
Abstract
Background:
Low-friction slide sheets (SS) are designed to reduce compression loads on the body during manual handling tasks, such as boosting patients. Using SS has been shown to decrease muscle activity in the lower back and upper extremities. However, it is unclear if this effect varies with different bed positions. To investigate this, we studied the effects of SS use, bed height, and their combination on muscle activity during a simulated patient boost.
Methods:
Thirty-three Japanese undergraduate students (age 21.0 ± 1.1 years; 14 men, 19 women) participated. Participants were asked to boost a dummy figure on the bed three times each using four conditions. During the repositioning task, electromyography of eight muscles of the lower back and upper and lower extremities, hip and knee joint flexion angles, pelvic forward tilt angle, and position of the center of mass based on the posterior superior iliac spine were evaluated.
Findings:
Electrophysiological activities of muscles of lower back and upper extremities were significantly lower with SS than without it in both bed positions (30% and 40% of body height); the reduction in muscle activities with SS use was 20% to 40%. Lowering the bed did not affect the SS effect magnitude on reducing muscle activities, although postural changes, including hip and knee joint flexion, were observed.
Conclusions/Application to Practice:
SS reduced muscle activities in the back, upper, and lower extremities when the bed was in the low position, and this effect persisted at a bed height of ≥30% of the participant’s height.
Background
Low back pain is one of the most common health conditions worldwide. The prevalence of chronic low back pain in the general working population is 19.6% (Jonsdottir et al., 2019). Furthermore, chronic low back pain, combined with depression and kinesiophobia, causes a decrease in labor productivity, called presenteeism (Yokota et al., 2019; Yoshimoto et al., 2020). Healthcare workers reported a higher incidence of low back pain than the general population (Alshahrani, 2020). The low work productivity of healthcare workers with lower back pain suggests that low back pain affects the health of healthcare workers and has socioeconomic consequences (Yoshimoto et al., 2020).
Manually lifting patients is one of the risk factors for lower back pain among healthcare workers. As far back as 1995 (Marras et al., 1995), occupational lower back pain has been associated with frequent lifting, stress on the lower back muscles, the lateral and rotational velocity of the trunk, and the angle of the trunk’s forward tilt. Therefore, healthcare workers should frequently lift and move patients horizontally (boosting up) on the bed while bending forward, which increases their risk for a lower back injury.
Some healthcare facilities have established policies and implemented programs for safe patient handling and mobility (American Nurse Association, n.d.). Lifts are recommended to avoid manual patient lifting (Iwakiri et al., 2021). The use of lifts in healthcare facilities has reduced back electrophysiological muscle activities, which are defined in this study as muscle activities and reflect the degree of muscle contraction (Vinstrup et al., 2020) and the incidence of lower back pain among healthcare workers (Gold et al., 2017).
Providing care at a low bed height may increase the burden on healthcare workers’ backs (Larson et al., 2022). Therefore, a bed height of approximately 50% of the height of the healthcare worker is recommended when providing patient care (Tamaru et al., 2017). However, in the case of fixed-height beds or when the bed is not sufficiently high to accommodate tall healthcare workers, the workers should perform a boosting action, where the patient, lying in a bed lower than 50% of their height, is moved horizontally from the foot side to the head side. In addition, since care is not always possible in the ideal bed position (50% of height), measures to prevent lumbar injuries in lower bed positions (e.g., 40% or 30% of height) should be considered.
The SS is considered a more reasonably priced and accessible tool designed to reduce compression loads while positioning patients (Andersen et al., 2019). SSs are made of low friction material and placed between the patient and the bed surface. SS use has decreased muscle activities in the back and upper extremities and subjective exertion (Amini Pay et al., 2021). Healthcare workers experience less fatigue when repositioning patients using a SS (Omura et al., 2019). The introduction of SS has also reduced disability of the spine and extremities and pain in healthcare workers and improved job satisfaction (Alperovitch-Najenson et al., 2020). Moreover, repositioning with a SS, pressure-reducing mattress and heel protection reduces pressure injury occurrence in patients (Källman et al., 2021). A SS is a safety tool for both healthcare workers and patients. However, it is unclear whether the use of SS reduces lumbar muscle activities even in the low bed position.
Therefore, this study aimed to examine the effects of SS use, lowering bed height, and a combination of both on muscle activities on the low back and upper and lower extremities when boosting a simulated patient. We hypothesized that the lower the bed, the greater the stoop, and the greater the strain on the lower back; however, the effect of SS in reducing lumbar and upper extremity muscle activities would be maintained. Experiments based on this hypothesis are expected to provide new insights that could be meaningful to occupational health professionals in protecting the health of healthcare providers.
