
Abstract
Low-back pain (LBP) is a medical condition that affects most people at some point in their lives. Exercise therapy has been found to be efficacious in treating LBP in some individuals; however, it is unclear which form of exercise demonstrates superior outcomes. It has been postulated that exercise combined with the unique properties of water may demonstrate favorable outcomes. Moreover, studies have evaluated the effectiveness of aquatic therapy as an intervention for patients with LBP. This review aims to explore the efficacy of aquatic therapy as an intervention for LBP. The findings from this review suggest that aquatic therapy is superior to no treatment; however, it did not always prove more effective when compared with other forms of conservative treatment. Whereas the outcome of this review supports aquatic therapy as an effective treatment for LBP, further research is needed to determine if it is superior to other interventions.
Water has many unique properties that make for a favorable exercise medium,
resulting in the suggestion that aquatic therapy programs possess advantages
over other forms of therapy.
Introduction
Low-back pain (LBP) is one of the most common and costly medical conditions in modern society. 1 Between 70% and 84% of people will experience LBP during the course of their lifetime. 1 The large majority of LBP patients—80% to 90%—recover from this condition within a 3-month period2-4; however, the remaining 10% to 20% will suffer from chronic LBP.1-4 The problem of LBP is of economic concern as well. In 1995, LBP patients cost the United States health care system $8.8 billion dollars, with LBP ranking as one of the most costly conditions. 5 Other countries have also noted the high cost of treating LBP, suggesting that LBP is of global economic concern. 6
The exact cause of LBP is often unclear, and disease or injury to many of the low-back structures could be implicated as a potential source of LBP. 7 In fact, only 15% of patients with LBP receive a definitive diagnosis because linking symptoms, imaging results, and physiological changes are often difficult. 7 This presents a challenge to clinicians when determining the most appropriate treatment approach.
There are many treatment options for patients with LBP; however, exercise does seem to have broad applications in its effectiveness. 2 Some studies focus on very specific muscle groups, whereas others focus more on general activity and musculature.8-10 Regardless of the approach, it has been documented that the environment may be one distinguishing factor that may influence outcomes.2,11,12
Water has many unique properties that make for a favorable exercise medium, resulting in the suggestion that aquatic therapy programs possess advantages over other forms of therapy.11,13,14 The physical properties of water such as surface tension and buoyancy may give aquatic therapy unique advantages compared with land-based interventions. These properties influence the length and type of therapy that can be conducted in water as well as progress that can be made in aquatic therapy programs.11,13,14 Ariyoshi et al 15 suggest that the ability to control gravitational force makes aquatic therapy highly advantageous for LBP patients. Also, the patient is able to experience the thermal effects of water much quicker when compared with a temperature controlled, land-based environment. 14
To care for their patients, practitioners need to know which treatments are effective in treating LBP. Although much debate exists regarding interventions for LBP, there seems to be evidence to support exercise therapy.2,11,12,14 These results agree with the suggestion that LBP patients should remain active to avoid prolonged disability. 15 Still, a paucity of literature exists to evaluate the effectiveness of aquatic exercise programs for patients with LBP. 2 Therefore, the purpose of this article is to systematically review the literature pertaining to aquatic exercise therapy and LBP. To our knowledge, there is one other systematic review that addresses aquatic exercise therapy and LBP. 12 However, the current systematic review condenses all relevant information pertaining to aquatic therapy and LBP, including information and studies not present in the previous systematic review. Also, unlike in the previous systematic review, we chose to include only randomized controlled trials in this review.
Aquatic Therapy as an Intervention for LBP
A search was performed to identify studies that addressed aquatic therapy as an intervention for LBP. A brief overview of the studies analyzed can be seen in Table 1.
Overview of Analyzed Studies.
