
Abstract
Background:
Healthcare workers report a higher incidence of depression than the general population. Work–family conflict is a risk factor, but the mechanisms explaining its association with depression are not well understood. This study examines the potential mediating and moderating role of sleep and decision latitude in translating work–family conflict into depression.
Methods:
In 2018, a cross-sectional survey was collected from healthcare workers (n = 1,059) in five public sector facilities in the northeast United States. The survey included questions on participants’ work–family conflict, depression, sleep duration and disturbances, decision latitude, and other work environments and socio-demographic characteristics. Multivariable linear and Poisson regression modeling were used to examine associations among variables.
Findings:
There was a significant association between work–family conflict and depression (β = 2.70, p < .001). Sleep disturbances, although not short sleep duration, partially mediated this association. The association between work family–conflict and depression was stronger among workers with low decision latitude.
Conclusions:
Depression was prevalent among healthcare workers and was associated with work–family conflict. Sleep disturbances served as a significant mediator, while decision latitude modified the strength of the association.
Application to Practice:
Evidence-based interventions seeking to alleviate the effect of work–family conflict and improve healthcare workers’ mental health should consider promoting employee sleep quality and improving employees’ decision-making on the job.
Background
Depression is attributed to a complex interaction of genetics, socio-environmental and psychological factors, contributing to an overall global burden of chronic disease and disability (World Health Organization, 2021). It is one of the most common mental disorders in the United States; 21.0 million adults in the United States were estimated to have at least one major depressive episode in 2020, representing 8.4% of all U.S. adults (National Institute of Mental Health, 2022). This prevalence was notably higher among women (10.5%) than men (6.2%) (National Institute of Mental Health, 2022).
Healthcare is one of the largest and fastest-growing sectors in the United States, employing 22 million workers, or 14% of the U.S. workforce (U.S. Census Bureau, 2019). The healthcare work environment imposes multiple physical and psychosocial work stressors on employees, including shift work and long work hours, excessive physical load, time pressure, chemical and biological hazards, and bullying and violence (Mohanty et al., 2019; National Institute for Occupational Safety and Health, 2022; Occupational Safety and Health Administration, 2022). Healthcare workers have experienced poor physical and mental health such as shortened and poor sleep, musculoskeletal pain, metabolic syndrome and cardiovascular diseases, and substance misuse (Mohanty et al., 2019; Weaver et al., 2018). In addition, healthcare workers report a higher rate of depressive symptoms than the general population (Khamisa et al., 2015; Weaver et al., 2018).
Work–family conflict occurs when a worker experiences incompatible demands between work and family roles in two directions, from work to family and/or from family to work (Greenhaus & Beutell, 1985). Work–family conflict has been frequently reported in healthcare workers and affects employees’ work and health, both physical and mental (Gisler et al., 2018; Minnotte & Yucel, 2018; Zhang, Punnett, & Nannini, 2017). Previous studies have linked work–family conflict to depression in nurses and nursing assistants (Zhang, Duffy, & De Castillero, 2017; Zhang, Punnett, & Nannini, 2017) and in other healthcare workers (Guille et al., 2017). Besides depression, work–family conflict has been associated with healthcare worker burnout and intention to leave the job (Blanco-Donoso et al., 2021; Chen et al., 2018; Kocalevent et al., 2020).
Although the association between work–family conflict and depression has been studied, the mechanisms explaining this relationship have not been well understood. In this study, we explore two modifiable factors, sleep and decision latitude (a worker’s ability to influence what happens in the work environment), as potential buffers of this association. The factors were selected for their potential to be changed within the workforce and the workplace. Low decision latitude has been reported as a significant psychosocial work stressor causing unhealthy behaviors and outcomes (Punnett et al., 2009). Specifically, improving sleep at the individual level and increasing decision latitude at the institutional level are feasible and acceptable points of intervention (Dugan & Punnett, 2017).
