
Abstract
This article explores stakeholders’ perceptions of the quality of occupational health service (OHS) delivery in South Africa. Using a purposive sampling technique, 11 focus group discussions (FGDs) were conducted in three provinces. Focus group participants (n = 69) were recruited through professional organizations of occupational physicians and occupational health nurses as well as employer representatives of major industries in South Africa. Transcriptions of FGDs were analyzed using thematic content analysis. South Africa has diverse models of OHS delivery with varying quality. Focus group participants criticized the outsourced model of service delivery and the excessive focus on physical examinations to achieve legal compliance. These problems are exacerbated by a perceived lack of employer emphasis on occupational health, insufficient human and financial resources, and lack of specific quality of care standards for occupational health. Improvement in the quality of OHS delivery is essential to realize South Africa’s quest for universal health coverage.
Keywords
In September 2015, the United Nations reiterated the centrality of universal health coverage and access to quality health care to achieving the 2030 sustainable development goals (United Nations, 2015). The notion of quality of care has generated a significant body of literature, both on its definition and measurement, and the increasing attention it has received from governments, health service providers, and the public (Casparie, 1998; Chassin & Galvin, 1998; Donabedian, 1978; Institute of Medicine, 2001; Shaw, 2004, 2006; Varkey, Reller, & Resar, 2007). The Donabedian framework posits that quality of health care results from a relationship among structure or the conditions under which care is provided, process or the activities that provide care, and outcome, often reflected or measured in individual health or care outcomes as depicted in Figure 1 (Donabedian, 2003). Although definitions of quality differ, the World Health Organization (WHO; 2009) defines quality as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (p. 18). Quality health care ensures patient safety, improves clinical effectiveness, promotes public accountability, and enhances the performance of national health systems (Shaw, 2004; WHO, 2007). In contrast, suboptimal quality of care results in negative consequences, including avoidable deaths, disability, and wasted resources (Chassin & Galvin, 1998), and in some instances could aggravate health inequalities (Figueras, McKee, Lessof, Duran, & Menabde, 2008).
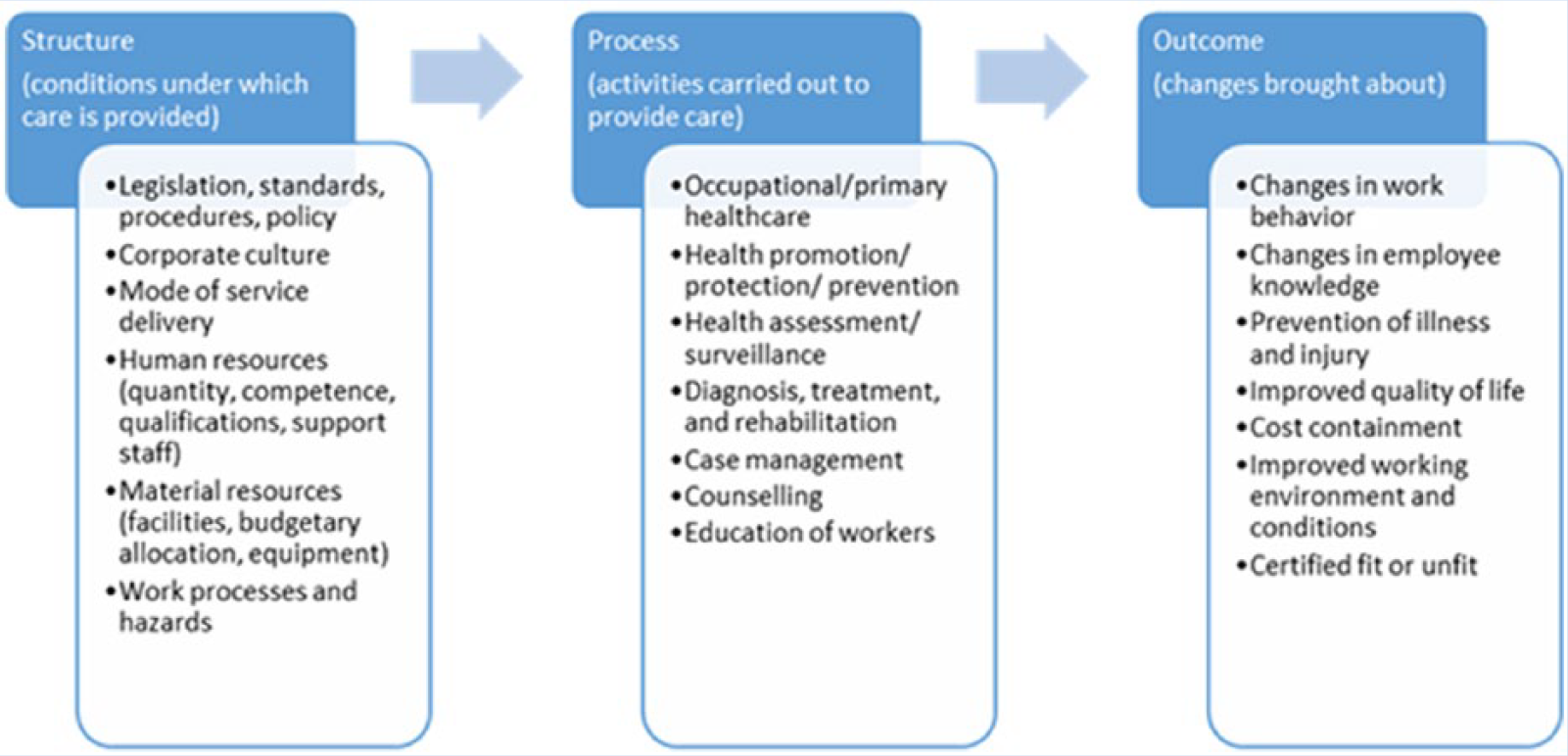
Listed aspects of quality assurance in OHS using the Donabedian Model.
In South Africa, quality of care initiatives have been a major part of the health policy reform agenda since democracy (Department of Health, 1997), but these initiatives must still be addressed in the country’s quest for universal health coverage (Armstrong, Rispel, & Penn-Kekana, 2015; The Presidency, 2014). The establishment of the Office of Health Standards Compliance in 2014 as an independent regulator was meant to ensure the protection and promotion of health service users’ health and safety and the enforcement of compliance with prescribed norms and standards (i.e., the National Core Standards; South Africa, 2013).
