
Abstract
Background:
Returning to work after childbirth is a common reason for women to stop breastfeeding. This study aimed to assess breastfeeding practices and breastfeeding support available to employed women in China, and factors affecting breastfeeding duration.
Methods:
A cross-sectional survey of 1,243 breastfeeding women employed full-time was conducted. Participants completed a sociodemographic questionnaire and the Workplace Breastfeeding Support Scale (WBSS). Multiple linear regression analysis was used to explore the factors that are associated with breastfeeding.
Results:
The mean exclusive breastfeeding duration and any breastfeeding duration of full-time employed women were 5.7 ± 0.5 months and 9.8 ± 1.5 months, respectively. The total WBSS score was 46.6 ± 5.3 (M ± SD). Generally, women perceived coworkers (M [SD] = 4.8 [1.0]) and supervisors (M [SD] = 5.7 [1.2]) to be supportive of breastfeeding. Lower scores on the WBSS were related to lack of technical and facility support, indicating no access to a refrigerator to store breast milk (M [SD] = 2.0 [1.5]) or to a breast pump (M [SD] = 1.7 [1.7]). Similarly, a private area for expressing breast milk (M [SD] = 1.4 [1.0]) was unavailable. Maternity leave, residential province, ethnicity, education level, average monthly household income, main reason for stopping exclusive breastfeeding, commute time greater than 1 hour, and the total WBSS score were also factors influencing breastfeeding duration of the full-time employed women.
Conclusions:
There were gaps in breastfeeding practices and workplace breastfeeding support of Chinese full-time employed women when compared with the World Health Organization recommendations. Occupational health providers should consider these findings when developing programs to support breastfeeding in the workplace.
Keywords
Background
Breast milk is the optimal source of nutrition for infants within 6 months after birth because it strengthens their immunity, prevents diseases, and improves intelligence while promoting health (Fang et al., 2021; Victora et al., 2016). Benefits for the mother include psychological health promotion, enhanced bonding, cost savings from not having to purchase infant formula, and lower rates of gynecological diseases (Camacho & Hussain, 2020; Victora et al., 2016).
Advocating for and supporting breastfeeding have benefits for society such as reducing employee health insurance costs and absenteeism because of better health of employees’ children, and reducing the economic burden to society from lower costs for disposing of cans, bottles, and cardboard (Rollins et al., 2016). Breastfeeding is encouraged as a natural, inherently human biological act (Morrell, 2017).
The World Health Organization (WHO) and other governmental and nongovernmental organizations have strongly advocated and invested intensively in promoting breastfeeding. One of the WHO global goals for 2025 is to increase the exclusive breastfeeding rate to more than 50% in the first 6 months (WHO, 2015). The development program for Chinese children (2011–2020) also proposed that the rate of exclusive breastfeeding for infants aged 0 to 6 months should reach more than 50% (The State Council, 2012).
A global investigation involving 194 countries indicated that only 40% of children below 6 months of age were exclusively breastfed, with only 23 countries achieving rates above 60% (United Nations International Children’s Emergency Fund [UNICEF], 2017). According to a 2019 government survey report, 29.2% of infants younger than 6 months old were exclusively breastfed in China, 33.5% were partially breastfed, and 6.3% received infant formula only (China Development Research Foundation [CDRF], 2019). Any breastfeeding was defined as feeding an infant with breastmilk (including expressed and wet nurses’ milk), plus anything else (liquids including animal milk and artificial formulas and/or foods). Only 20.8% of newborns were exclusively breastfed within 6 months of age from recent data (WHO & UNICEF, 2022), which is well below the expected goal in spite of vigorous promotion.
Women of childbearing age are an important part of the labor force and have made an important contribution to the Chinese economy. In 2019, the rate of female employment was 60.57% in China (International Labour Organization, 2021). Female employment can have many positive effects on families. For example, income from female employment can increase household spending, improve financial stability, and enhance investment in human capital, such as education (Ortiz-Ospina et al., 2018).
Maternity protection legislation exists in most countries and Chinese employed women are entitled to a 98-day paid maternity leave, with 15 days added if cesarean delivery or multiple births occurred. After returning to work, employed Chinese women are entitled to a 1-hour breastfeeding break every day in the first year postpartum (Jia et al., 2018). This policy falls short of the WHO recommendations of breastfeeding infants to 2 years of age (WHO, 2017).
Despite documented benefits and efforts, committing to breastfeeding can be challenging for mothers. Returning to work has been identified as one of the most important reasons to stop breastfeeding at age of 3 to 6 months (J. Chen et al., 2019). Most women have to face great barriers to breastfeeding at work (Rollins et al., 2016). Workplace support is crucial for continuing breastfeeding (Tomori, 2022). Use of a lactation room, breast-pumping breaks, and colleagues’ support were significant factors for continuing to breastfeed (Tsai, 2022). Mothers reported that they did not have accessible workplace lactation facilities to pump during the day (Rangel et al., 2018). Barriers to breastfeeding for employed women include the perception of breastfeeding as impeding mothers’ job performance, lack of a private room for expressing breast milk or direct breastfeeding, the neglect of colleagues and leaders, inability to find a daycare facility at or near the workplace, the high cost of daycare, and rules limiting breastfeeding in workplaces (Rangel et al., 2018; Steurer, 2017; Whipps & Honoroff, 2019).
