
Abstract
Background:
Female nurses are a high-risk group for pelvic floor dysfunction (PFD). Predictors of female nurses’ PFD among work-related factors are not well known. The aim of this study was to investigate the prevalence of PFD and its association with workplace conditions among female nurses in China.
Methods:
An online cross-sectional survey was conducted in May 2021. A sample of 380 registered nurses working in six tertiary hospitals in Nanjing, China participated. Data on individual characteristics, work-related factors, the Pelvic Floor Distress Inventory-20 and Pelvic Floor Impact Questionnaire-7 were used.
Findings:
The overall prevalence of PFD among nurses was 83.9%, with 43.9% of participants experiencing pelvic organ prolapse, 66.6% experiencing anorectal dysfunction and 60.5% experiencing lower urinary tract symptoms. In terms of work-related factors, PFD was associated with heavy lifting, pushing, and carrying at work, delayed toileting at work and fluid intake. Female nurses with PFD reported lower quality of life (QoL) relative to nurses without PFD.
Conclusions/Application to Practice:
Our findings provide initial insights into workplace conditions that promote PFD among female nurses. Occupational health nurses should consider providing educational information for female workers who are potentially at risk for PFD and consider integrating screening of PFD into practice.
Background
Pelvic floor dysfunction (PFD) is a broad term used to describe the clinical conditions of the pelvic floor, caused by pelvic floor support tissue damage, dysfunction and degenerative diseases, mainly lower urinary tract symptoms (LUTS), anorectal dysfunction, pelvic organ prolapse (POP), pelvic pain and sexual dysfunction (D’Ancona et al., 2019). More than 50% of women are affected by PFD worldwide (Milsom et al., 2014). The top three symptoms are LUTS, anorectal dysfunction and POP, and the prevalence in China is 39.7% to 55.5%, 30.9% (L. Zhang et al., 2015; W. Zhang et al., 2005) and 1.28% (Chan et al., 2013), respectively. Although it is not a life-threatening condition, evidence suggests that PFD is chronic and related to lower quality of life (QoL) and a decline in physical, social, and mental health (Berzuk & Shay, 2015). Women with PFD are more likely to experience decreased sexual activity (Tannenbaum, 2015), reduced social activities, and emotional disturbances (Choi et al., 2016). Furthermore, with diagnosis and treatment, PFD contributed to high consumption of healthcare services and low workforce participation.
Despite the high prevalence and negative effects of PFD, its pathogenesis is not well understood. The consensus is that the development of PFD is a complex process secondary to multifactorial etiology. Pregnancy and childbirth are recognized as important risk factors for women’s PFD (Li, 2014). In addition, the physiological degeneration of the pelvic floor that occurs with increasing age can cause PFD (Kim et al., 2012), which is more likely to occur in elderly and perimenopausal women. The available evidence also suggests that many factors are related to PFD, including higher parity (Wang et al., 2011), higher body mass index (BMI) (Liao et al., 2008), chronic cough, and unhealthy toileting behavior (Liu, 2013). These risk factors are closely related to a recurrent increase in intra-abdominal pressure, which leads to fatigue and damage to the muscular and connective structures of the pelvic floor muscles (Abrams et al., 2016; Erekson et al., 2015).
Individual characteristics are well known to cause PFD but, in general, the influence of workplace conditions on PFD has been ignored. Regarding nurses, the majority is female and constitutes almost half of the healthcare workforce (Wan et al., 2017). As a specific occupational group, female nurses have a high incidence of PFD (Lopes et al., 2019). Nurses spend a great deal of time at work, and they face potentially damaging job conditions and environmental factors. Because workplace conditions differ among various economic states, a study to explore the association between PFD and nurses’ workplace conditions in each region or country is necessary to improve the healthcare of female nurses.
With a current shortage of nurses and a rapidly aging population in China, nurses face a heavy workload and high levels of occupational stress (Jia et al., 2020; Yin & Qian, 2020). The spirit of Chinese traditional culture advocates the spirit of dedication; nurses always make the patient the center of their work, and they often reduce or delay toileting to take care of their patients. Most nurses reduce their water intake due to their busy work schedules. Since automation equipment is not advanced and there are a limited number of caregivers, nurses usually need to move beds and wheelchairs, carry heavy instruments, and transport patients (Wang et al., 2011). In the working model of Chinese nurses, except for those who specialize in handling medical orders, nurses are on their feet most of their shift and only sit down briefly to add notes to patient charts (Xu, 2016). These unique workplace characteristics may be related to the PFD epidemic.
To our knowledge, existing studies (Choi et al., 2016; Liao et al., 2009; Wan et al., 2017) on Chinese nurses’ PFD are almost all focused on single-symptom LUTS, and the exploration of related factors is focused on individual characteristics. We sought to investigate the distribution of the top three symptoms of PFD among female nurses The purposes of this study were to examine the prevalence of PFD and to identify what workplace factors are associated with PFD among a sample of female nurses in China.