Methods
This study estimated the effects of two factors (two types of lower bed positions and the presence/absence of a 10 cm SS (TORAYEASY slide sheet, TORAY, Tokyo)). The two types of lower bed positions were defined as 40% and 30% of the participant’s height. Accordingly, the following four conditions were used: a bed that was 40% of the participants’ height without SS (SS−/40%), 40% height with SS (SS+/40%), 30% height without SS (SS−/30%), and 30% height with SS (SS+/30%). The mattress on the bed was wrapped in a cotton sheet, and the SS was placed between the sheet and the dummy figure. The primary outcome was muscle activity in the back. Electromyography measures muscle activity or electrical activity in response to a nerve’s stimulation of the muscle. The test is used to help detect neuromuscular abnormalities. During the test, muscle activity is picked up by electrodes and then displayed on an oscilloscope, which is a monitor that displays muscle activity in the form of waves. For purposes of this study, muscle activity is the measurement of choice as it may best reflect compression load to the body when performing manual handling tasks that are associated with the risk of long- or short-term musculoskeletal disorders.
The weight of the dummy figure was set for each participant based on their body weight. Given that the risk of back injury when performing the repositioning task in a low bed by a single participant and the weight that can be safely lifted is a maximum of 35 lbs (approximately 16 kg) (Centers for Disease Control and Prevention, 2013), the weight of the dummy figure was standardized to 50% and 40% of the body weight for male and female participants, respectively. The dummy figure was made lighter for female participants to account for sex differences in muscle strength. The weight of the dummy figure was set lighter than that of a typical patient to guarantee the safety of the participants.
The repositioning task in this study was horizontally moving a dummy figure lying in the supine position on a SS or sheets to the right side, 10 cm above the bed (boosting up). Participants performed the repositioning task three times each in four conditions (SS−/40%, SS+/40%, SS−/30%, and SS+/30%). A 1-minute rest period was allowed between the trials. Participants performed the tasks alone.
Participants in this study were Japanese undergraduate students enrolled in the Department of Physical Therapy at the Takasaki University of Health and Welfare, Faculty of Health Care, who responded to email recruitment. The exclusion criteria included those whose average back pain in the past week was ≥8 on an 11-point numerical rating scale (NRS), which has been confirmed to have high test–retest reliability (Alghadir et al., 2018) and responsiveness (Ferreira-Valente et al., 2011) and those who complained of anxiety about lower back pain caused by lifting heavy objects. A score of 0 on the NRS was defined as no low back pain, whereas a score of 10 was defined as unbearable low back pain.
Measurements
Muscle Activities
Electromyographic (EMG) activities of eight muscles were recorded at 2000 Hz using wireless sensors (Ultium, Noraxon, Scottsdale, AZ, USA). After cleaning the skin of the measured area, two disposable surface electrodes were attached bilaterally to the target muscles, as recommended by surface electromyography for the noninvasive assessment of muscles (Surface Electromyography for the Non-invasive Assessment of Muscles, n.d.). In addition, a ground electrode was embedded in each EMG sensor used in this study. The raw EMG signals were demeaned, fully rectified, and smoothed by the moving average with a time window of 50 ms. Finally, we normalized the EMG signals of each channel using the peak values across all conditions.
The target muscles for this study were the lumbar erector spinae, lumbar multifidus, rectus femoris, and biceps brachii. Lumbar erector spinae, lumbar multifidus, and biceps brachii are frequently employed in repositioning (Amini Pay et al., 2021) or lifting tasks (Yang, 2018). Lifting styles involve stooping and squatting (Luger et al., 2021), and involvement of the rectus femoris is assumed, particularly in the squat style, which requires large flexion of the hip and knee joints (Slater & Hart, 2017).
Kinematics
Kinematic data were obtained using 13 inertial measurement unit (IMU) sensors at 100 Hz (myoMOTION, Noraxon, Scottsdale, AZ, USA). The IMU sensors were attached to standardized locations on the head, upper trunk, lower trunk, pelvis, upper arms, forearms, thighs, and shanks. Furthermore, one IMU sensor was attached to the chest of the dummy figure to determine movement onset and offset. The IMU system provides raw data of three axial acceleration and processed data of three axial segment angles in the global coordinate, anatomical joint angles, and center of mass (COM) position in the global coordinate. Joint angles calculated from the IMU system are reliable and similar to those obtained from optical motion capture systems (Feuvrier et al., 2020; Khobkhun et al., 2020).