Studies showed that breastfeeding support initiatives and having special accommodation to pump and preserve breast milk are associated with a longer breastfeeding duration (Cervera-Gasch et al., 2020; van Dellen et al., 2021). Yet, employed women in the United States reported lack of breast pumps, lactation consultants, and support groups (McCardel & Padilla, 2020). In China, a qualitative study identified influencing factors of breastfeeding practices in employed mothers, including employment benefits, commute time, workplace environment, and labor intensity (J. Chen et al., 2019). Nevertheless, an investigation of the workplace supports for breastfeeding women in China is lacking. This study aimed to investigate breastfeeding practices and breastfeeding supports available to women employed full-time in five distinct geographic areas of China, and factors affecting breastfeeding duration in this cohort.
Methods
Research Design
A cross-sectional survey was conducted of working women from December 2018 to December 2019 using a quota sampling method with the aim of recruiting a diverse sample from designated health care facilities. The study was reviewed and approved by the Research Ethics Committee of Wuhan University School of Nursing.
Setting
Participants were recruited from five distinct geographic areas of China (east, west, south, north, and central). The province served as a proxy for income and educational level.
Sample
Postpartum working women were identified through discharge records from hospitals in the five provinces. Inclusion criteria were women (a) aged 18 years and older, (b) returned to full-time work after childbirth with continuous breastfeeding, (c) having initiated continuous breastfeeding but stopped currently (the time of data collection), and (d) having healthy infants less than 2 years of age. Exclusion criteria were (a) multiple pregnancies, (b) widowed or divorced women, and (c) postpartum complications or breastfeeding contraindications. A sample size of 1,207 participants was estimated by conducting a power analysis using G-Power 3 and an effect size of 0.03 and 15 predictors for linear multiple regression modeling (Faul et al., 2007).
Measurements
The primary outcomes for the study were duration of any breastfeeding and duration of exclusive breastfeeding. These were measured by self-report based on two questions which were included in the follow-up records from community nurses (National Health Commission, 2021): How many weeks have you breastfed your most recent child? and how many weeks have you breastfed your most recent child exclusively? A researcher-designed questionnaire was used to collect information, including maternal age in years, residential province (Hubei, Guangdong, Shanghai, Jilin), ethnicity (Han nationality, minority), education level (high school, college or university, master’s degree or higher), average monthly income per person of family (3,000–5,000, 5,001–8,000, >8,000), religious affiliation, parity, delivery mode, maternity leave, employment type, main reason for stopping breastfeeding (family reason, work reason, employment reason), commute time greater than 1 hour, 1-hour breastfeeding breaks every day, exclusive breastfeeding, and breastfeeding duration. If the participant had more than one child, she was asked to answer the questionnaire based on her most recent breastfeeding experience.
To assess a mother’s perception of the support for breastfeeding in the workplace, the Workplace Breastfeeding Support Scale (WBSS) was used (Bai et al., 2008). The scale includes 12 items with four dimensions (technical support, environmental support, facility support and peer support). The scale uses a 7-point Likert-type scale (1 = strongly disagree to 7 = strongly agree), where 1 is the lowest and 7 is the highest score. Given a total score ranging from 12 to 84, higher scores indicate a higher perception of breastfeeding support in the workplace. The measure showed acceptable reliability (Cronbach’s α = .77, r = .86; Bai et al., 2008).
After authorization was obtained, researchers translated the WBSS into Chinese and back translated the scale. Then, the scale was sent to 10 experts in the field of breastfeeding to assess content validity. Later, cognitive interviews involving 30 mothers returning to work were conducted to adjust and revise the scale. Finally, a pilot study involving 120 mothers in a hospital in Hubei province was conducted to assess reliability and content validity. Statistical Program for Social Sciences (SPSS, version22.0) was used to analyze data. The Cronbach’s alpha of the scale is .756 and the content validity index is 0.892. All items and structures of the original scale were retained and a 12-item scale was included. The Chinese version of the WBSS was used in the study.
Data Collection
Research assistants collecting data were provided with 2 days of training prior to initiating the survey. Participants were recruited from community health service centers and pediatric out-patient units of comprehensive large hospitals in five different provinces. When eligible women brought their sick children to the hospital or they brought their healthy children to get vaccinated, they were approached and invited to participate. After obtaining informed consent, participants were asked to answer the questions regarding breastfeeding duration and to complete the paper-based questionnaires (sociodemographic questionnaire and the WBSS) independently. Participants were offered free access to an educational video on growth and development of children after completing the questionnaire. To protect participants’ anonymity, only the research team had access to the questionnaires that were stored in a secure location. A flow diagram of data collection is shown in Figure 1.