Notwithstanding the global focus and vast literature on quality of care, insufficient attention has been paid to the quality of occupational health service (OHS) delivery. Both the United Nations and the Commission on Social Determinants of Health have highlighted the need for a healthy, well-educated workforce and compliance with Occupational Health and Safety standards to enable all workers to participate fully and productively in society (Commission on Social Determinants of Health, 2008; United Nations, 2015). Unfortunately, workplaces can cause debilitating morbidity, disability, or death (Delclos et al., 2007; Fingerhut et al., 2005; Michell, 2010; Murray, Davies, & Rees, 2011), with the resulting financial burden for both individuals and society (Loewenson, 2001; Macdonald, 1992; Yodaiken & Zeitz, 1993). Occupational health service personnel can identify occupational diseases through early detection of deviations in health associated with occupational exposures (Casparie, 1998; De Valk, Oostrom, & Schrijvers, 2006; International Labour Organisation, 2009; Michell, 2012). Surveillance is used to monitor worker health and is defined by Rogers as “the systematic ongoing analysis, collection and evaluation of employee health data to identify specific instances of illness or health trends suggesting an adverse effect of workplace exposure” (Rogers, 2003).
In South Africa, more than 15 million workers are employed in the formal sector (Statistics South Africa, 2014). The National Core Standards emphasize effective occupational health and safety systems for staff in health facilities, but do not set specific standards for OHS outside this sector (Department of Health, 2011b). The provision of OHS is complicated by the three legislative frameworks that govern these services (i.e., the Department of Mineral Resources governs occupational health in mining and quarries; the Department of Labour governs occupational health in all other sectors; and the Department of Health governs health care establishments and has little involvement in occupational health). The Occupational Health and Safety (OSH) Act (South Africa, 1993) and the Mines Health and Safety (MHS) Act (South Africa, 1996) govern OHS in South Africa and prescribe employer responsibility to implement risk-based physical examinations and certificate of fitness (COF) assessments to determine employees’ fitness to work. However, no statutory controls over, or policy guidelines on the establishment and implementation of these services have been promulgated. Limited literature on the quality of OHS in South Africa is available. Investigations into the quality of audiometry (Michell, 2012), spirometry (Michell, 2003), and occupational health histories (Oosthuizen, 2009) have found suboptimal quality in service delivery and lack of compliance with recognized standards.