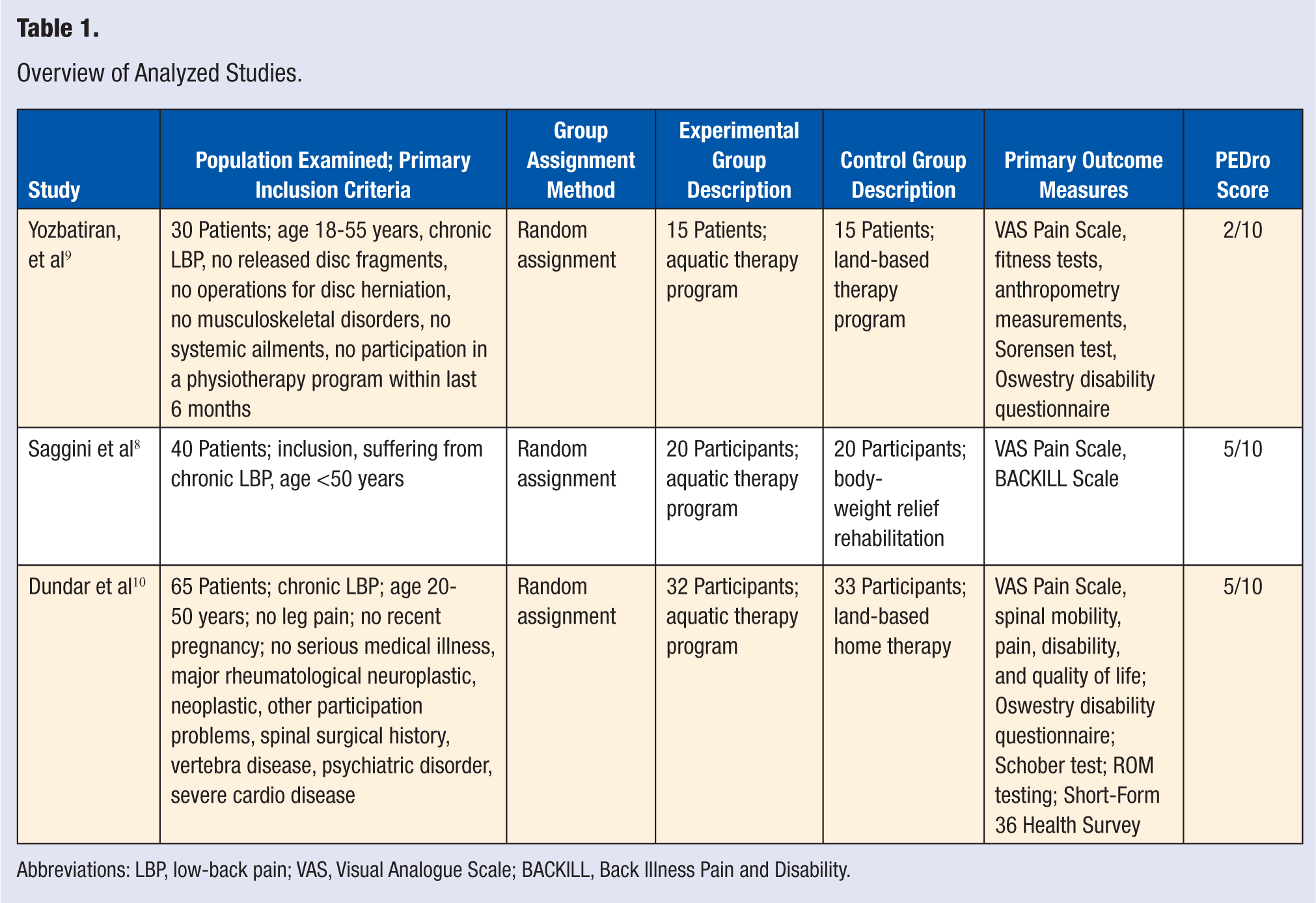
Abbreviations: LBP, low-back pain; VAS, Visual Analogue Scale; BACKILL, Back Illness Pain and Disability.
Methods
Data Sources and Searches
A computerized electronic search was conducted on PubMed (1950 to December 2011), CINAHL (1982 to December 2011), SPORTDiscus (1975 to December 2011), AMED (1985 to December 2011), and PEDro (1929 to December 2011) databases. The following keywords were used independently and in combination: low-back pain, exercise, and aquatic therapy. One researcher (DAO) collected the relevant studies by examining the abstracts to determine eligibility. Another reviewer (WJH) independently reviewed each article for eligibility. If agreement on eligibility could not be determined, a third reviewer (MJK), blinded to the other reviews, determined eligibility.
Study Selection
Articles were retained if they met the following criteria: they (1) used a randomized controlled trial design, (2) were published in a peer-reviewed journal, (3) tested aquatic exercise therapy as a treatment for LBP in at least 1 group, (4) were published in the English language, (5) clearly identified outcome measures for pain or disability at each assessment point.