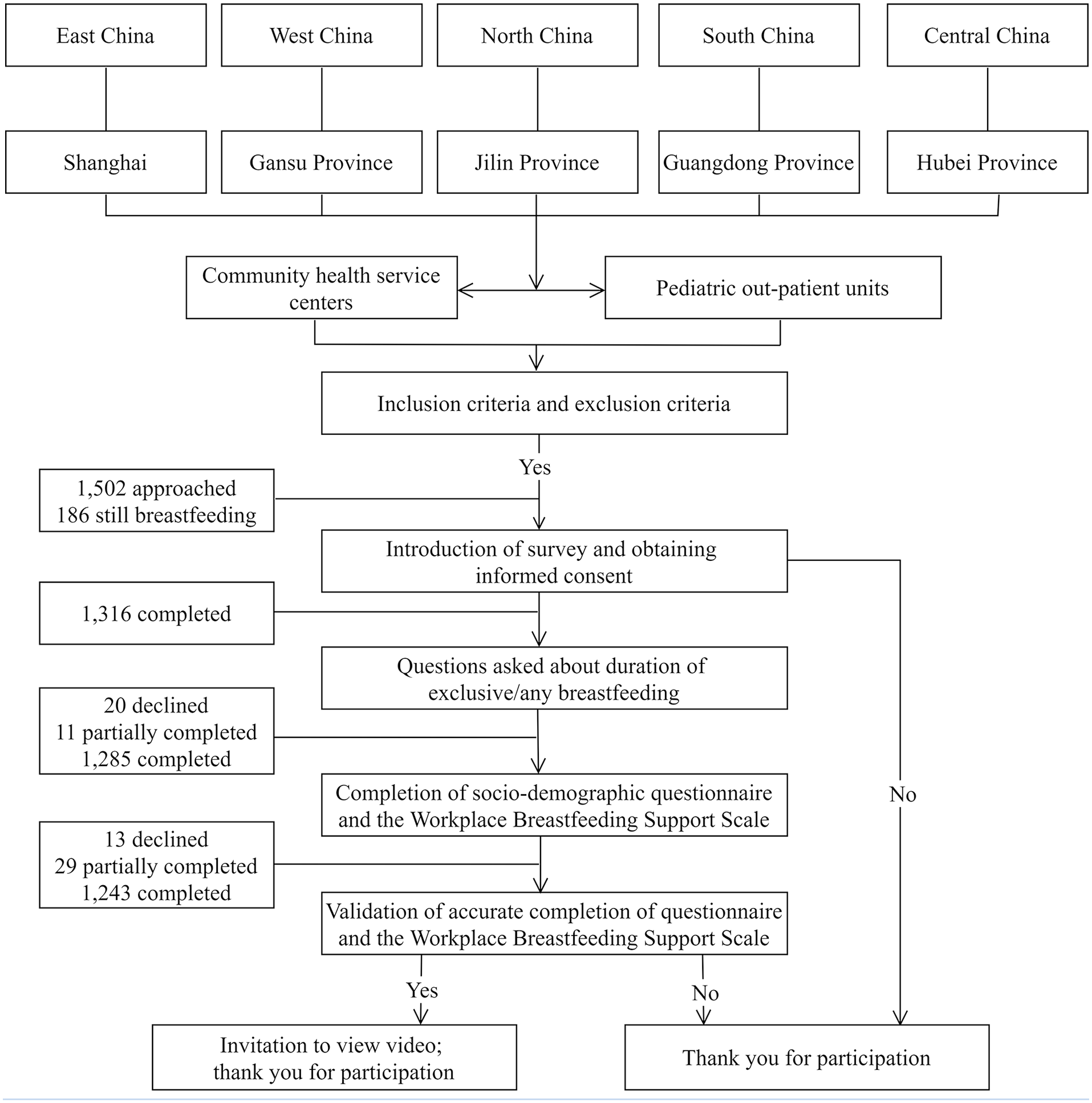
Flow diagram of data collection.
Data Analysis
Data were entered in the Statistical Program for Social Sciences (SPSS, version 22.0). For the WBSS, the total score is calculated by adding the scores of each item (Bai et al., 2008). Demographic data and responses to the WBSS were described using descriptive statistics (means, standard deviations, frequencies, and proportions). In the single-factor analysis, the dichotomous variables were analyzed by independent-sample t test; the polytomous variables with homogeneity of variance were analyzed by one-way analysis of variance (ANOVA); and the polytomous variables with heterogeneity of variance were analyzed by the Kruskal–Wallis H test. Pearson’s correlation was used to present the correlation between the factors. Multiple linear regression analysis was used to explore the factors influencing breastfeeding duration. Statistically significant predictors in the univariate analysis were entered into a multiple linear regression model. All assumptions of linear regression should be met. A p value of less than .05 was considered statistically significant.