Methods
We conducted an anonymous cross-sectional survey among nurses employed in Nanjing, China. We sent the link of the online questionnaire to the nursing department of all tertiary hospitals in Nanjing, and the nursing department forwarded it to their nurses. Informed consent was provided at the beginning of the online survey and participants needed to agree to participate before continuing to the survey questions. Nurses were eligible to participate if they were: female registered nurses, at least 18 years of age, had proficiency in Chinese, and had access to the internet. Nurses were excluded if they were pregnant or had given birth in the previous 6 months and/or had a diagnosis and treatment for PFD.
Data Collection
Data were collected from May 1 to 27, 2021, through the online platform Wenjuanxing (www.wjx.cn), on which only a fully completed questionnaire can be uploaded. Completing the entire questionnaire took approximately 8 to 10 minutes. The participants were informed of the objectives and procedures of the study.
The questionnaire ascertained information regarding individual and work-related conditions. Individual characteristics included: age, BMI (calculated from self-reported weight and height, [kg/m2]), education level, marital status, menstruation (regular: the menstrual cycle is 24–35 days and the period lasts 2–7 days; irregular: irregular: without a predictable cycle or duration), history of sexual activity (yes; no), prior pregnancy delivery (yes: vaginal delivery and/or cesarean section; no: never given birth), living status (alone: have lived alone for at least 1 year; shared accommodations: have lived with two or more people for at least 1 year), exercise frequency (almost never, 1–2 times/week, ≥3 times/week), smoking (yes: past or current; no: never), alcohol (yes: past or current; no: never), history of a urinary tract infection (yes/no), history of obstetrics and gynecology surgery (yes/no), and one or more chronic conditions (constipation, chronic cough, diabetes, and hypertension).
Work-related variables included: work department, number of years worked, number of hours worked per day, number of hours of standing per day, being too busy to drink fluid at work (never; sometimes: 1 day a week or less; usually: 2 or 3 days a week; always: every day or nearly every day), amount of fluid intake per day (<500 mL/day, 500–999 mL/day, ≥1000 mL/day), days per week toileting was delayed because of busy work (never; sometimes: 1 day a week or less; usually: 2 or 3 days a week; always: every day or nearly every day), time duration of delayed toileting (<0.5 hour, 0.5–1 hour, 1–2 hours, >2 hours), and how many days per week they were required to do the following tasks such as heavy lifting\pushing\carrying at work (never; sometimes: 1 day a week or less; usually: 2 or 3 days a week; always: every day or nearly every day (Lopes et al., 2019)).
We administered the Pelvic Floor Distress Inventory-20 (PFDI-20) Chinese version (Ma et al., 2019) for measure pelvic floor symptoms and the degree of distress and discomfort associated with those symptoms. The scale consists of three subscales: Pelvic Organ Prolapse Distress Inventory (POPDI-6), Urinary Distress Inventory (UDI-6), and Colorectal-anal Distress Inventory (CRADI-8). Participants were asked to complete questions in which they were initially asked to indicate yes/no about a symptom (e.g., pressure in lower abdomen). If not, they were scored “0” on the scale, if yes, they were then asked to rate the degree to which the symptom “bothered” them on one 4-point scale ranging from not at all (1) to quite a bit (4). Each item within the scale were scored and multiplied by 25 to achieve a total maximum score of “100.” The score range of each subscale is 0 to 100, which is the sum of item scores divided by the number of items. The scale score range of “0” (none/minimal symptoms) to “300” (maximum symptoms) (Barber et al., 2005).
We also administered the Pelvic Floor Impact Questionnaire-7 (PFIQ-7) Chinese version (Zhu et al., 2011) which includes three corresponding subscales pertaining to symptoms that impact the participants activities, relationships, and/or feelings including Urinary Impact Questionnaire (bladder and urine symptoms) (UIQ-7), Colorectal–Anal Impact Questionnaire (bowel and rectum symptoms) (CRAIQ-7), and Pelvic Organ Prolapse Impact Questionnaire (vagina or pelvis symptoms) (POPIQ-7). Participants were asked to answer questions based on a Likert-type scale of not at all (0), somewhat (1), moderately (2), and quite a bit (3). Each item within the scale were scored and multiplied by 33.3 to achieve a total maximum score of “100.” The score range of each subscale is 0~100, which is the sum of item scores divided by the number of items. The scale score range of “0” (no negative impact) to “300” (high negative impact).
The study was approved by the Committee on the Ethics of Medical Research of the Second Affiliated Hospital of Nanjing University of Chinese Medicine (2021SEZ-027-01).
Data Analysis
Continuous variables were calculated as means and standard deviations (SDs), whereas categorical variables are presented as frequencies with percentages. First, the influencing factors were analyzed by univariate logistic regression. We set the significance level p < .10 as the criterion for including the variables. Second, based on the results of univariate logistic regression analysis, we identified the most significant variables associated with POPDI-6, CRADI-8, UDI-6 among the work-related factors. We then selected independent variables on the basis of their associations with the outcomes of a change in effect estimate of more than 10% (Jaddoe et al., 2014). We then incorporated these independent variables into a multivariate logistic regression equation to further clarify factors influencing PFDI-20. Each of the outcome variables were operationalized into a dichotomous variable in which a score of “0” was defined as no symptoms, and score ≥1 was defined as having symptoms. The PFDI-20 with score “0” indicated the participants had no PFD symptoms and with score “1–300” indicated participants experienced at least one symptom among LUTS, anorectal dysfunction, and POP. The POPDI-6 with score “0” indicated the participants had no POP symptoms and with score “1–100” indicated participants experienced POP symptoms. The CRADI-8 with score “0” indicated the participants had no anorectal dysfunction symptoms and with score “1–100” indicated participants experienced anorectal dysfunction symptoms. The UDI-6 with score “0” indicated the participants had no LUTS and with score “1–100” indicated participants experienced LUTS.