The flexion angles of the bilateral hip and knee joints, pelvic forward tilt angle, and COM position were extracted from the IMU system to assess the kinematics of lifting movements (stooping and squatting) during the repositioning task. The distances in the sagittal, frontal, and horizontal planes between the midpoint of both posterior superior iliac spines (PSIS) and the COM position were calculated. Positive values of these distances represented the superior, anterior, or right from the midpoint of the PSIS.
The EMG and IMU systems were synchronized using an electrical synch signal and integrated into the software (MR3, Noraxon). The IMU signals were upsampled to match the data length with that of the EMG signals.
Subjective Physical Burden
The subjective physical burden (SPB) in this study was also assessed using the NRS because this scale can be used to quantify pain and subjective measurement constructs, such as sleep disturbance (Puelles et al., 2022), fatigue (Machado et al., 2021), and shortness of breath (Chowienczyk et al., 2016). Zero was defined as no physical burden, whereas 10 indicated the greatest physical burden. Participants were asked to verbally confirm their score immediately after the measurement in each condition.
Data Analysis
The minimum sample size required for this study was calculated using the G power version 3.1 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) and was determined to be 23 for the paired t-test, d = 0.8, α = 0.05, and 1 − β = 0.95.
To eliminate bias, we did not screen the undergraduate students who applied but included all of them. The order of the four conditions was randomized by computer-generated random numbers. The EMG and IMU waveforms were checked after each trial, and remeasurements were made if waveforms were lost or abnormal waveforms were observed to address missing data.
Mean, median, quartiles, and maximum and minimum values for muscle activities, angle, and SPB were calculated for the four conditions. The assessed items were compared between the SS−/40% and SS+/40% conditions and between the SS−/30% and SS+/30% conditions to evaluate the effectiveness of SS. In addition, to evaluate the change in the effectiveness of SS use by lowering the bed, the assessed items were compared between SS+/40% and SS+/30% conditions. A paired t-test was used for comparison.
All statistical analyses were performed using R, version 4.1 (R Foundation, Vienna, Austria) or HAD, version 17.2 (Shimizu, 2016). A p value of .05 was set as the significance level and was corrected using Holm’s method to avoid type 1 error. Absolute values of the effect size “d” for the main effect represent a large difference between with and without SS or 40% and 30% height.
The study was approved by the ethics review committee of Takasaki University of Health and Welfare (approval number: 2136) and conducted following the Declaration of Helsinki 1983 (World Medical Association n.d.). Participants were asked to sign a consent form for participation in the study after carefully reading an explanation of the study; for those <20 years of age, guardians were also asked to sign the form. After the measurements were completed, a form allowing withdrawal of consent was also distributed, explaining that the participants could withdraw their consent at any time.
Results
Of the 185 students who received the email requesting participation in the study, 185 students, and 33 (17.8%) responded to the recruitment process. Five of the 33 (15.2%) students had back pain in the past week, with an average intensity of 2 points on the NRS for two students and 3, 4, and 6 points for the other three students. None of the students complained of anxiety about back pain caused by lifting heavy objects. Therefore, all applicants were included in this study. The participants’ mean age was 21.0 ± 1.1 (19–22) years, and there were 14 men and 19 women. The mean heights of the men and women were 173.1 ± 3.6 (168–183) cm and 160.7 ± 4.4 (153–171) cm, respectively, and the mean weights were 66.1 ± 7.9 (56–83) kg and 52.4 ± 3.9 (44–60) kg, respectively.
All participants completed the repositioning task of moving the dummy figure 10 cm upward in all 12 trials (three trials for each of the four conditions).
The effectiveness of SS use at both 40% and 30% bed height positions was greater than the expected (d = 0.8) for the right lumbar erector spinae and lumbar multifidus, bilateral biceps brachii, and SPB. EMG activities of these muscles and SPB were significantly lower in the SS+ condition than in the SS− condition. There were no significant differences in EMG activities during SS use by bed position. However, the bilateral hip and knee flexion angles and pelvic forward tilt angle in the 30% bed height condition were significantly greater than those in the 40% height condition. However, these effect sizes were greater than expected (d = 0.8; Table 1).
