with higher OHS awareness levels had more frequently reported their injuries, but those with higher empowerment levels had less frequently reported their injuries unexpectedly.
The literature suggests that underreporting of injuries is associated with some factors such as students do not know the negative consequences of injuries or how and where to report their injuries, complex reporting processes, lack of time, and fear of report (Handiyani et al., 2018; Song & Guo, 2019; Wang et al., 2020). According to the results, there was no clarity on reporting of injuries, and only one of 10 students had reported their injuries to the OHS unit. The present study has also shown that there needed to define and structure reporting processes during the education period in OHS functionality.
In practice, infection control committees often implement procedures of post-exposure prophylaxis only in the event of an injury due to sharps contaminated with blood or body fluids (Ministry of Health, 2005). However, OHS units participate in taking all types of protective, preventive, and corrective measures against health and safety risks and recording and notifying processes of OHS events in case of any injury (MLSS, 2012b). Besides, according to the national regulations in Turkey, university administrations shall provide occupational accidents and diseases insurance for nursing students during clinical placements, and health care organizations shall notify occupational injuries experienced by students to authorized bodies (MLSS, 2006). Therefore, reporting of all injuries to OHS units is vital in terms of both preventing NSIs and ensuring students’ access to their social security rights in case of necessity.
Within the scope of this study, it has been recommended to establish a workplace occupational health surveillance system guided by OHS units, together with increasing students’ awareness and empowerment levels. Above all, it is crucial to develop a reporting system that obliges reporting all injuries to the OHS units and integrated with the curriculum. Furthermore, examining factors excluding awareness and empowerment levels regarding underreporting of injuries could contribute to the development process of the reporting system.
This study was conducted with limited participation in a single nursing school that had a mutual safety culture and provided compulsory OHS training to almost all of the students. Although this situation leads to a limitation, it can be accepted as a relative homogeneity in evaluating the results. But it is also significant to keep in mind that the results cannot be generalized. Further research is necessary to evaluate the relationship between awareness and empowerment levels of nursing students and the occurrence and underreporting of NSIs.
Implications for Occupational Health
Nursing schools’ managers and OHS professionals, including occupational health nurses, have ethical, conscientiously, and legal responsibilities to protect nursing students against NSIs and ensure a healthful and safe clinical environment for them.
In addition to existing OHS practices such as avoiding unsafe injection practices, using safety-engineered devices, and providing safe work and infection control guidelines, increasing students’ awareness and empowerment levels can be one of the main approaches for reducing NSIs among nursing students and encouraging reporting of injuries. In this context, it is recommended that occupational health nurses and other OHS professionals consider increasing students’ awareness and empowerment levels by appropriate and efficient training. As a result, evaluating and monitoring awareness and empowerment levels of students with developing a reporting system integrated with the curriculum may open a gateway for reducing NSIs among nursing students both during clinical placements and in postgraduate working life.
Applying Research to Occupational Health Practice
This study demonstrated that the occurrence of needlesticks and other sharps injuries (NSIs) continues to be a primary concern among nursing students, and they do not correctly report their injuries. Findings suggest that the occurrence and underreporting of NSIs might be related to lower levels of students’ occupational health and safety (OHS) awareness and empowerment, and training provided for students could increase their OHS awareness and empowerment levels. As the working intensity and procedures are core to professional practices, clinical placements can be considered a critical period to develop early solutions in OHS practices and reduce OHS vulnerability. Within this context, evaluating students’ OHS vulnerability related to OHS awareness and empowerment dimensions, determining the requirements, and structuring training programs can provide a different approach for OHS professionals, including occupational health nurses, in OHS practices. This approach can contribute to reducing NSIs experienced by students during their clinical placements and in their future working life. However, providing training is not enough. The effectiveness of training provided for students should also be considered, and refresher training should be ensured. Besides, developing a reporting system integrated with the education period will provide an opportunity for evaluating and continuously improving protection measures based on feedback.
Footnotes
Acknowledgements
The authors acknowledge facilitating the permission-related process by Hacettepe University Practice and Research Center for Occupational Health and Safety (Hacettepe Üniversitesi İş Sağlığı ve Güvenliği Meslek Hastalıkları Uygulama ve Araştırma Merkezi [HİSAM]).
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the hacettepe üniversitesi.