Odds ratios and 95% confidence intervals were calculated for all regression analyses. Pearson’s correlation analysis was carried out to examine the relationships between the PFDI-20 and PFIQ-7. Data were analyzed using R 4.0.3 and SPSS 20.0.
Results
A total of 380 female nurses participated in this study (Table 1), including 86.8% aged 18 to 39 years old. A total of 73.4% of the participants had bachelor’s degrees, 66.8% were married, and 61.3% reported that they had previously given birth. More than half of the participants (60.3%) had worked for 1–9 years, and 62.4% worked 6–8 hours per day. A total of 33.4% of participants worked in the medical department, and 34.2% worked in the surgical department.
Demographic and Selected Work-Related Characteristics of Study Nurses

Note. N = 380. BMI = body mass index.
The overall prevalence of PFD among female nurses was 83.9%, with 43.9% reporting POP, 66.6% experiencing anorectal dysfunction and 60.5% experiencing LUTS (Table 2). The mean score of the PFDI-20 was 42.34 (SD = 38.09, range: 3.13–229.17). The mean score of the POPDI-6 was 16.97 (SD = 11.38, range: 4.17–50). The mean score of the CRADI-8 was 18.33 (SD = 15.76, range: 3.13–100). The mean score of the UDI-6 was 21.42 (SD = 16.99, range: 4.17–100).
PFDI-20 Scores Among the Study Nurses
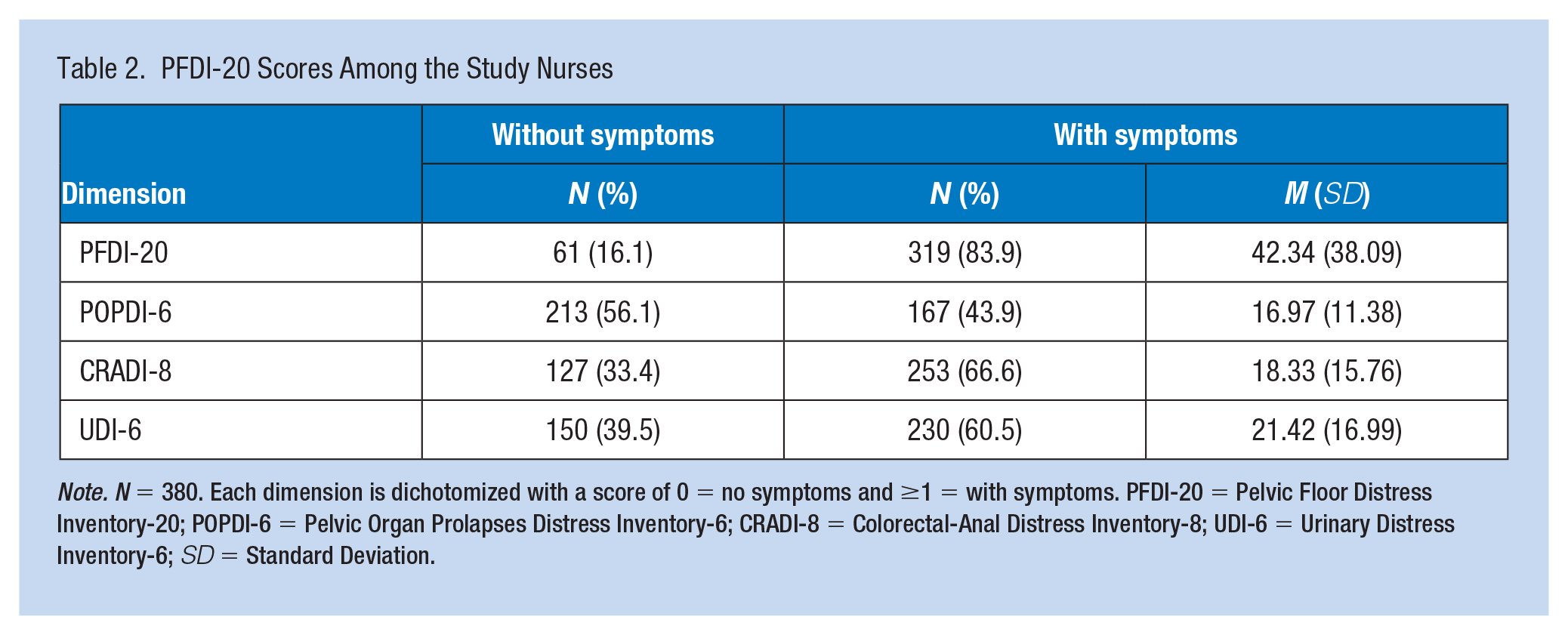
Note. N = 380. Each dimension is dichotomized with a score of 0 = no symptoms and ≥1 = with symptoms. PFDI-20 = Pelvic Floor Distress Inventory-20; POPDI-6 = Pelvic Organ Prolapses Distress Inventory-6; CRADI-8 = Colorectal-Anal Distress Inventory-8; UDI-6 = Urinary Distress Inventory-6; SD = Standard Deviation.