Sleep, both quantity and quality, plays a critical role in mental health (Magnavita & Garbarino, 2017). Healthcare workers are at risk for short and disturbed sleep (Hulsegge et al., 2019; Zhang et al., 2021). Sleep deficiency, in terms of short sleep duration and sleep disturbances, was reported as a potential consequence of work–family conflict in healthcare workers (Jacobsen et al., 2014). In turn, short sleep duration and poor sleep quality both contribute to depression (Zhai et al., 2015; Zhang, Duffy, & De Castillero, 2017). Therefore, it is plausible that sleep could play a role in the relationship between work–family conflict and depression, and one previous study reported that sleep disturbances mediated this relationship (Zhang, Duffy, & De Castillero, 2017).
Low decision latitude at work, a key dimension of work stress, contributes to mental disorders such as anxiety and depression (Too et al., 2020) as well as poor self-rated health (Cho et al., 2018). Low decision latitude has been correlated with work–family conflict (Zhang, Duffy, & De Castillero, 2017) and is a potential mediator between job demands and mental strain (Ogunyemi et al., 2019), as well as between long working hours and self-rated health (Cho et al., 2018). However, its potential contribution to the relationship between work–family conflict and depression has not been studied and warrants further examination.
The objectives of this study were therefore (a) to examine the association between work–family conflict and depression among healthcare workers; and (b) to explore the mediating or moderating role of sleep (both quantity and quality) and decision latitude in the relationship between work–family conflict and depression among these workers.
Method
Setting and Subjects
Healthcare workers were invited to participate in a research study from five public sector facilities in the northeastern United States, two mental health hospitals and three veterans’ facilities (Punnett et al., 2020). All facilities were managed by the State or Federal government and all workforces were unionized. This analysis is part of a larger research project, using the baseline survey data collected from a sample of 1,059 healthcare workers from January to June 2018. All full-time, part-time, and per-diem employees over 18 years old and hired directly by these facilities were eligible to participate.
Measurements
Dependent Variable
Independent Variable
Potential Mediators and Moderators
Covariates
Physical demands (five items), psychological demands (two items), and social support (four items) were selected from the subscales of the JCQ (Karasek et al., 1998) and assessed with a 4-point Likert-type scale. The JCQ subscales demonstrated good validity and acceptable reliability in large study populations from six countries (Karasek et al., 1998). The Cronbach’s alpha coefficients of these subscales were good at 0.88 (physical demands), 0.61 (psychological demands), and 0.75 (social support) in this study sample, similar to the values reported in a previous study of nursing assistants (Zhang et al., 2016).
Schedule control was measured with two items selected from the Center for the Promotion of Health in the New England Workplace All Employee Survey (CPH-NEW AES; Center for the Promotion of Health in the New England Workplace, 2020). The scale demonstrated very good reliability for this study sample (Cronbach’s α = 0.87). Emotional labor was assessed with three items on surface-acting emotional labor selected from Brotheridge and Grandey (2002), also with very good reliability (Cronbach’s α = 0.85). Job hazards was assessed with one item written by the research team and three items selected from (Silver & Boiano, 2019). This scale had a Cronbach’s alpha value of 0.59. Participants’ perceived safety on their current job in the facility was measured with seven items selected from the CPH-NEW AES. The scale demonstrated very good reliability for this study sample (Cronbach’s α = 0.86). Organizational support for safety was measured with eight items from the Nordic Occupational Safety Climate Questionnaire (Kines et al., 2011). The scale had a Cronbach’s alpha value of 0.65 in this sample.
Negative behaviors at work were assessed with six items from the Negative Acts Questionnaire-Revised, which covers being humiliated or ridiculed, ignored or shunned, insulted, shouted at or targeted, intimidated with threatening behaviors, or being the subject of excessive teasing and sarcasm in the past 6 months (Einarsen et al., 2009). This variable was dichotomized as yes (any) or no (none) for these analyses.
Data Collection
The research team distributed and collected the questionnaires at each facility over a 2 to 5-day period to accommodate employees working at different shifts and units. The team members explained the study purpose and procedure, potential benefits and risks, and protection of confidentiality to participants. Employees were given the option to take home the questionnaires to complete in private. Compensation of US$10 was offered for each completed questionnaire with a consent form. The study was approved by the University of Massachusetts Lowell Institutional Review Board (Number 16-131-PUN-XPD).