Quality Assessment
The quality of the included trials was evaluated using the PEDro Scale using scores from the PEDro database. Maher et al 16 found k values to be between 0.36 and 0.80 for individual assessors and 0.50 and 0.79 for consensus ratings generated by groups of 2 to 3. They concluded that the PEDro Scale items’ reliability ratings varied from fair to substantial, and the total PEDro score reliability was fair to good.
Results
Study Selection
The initial electronic database search revealed a total of 541 590 articles. Of these articles, 9 were selected for further review based on the title and abstract. Examination of the full text articles yielded 3 studies that fit inclusion criteria (Figure 1).
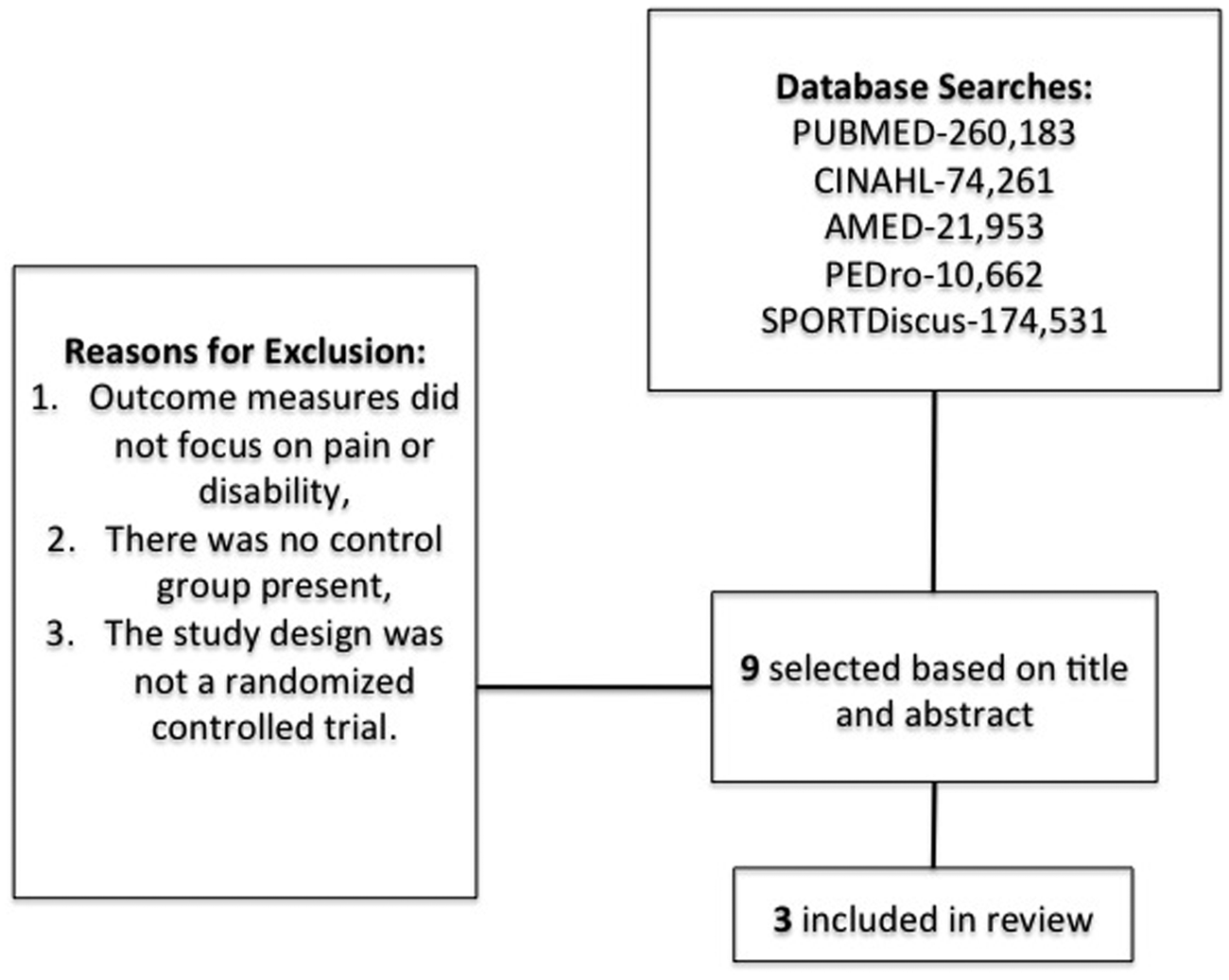
Search strategy for selected articles.