Univariate logistic regression analysis (Table 3) indicated significant differences between heavy lifting\pushing\carrying and the UDI-6, CRADI-8, and POPDI-6 scores. Based on model analysis, we found that nurses who had previously given birth and those with longer hours of delaying toileting and heavier lifting\pushing\carrying were more likely to report PFD. The higher frequency of delayed toileting nurses had, the higher risk of LUTS and anorectal dysfunction those reported. Nurses who drank more water were more likely to suffer from LUTS. Nurses with long working years had higher likelihood of POP. Besides, nurses having sexual activity, with higher BMI, sharing accommodations with others, reporting a history of urinary tract infection, obstetrics and gynecology surgery, chronic diseases (constipation, chronic cough, diabetes, and hypertension), or with longer hours standing per day were more likely to experience anorectal dysfunction.
Univariate Associations of PFD in Female Nurses by Demographic and Work-Related Characteristics
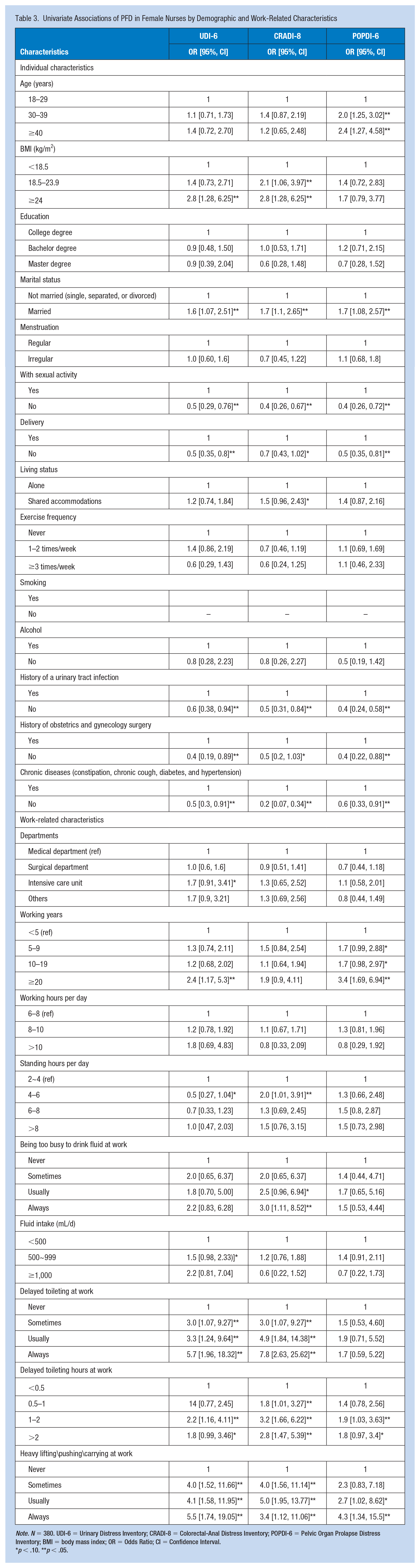
Note. N = 380. UDI-6 = Urinary Distress Inventory; CRADI-8 = Colorectal-Anal Distress Inventory; POPDI-6 = Pelvic Organ Prolapse Distress Inventory; BMI = body mass index; OR = Odds Ratio; CI = Confidence Interval.
p < .10. **p < .05.
As shown in Table 4, heavy lifting\pushing\carrying at work, delayed toileting at work, fluid intake, and delivery were the significant influencing factors of the UDI-6. The risk of LUTS was 4.2 (95% CI:1.07–17.6) times more likely for nurses who indicated “always” heavy lifting\pushing\carrying at work compared to those who reported never, 4.0 (95% CI: 1.35–13.24) times more likely for nurses who indicated “usually” and 3.9 (95% CI: 1.30–12.59) times more likely for nurses who indicated “sometimes.” The risk of LUTS was 4.4 (95% CI: 1.07–19.29) times more likely for nurses who indicated “always” with delaying toileting at work compared to those who reported never, 4.2 (95% CI: 1.39–15.32) times more likely for female nurses with fluid intake ≥1,000 mL/d compared to those with fluid intake <500 mL/d, and 2.0 (95% CI: 1.23–3.31) times more likely for female nurses with fluid intake 500 to 999 mL/d compared to those with fluid intake <500 mL/d. A reduction in LUTS of 0.5 (95% CI: 0.33–0.81) was observed for nurses without delivery compared to those with delivery. Significant influencing factors of the CRADI-8 included delayed toileting at work, sexual activity, and chronic diseases (constipation, chronic cough, diabetes, and hypertension). The risk of anorectal dysfunction was 20.3 (95% CI: 1.87–514.41) times more likely for nurses who indicated “always” heavy lifting\pushing\carrying at work compared to those who reported never. A reduction of CRADI-8 of 0.4 (95% CI: 0.19–0.81) was observed among nurses without sexual activity compared to those with sexual activity, and 0.1 (95% CI: 0.06–0.32) times more likely for female nurses without chronic diseases (constipation, chronic cough, diabetes, and hypertension) compared to those with chronic diseases. In terms of the POPDI-6, heavy lifting\pushing\carrying at work and age were the primary risk factors. The risk of POP was 4.9 (95% CI: 1.38–19.54) times more likely for female nurses who indicated “always” heavy lifting\pushing\carrying at work compared to those who reported never and 2.2 (95% CI: 1.01–4.74) times more likely for female nurses aged 30 to 39 years compared to those aged 18 to 29 years.