In light of major impending health sector reforms in South Africa, including the statutory accreditation of all health care establishments (South Africa, 2013), this study explored stakeholders’ perceptions of the models and quality of OHS delivery in South Africa. The research is part of a larger doctoral study that examined the governance, quality and accreditation of OHS in South Africa.
Method
The University of the Witwatersrand Human Research Ethics Committee (Medical) (M140442) granted study approval and standard ethical procedures were followed. During 2014, three South African provinces—Gauteng, KwaZulu-Natal, and Western Cape—were selected purposively for an in-depth qualitative study because of the concentration of major industries, location of relevant occupational health (OH) governance authorities, and geographical access along with the researchers’ budgetary constraints. The inclusion criteria for focus group participants were occupational health expertise or professional interest ensuring broad representation from professional bodies, trade unions, current practitioners (occupational health nurses and occupational physicians), and employers from a range of industries (e.g., mining, retail). The purpose of the focus group discussions (FGDs) was to gather qualitative information from various stakeholders about the models of care provision and their perceptions of OHS delivery quality.
Using a purposive sampling technique and the above-mentioned criteria, FGDs were conducted in three provinces after securing informed consent from each participant. One researcher (K.E.M.) conducted all the FGDs, facilitating 11 FGDs in the provinces of Kwa Zulu Natal (n = 2), Western Cape (n = 2), and Gauteng (n = 7), reaching a total of 69 respondents from various stakeholder groups and all models of OHS (Table 1).
Summary of the Affiliations of Focus Group Participants
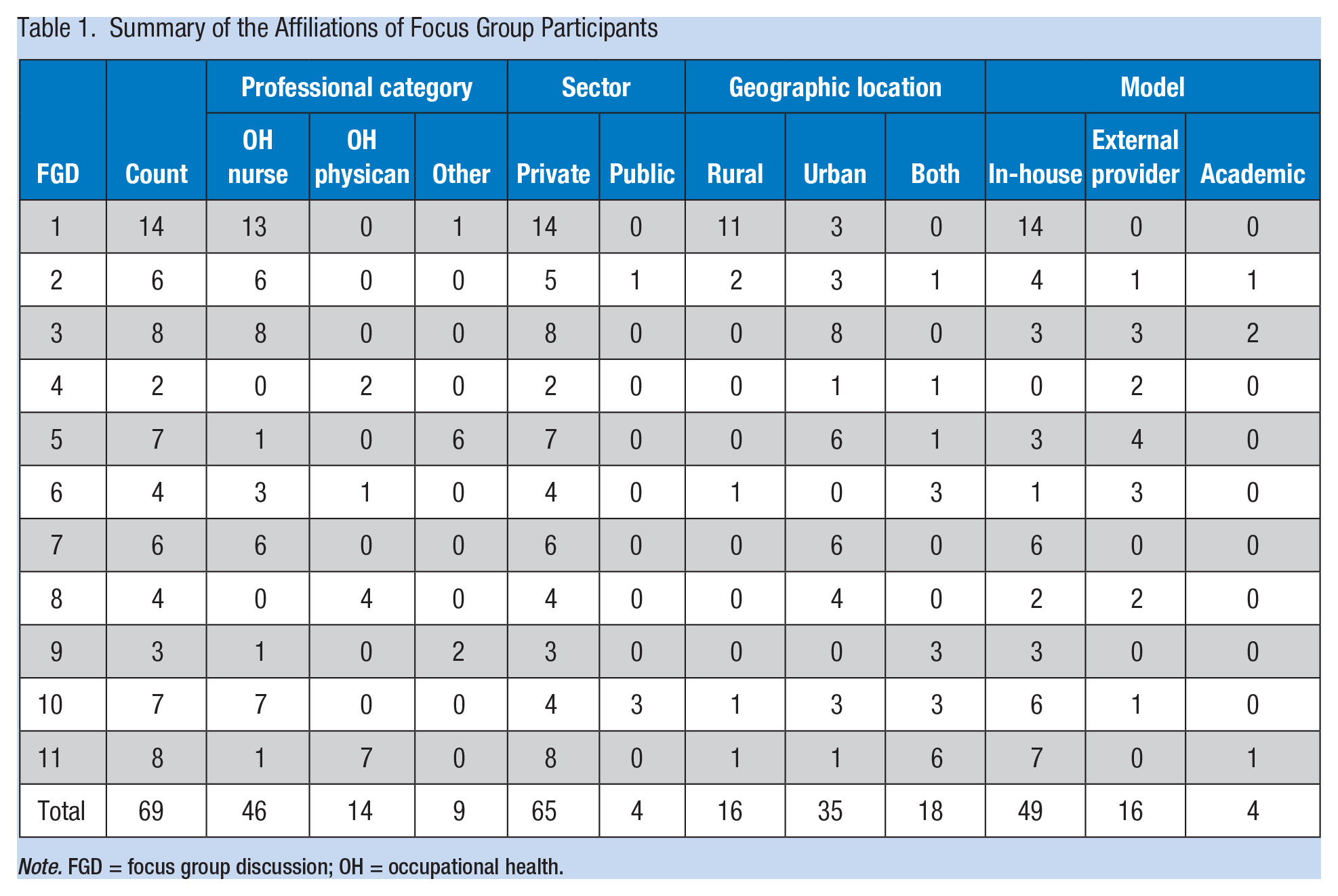
Note. FGD = focus group discussion; OH = occupational health.
The guiding discussion questions focused on current models of service delivery, participants’ involvement in OHS quality assurance, perceptions of OHS quality in their own industries and in South Africa, and their recommendations for OHS delivery. Each FGD lasted approximately 1 hour, but varied depending on the number of and discussion among participants. Interviews were digitally recorded, transcribed verbatim, and reviewed by the researcher for accuracy.