Data Analysis
The SPSS software 26.0 was used to complete all statistical analyses. Work–family conflict and depression were treated as continuous, while sleep duration, sleep disturbances, and decision latitude were dichotomized. The associations of socio-demographics and working conditions with work–family conflict and depression were examined using independent samples t-test (for means of two independent groups), ANOVA (means of three or more independent groups), and Spearman correlation coefficients (for variables that are not continuous or not normally distributed) (Field, 2013).
Multivariable linear regression modeling was used to calculate coefficients and 95% confidence intervals (CI) for depression (continuous). The prevalence of sleep disturbances, short sleep duration and low decision latitude were all over 10%, so Poisson regression modeling with robust variance estimates was used to calculate prevalence ratios (PR) and 95% CI as more conservative and accurate than logistic regression modeling (Barros & Hirakata, 2003). Multicollinearity assumptions were checked using variance inflation factors (VIF) to quantify how much the variance is inflated in the multivariable linear regression models (Field, 2013). Socio-demographics and working conditions were adjusted as covariates in the multivariable regression models if they were significantly associated with either work–family conflict or depression at the bivariate level.
Baron and Kenny’s (1986) method was used to assess potential mediating effects on the association between work–family conflict and depression by evaluating: (a) work–family conflict association with depression; (b) work–family conflict association with sleep disturbances (or sleep duration or decision latitude); (c) sleep disturbances (or sleep duration or decision latitude) association with depression; and (d) attenuation of the association between work–family conflict and depression with inclusion of sleep disturbances (or sleep duration or decision latitude).
To assess the potential moderating effect of sleep disturbances, sleep duration or decision latitude, an interaction term for each variable with work–family conflict was introduced into the multivariable linear regression models separately after the main effects.
Results
Descriptive Analyses
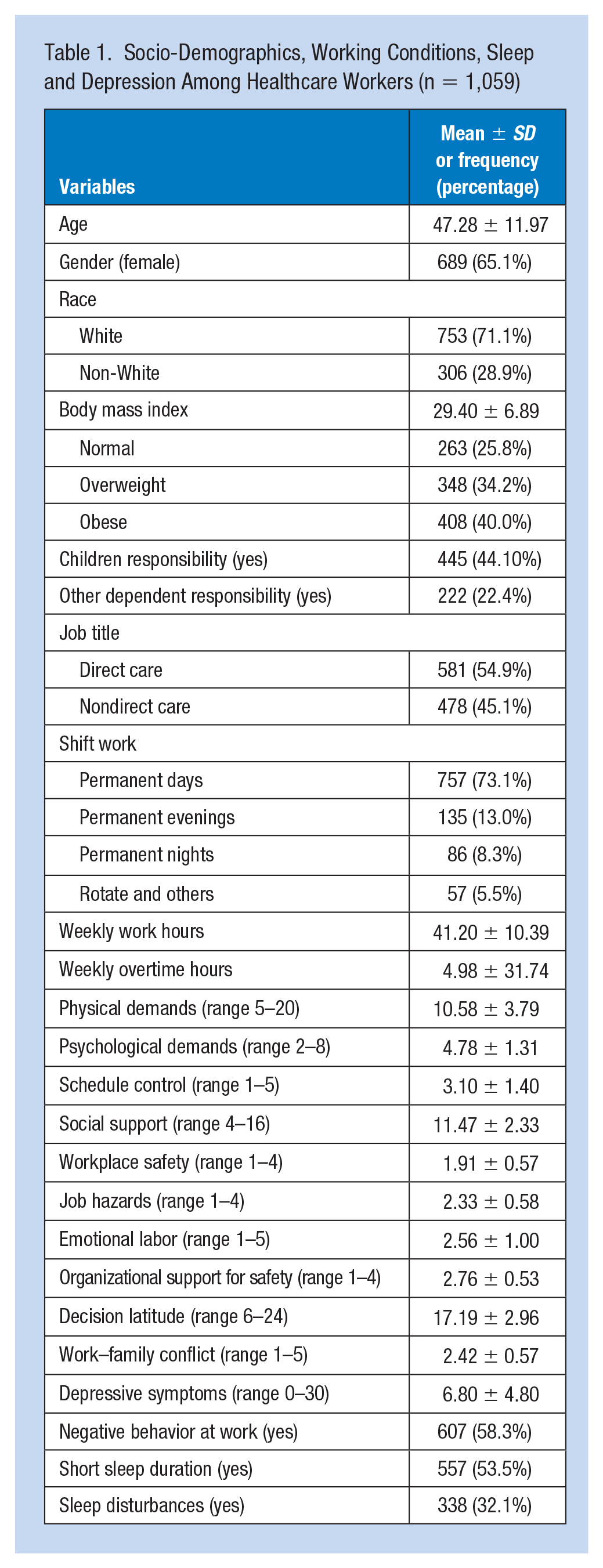
A total of 1,059 healthcare workers completed the survey (response rate of 38%), with an average age of 47 years (Table 1). Over one half were involved in direct care, three fourths were overweight or obese, and about one fourth routinely worked evenings, nights or rotating shifts. Nearly one half reported responsibility for children at home and nearly one quarter had responsibility for other dependents. Depression (CES-D ≥ 10) was experienced by 22%. Both short sleep duration (53.5%) and sleep disturbances (32.1%) were relatively common.