Results
Sociodemographic Characteristics
Details of sociodemographic characteristics are shown in Supplemental Table 1. A total of 1,502 women were approached and 1,243 participants completed and returned the questionnaire, yielding a response rate of 82.8%. Participants had an average age of 26.2 ± 3.2 years and the average length of maternity leave was 5.3 ± 0.8 months. The majority were of Han ethnicity (87.6%) and primiparas (82.3%). The mean exclusive breastfeeding duration was 5.7 ± 0.5 months and the mean any breastfeeding duration was 9.8 ± 1.5 months. The exclusive breastfeeding rate at 6 months was 68.8%. The overall any breastfeeding duration ranged from 6 to 16 months. The any breastfeeding duration of full-time employed mothers and their sociodemographic characteristics varied and the results of single-factor analysis for each characteristic are shown in Table 1. According to univariate analysis, these factors were found to significantly influence breastfeeding duration in the cohort: residential province (p < .001), ethnicity (p < .001), education level (p < .001), average monthly household income (p = .01), religious affiliation (p = .003), maternity leave (p < .001), main reason for stopping breastfeeding (p = .01), commute time greater than 1 hour (p < .001) and the total score of the WBSS (p < .001).
Univariate Analysis of Sociodemographic Characteristics and Breastfeeding Duration (n = 1,243)
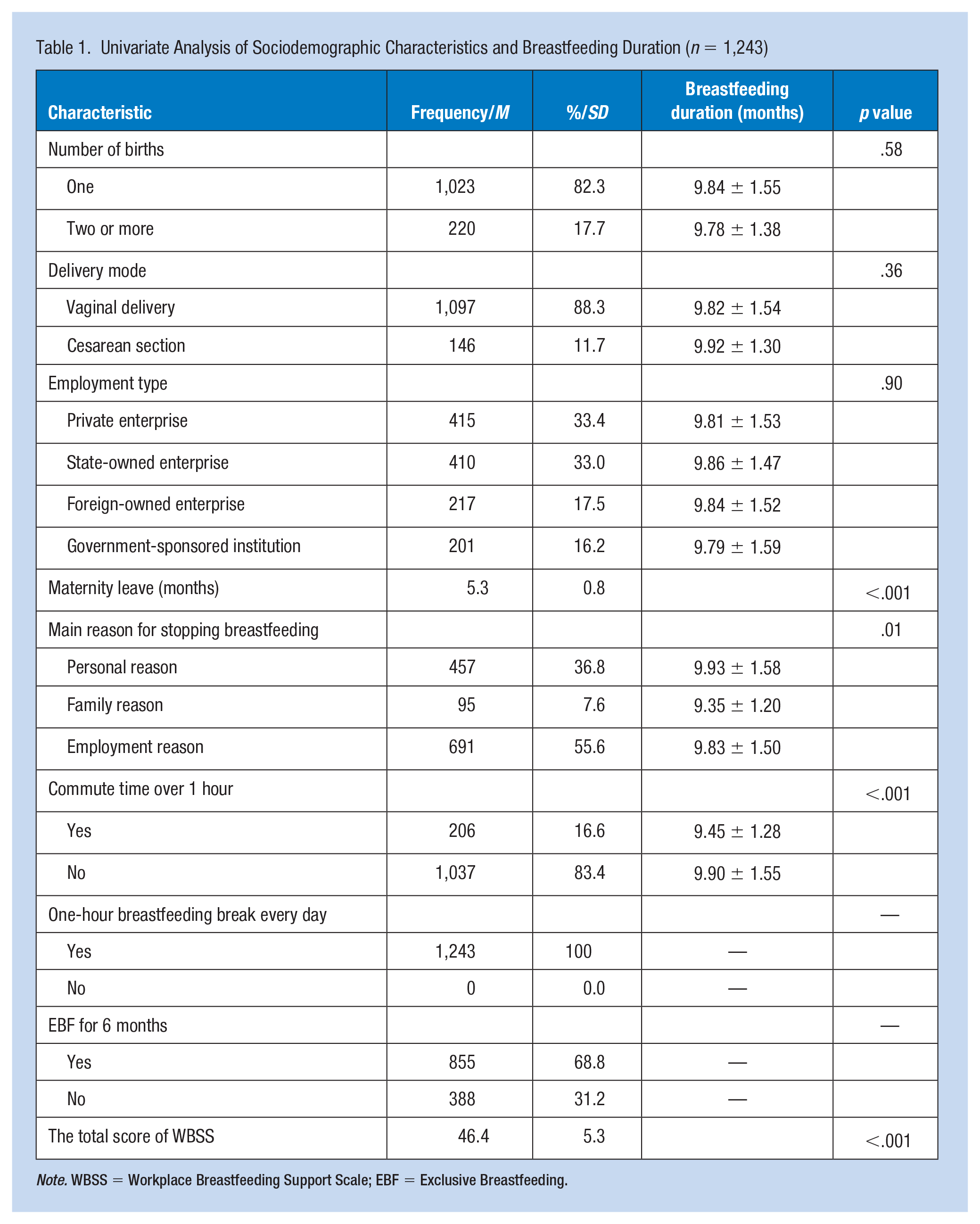
Note. WBSS = Workplace Breastfeeding Support Scale; EBF = Exclusive Breastfeeding.