Methodological Quality
The methodological quality assessment using the PEDro Scale gave a mean score of 4 with scores ranging from 2 to 5 (Table 1). Each study used random assignment and baseline comparability. Because of the nature of the studies involved, blinding of the participants or therapists was not possible. However, the study conducted by Dundar et al 10 used blind assessors.
Study Characteristics
Multiple systematic reviews have shown that exercise therapy is an effective method of treatment for LBP patients. 17 Yet there is no consensus on which type of exercise therapy is best. The studies addressed in this review collected data aimed at comparing aquatic therapy exercise programs with land-based therapy exercise programs.
A study conducted by Dundar et al 10 suggests that aquatic exercise therapy is effective in treating patients with LBP. The study consisted of 65 patients between the ages of 20 and 50 diagnosed with chronic LBP. Chronic LBP was defined in this study as having LBP for more than 3 months. Participating patients did not have leg pain, were not recently or currently pregnant, and had no other serious medical illness or symptoms. Patients also did not have a history of spinal surgery, vertebra disease, psychiatric disorder, and known cardiovascular disease. The 65 patients that met the inclusion/exclusion criteria were sequentially assigned to either the experimental or the control group.
The experimental group consisted of 32 patients participating in an aquatic therapy program, which consisted of 5 sessions per week for 4 weeks in a swimming pool at 33°C. The control group participated in a land-based therapy program, which consisted of 1 session with a physiotherapist to review the land-based program. Patients then received notes and instructions on how to continue their therapy at home. To ensure that patients were keeping up with their home-based program, telephone