Effects of SS Use and Change in the Effectiveness of SS Use by Lowering the Bed on Muscle Electrical Activity and Kinematic Parameters (n = 33)
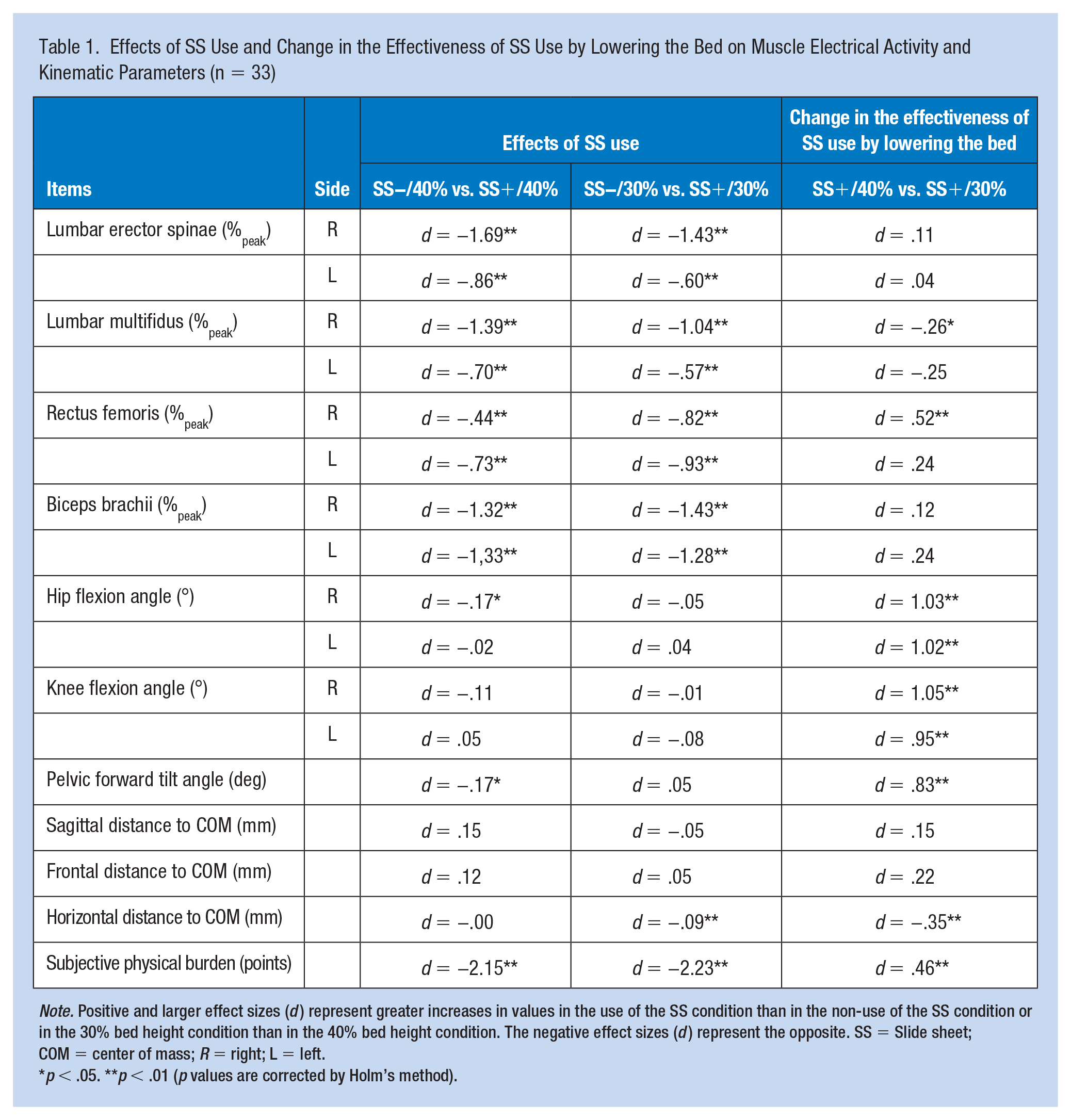
Note. Positive and larger effect sizes (d) represent greater increases in values in the use of the SS condition than in the non-use of the SS condition or in the 30% bed height condition than in the 40% bed height condition. The negative effect sizes (d) represent the opposite. SS = Slide sheet; COM = center of mass; R = right; L = left.
p < .05. **p < .01 (p values are corrected by Holm’s method).