Breastfeeding Support in the Workplace
The total score of the WBSS was 46.6 ± 5.3. It was found that mothers who were breastfeeding received much compassionate support from co-workers such as agreement that “breastfeeding is better” (M [SD] =6.8 ± 0.6) and “listen to my breastfeeding experience” (M [SD] = 6.0 ± 1.0). Overall, women reported that their workplaces did not offer sufficient on-site facility resources such as a refrigerator (M [SD] = 2.0 ± 1.5) or a private area for breastfeeding (M [SD] = 1.4 ± 1.1) (Table 2).
Scores of Workplace Breastfeeding Support Scale (n = 1,243)
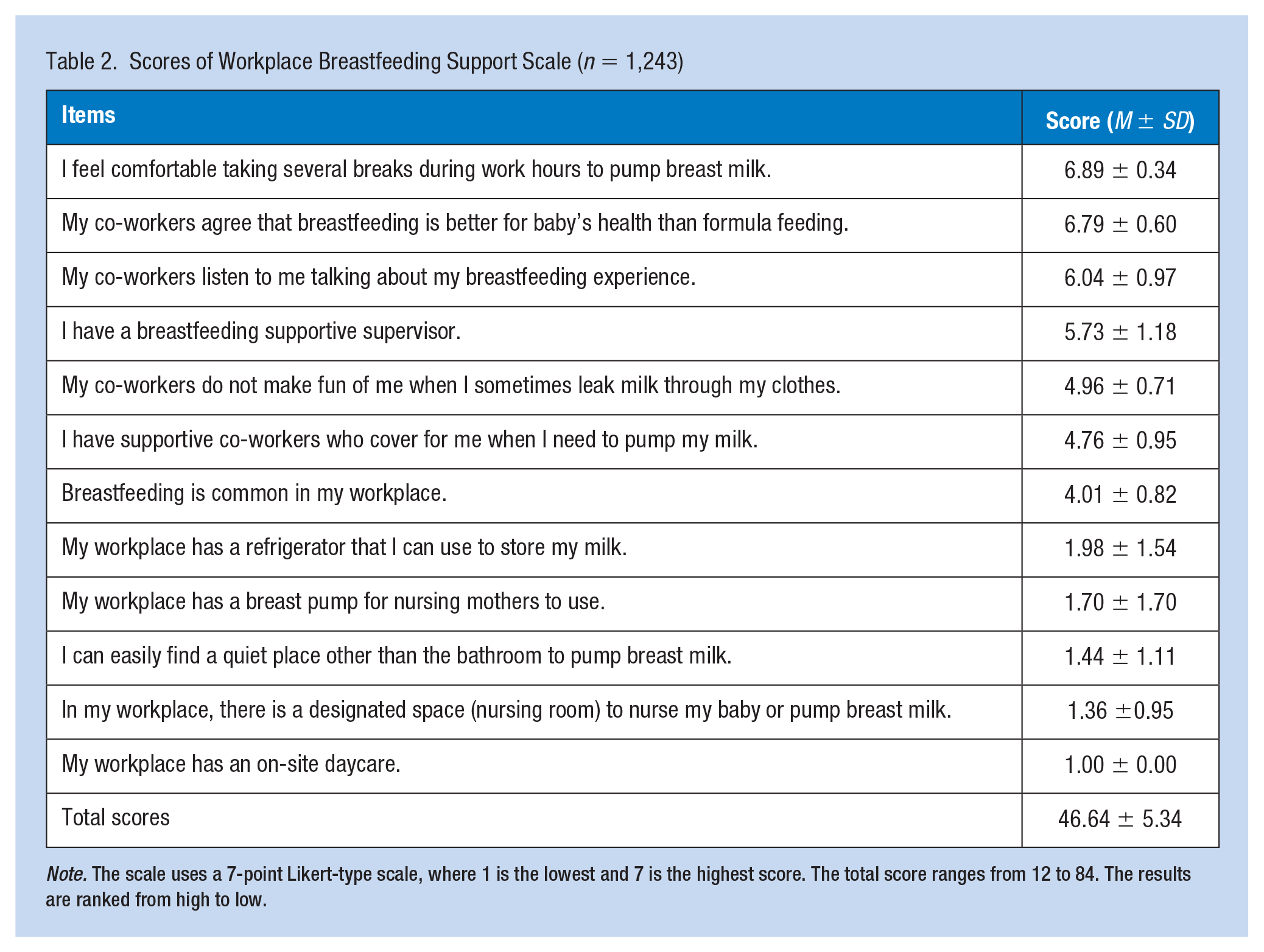
Note. The scale uses a 7-point Likert-type scale, where 1 is the lowest and 7 is the highest score. The total score ranges from 12 to 84. The results are ranked from high to low.