Binary Logistic Regression for the Factors of Influence on PFD Including UDI-6, CRADI-8, and POPDI-6 in Female Nurses
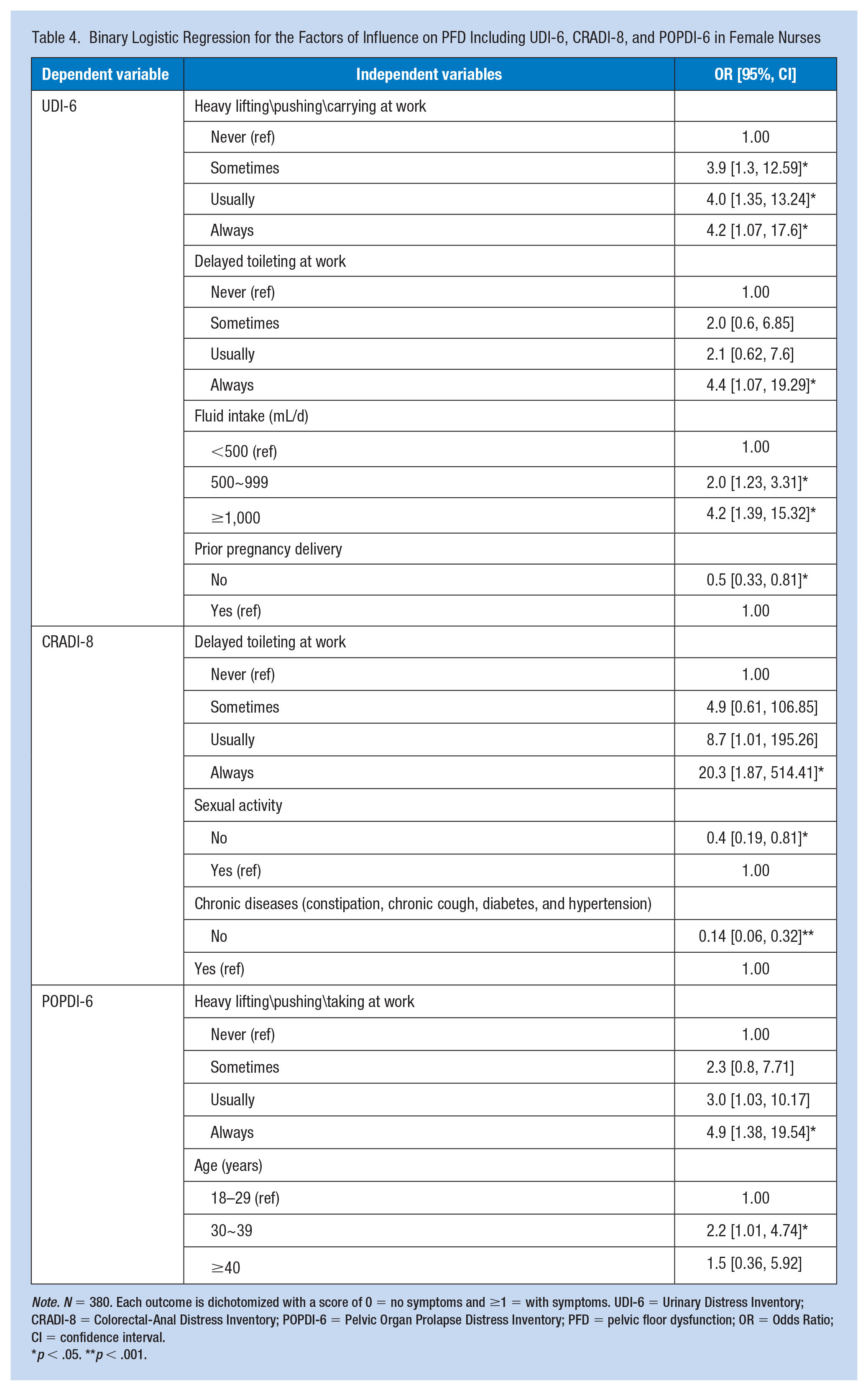
Note. N = 380. Each outcome is dichotomized with a score of 0 = no symptoms and ≥1 = with symptoms. UDI-6 = Urinary Distress Inventory; CRADI-8 = Colorectal-Anal Distress Inventory; POPDI-6 = Pelvic Organ Prolapse Distress Inventory; PFD = pelvic floor dysfunction; OR = Odds Ratio; CI = confidence interval.
p < .05. **p < .001.