Discussion
Although the use of lifts is the recommended method for preventing back injury in many care settings, it may not always be necessary. An SS may be an appropriate technology in certain situations, such as home care, longterm care or other setting where adjustable beds are not available. However, it was unclear whether the SS, even with a low bed, would effectively reduce the compression load on the back. Therefore, the electrophysiological activities of the low back and extremity muscles and posture were compared under different conditions, combining the presence or absence of SS with beds set at two fixed heights and using a dummy figure as the simulated patient. The effects of SS and bed height on muscle activities were quantitatively evaluated using this method.
Effectiveness of SS Use in Reducing Muscle Activities and SPB
EMG activities of the right lumbar erector spinae and lumbar multifidus, bilateral biceps brachii, and SPB in the SS+ condition were significantly lower with large effects than in the SS− condition, even with two different low beds. The rate of decrease in EMG activities with SS usage ranged from approximately 20% to 40%. The relationship between lifting and EMG activity of back muscles has been examined for decades (Poulsen & Jørgensen, 1971). The SS reduces friction between the dummy figure and the bed surface, allowing the dummy figure to slide over the bed without lifting. This may result in reduced electrophysiological activity of the back muscles. Our results suggest that using an SS reduces the risk of a back injury during repositioning. However, the dummy figure was light; thus, the experiments did not reproduce patient repositioning in a clinical setting with a high degree of accuracy. Moreover, there is a report that the SS does not provide the same physical burden reduction as the lift (Wiggermann et al., 2021). Therefore, further studies are needed to clarify the positions under which the safety of healthcare workers can or cannot be assured using SS.
The greatest reduction in muscle activities was noted in the biceps brachii, which were reduced by approximately 40% on both sides. During the patient repositioning, Novice caregivers showed significantly less activity than veteran caregivers in the spinal erector spinae and rectus femoris. Simultaneously, their biceps brachii were significantly more active (Daikoku & Saito, 2008), indicating that novices tend to move patients using their arm strength. The participants in this study had little experience in care, which may explain why the effect of the SS was more pronounced in the biceps brachii than in other muscles.
No significant difference was found in outcomes related to posture, with or without SS. Therefore, we speculated that using SS did not change the repositioning posture of the healthcare workers, implying that they adopted a similar posture with or without SS. Conversely, it has been reported that using SS increased the forward-leaning of healthcare workers. This discrepancy in results was possibly caused by differences in the weight of our dummy figure (17.6–41.5 kg) and real patients in the previous studies (51 or 70 kg) (Amini Pay et al., 2021).
In addition, the effectiveness of the SS was also found in subjective outcomes. For example, SPB was significantly reduced by half or more in the NRS score with SS use. This reduction rate was similar to that reported by Omura et al. (2019). Therefore, using SS may reduce back muscle activity and SPB, regardless of bed height.
Change in the Effectiveness of SS Use by Lowering the Bed
The comparison of the SS+/40% and SS+/30% conditions showed significant and large effects on bilateral hip and knee flexion angles and pelvic forward tilt angle. Specifically, hip and knee flexion and pelvic forward tilt angles increased as the bed height decreased from 40% to 30% of body height. These significant changes in hip and knee flexion angles should be separated from the effectiveness of the SS and viewed as an effect of the bed height. Conversely, no difference was observed in the relative position of the COM from the pelvis. We believe this finding reflected a squatting style (Washmuth et al., 2022) where participants flexed their hip and knee joints as the bed was lowered so that the height difference between the dummy figure and the participant’s upper body remained unchanged. Since the height difference between the dummy figure and the participant’s upper body did not differ when the bed was lowered, the effectiveness of the SS in reducing muscle activities may have been equivalent regardless of the bed height.
We also observed a significant decrease in right rectus femoris activity as the bed was lowered, although the effect size was smaller than expected. We speculated that the significant increase in the right rectus femoris reflected a starting position where the COM is shifted to the right side, the side on which the body weight is boosting; specifically, a posture where the body weight is shifted to the right foot.
SPB scores increased significantly with lower bed height regardless of SS use, although the effect size was smaller than expected. As the only measured muscles that showed a negative effect for a lower bed were the right rectus femoris, we speculated that the increase in SPB reflected a greater effort by the right rectus femoris to maintain the crouching position. This negative effect of bed height on SPB should not be confused as counteracting the positive effect of using the SS but should be interpreted independently.
These results suggest that the effectiveness of the SS in reducing muscle activities in the lower back and extremities is maintained to the same extent at lower bed heights. However, it should be noted that these findings do not recommend that SS be used as an alternative to lifting technology and equipment.