The data were analyzed using thematic content analysis (Polit & Beck, 2012). The first step in the analysis was to examine participants’ words and phrases in two of the FGDs without preconceived notions or classification. To ensure reliability, two researchers with OH experience were given the same FGD transcripts to code independently from each other. The coded transcripts were reviewed to ensure the same coding had been applied. Where inconsistencies in coding were identified, differences were discussed until agreement was reached. A code book was developed based on recurring themes, and all FGDs were analyzed using MAXQDA version 11.
Results
Focus group participants described various models of OHS in South Africa (Figure 2). The in-house model established an OHS at the place of employment. Although services tended to be more comprehensive, the scope was determined by the employer’s interpretation of existing legislation, workplace exposures, employee health needs, and available budget. The services could be provided by either a full-time or part-time occupational health practitioner (occupational physician and/or occupational health nurse) employed by the company or through service providers. The outsourced or external model offered services from a provider outside the company. This model was used by smaller employers with limited resources. The services could be delivered in a mobile structure provided by the service provider or a temporary room(s) provided by the employer at the place of employment. A hybrid of these two models was a walk-in facility, characterized by an OHS at a venue in close proximity to a number of industries; employees are referred to these facilities for required physical examinations on a fee-for-service basis. Focus group participants described varying quality across all OHS models, a recurring theme through all discussions. Participants believed this variation resulted from both structural and process issues. Although these issues overlap, they are described below using Donabedian’s (1978) notion about the structure and process of care quality.
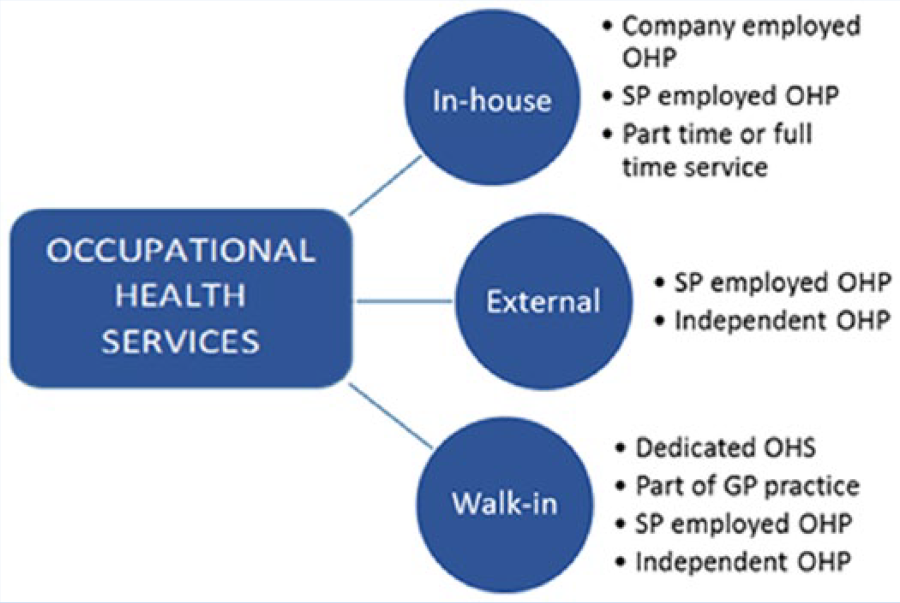
Representation of the models of OHS.