The scores of PFIQ-7 (0-300) indicate the impact of PFD on the participants’ QoL, the higher the participant’s scores, the greater the negative impact of PFD symptoms. Scores from the female nurses’ PFIQ-7 (57.29 ± 62.31) indicated that PFD had a negative impact on their QoL. The mean score of the UIQ-7 was 26.40 (SD = 20.97). In terms of the CRAIQ-7, the mean score was 28.04 (SD = 22.98). Regarding the POPIQ-7, the mean score was 27.25 (SD = 22.30). The female nurses’ QoL was negatively affected in all three subdomains. There was a statistically significant positive correlation between PFDI-20 and PFIQ-7 (r = 0.520; p < .001); UDI-6 and UIQ-7 (r = 0.507; p < .001); CRADI-8 and CRAIQ-7 (r = 0.469; p < .001); POPDI-6 and POPIQ-7 (r = 0.395; p < .001), indicating that the more severe symptoms of PFD nurses showed, the lower QoL they had (Table 5).
Correlation Between Pelvic Floor Function (PFDI-20) and PFIQ-7 Scores Among a Sample of Nurses
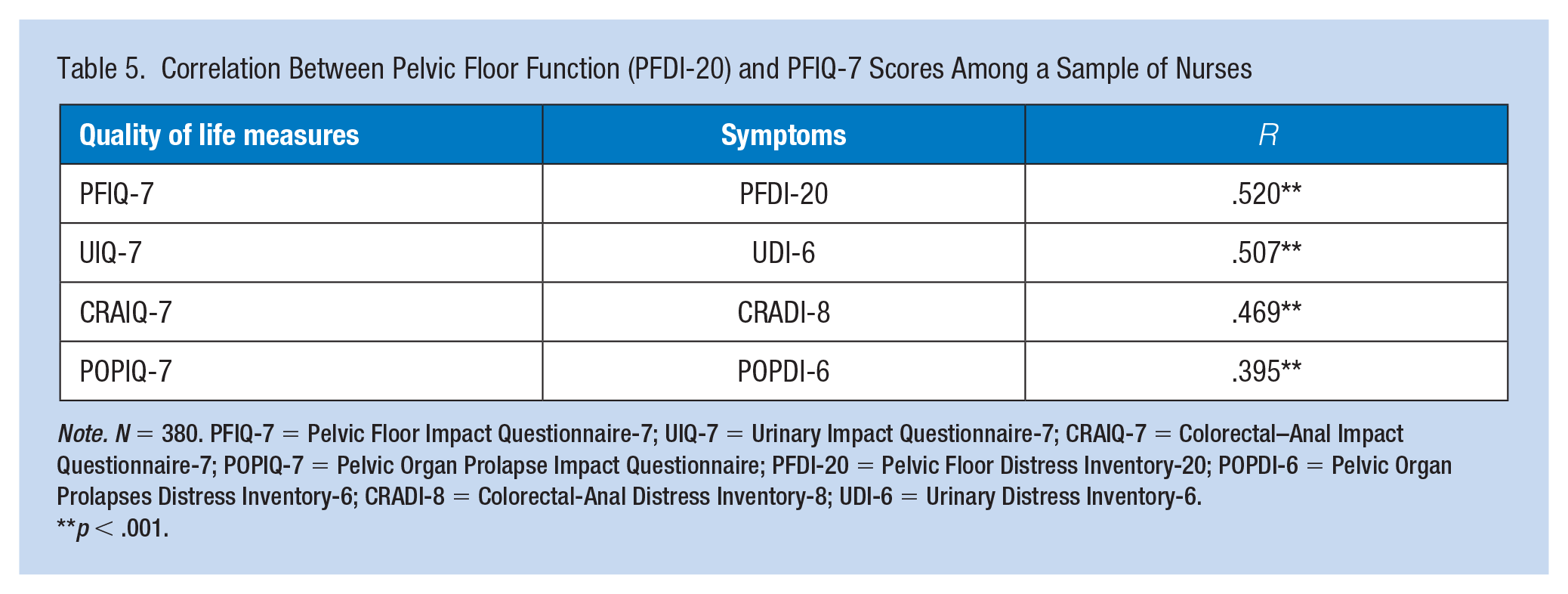
Note. N = 380. PFIQ-7 = Pelvic Floor Impact Questionnaire-7; UIQ-7 = Urinary Impact Questionnaire-7; CRAIQ-7 = Colorectal–Anal Impact Questionnaire-7; POPIQ-7 = Pelvic Organ Prolapse Impact Questionnaire; PFDI-20 = Pelvic Floor Distress Inventory-20; POPDI-6 = Pelvic Organ Prolapses Distress Inventory-6; CRADI-8 = Colorectal-Anal Distress Inventory-8; UDI-6 = Urinary Distress Inventory-6.
p < .001.