check-ins were made weekly during the entire program (Table 2). The results indicate that aquatic therapy could be more effective than land-based therapy in improving functional ability of LBP patients as assessed by the Oswestry Disability Index (ODI); however, there was no difference between the groups in the Visual Analogue Scale (VAS) Pain Scale.
Group Descriptions Reported by Dundar et al 10 .
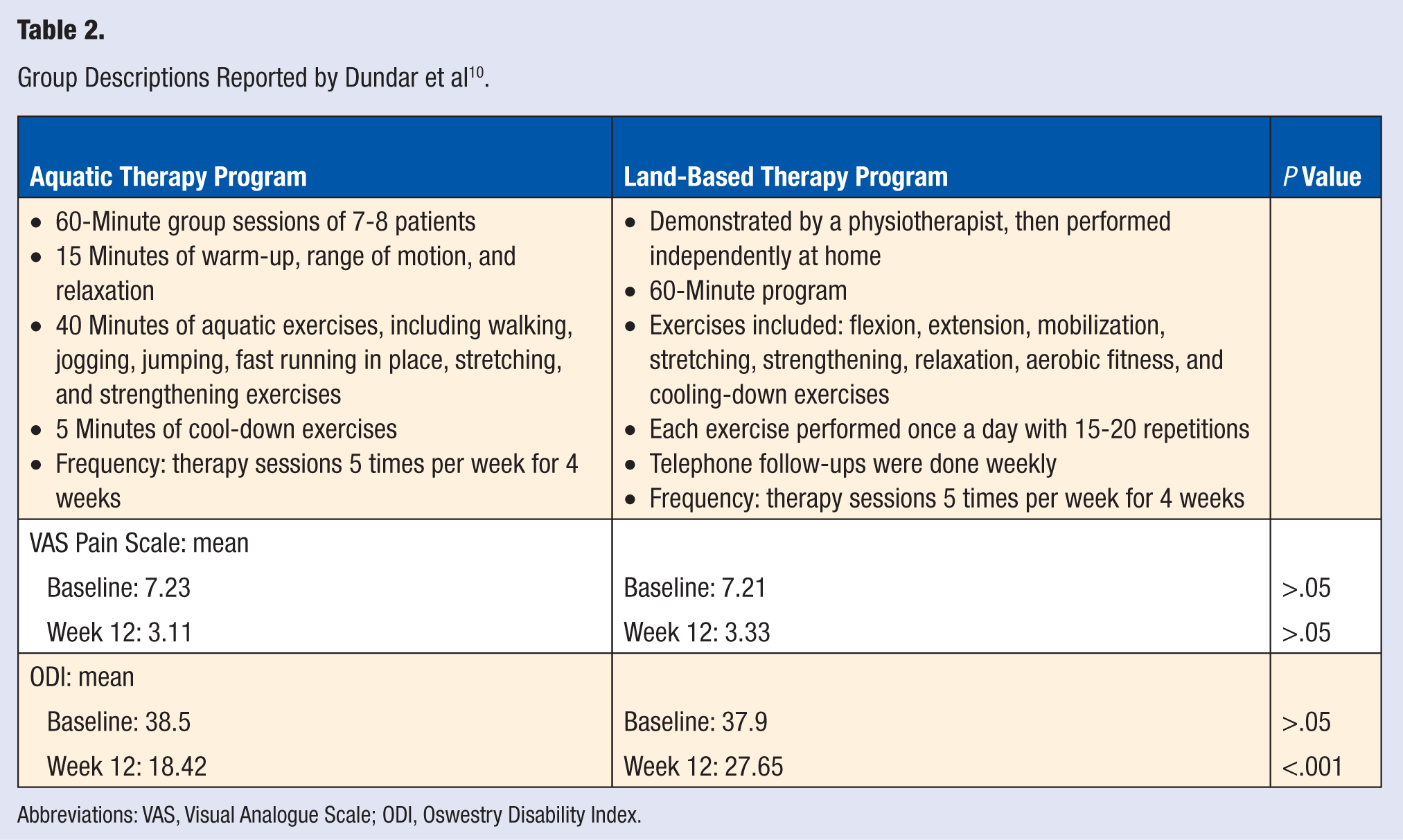
Abbreviations: VAS, Visual Analogue Scale; ODI, Oswestry Disability Index.
A study conducted by Yozbatiran et al 9 also chose to see if the exercise medium had any substantial effect on treatment efficacy (Table 3). The study population consisted of 30 chronic LBP patients who were referred for physical therapy by the same hospital neurosurgery department. This study also chose to define chronic LBP as LBP present for more than 3 months. Participants were between the ages of 18 and 55 years, were suffering from chronic LBP, had no sequestered disc fragments, and had had no operations for disc herniation. They were excluded from the study if they exhibited any musculoskeletal disorders other than LBP, had systemic ailments, or had participated in any physical therapy program within the previous 6 months. Those meeting the defined criteria were then randomized to the experimental or control group.
Group Descriptions Reported by Yozbatiran et al 9 .
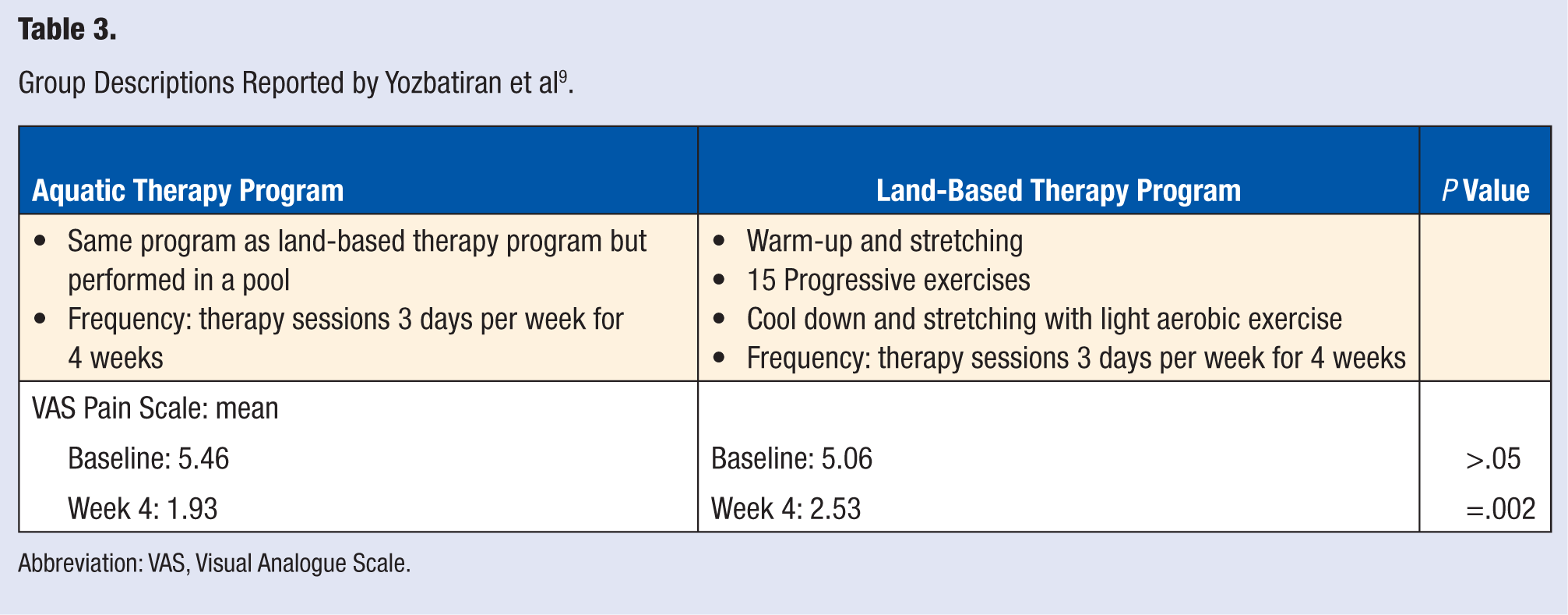
Abbreviation: VAS, Visual Analogue Scale.
The experimental group consisted of 15 patients enrolled in an aquatic therapy program, whereas the control group consisted of 15 patients enrolled in a land-based therapy program. Both programs consisted of 12 physiotherapy sessions during 4 weeks in their respective mediums. Measurements were taken using the VAS Pain Scale, aerobic fitness testing, musculoskeletal fitness testing, motor fitness testing, anthropometry measurements, Sorensen isometric trunk testing, and the ODI questionnaire.