Structural Issues Influencing the Quality of OHSs
Structural issues affecting OHS quality included the type of OHS model provided by the employer, lack of understanding about and/or prioritization of OHS at the company, inadequate emphasis on standards or quality of services, insufficient financial and human resources for OHS, and the desire of employers to save money on OHS. Perverse incentives on the part of external service providers to save costs were also identified. Focus group participants believed that the in-house model provided better OHS quality because both employer and practitioner were involved in the provision of services, continuity of care was emphasized, and workers received ongoing monitoring and additional health care treatment after screenings as illustrated by the comments below: You have to appreciate, if you are working for a company and you are stationed at the company and you are part of the company then it’s different from working for a contractor, because I previously used to work for a contractor. So you do the medical [examination] and so you are not there for the follow up and to see what happens with this patient. So if he was unfit, does he get treatment, what happens to him? (Focus Group 1 participant, Kwa-Zulu Natal)
Although focus group participants recognized that outsourced services may be warranted, the majority expressed negative views on this model, often referring to this model in derogatory terms as the bakkie brigades (bakkie = small van). These OHS were often limited in scope, established to achieve legal compliance and provided in substandard physical facilities. This OHS model is also less expensive for the company and the general perception was that outsourced services provided inferior quality of care, illustrated by the comments below.
I think mobile services have become easy money-making opportunity for nurses [as SP] and because of that, because there is a bit of competition, it also becomes price sensitive. The way they keep their prices down, is by reducing their quality . . . They [employers] don’t look at the quality, they look at the price of the service rendered. (Focus Group 11 participant, Gauteng) More and more companies are opting for this once a year mobile [OHS service] that comes in and then we use the boardroom and out goes OH for the rest of the year. Personally I don’t believe in mobile clinics at all because there is no consistency and there is no continuation, it’s a different person, it’s a different form, it’s a different day, it’s different equipment, you can’t compare apples and pears, so what you basically do is just a once-off truck stop. (Focus Group 4 participant, Western Cape)
Physicians provided examples of how an external SP prioritizes financial over quality concerns when contracts are renewed.
You’re (the physician) not allowed to address this (quality) issue until we have secured the tender again. (Focus Group 4)
Further examples of the financial priorities over quality related to managers setting unrealistic workloads for practitioners and understaffing to increase profit margins; service providers “pushing the numbers” (e.g., booking as many physical examinations in a session as possible; Focus Group 7, Gauteng), a single occupational health nurse conducting physical examinations on up to 60 workers a day (Focus Group 6), and a physician issuing certificates of fitness for up to 80 workers in a morning (Focus Group 5).
Participants reported that employers’ lack of understanding about OHS is a structural constraint to quality service delivery. An occupational health nurse stated that employers have limited understanding of OH, as it is not their core business.
Employers are not educated enough when they make a decision on a service provider or even if they employ a nurse. They have no idea what qualities the nurse must have to fulfill this job because they have no idea what an OHS does. (Focus Group 2, KwaZulu Natal)
This view was also communicated by a physician in another focus group: I think they [employers] want to have basic legal compliance and they search for the cheapest option to reach that, but the essence or the principles of the OHS doesn’t really matter to the company. (Focus Group 4, Western Cape)
The described lack of understanding of OH by employers is exacerbated by employers’ low priority for OHS. The situation is further complicated by companies’ workplace HIV and wellness programs, which tend to overshadow occupational health. As stated by a focus group participant, They [employers] are displacing the focus and instead of being interested in occupational health they are more interested in how many HIV tests did we do, did we have a wellness day for chronic conditions. (Focus Group 2, Kwa Zulu Natal)
Participants were of the opinion that lack of OH-specific standards influences quality of services provided: We have regulations that say you must have been medically examined . . . that you must have a certificate of fitness . . . but there is nothing that states what those examinations should include. (Focus Group 8, Gauteng) If you open a General Practice, you know your premises have to be inspected. In OH you’re not treating anyone so nothing gets inspected . . . which means that you could be put into a broom cupboard at the back of a factory. (Focus Group 4, Western Cape)
The employers were of the opinion that an absence of standards leaves them vulnerable to exploitation, a situation compounded by the absence of sanctions when complaints are raised.