Socio-Demographics, Working Conditions, Sleep and Depression Among Healthcare Workers (n = 1,059)
Bivariate Analyses
Work–family conflict, the primary independent variable, was positively associated with symptoms of depression, short sleep duration and sleep disturbances (p < .01 for all three). Employees reported higher work–family conflict scores when they also experienced lower decision latitude as well as ten other demands and stressors at work shown in Table 1 (all p values < 0.01). These variables were all subsequently included in multivariable modeling. Younger, White, and direct care workers reported higher work–family conflict scores than older, non-White, and nondirect care ones, as did those with children or other dependent responsibilities (all p values < 0.05).
Depression was further positively associated with short sleep duration and sleep disturbances (p < .01 for both). Depression scores were also higher among employees reporting lower decision latitude (p < .01) as well as the same other demands and stressors at work. Younger and White workers reported higher depression scores than older and non-White ones (all p values < 0.01).
Besides higher work–family conflict, direct care workers reported higher decision latitude but more weekly overtime hours, higher physical demands, more job hazards, lower workplace safety and organizational support for safety, more negative behaviors at work and higher prevalence of short sleep duration (all p values < 0.05).
Multivariate Analyses
Multivariable linear regression model of work–family conflict and depression was built (Table 2). VIF ranged from 1.10 to 1.97, indicating nonmulticollinerity. There was a significant association between work–family conflict and depression. With every unit increase of the work–family conflict score, the depression score increased by 2.70 units (Table 2, Model 1).