Discussion
In this study, we aimed to understand the prevalence of PFD among Chinese female nurses and clarified the relationships between PFD and work-related factors. The investigation showed that approximately 84% of study participants reported experiencing at least one type of PFD, which was significantly higher than the prevalence reported in Chinese women overall (Zhang et al., 2015; Zhu et al., 2009). These prevalence data are higher than those reported in studies from the United States (Markland et al., 2010), Turkey (Yağmur & Ulukoca, 2010), and Sweden (Stenzelius et al., 2004). Of the PFD reported, 60.5% experienced LUTS, which is similar to the findings of Wan et al. (2017), who reported that nearly 68% of the 636 female clinical nurses in tertiary hospitals in Jinan experienced at least one type of LUTS. However, this prevalence was lower than that found in a study of 1,070 female nurses in Beijing (Zhang et al., 2013), which showed that 89.6% displayed at least one symptom of LUTS. Nevertheless, the prevalence of LUTS among female nurses in this study was higher than the prevalence (55.5%) in the general population of adult women in China (Zhang et al., 2015). Regarding anorectal dysfunction, in this study, 66.6% had anorectal dysfunction, which is higher than the findings of general population-based studies in other countries (Matthews et al., 2013; Rogers et al., 2018); however, studies on the prevalence of anorectal dysfunction in Chinese women are sparse, and only one study reported that the prevalence of fecal incontinence was 28% among female nurses in China (Xu et al., 2016). The prevalence of POP among female nurses was 66.6% in this study, which is comparable to the prevalence of 70.6% among Taiwanese nurses (Tosun et al., 2019). Foreign studies revealed that the prevalence of POP ranges from 4.3% to 52.3% in women (Horst et al., 2017; Woodman et al., 2006). Although there are limited reports on anorectal dysfunction and POP among Chinese nurses, this study found a higher prevalence than that in the general population.
In this study, we found that an increased risk of PFD was associated with work-related factors among female nurses, especially with heavy lifting\pushing\carrying and delayed toileting at work. Female nurses stated that LUTS and POP increased in frequency as heavy lifting\pushing\carrying tasks increased. These findings are consistent with a previous study (Higa & Lopes, 2007; Lopes et al., 2019), which found that heavy lifting was associated with LUTS among female nurses. Woodman et al. (2006) reported that women who were laborers/factory workers had significantly more POP than women in the other jobs, and these jobs require more heavy lifting. One study (Jørgensen et al., 1994) was conducted in a population of assistant nurses in Denmark, where heavy lifting at work was associated with a 60% increase in the risk of a POP operation. Heavy lifting is more common in Chinese nurses’ work, due to the lack of advanced automation equipment and specific care staff, and almost all equipment handling and transportation tasks are completed by nurses. However, long-term repetitive heavy lifting\pushing\carrying can cause increases in intra-abdominal pressure, which can lead to fatigue and damage the muscles and connective structures of the pelvic floor muscles. In this study, female nurses stated that LUTS and anorectal dysfunction increased in frequency with delayed toileting. Similarly, Wan et al. (2017) and Kaya et al. (2016) found that the prevalence of LUTS increased as delayed voiding increased at work. Recently, a cross-sectional study (Xu et al., 2016) involving 636 female Chinese nurses reported that 53.6% of participants often or always delayed emptying their bladders while working, and 67.5% of participants had at least one type of LUTS. The prevalence of fecal incontinence was 28%, although the relationship between fecal incontinence and delayed toileting was not further explored. Several studies (Palmer et al., 2012; Yüksel et al., 2014) have indicated that delayed voiding can lead to bladder hypertension and make it difficult to relax the sphincter, which is an explanation for bladder dysfunction. It is possible that delayed toileting also plays an important role in the development of anorectal dysfunction. In China, the bed-to-nursing ratio is not up to the standard because of the shortage of nurses. One nurse manages too many patients, and they usually choose to reduce water intake and toileting to take care of their patients. As a part of their unique culture, the Chinese often use old-fashioned squat toilets. In recent years, most hospitals have been equipped with Western-style toilets, but most nurses have reduced or avoided toileting because the number of these toilets is limited and they consider them unsanitary. Chinese nurses face severe workplace conditions, and they may experience repetitive or progressive damage to the pelvic floor over time if the workplace conditions do not improve.
In this study, we also found that the prevalence of LUTS increases with increase fluid intake. Similar to the findings of other research (Liao et al., 2009), we found a high level of reduced fluid intake among the nurses. However, the correlation between the prevalence of LUTS and fluid intake is contrary to some previous studies (Cotterill et al., 2018; Higa & Lopes, 2007; Liao et al., 2009), which suggests that the prevalence of LUTS increases with increased fluid intake. This interesting result may be related to the fact that the nurses could not go to the toilet in a timely manner after drinking fluids, which results in increased intra-abdominal pressure and damage to the pelvic floor muscles. In response to this phenomenon, further studies are needed.