My concern, it’s that there is no standard set for this (medical examination), and in terms of a universally or countrywide accepted medical, there is no quality system and no sanction on substandard performance. (Focus Group 5, Gauteng)
The majority of participants reported that insufficient financial and human resources were available for OHS. Practitioners reported a disconnect between the OHS the employer wants and the cost they are willing to pay for these services. This disconnect is exacerbated by a perceived decline in the competence of OH practitioners, with reports of occupational physicians who are unable to interpret an audiogram or spirogram, and occupational health nurses who cannot conduct a physical examination. Participants believed that the lack of standardization of OH training programs and accompanying lack of mentorship contribute to competency concerns.
Process Issues Influencing the Quality of OHS
The process issues raised included excessive focus on physical examinations to achieve legal compliance, variations in type and range of OHS provided, poor application of the principles of health surveillance, and the lack of case management and continuous monitoring.
The study participants criticized the excessive focus on the completion of physical examinations to achieve legal compliance, rather than focusing on the goals or quality of these examinations.
They do mindless medicals in this country because they [examinations] are not worth anything. (Focus Group 6, Gauteng) Here comes my concern—it’s that there is no standard set for this, and in terms of a universally or countrywide accepted medical [examination] there is no quality system and no sanction on substandard performance. It doesn’t matter if they [workers] go to Medupi or they go to a Transnet or they go to a Sasol . . . it [medical certificate] is accepted. (Focus Group 5, Gauteng) I honestly feel that the person that’s been the most done in at the moment by OH is actually those employers and employees because . . . the employer is paying for a service that actually isn’t worth the piece of paper that it’s written on in many cases; the employee often is going through a sausage machine that adds absolutely no value to him. I feel that when you finish an OH medical . . . you should have a solution at the end of that [examination], which actually brings value to the person’s life. (Focus Group 1, Kwa Zulu Natal)
The employers complained about variations in type and range of OHS provided as shown below: There is no specific standard like A to Z should be done on each and every medical. You’ll get a service provider that says we want to do a drug test, the other one will not do a drug test . . . (Focus Group 5, Gauteng) A physical [examination] done by one person and physical done by another person could be completely different. There is no document that says a physical [examination] needs to ask the following sets of questions . . . (Focus Group 5, Gauteng)
This concern was reiterated by nurses and physicians who stated inconsistencies in service provision are due to the lack of OH-specific standards.
You follow the audiometry guidelines, you follow the spirometry guidelines, medical waste guideline, you follow whatever rumor is going around about the guidelines, but there is no structure that we can follow that is
The principles of health surveillance include the systematic review of workers’ health to monitor changes associated with workplace exposures. Physicians and nurses believed that the current approach to surveillance was not aligned with these principles.
We would be challenged in our country if we use the terminology medical surveillance. In many instances it is a medical examination at that point in time—and that’s not what OH is about. (Focus Group 6, Gauteng) In order for you to design a medical surveillance programme . . . you need to have health risk assessments that identify all the hazards and the associated risks that the employees are exposed to. Most of the companies are making use of the external providers and they don’t provide external providers with that particular information and now it ends up having medicals that are not risk based. (Focus Group 3, Cape Town)
The lack of case management and continuous monitoring of health problems identified during a physical examination was another concern expressed by focus group participants, particularly in the case of external service providers.