Multivariate Linear and Poisson Regression Models for Work–Family Conflict, Sleep, and Depression Among 1,059 Healthcare Workers
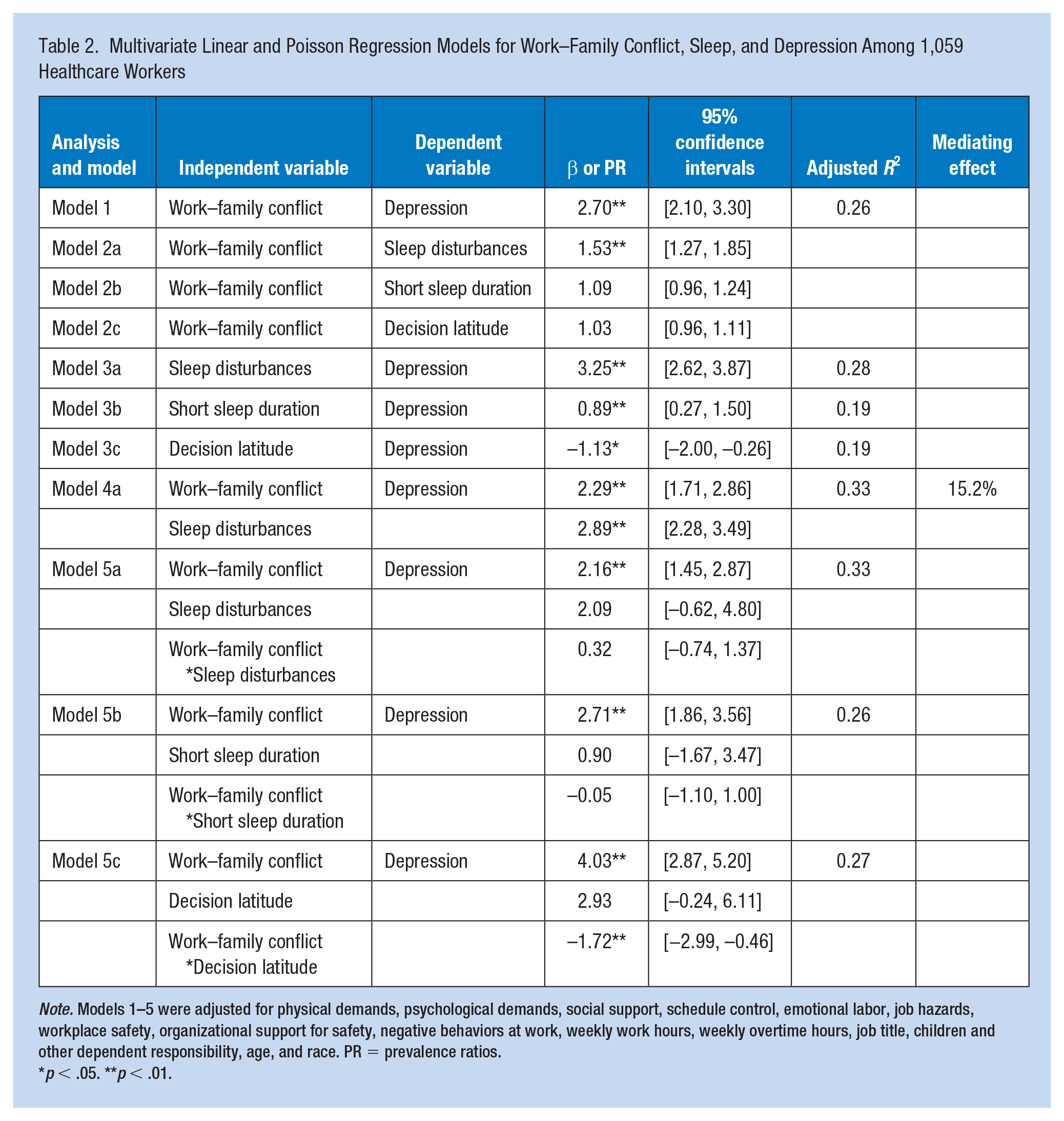
Note. Models 1–5 were adjusted for physical demands, psychological demands, social support, schedule control, emotional labor, job hazards, workplace safety, organizational support for safety, negative behaviors at work, weekly work hours, weekly overtime hours, job title, children and other dependent responsibility, age, and race. PR = prevalence ratios.
p < .05. **p < .01.
In the multivariable Poisson and linear regression models, there were statistically significant associations between work–family conflict and sleep disturbances (Table 2, Model 2a), and between sleep disturbances and depression (Model 3a), after adjustment for covariates (Table 2). After introducing sleep disturbances into the model (Model 4a), work–family conflict retained its association with depression; sleep disturbances were associated with depression; and the correlation coefficient between work–family conflict and depression reduced from 2.70 (Model 1) to 2.29 (Model 4a), suggesting that 15.2% of this association was mediated by sleep disturbances (Figure 1).
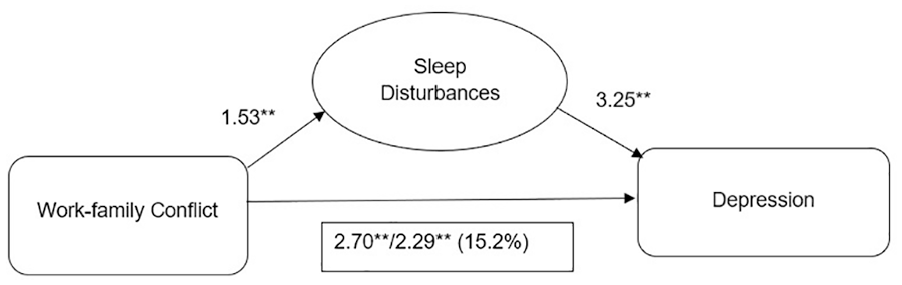
Occurrence of Sleep Disturbances Mediate the Association Between Work–Family Conflict and Depression
Although the associations of short sleep duration or decision latitude with depression were significant (Table 2, Model 3b/3c), neither the association between short sleep duration and work–family conflict, nor the association between decision latitude and work–family conflict, was significant (Model 2b/2c), after adjustment for covariates. Therefore, neither short sleep duration nor decision latitude was considered as a potential mediator.