To the best of our knowledge, this is the first study to systematically and quantitatively evaluate the effects of SS use, bed lowering, and a combination of both on muscle activities in the low back and extremities using a dummy figure. The study confirmed that using SS reduced muscle activities in the low back and extremities, even under lower bed positions, which had not been tested in previous studies. Simulation studies of various SS use situations and the accumulation of knowledge on the effects of SS use will contribute to broadening the range of applications of SS.
This study has some limitations. First, the participation rate was only 17.8% of undergraduates who sent out the recruitment email because the first recruitment met the calculated sample size; therefore, no additional recruitment was conducted. This cohort, composed of undergraduates who took the initiative to respond to the recruitment email, may have been more interested in low back pain and its prevention than undergraduate students who did not respond to recruitment for this study. This bias may also have affected individuals’ choice of strategies for the repositioning task, limiting the generalizability of the findings in this study. Second, the dummy figure’s weight setting was set at 50% and 40% body weight for men and women, respectively, to avoid the onset or worsening of low back pain and incomplete or inability to perform the task for the participants. Based on this setting, the dummy figure weighed approximately 30 kg and 20 kg for men and women, respectively. A complete reproduction of muscle activities in hospital care was not accomplished because the weight was light compared to the average weight of older adults (Shimizu, 2016). This suggests that it is challenging to implement the findings of this study directly in the real world. Therefore, future clinical practice-based studies should be conducted to measure lower back muscle activities among healthcare workers who routinely perform repositioning of patients in the hospital, and the weight of the dummy figure should correspond to the average weight of patients in these studies to assess the actual effectiveness and safety of the SS.
In conclusion, using a dummy figure, this study systematically evaluated the effects of using the SS, lowering the bed, and the combination of both on muscle activities in the low back and extremities. SS significantly reduced muscle activities in the lumbar erector spinae, lumbar multifidus, rectus femoris, and biceps brachii. Lowering the beds further did not significantly increase the muscle activities of the lumbar erector spinae, lumbar multifidus, and biceps brachii. Further lowering of the bed increased the rectus femoris muscle activity but did not attenuate the effectiveness of the SS in reducing muscle activities. The effectiveness of the SS in our experimental study should be validated in actual patients before it can be used in clinical settings.
Implications for Occupational Health Practice
Occupational health professionals can make recommendations for devices, such as lift technology and equipment, based on exposure and ergonomic assessment of the work. The findings of this study provide evidence for occupational health professionals to consider SS as a tool for healthcare workers who position. Although the effectiveness of SS in reducing lumbar strain may be independent of bed height, this experimental study confirmed that SS reduces low back burden at bed heights up to 30% lower than the body height when using dummies that generally weigh less than typical patients.
Applying Research to Occupational Health Practice
This study was an experimental study using a dummy figure that was lighter than most human patients. Therefore, the results of this study may have no immediate impact on occupational health practice. However, the results suggest that SS use reduces the burden on the healthcare worker’s lower back and upper and lower extremities, even when the bed position is lower than the preferred bed position, which is 50% of the height of the healthcare worker. However, additional practical validation using dummy figures of the equivalent weight of actual patients is needed.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231155626 – Supplemental material for Effects of Slide Sheet Use and Bed Position on Muscle Activities in the Low Back and Extremities: A Pilot Experimental Simulation Study
Supplemental material, sj-docx-1-whs-10.1177_21650799231155626 for Effects of Slide Sheet Use and Bed Position on Muscle Activities in the Low Back and Extremities: A Pilot Experimental Simulation Study by Daisuke Higuchi, Yuko Takahashi and Yosuke Tomita in Workplace Health & Safety
Footnotes
Acknowledgements
The authors are deeply grateful to professor Harumi Tsuruta, Department of Nursing, Takasaki University of Health and Welfare, for providing them with the experimental equipment and Editage for proofreading the English text.
Author Contributions
D.H. contributed to the conceptualization, data acquisition, analysis, and writing of the manuscript.
Y. Takahashi contributed to the data acquisition for this work.
Y. Tomita contributed to the interpretation of the data for this work and critical revision of the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gunma Foundation for Medicine and Health Science (grant number: #2, 2021).
Ethical Considerations
The study was approved by the ethics review committee of Takasaki University of Health and Welfare (approval number: 2136). It was also conducted in accordance with the Declaration of Helsinki (1983). Participants were asked to sign a consent form for participation in the study after carefully reading an explanation of the study; for those younger than 20 years of age, their guardians were also asked to sign the form. After the measurements were completed, a form allowing withdrawal of consent was also distributed, explaining that the participants could withdraw their consent at any time.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.