Factors Associated With Any Breastfeeding Duration
The influencing factors on any breastfeeding duration of full-time employed mothers are shown in Table 3. In the multivariable model, religion was considered as no longer related to any breastfeeding duration. Residing in Shanghai (p = .027), being of Han nationality (p = .017), holding a master’s degree or higher (p < .001), having middle-level household income (p = .044), having long maternity leave (p < .001), personal reason for stopping breastfeeding (p = .001), having a commute time to work of less than 1 hour (p < .001), and a high WBSS score (p < .001) were the factors positively influencing breastfeeding duration among full-time employed women.
Results of Multiple Linear Regression Analysis on Influencing Factors of Any Breastfeeding Duration
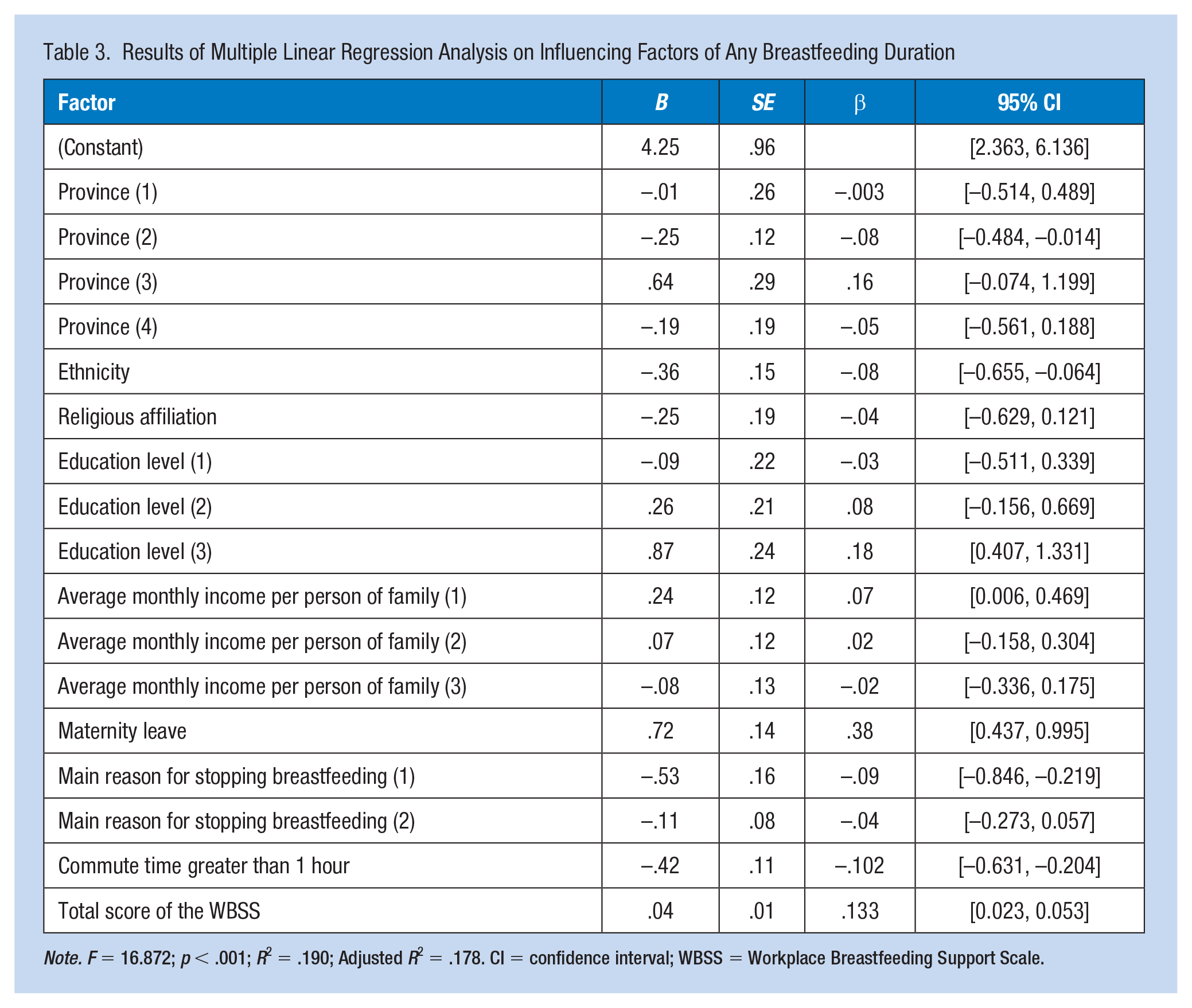
Note. F = 16.872; p < .001; R2 = .190; Adjusted R2 = .178. CI = confidence interval; WBSS = Workplace Breastfeeding Support Scale.