In the multivariable linear regression model with work–family conflict and depression as main effects (Table 2), the interactions between work–family conflict and sleep disturbances/short sleep duration were not significant (Model 5a/5b). However, the interaction between work–family conflict and decision latitude was significant (Model 5c, β = −1.72, p < .01).
Compared with low decision latitude, medium to high decision latitude significantly reduced the association between work–family conflict and depression (p < .01). In other words, there was a weaker association between work–family conflict and depression among workers with medium to high decision latitude than those with low decision latitude (Figure 2).
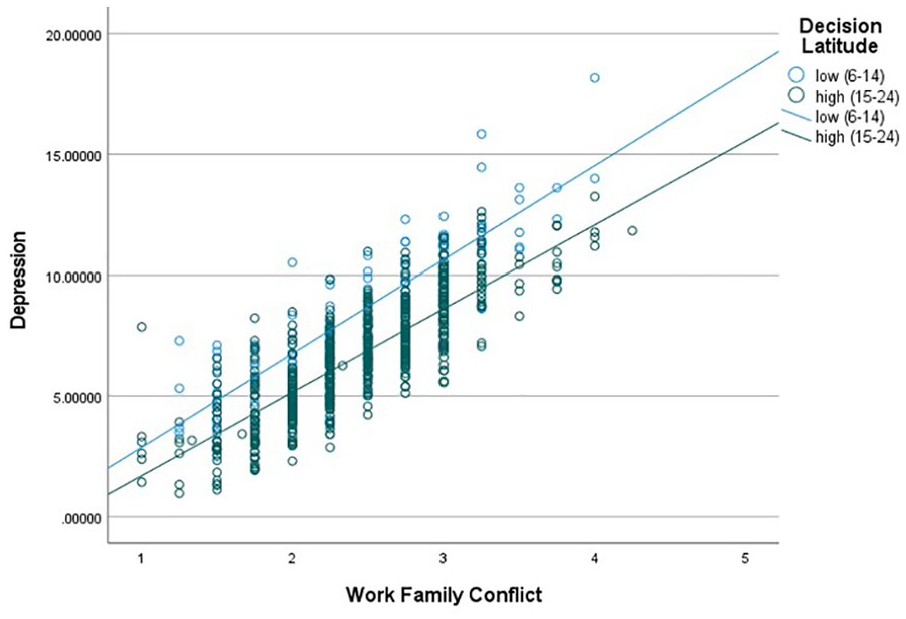
Decision Latitude Moderates the Association Between Work–Family Conflict and Depression
Discussion
Given the essential role of healthcare workers in caring for the health of the public, it is an important priority to address deficits in their mental health, especially with regard to modifiable risk factors that might affect their willingness to remain at work. This was true before 2020, and it is even more critical during the COVID-19 pandemic while healthcare workers are under extreme stress and working with insufficient resources. Preventing strain, burnout, and job dissatisfaction enables healthcare workers to better maintain their physical and mental well-being, to remain productively engaged in the workforce, and it also supports the quality of patient care delivered (Dyrbye et al., 2017; Greenberg et al., 2020; Hall et al., 2016; Thanacoody et al., 2014).
In our study of 1,059 mixed-occupation healthcare workers, nearly a quarter reported depression in the past week. This prevalence of depression is three times higher than that reported in the general U.S. population (8.4%, National Institute of Mental Health, 2022). Over one half of the study participants reported short sleep duration (≤6 hours per day) and nearly a third reported sleep disturbance. These rates were similar to those reported by a sample of hospital nurses (Zhang, Duffy, & De Castillero, 2017), even though our sample included nondirect care staff who are not typically thought of as healthcare workers.