The results did not reveal significant differences between the treatment groups. Both groups showed increased walking distances, lower pain levels, increased dynamic sit-up counts, increased spinal flexibility, significant improvement in isometric trunk exercises, and a slight body fat distribution decrease. Once again, these results yield data supporting aquatic therapy and land-based therapy as effective treatments for LBP patients. Yet the small sample size in this study could have posed some difficulties to seeing differences between the groups.
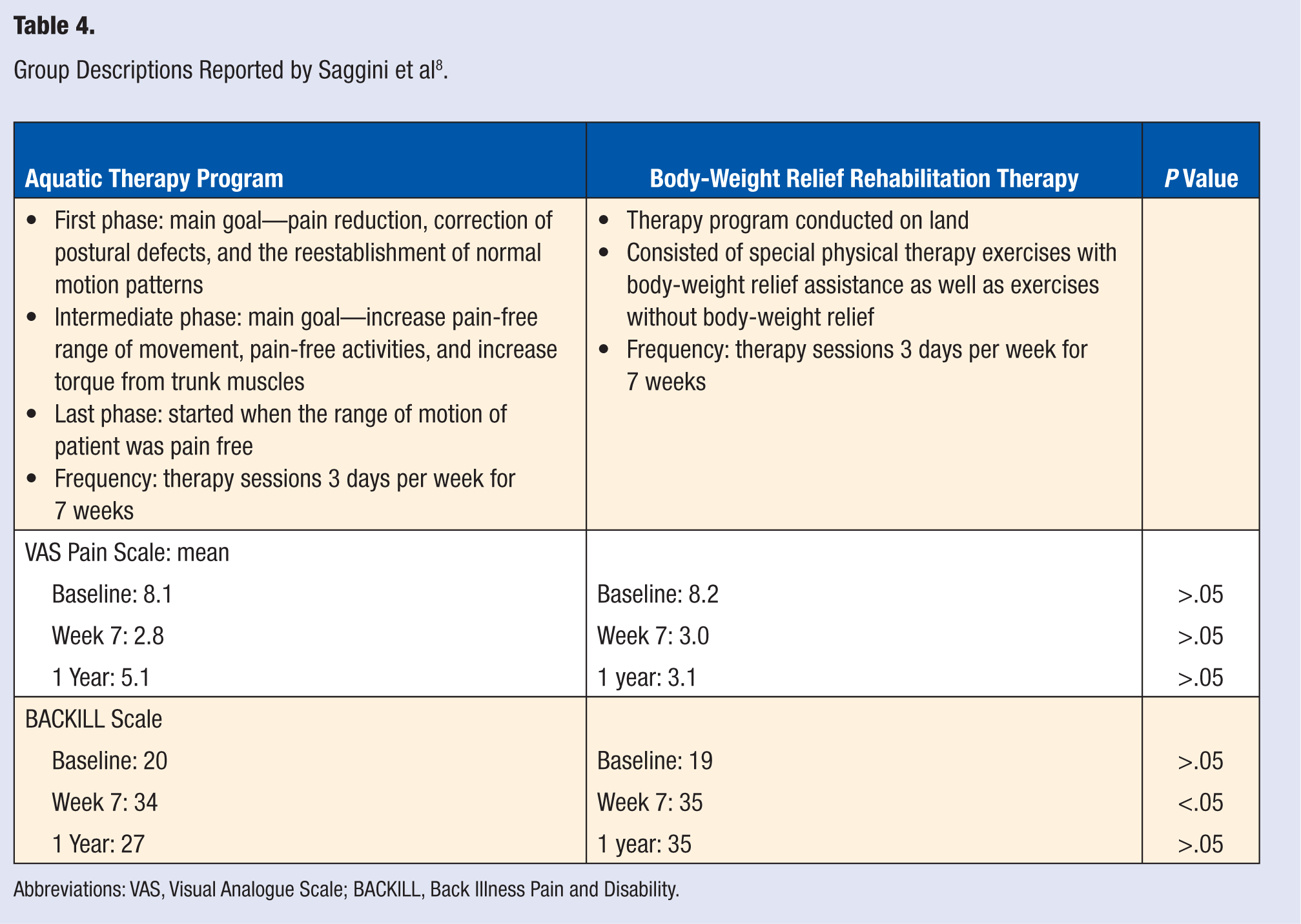
A study conducted by Saggini et al 8 chose to examine the efficacy of aquatic therapy as well as land-based body-weight relief rehabilitation therapy as treatments for LBP patients (Table 4). This study used body-weight relief instruments in the control group program. Also, this study chose to monitor not only short-term results at the end of the study but also long-term results at 1 year posttreatment.
Group Descriptions Reported by Saggini et al 8 .
Abbreviations: VAS, Visual Analogue Scale; BACKILL, Back Illness Pain and Disability.
The study population consisted of 40 consecutive LBP patients younger than 50 years. Patients were excluded from the study if they did not meet the following inclusion criteria: primary LBP for at least 12 months, increase in pain beginning at least 4 months before, MRI-confirmed disc herniation or protrusion, and assurance of cooperation with study requirements. The patients who met the inclusion requirements were then randomly assigned to the experimental or control group.