Discussion
The mean exclusive breastfeeding duration was 5.7 ± 0.5 months and the mean any breastfeeding duration was 9.8 ± 1.5 months in this study, which was longer than that in South Africa (Somé et al., 2017). The difference in national economic development level may account for this difference. Nevertheless, this did not meet the recommended length of breastfeeding according to the WHO: exclusive breastfeeding up to 6 months and continue breastfeeding for 2 years (WHO, 2017). There is still a long way to achieve the goal, especially when it comes to strengthening workplace breastfeeding support.
The exclusive breastfeeding rate at 6 months was significantly higher than that in other studies. Another study about Chinese employed women showed that the exclusive breastfeeding rate at 6 months was 15.38% (J. Chen et al., 2019). There were various possible reasons for this difference. The release of the “Breastfeeding Promotion Strategy Guidelines” in 2018 may account for this (Chinese Medical Association, 2018): Women may have enhanced knowledge and stronger beliefs about breastfeeding than before. Sample selection bias may be another explanation.
The total score of the WBSS in the current study was 46.0 ± 5.34. This indicated that mothers perceived lack of breastfeeding support in the workplace. Support from the workplace is necessary to promote exclusive breastfeeding (Jantzer et al., 2018; Leon-Larios et al., 2019; Martin et al., 2015). In a study investigating active-duty military mothers’ breastfeeding support, the overall average WBSS score was 50.2 (SD = 15.8; Martin et al., 2015), which was slightly higher than the results in the current study. The reason for this may be that the U.S. Department of Defense was able to improve breastfeeding rates for mothers by implementing and adhering to lactation policies (Martin et al., 2015).
Women perceived great coworker and supervisor support in this study and the scores were slightly higher than that in a Spanish study (Leon-Larios et al., 2019). Another study identified break times and coworker support as positive elements among the factors that influence lactation maintenance (Jantzer et al., 2018). This indicates that increased breastfeeding duration may be achieved by realigning breastfeeding policy and coworker attitudes toward breastfeeding.
However, having supportive policies in workplace may still not be enough to sustain breastfeeding among working mothers. In the current study, women did not have access to a breast pump or refrigerator to store their breast milk. Similarly, a nursing room to express milk was indicated as lacking as well as an on-site daycare. These results are in line with a previous study (Leon-Larios et al., 2019). One study indicated that the lack of space for expressing breast milk was the primary obstacle at their workplace, despite policies in place that required nursing mothers having time and a place to express (Martin et al., 2015). Researchers found that women with private space and breast pumps in the workplace were more likely to continue breastfeeding (McCardel & Padilla, 2020). Accordingly, facility support for breastfeeding women at work (such as rooms for milk expression, tools to pump and store breast milk) should be provided to promote expressing breast milk and breastfeeding.
With respect to the influencing factors, the current study showed differences in breastfeeding duration of full-time employed mothers among provinces, especially Guangdong Province representing the South of China, and Shanghai representing the East of China. This may be due to different economic development levels across study sites (Li et al., 2020). Due to recent economic reform, an extensive economic model of development has been occurring in China. Guangdong Province and Shanghai have been beneficiaries. The sociodemographic differences between these five sites may be another reason. Guangdong Province and Shanghai have a large population of young people (Kuang et al., 2020), and their intentions and acceptance of policies are at high level. Colleagues may also be more receptive and supportive of breastfeeding in the workplace.
The ethnic affiliation of women was found to influence breastfeeding duration. A similar finding has been reported in Fryer et al.’s (2018) study. The influence of ethnicity on breastfeeding duration could be explained by the influence of cultural beliefs and practices of the various ethnic groups in China on breastfeeding practices. For instance, some mothers may believe that the breast is filled with breast milk on the third day after childbirth, which may change the habit of breastfeeding (Asare et al., 2018). Breastfeeding is less normative among some ethnic groups (Zhang et al., 2020). In this case, the variations of breastfeeding patterns and the acculturation of ethnic minorities to the Han group should be provided to women from minorities by occupational health providers.
The present study confirmed the existing evidence that the maternal education level can influence breastfeeding duration. Employed women with higher education levels may learn more about the benefits of breastfeeding and remain committed to it in various ways. Similar results were also found in an investigation conducted in France (Castetbon et al., 2020). One study exploring breastfeeding intention of female physicians suggested that breastfeeding duration of employed women might be influenced by health educators and found that their intentions and knowledge correlated with their breastfeeding initiation practices (Sattari et al., 2016). Therefore, employed women with low education level should be offered to breastfeeding information and help by occupational health providers.