Although the conditions of PFD do not carry a serious risk to life, women who experience PFD usually report that the condition has a negative impact on their QoL. In this study, the findings demonstrated that PFD had a significantly negative influence on overall QoL among the nurses. Similarly, a systematic review (Pierce et al., 2016) reported that participating female nurses experiencing PFD had lower QoL scores than those without symptoms, although the instruments (the Medical Outcomes Study-Short Form 36, SF-36; the Incontinence Quality of Life Questionnaire, I-QOL) (Araki et al., 2005; Liao et al., 2009; Yağmur & Ulukoca, 2010) used to evaluate QoL were different. A previous study (Matthews et al., 2013) reported that women who experience PFD tend to suffer from anxiety and depression. Characteristically, Chinese women are more conservative, and women with PFD do not actively seek treatment or help, which may result in aggravated symptoms. Long-term physical discomfort can lead to a decreased ability to concentrate on work, perform physical tasks, or complete tasks without interruption (Fultz et al., 2005). Irwin et al. (2006) and Kannan et al. (2009) reported that women with LUTS were shown to have decreased work productivity and were more likely to be unemployed. The conditions of female nurses with PFD not only influence their work efficiency but also may lead to low quality of care for patients and reduce patient satisfaction.
There are several limitations to this study. First, we recruited participants and collected data through online platforms, and the self-reported measures might have resulted in common-method variance and social desirability bias. Second, due to the constraints of time and human resources, this study only selected female nurses from six tertiary hospitals in Nanjing. In the future, we will adopt more complicated sampling methods, enlarge the sample size, and increase the diversity of female nurses’ coverage in different levels of hospitals and departments to obtain more comprehensive data and further confirm or amend our research conclusions. Third, due to inconvenient measurements and inconsistent infrastructure among hospitals, this study only explores some workplace conditions, and the variables we chose contribute only a partial explanation of the results. In the future, quantitative research should be combined with qualitative research to comprehensively and deeply explore the relationship between the conditions of female nurses’ PFD and workplace environments.
Implications for Occupational Health Nursing Practice
This study found a high prevalence of PFD among female nurses and that workplace conditions play an important role in nurses’ pelvic floor health, suggesting that nurses, as an important part of providing healthcare services, are an underserved group. Occupational health leaders need to pay more attention to nurses’ health. Hospital management is directly responsible for the protection of the health of nurses in the workplace. The department needs to recruit enough nurses so that the hospital can provide a sufficient number of nurses to meet the standard bed-to-nurse ratio. It is common for nurses to transfer patients and heavy objects. Therefore, it is necessary to configure transfer facilities and use automated equipment to reduce the unnecessary physical labor of nurses. A hygienic and comfortable ward environment should be a basic guarantee for nursing work, especially the provision of convenient tea and water services, sufficient and hygienic toilets, and a relaxed work environment. For government health management departments, strengthening the publicity of pelvic floor health knowledge, and raising people’s awareness of pelvic floor health should include pelvic floor health examinations in annual routine physical examinations of female employees and a reasonable ratio of beds to nurses to reduce nurses’ work pressure. Our findings provide initial insights into the workplace conditions that could be jeopardizing pelvic floor health among female nurses.
Conclusion
Our study was the first to comprehensively investigate the prevalence of LUTS, POP, and anorectal dysfunction and explore the associations between work-related factors and these conditions among female Chinese nurses. We found that the level of PFD among these nurses was significantly higher than that reported in the general populations, and workplace conditions play an important role in their pelvic floor health. Our data indicated that in terms of work-related factors, PFD has a significant association with heavy lifting\pushing\carrying at work, delayed toileting at work and fluid intake among female nurses. Nurses with PFD reported decreased overall QoL. Future studies, in other countries or regions should explore the relationship between workplace conditions and nurses’ pelvic floor health.
Applying Research to Occupational Health Practice
Our study found the level of PFD among female nurses was significantly higher than that of the general populations in China, and workplace conditions play an important role in pelvic floor health. Occupational health providers should pay/give attention to nurses’ health and create convenient and comfortable workplace environments, especially with a reasonable bed-to-care ratio and infrastructure configuration. Female nurses are an important group to provide healthcare services. Government health management departments, as the makers of healthcare policies and regulations, should not ignore female nurses’ health problems. Strengthening the publicity of pelvic floor health knowledge and formulating reasonable policies that are beneficial to the occupational health of nurses are the basis for ensuring the health of female nurses.
Footnotes
Acknowledgements
The authors would like to thank all participants and researchers for their great contribution to this study.
Author Contributions
Concept and design: Rumeng Chen, Ya Zhu. Acquisition of the data: Rumeng Chen, Ya Zhu, Xirong Cheng, Chao Jin, Chunxia Zhang, Shenshen Wang. Analysis and interpretation of the data: Rumeng Chen, Lixia Chen, Yue Su. Drafting of the manuscript: Rumeng Chen. Critical revision of the manuscript: Ya Zhu, Xirong Cheng.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The study was approved by the Committee on the Ethics of Medical Research of the Second Affiliated Hospital of Nanjing University of Chinese Medicine (2021SEZ-027-01).