[Referring to external services] . . . they [employers] have got the mobile going around once a year and the next year if you see the chronic condition it’s not controlled, this [chronic condition] has never been sorted out, . . . so you can have 5 years of so-called surveillance, it’s not surveillance, it’s never properly managed . . . (Focus Group 4, Cape Town) They [practitioners] will examine the patients . . . and if there are people to be referred for medical conditions they will give the paperwork to the safety office. If you come back next year to follow up that paper is still with the safety officer and the patient still has the same problem. They did not even go to the medical facility you referred him to. (Focus Group 1, Kwa Zulu Natal)
Discussion
This is one of the first qualitative studies to explore the quality of OHS delivery in South Africa since the Office of Health Standards Compliance was established in 2014. Study participants discussed models of OHS delivery, and this discussion provided a foundation from which to initiate future OHS quality improvements.
However, focus group participants criticized the outsourced model of OH service delivery, and expressed preference for the in-house model, as the latter was perceived to provide opportunities for comprehensive OH service delivery, better value, enhanced quality of care, and integration with employer or company systems. This preference for the in-house OH service model has also been found in other studies (American Association of Occupational Health Nurses, 2013; De Valk et al., 2006; Venables & Allender, 2008b). Bråtveil, McCormack, and Moen (2001) found that need and geographical location influenced the model of OHS provision. However, the perception in this study was that employers select a model based on financial motivation and a desire to achieve legal compliance. A small South African study found that the outsourced model of OHS delivery enabled workers to access OHS when companies could not otherwise provide OHS due to high cost and lack of economies of scope and scale (Michell, 2012).
An emergence of outsourced service providers in South Africa is due to perceived commercial opportunities. Donabedian (2003) highlighted the importance of structure, which includes the adequacy of facilities and equipment and the nature of institutions providing care to overall health care quality. No empirical studies have evaluated models of OHS delivery. Hence, further research is needed to determine whether the perceptions of focus group participants about the benefits and disadvantages of particular models are borne out by a formal evaluation.
A recurring focus group theme was the perception of excessive focus on physical examinations to achieve legal compliance. This compliance focus was viewed negatively; participants believed the focus on compliance often led to suboptimal quality, inappropriate case management, and inadequate monitoring of identified health problems. Participants also felt that the focus on physical examinations mitigated a comprehensive approach to health surveillance. Existing occupational legislation in South Africa (South Africa, 1993, 1996) requires employers to conduct physical examinations for workers prior to and through their employment but does not address comprehensive OHS. This situation may explain participants’ perceptions of excessive focus by employers on physical examinations. The lack of statutory controls over and policy guidelines for the establishment and implementation of OHS is a contributing factor to the negative consequences of compliance-based physical examinations. Some researchers have suggested that increasing statutory controls is not without its challenges, stating that no clear evidence indicates how statutory controls affect practice (Braithwaite et al., 2010). Other studies have shown that implementing controls does improve quality (Lalloo, Demou, & Macdonald, 2015; Lukes & Schiavone, 2001). Lalloo et al. (2015) were unable to determine whether reported quality improvements in their study were due to practitioners’ desires to comply with established standards or that being given feedback indicated areas that needed improvement, which in itself led to improved quality of practice. Considering the current perceptions of suboptimal quality and the lack of statutory guidance for the implementation of OHS, further investigation into the development and statutory enforcement of OH-specific standards would be beneficial.
The lack of OH-specific standards to direct service delivery in South Africa was a recurring theme and perceived by participants to contribute to suboptimal OHS quality. OHSs monitor and protect the health of workers from potential harm caused by workplace exposures. Focus group participants believed that the lack of OH-specific standards allows employers to withhold employee exposure information from service providers; service providers conduct physical examinations but, without exposure information, cannot link health outcomes to workplace exposures. Bråtveil et al. (2001) described service providers’ inability to link occupational exposures to occupational illness as a weakness, which could be a contributing factor to the burden of occupational disease. When employers fail to give service providers accurate exposure information, examinations are of limited value to employers in terms of occupational disease prevention and early detection because the examinations are not based on risk assessments. Participants indicated that the lack of OHS standards has resulted in employers continued lack of occupational health awareness, low priority for securing quality OHSs at a reasonable price. A financially driven approach to buying OHS as opposed to a standards or quality driven approach does not serve the company or its workers. All stakeholders indicated that national OH standards could improve service delivery, perceptions supported by research in other countries where OHS quality improved following the implementation of regulated standards (Franco & Marquez, 2011; Migliozzi, 1990). However, the existence of standards for audiometry and spirometry (Michell, 2010; South African National Standards, 2008) did not result in service provider compliance (Michell, 2003, 2010). However, legislated standards would allow for enforcement, a key to quality found in other studies (Lukes & Schiavone, 2001).