Compared with the lowest or the highest, women with middle-level household income were more likely to continue breastfeeding in the current study. Similar conclusion was found in some studies (Ajami et al., 2018; Qin et al., 2017). Women with low household income were prone to cease breastfeeding early (Santos et al., 2019). According to a study in China, infants whose mothers had a high score on the International Socio-Economic Index of Occupational Status (ISEI) were more likely to experience breastfeeding cessation, as were infants whose fathers had a high ISEI score (C. Chen, Cheng, & Pan, 2019). These findings were consistent with the results of the current study.
Maternity leave is closely related to any breastfeeding duration. Similarly, a review of the effects of maternity leave length and workplace policies on breastfeeding indicated that long maternity leave was one of the common facilitators to sustain breastfeeding (Steurer, 2017). Researchers found that employed women who took shorter maternity leave were more likely to stop breastfeeding in the first 6 months postpartum in a cohort study (Dagher et al., 2016).
In China, women are entitled to a 98-day paid maternity leave. However, maternity leave varies widely from country to country. In European, including Sweden, France, and Finland, mothers are given high levels of maternity leave, while in some Asian and African countries like Tunisia, it is not so satisfying. In European countries, including Sweden, France and Finland, maternity leave is between 3 and 8 months (Sonjia Blum et al., 2018; Ülla Jurviste & Chahri, 2022). In Asian and African countries like Tunisia, maternity leave is one month. A 1-hour breastfeeding break for the first year postpartum is allowed in some countries, such as Ireland and China (National HR Employee Helpdesk, 2021). Actually, many countries do not have these generous policies. Therefore, it should be discussed in combination with the specific national maternity leave policy.
Compared with employed women who stopped exclusive breastfeeding due to personal and work reasons, women had shorter exclusive breastfeeding duration due to family reasons. This emphasized the importance of family support for breastfeeding to employed women. Some mothers suggested that their family members could use this opportunity to help out if they worked nearby. But not all mothers get support from their family members in providing convenience to continue breastfeeding (J. Chen et al., 2019). Advocating family support is also important to continuing breastfeeding.
Commute time was one of the factors that influenced breastfeeding practices for mothers who had resumed work. Breastfeeding and caring for children demand time, energy, and effort. One study indicated that a long commute time negatively affects breastfeeding duration (J. Chen et al., 2019). If mothers live close to their employment site, they may go home during work breaks to feed their children, or with the help of family members to express breast milk. If the commute time is too long, breastfeeding may fail because of time and energy restrictions. Researchers found that during the COVID-19 pandemic, mothers are more likely to continue breastfeeding if they could work remotely (Badr & Alghamdi, 2022).
Strengths and Limitations
The present study is one of only a few that have examined the breastfeeding practices and breastfeeding support in the workplace among Chinese full-time employed women, providing evidence of the necessity of some related policies made by government and interventions made by occupational health providers. In addition, this study is based on a large, population-based survey with an extensive large sample size, providing for the generalizability of the findings among women returning to full-time employment while exclusively breastfeeding.
At the same time, it has several limitations. First, this was a cross-sectional study; it can only assess the influence of variables that are measured. Data in the study were based on self-reporting, which might involve recall bias or social desirability biases. Second, this study was only representative of women who returned to full-time work while still exclusively breastfeeding. Women with postpartum complications or with breastfeeding contraindications were not investigated. At last, not all of the women returned to work following national statutory maternity leave time in China. Maternity leave is different among countries and women are not entitled to breastfeeding break in many countries, which limits the generalizability of findings from this study. Therefore, longitudinal, multicentric studies are required in the future. The impact of maternity leave should be explored and discussed in combination with the specific national maternity leave policy.
Applying Research to Occupational Health Practice
This study presented information about breastfeeding practices, workplace breastfeeding support, and factors influencing breastfeeding of full-time employed women in China. The results suggested that current practices do not meet the WHO and Chinese government’s recommendations; mothers perceived a lack of technical and facility support in the workplace, and employers have not provided a breastfeeding-friendly work environment for women to facilitate continued breastfeeding practices. Occupational health professionals should collaborate with management to reduce barriers to breastfeeding at work. Furthermore, these findings have potential policy implications for longer maternity leave to achieve the WHO recommendations for breastfeeding duration of 2 years.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221126371 – Supplemental material for Breastfeeding Practices of Women Returning to Full-Time Employment in China: Prevalence and Determinants
Supplemental material, sj-docx-1-whs-10.1177_21650799221126371 for Breastfeeding Practices of Women Returning to Full-Time Employment in China: Prevalence and Determinants by Yi-Yan Huang, Qian Liu, Jun-Yan Li, Shu-Wen Yue, Bing Xue, Sharon R. Redding, Wen-Bin Zhou and Yan-Qiong Ouyang in Workplace Health & Safety
Footnotes
Acknowledgements
We want to give a special thanks to the women who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.