The experimental group consisted of 20 patients enrolled in an aquatic therapy program 3 times a week for 7 weeks. The aquatic exercises were divided into 3 phases with specific goals. First, exercises were focused on pain reduction, correction of postural defects, and reestablishment of normal motion patterns. Next, the second phase focused on increasing pain-free range of motion, increasing the capacity of trunk muscles to generate torque, and increasing the number of activities that can be performed without pain. Finally, the last phase was initiated when the range of motion of the patient was completely pain free. This phase focused on dynamic control for posture and muscular endurance and included exercises such as twisting and lateral bending and flexing-extending exercises for the hip joint. The control group consisted of 20 patients enrolled in a land-based rehabilitation therapy program. This program consisted of exercises performed with equipment that helped reduce the body weight experienced by the patient during the exercise as well as exercises performed with no mechanical assistance. Similar to the experimental group, this program was given to patients 3 times a week for 7 weeks.
Measurements were taken using a VAS Scale to measure pain as well as the BACKILL (Back Illness Pain and Disability) Scale for assessing spinal column function. The participants were analyzed using these 2 methods prior to the start of treatment, immediately when treatment ended, and at 1 year posttreatment. At the immediate conclusion of their respective exercise programs, both groups showed a significant improvement in both VAS and BACKILL values. However, after 1 year, the control group scores were unchanged from the scores initially following treatment, whereas the experimental group scores were significantly different from the scores initially following treatment. Aquatic therapy proved to be an effective treatment for reducing LBP pain and increasing LBP patient functionality in the short term. However, in the long term, land-based body-weight rehabilitation therapy proved to be more effective for pain and disability caused by LBP.