Participants in this study were unaware of the Office of Health Standards Compliance and the Department of Health’s intention to certify health care facilities (Department of Health, 2011a) using the National Core Standards developed for this purpose (South Africa, 2013). When the framework from the Office of Health Standards Compliance and the National Core Standards was explained, participants agreed that OHS providers should be held accountable to the same certification processes as other health care facilities in an effort to improve the current quality of OHS delivery. However, stakeholders raised concerns that the current National Core Standards address the needs of hospitals and primary care clinics, the needs of which are dissimilar to those of OHS and that OHS delivery is not mentioned in the current policy documents. The inclusion of OHS in the Department of Health certification of health care establishments should be investigated as a method of quality improvement and quality control in this sector.
Focus group participants reported that the quality of OHS delivery was affected by human resources, including lack of trained occupational physicians and occupational health nurses, the declining competence of practitioners, and the understaffing of OH facilities with unrealistic workloads for existing practitioners. These concerns mirrored those described by Venables and Allender (2008) in an environment, similar to South Africa, with no legal obligation to offer comprehensive OHS. Understaffing of OHS is believed to be the consequence of both service providers and employers prioritizing commercial profit over care quality. Empirical information on the decline in practitioner competence is outside the scope of this study but warrants further research; national OH-specific standards should speak to staffing norms and standards to address the issues identified.
Limitations of the Study
Despite numerous attempts to include trade union representatives, the study did not include the views of employee representatives. Hence, further research is needed to gather a wider range of opinions including trade union representatives. In this study, no quantitative assessment of care or measurement of outcomes was included. Finally, the study was conducted at one point in time, and the information was directly influenced by focus group participants.
Conclusion
This study found that stakeholders perceived the quality of OHS to be suboptimal with a dominant concern regarding the financial motivation for service delivery and the apparent need to address employer and service provider priorities rather than the needs of workers. Study participants reported that the quality of OHS warrants attention for the benefit of all stakeholders; this could best be achieved through the development and enforcement of national OH-specific standards addressing the various models of OHS delivery, and should be considered a priority. Standards must be developed and enforced by a government department with the requisite political will and authority to do so. The Office of Health Standards Compliance as an independent regulator is well suited to assume this role with input from stakeholders. The South Africa National Department of Health has initiated plans to improve the quality of health care in South Africa through certification and this should apply equally to the OH sector. Through such an initiative, an overall improvement in the quality of OHS should be seen with enhanced accountability from all stakeholders and an expectant reduction in the burden of occupational disease, which is essential to realize South Africa’s quest for universal health coverage.
Applying Research to Practice
Several models of occupational health service (OHS) delivery have been implemented in South Africa with external services perceived as limited in scope, providing physical examinations to employees for meeting legal compliance as opposed to offering comprehensive OHSs. Occupational health stakeholders perceived the quality of South African OHS structural and process components to be suboptimal because the system is financially driven rather than standards driven. Occupational health-specific standards are nonexistent, resulting in an inconsistent approach to service delivery with no sanctions for suboptimal services. The Department of Health’s current initiative to improve the quality of health care in South Africa does not address the quality of OHS; these services should be subject to the same assessment and certification as other health care facilities. The implementation of OH-specific standards enforced by a government agency with requisite political will is likely to contribute to a decrease in the current burden of occupational disease.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was facilitated by attending the University of Witwatersrand, School of Public Health Thanda Ukubhala writing retreat, which received financial support from the Faculty of Health Sciences Research Office.
Author Biographies
Karen Michell is a member of Concept Safety Systems and a past president of the South African Society of Occupational Health Nurses, where she is also an honorary life member. She was inducted as a fellow of the Academy of Nursing South Africa in 2015. She has registered for a PhD at the School of Public Heath, University of Witwatersrand, South Africa, investigating the quality and governance of occupational health services in South Africa.
Laetitia Rispel is professor of public health and the head (dean) of the School of Public Health at the University of the Witwatersrand in Johannesburg, South Africa. She also holds a Department of Science and Technology/National Research Foundation research chair. She has published extensively on different aspects of health policy and health systems research that are central to many of the issues involved in the re-structuring and transformation of the South African health system.