We selected work–family conflict as the primary risk factor, a form of inter-role conflict that is highly correlated with depression (Allen et al., 2000) and was moderately high in our sample. Work–family conflict is a salient form of stress for our sample given that almost half had child care responsibilities and nearly a quarter reported other dependent care responsibilities. Not surprisingly, we found that workers with greater family demands (child and dependent care) and greater work demands (physical, psychosocial, temporal) had higher work–family conflict. Work–family conflict was positively associated with depression, as previously reported in studies of hospital nurses (Mohamed et al., 2022; Zhang, Duffy, & De Castillero, 2017) and in other occupational groups within the healthcare sector (Guille et al., 2017; Hao et al., 2015).
We examined two possible mechanisms of the association between work–family conflict and depression. There are well-established associations between work–family conflict and poor sleep health in healthcare workers (Cheng et al., 2019; Jacobsen et al., 2014). Moreover, sleep plays a significant role in mental health, and short or poor sleep is associated with depression (Diaz et al., 2022; Zhai et al., 2015).
In this study, we found that sleep disturbances were associated with both work–family conflict and depression, and that sleep disturbances partially mediated the association between these two variables. These findings were confirmed in a similar study of nurses (Zhang, Duffy, & De Castillero, 2017). We explained this using the conservation of resources theory (Hobfoll, 1989). Specifically, work–family conflict arises when competing role demands from the work and family domains vie for a person’s finite time and energy resources, resulting in experienced distress and mental health symptoms; but drained resources can decrease opportunities for stress-reducing activities including sleep (Dugan & Barnes-Farrell, 2017). Sleep is vital self-care behavior because it enables the central nervous system to recover from effort expended in daily life, and restores alertness, memory, and mood (Åkerstedt et al., 2009). Over time, insufficient recovery may result in chronic suboptimal physical and psychological states, including depression. This study contributes to a growing body of research on the implications of inter-role conflict for sleep disturbances and related adverse effects on mental health.
We also found that the association between work–family conflict and depression was stronger among workers with low decision latitude. One previous study showed that decision latitude moderated the relationship between work–family conflict and psychological strain in workers from the United States and Canada (Billing et al., 2014). As explained by both the job demand-control model (Karasek et al., 1998) and the job demands-resources model (Bakker & Demerouti, 2007), decision latitude is a resource that provides workers with a combination of skill discretion (e.g., they can choose which of their skills to use) and decision authority (e.g., they have autonomy in making decisions about work). These types of job control moderate stressor-strain relationships within the work domain. According to the job demands-resources model, job and personal resources (including control) may buffer the strain posed by the demands of both work and family life, by inhibiting the health impairment process (Bakker & Demerouti, 2007). Our findings support that such resources should be strengthened as buffers of the work–family conflict and depression relationship.
Strengths and Limitations
The strengths of this study include a large sample of mixed-occupation healthcare workers, adjustment for multiple covariates, and the ability to test for potential mediating and moderating effects of sleep and decision latitude. This study also has several limitations. The cross-sectional design of the study limits our ability to draw definitive conclusions about causal relationships. Future longitudinal studies are needed to verify the study findings. The workforce of these five public sector facilities had union representation, which may limit the generalizability of the study findings. In addition, with a survey response of 38% of all employees, there might be selection bias. Without questionnaire data from the nonrespondents, we have no way to determine if they differed from the study participants in their socio-demographic characteristics, working conditions, and/or health outcomes.
Implications for Occupational Health Nursing Practice
Occupational health nurses play a critical role in the workplaces to assess and mitigate workplace hazards and prevent and treat work-related injuries and illnesses. In light of the high prevalence of depression in this critical workforce, organizations may also consider offering confidential and supportive mental health resources such as psychological counseling and employee assistance programs (Attridge, 2019) and peer support (Agarwal et al., 2020). Sleep as a modifiable individual factor and decision latitude as a modifiable institutional factor are also both suitable targets for future workforce and workplace interventions to alleviate the adverse effect of work–family conflict and promote employee mental health.
Initiatives to address work–family conflict with the purpose of promoting work–life balance are heavily affected and shaped by cultural, economic, and institutional factors. Organizational support and resources are important to promote work–life balance (Allen et al., 2015). Leadership training and understanding of these factors, along with engaging employees, is crucial to identify and offer the resources needed to support staff work–life balance.