Discussion
Patients with LBP are presented with many different treatment options, and the unique properties of water have sparked an interest in aquatic-based exercise treatment programs. 2 The results of this systematic review produce evidence to suggest that aquatic therapy can be an effective treatment for LBP patients. However, the results of this review suggest that aquatic therapy is not necessarily more effective than land-based therapy in treating LBP patients.
The primary outcome measurement used to compare and contrast the included studies was the VAS Pain Scale. The VAS Scale works by using a 10-cm line labeled at both ends. One end is labeled “no pain at all” and the other “unbearable pain.” The line may also have points in the middle that are labeled with other pain intensity descriptions. 18 Patients using this tool are asked to point to a spot on the line that best represents the pain intensity they are experiencing. The VAS Pain Scale has become one of the leading pain measurement tools for a multitude of reasons. Because of its simplicity and universal understanding, it is an accepted instrument to assess pain in various populations and cultures, including children from 7 years of age. 19 It is one of the most commonly used instruments to assess pain. A recent systematic review has found the VAS to be not only one of the most commonly used but also one of the most reliable and most responsive assessment tools for chronic LBP. 20 In addition, the VAS has been found to have a significant correlation with the ODI for acute (r = 0.584; P = .000), subacute (r = 0.475; P = .047), and chronic (r = 0.532; P = .000) LBP. 21 The VAS Scale also offers the advantage of being able to statistically quantify the pain level of patients because of its ratio scale properties. Many other pain measurement scales are unable to accomplish this task in an effective manner. 18
Because of the advantages of the VAS Scale, we chose to use it as our main measurement comparison between the included studies. Although the included studies did use the VAS Scale to assess patient pain intensity, they were unclear as to the specific labeling of the scale itself. Having intermediate labels in between the ends of the 10-cm line could create bias in the reporting of pain data. Numbers that are favored, such as the halfway point of 5, could collect an unfair share of the data results. 22 Thus, the most effective and unbiased VAS Scale should have no labeling between the 2 ends of the 10-cm line.22,23 Pain studies in the future should strive to include this detail into their VAS Scale measurement techniques for appropriate interpretation by reviewers.
The long-term effectiveness of aquatic therapy as a treatment for LBP patients seems to be unclear. All the studies collected measurements immediately after termination of the treatment programs. In doing so, all studies produced results suggesting that aquatic therapy was as effective as or more effective than land-based therapy in treating LBP. However, Saggini et al 8 chose to also collect measurement data at 1 year posttreatment. At this checkpoint, the data showed that land-based therapy produced longer-lasting results than aquatic therapy. Perhaps the extra gravitational stress experienced by LBP patients in land-based therapy helps create pain-relieving results that last longer. 11
Dundar et al 10 chose to use a land-based therapy program that was essentially unsupervised. As a result, patients in the land-based group were given an exercise program that lacked assurance of compliance, assurance of good technique, and the positive role of therapist reinforcement. 10 Despite the potential shortfalls created in the land-based exercise program, the results showed that there was no significant difference between the 2 groups in pain intensity as assessed by the VAS Scale. These data suggest that a home-based independent exercise program can be as effective as a therapist-led, out-of-home program in reducing pain experienced by LBP patients. Perhaps future programs, both aquatic and land based, can be effectively designed to treat LBP in an independent environment.
This systematic review chose to analyze the outcomes of LBP treatments as described by the VAS Pain Scale; thus, mechanistic explanations for the results were not discussed at length. Also, because of the few studies included in the review, a meta-analysis was not performed. Because of the use of the VAS Pain Scale as the determination of effectiveness, one should consider that other measurements could be used in the future to analyze the effectiveness of aquatic therapy as a treatment for LBP.
Conclusions
In conclusion, the belief that aquatic therapy is an effective treatment for LBP patients was supported. However, the results did not show that aquatic therapy was more efficient than land-based therapy in treating LBP. Advocates of exercise therapy should find the results of this systematic review encouraging. Exercise therapy, regardless of medium, was proven to be an effective treatment for LBP in all studies addressed. However, further research is needed to test the efficacy of aquatic therapy versus other LBP treatment options.