Sufficient sleep is important for optimum human function. Although sleep is an important self-care domain, it is greatly affected by extrinsic factors. As we have found in this study, numerous work stressors such as shift work, demands, support, hazards, negative behaviors, and emotional labor significantly affect healthcare workers’ sleep. Healthcare workers’ sleep quantity and quality could be improved at the individual level through promoting healthy sleep practices and use of nonpharmacological strategies, such as meditation, mindfulness, yoga, and other complemetary medicines (Sarris & Byrne, 2011). In addition, workplace interventions or programs are encouraged to improve employee working conditions as a critical and meaningful way to build healthy work environment, reduce work stress, improve sleep, and promote mental health and well-being of healthcare workers.
Organizations must commit to shared decision-making structures and processes that will allow increased staff participation at all levels. It is imperative that organizations offer training for both administrators (or leadership) and staff along with the support and resources needed (such as scheduling, technology, and space needed for meetings) to implement and promote such shared decision-making structures. This will allow for increased staff input, job control, autonomy, and empowerment, such as evidenced from the Magnet work environments (Graystone, 2019).
Practical strategies by the organizations to improve decision latitude in both direct care and nondirect care workers include: Encouraging workers to express opinions (e.g., having an open door policy) and guarantee no retribution; involving workers in determining work schedules, work processes, and work stations; empowering workers to propose ideas about and participate in facility changes (e.g., implementing new safety and health programs); and giving equal opportunity to nondirect care workers to serve as representatives and become involved in patient care procedures (e.g., diet and housekeeping; Punnett, 2022). For example, schedule flexibility was found to moderate the association between work–family conflict and work-related outcomes such as job satisfaction and work engagement (Yucel, 2019). Flexible work arrangements are becoming common in the emerging economy and have been associated with work–family conflict (Bayazit & Bayazit, 2017; Beigi et al., 2018). It is important to assess the feasibility of implementing such policies in the healthcare industries for the improvement of worker health and well-being.
Effective workplace intervention programs should not only address individual behavior changes but also address work features that affect health behaviors and outcomes (Punnett et al., 2009). The present results identify feasible and acceptable points of intervention at levels of both the individual (sleep) and organization (decision latitude). The above approaches for improvement would be compatible with a Total Worker Health® approach, defined by NIOSH as “policies, programs, and practices that integrate protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker well-being” (Tamers et al., 2018). Workplaces that seek to be health-promoting should consider an integrated approach to simultaneously prioritize reduction of workplace safety and health hazards while promoting health and well-being of workers.
Applying Research to Occupational Health Practice
This study provides innovative information about sleep disturbances as a partial mediator and decision latitude as a moderator in the association between work–family conflict and depression among healthcare workers. Both sleep and mental health of healthcare workers are of significance since their ability to mentally function at a high level is essential to ensure patient safety and quality of care. Findings from this study provide useful information to occupational health nurses to identify organizational risk factors associated with work–family conflict and decision latitude and to understand poor health behaviors and outcomes resulting from them. Workplaces need programs that improve healthcare workers’ decision-making power and help them balance their work and family needs. Developing such innovative policies and procedures can reduce the negative impact of work–family conflict. Furthermore, sleep promotion must also receive considerable attention in order for healthcare workers to mitigate the negative effect of work–family conflict on their mental health and well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Center for the Promotion of Health in the New England Workplace is supported by Grant Number 2 U19 OH008857 from the National Institute for Occupational Safety and Health (CDC). This work is solely the responsibility of the authors and does not necessarily represent the official views of NIOSH. We are grateful to the CPH-NEW Research Team members who collected the questionnaire data and the workers who shared their experiences with us. Total Worker Health® is a registered trademark of the U.S. Department of Health and Human Services (HHS). Participation by the University of Massachusetts Lowell does not imply endorsement by HHS, the Centers for Disease Control and Prevention, or the National Institute for Occupational Safety and Health.
IRB Protocol Number
This study was approved by the Institutional Review Boards at University of Massachusetts Lowell (Number 16-131-PUN-XPD).